The Sclera

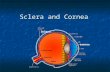
Sclera
** Also known as the white of the eye, is the opaque, fibrous, protective, outer layer of
fibers. elastic and collagen containing eye the (it forms 5/6 of the anterior outermost layer of the eye).
** It’s formed from interwoven collagen fibrils of different widths lying within a ground substance and maintained by fibroblasts.
** It’s of variable thickness, 1 mm around the optic nerve head and 0.3 mm just posterior to the muscle insertions.

** In adults, the sclera is white.
** In some children, the sclera is blue due to
it’s thinning that shows the pigment cells of
the choroid.
** In the elderly, it maybe yellow due to
deposition of fat.


Anatomy of the Sclera
• The Sclera is divided into 3 layers :
1) The episclera.
2) Scleral stroma.
3) Lamina fusca.

1) Episclera :
• it’s the outermost layer
• Anteriorly the episclera consists of a dense,
vascular connective tissue which lies between
the superficial scleral stroma and Tenon
capsule.
** Tenon capsule : the facial sheath that envelopes the
eyeball and seperates it from the orbital fat.

2) Scleral stroma :
• it’s a dense fibrous tissue with fine elastic fibers.
3) Lamina fusca :
it’s the innermost layer of the sclera , it
continues with the suprachoroidal and
supraciliary lamellae of the uveal tract.

Diseases of the sclera

Episcleritis
• It’s the inflammation of the superficial layer of the
sclera,it’s a common, benign, usually idiopathic,
recurrent and frequently bilateral condition.
• It causes mild discomfort , and it’s rarely associated with
systemic diseases.
• It’s usually self-limiting , but as the symptoms are
tiresome , topical anti-inflammatory treatment can be
given.
• In rare severe cases systemic anti-inflammatory drugs
maybe given.
• And it’s classified into simple and nodular types.

A. Simple Episcleritis
• Simple episcleritis accounts for 3/4 of all cases and predominantly affects females. It has a great tendency to recur either in the same eye, or sometimes both together. The attacks become less frequent and after many years disappear completely.
** Presentation is with redness and mild discomfort
** Signs Redness may be sectoral or diffuse. Often it has an interpalpebral distribution, in contrast with scleral disease which commonly starts in the upper temporal quadrants.
** Treatment If mild, no treatment is required. • Cool artificial tears may be adequate in some cases. • A weak topical steroid for 1–2 weeks is usually sufficient. • Oral NSAIDs are sometimes required for 10 days.

B. Nodular Episcleritis
• Nodular episcleritis also tends to affect young females
but has a less acute onset and a more prolonged course
than the simple variety.
**Presentation is with a red eye typically first noted on waking.
Over the next 2–3 days the area of redness increases in size,
becomes more uncomfortable, but remains in the same
position.
** Signs one or more tender nodules, almost always within the
interpalpebral fissure.
**Treatment is similar to that of simple episcleritis.

Simple episcleritis A.sectoral B.diffuse
Nodular episcleritis

Scleritis
** Scleritis is an uncommon condition characterized by edema and cellular infiltration of the entire thickness of the sclera. It is much less common than episcleritis and covers a spectrum ranging in severity from self-limiting episodes to a necrotizing disease that may involve adjacent tissues and threaten vision.
** It can be associated with collagen vascular diseases, most commonly rheumatoid arthritis.
** It causes intense occular pain, and both inflammatory and ischemic areas may occur in the sclera. ** Scleritis affecting the posterior part of the globe may cause choroidal effusions or simulate a tumor.

** The following may complicate the situation :
*Scleral thinning (scleromlalacia), sometimes with
perforation.
*Keratitis.
*Uveitis
*Cataract formation.
*Glaucoma.
** Treatment may require high doses of systemic
steroids or in severe cases cytotoxic therapy and
investigation to find any associated systemic
diseases.

Infectious scleritis
• Infectious scleritis is rare but may be difficult to diagnose because the initial clinical features may be similar to those of immune-mediated disease. In some cases infection may follow surgical or accidental trauma, severe endophthalmitis, or may occur as an extension of primary corneal infection .
• Causes : 1)herpes zoster. 2)tuberculous scleritis. 3)leprosy. 4)syphilis. 5)lyme disease.

Infectious scleritis

Blue sclera
** Blue discoloration is caused by thinning or
transparency of scleral collagen with
visualization of the underlying uvea.
**Important causes include the following:
1) Osteogenesis imperfecta.
2) Ehlers–Danlos syndrome type VI
3) Marshall–Smith syndrome , Russell–Silver syndrome ,
Hallermann–Streiff–François syndrome.

Osteogenesis Imperfecta
** It is an inherited disease of connective tissue, usually caused by defects in the synthesis and structure of Type 1 collagen. There are multiple types, at least two of which have ocular features.

Yellow Sclera
** It manifests in jaundiced patients, it’s not
due to pigment on the slcera itself but to
accumulation of bilirubin in the vascular
cojunctiva.

Thank you
Hala Shatnawi