GM Devolution: CAMHS Revolution – Eating Disorders Leading the Way
Dr Sandeep Ranote – NHSE Strategic Clinical Network Lead - CAMHS
WHY, HOW & WHEN?
1 in 150 female YP – anorexia nervosa (AN)
1 in 25 female in lifetime – bulimia nervosa (BN)
90% female
1.6 million UK people directly affected – BEAT 2007
High rates of co-morbidity
AN highest mortality of any psychiatric disorder
Geographical variations in service provision still high
Total annual UK cost £1.2 bn - £9.6 bn – BEAT review 2012 & 2014
Carer burden high and underestimated
CAMHS use of tier 4 admission for ED high > 35%
Often due to poor/no specialist community or ‘mini team’ provision

WHY, HOW & WHEN?
Wigan pilot (> 200 families) demonstrates need
> 90% families treated rated service 4/5 out of 5
> 90% families would recommend service (F & F
test)
> 85% improved outcomes
10-12% admission rate to Tier 4
Increase in admissions seen in 2013 with
national picture

WHY, HOW & WHEN?Evidence base supports CEDS-CYP – community adolescent eating disorder service as most cost effective
MDT integrated model recommended
Partnership working
Critical window for intervention 3-5 years
Clear transition pathway
Multimodal therapeutic package of care, person centred, evidence based, National clinical outcome measures (DATA!)
EARLY INTERVENTION KEY – delay increases long term health costs
Shared decision making
Experts by experience to co-develop pathways
Recovery Model
More studies underway

ASPIRATIONS
Education and training in primary care and schools
Junior MARSIPAN in reach to paediatric ward / Junior
MARSIPAN hub
Day unit
Tier 4 provision
0-25 or ageless service
Peer Mentoring
Parent Support Groups led by parents
Primary care / schools link

WHAT NOW?
£30m recurrent funding – Autumn budget 2014
£150m in total over 5 years
Transformation of services in England for children and
young people with eating disorders up to 18 years old
Development of CEDS-CYP
Population minimum for service – 500k (all ages)
Access and waiting time standards guide – July 2015
National whole team training curriculum – 2016
QNCC CEDS-CYP Standards - 2016

WHAT NOW?

Wigan Borough ED CQUIN
Tier 4 Specialist Eating Disorder Unit

Proposed CEDS-CYP Pathway
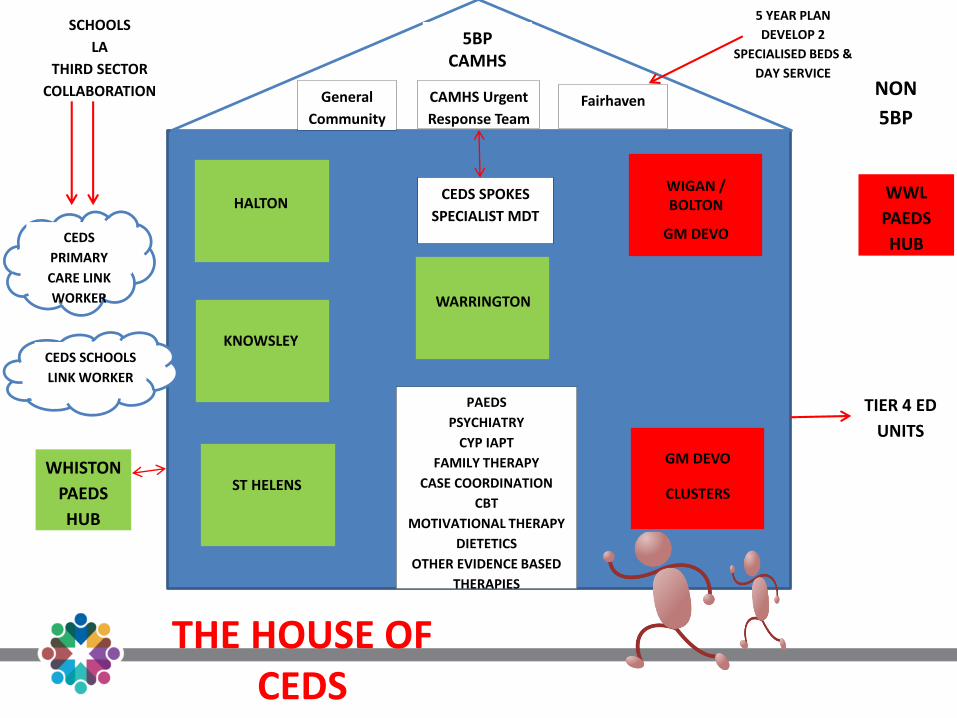
CEDS SCHOOLS
LINK WORKER
CEDS
PRIMARY
CARE LINK
WORKER
TIER 4 ED
UNITS
NON
5BP
5BP CAMHS
General
Community
CAMHS Urgent
Response TeamFairhaven
5 YEAR PLAN
DEVELOP 2
SPECIALISED BEDS &
DAY SERVICE
SCHOOLS
LA
THIRD SECTOR
COLLABORATION
HALTONCEDS SPOKES
SPECIALIST MDT
WIGAN / BOLTON
GM DEVO
WARRINGTON
ST HELENS
KNOWSLEY
PAEDS
PSYCHIATRY
CYP IAPT
FAMILY THERAPY
CASE COORDINATION
CBT
MOTIVATIONAL THERAPY
DIETETICS
OTHER EVIDENCE BASED
THERAPIES
THE HOUSE OF CEDS
WWL
PAEDS
HUB
GM DEVO
CLUSTERS
WHISTON
PAEDS
HUB

Community Eating Disorder Service
• Population-based: minimum 500K (all ages) so may span more than one CCG • Referrals for anorexia nervosa, bulimia nervosa, binge eating disorders and co-existing
problems (e.g. anxiety and depression)• Min of 50 referrals per year• Enable direct access to community eating disorder treatment via self-referral, GPs,
schools, colleges and voluntary sectorTable 5: Whole time equivalent staff broken down by profession
Number of referrals per annum
Head of service (psychiatry/psychology)
Clinical psychologists
Eating disorder therapists (SFT-ED/MSFP-ED/CBT-ED)
Nursing staff (nursing/home treatment)
Speciality doctors (psychiatry)
Assistant psychologists (SFP-ED/ MSFP-ED/CBT-ED support)
Paediatricians (physical health)
Dieticians
Administrative staff

GM DEVO
• Strategic priority
• 3 Clusters
Pennine
Salford/Central
Wigan/Bolton
• Networked approach
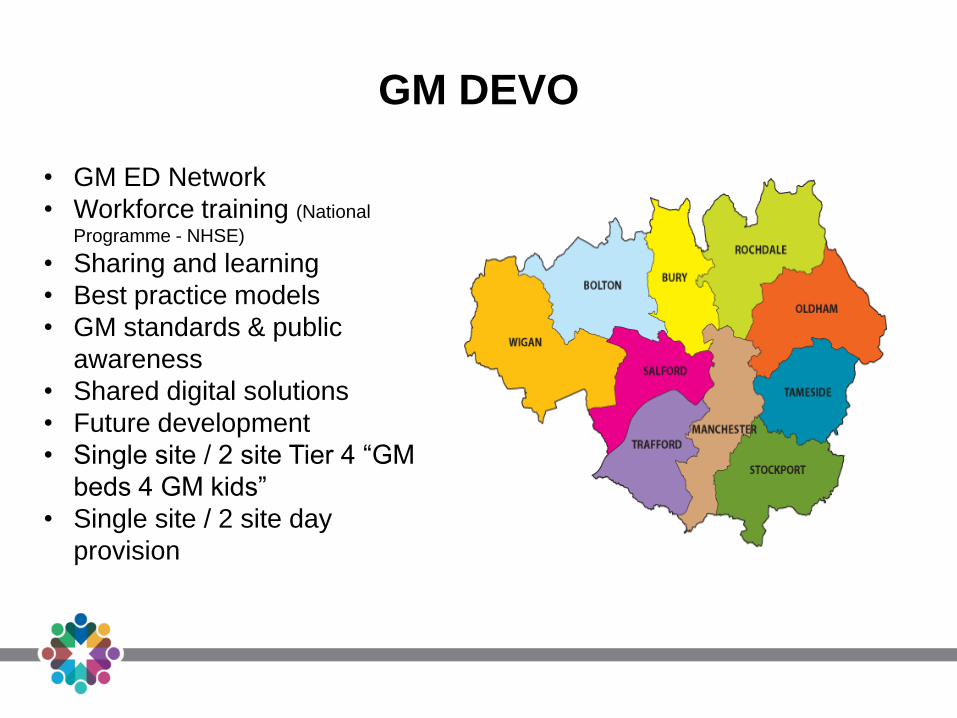
GM DEVO
• GM ED Network
• Workforce training (National
Programme - NHSE)
• Sharing and learning
• Best practice models
• GM standards & public
awareness
• Shared digital solutions
• Future development
• Single site / 2 site Tier 4 “GM
beds 4 GM kids”
• Single site / 2 site day
provision

GM DEVO
• Shared VCS / University work
• School / primary care work
• Thrive
• Minded 4 MCR
• KPIs
• Crisis
• Service specification

ILLNESS IMAGERY
“BITCH”
“IT”

CLINICAL LEADERSHIP
Collective leadership
Creative talent mapping
Clinical voice and drive
Clinical quality
Clinical conduit

GM DEVOLUTION: HEALTHCARE
REVOLUTION

Children & Young People
A third of our population BUT all
Of our future
@GMLSC_SCNs
#time4CAMHS2Bseen&heard