


Review: Pharmacokinetics of illicit drugs in oral fluid
Olaf H. Drummer *
Victorian Institute of Forensic Medicine and Department of Forensic Medicine, Monash University,
57-83 Kavanagh Street, Southbank, Melbourne 3006, Australia
Received 4 November 2004; received in revised form 22 November 2004; accepted 22 November 2004
Available online 18 April 2005
www.elsevier.com/locate/forsciint
Forensic Science International 150 (2005) 133–142
Abstract
This article reviews studies that have measured drug concentrations in oral fluid following controlled dosing regimens. A
total of 23 studies have been identified over the last 15 years. These show that the amphetamines including designer
amphetamines, cocaine, cannabis and cocaine are quickly found in oral fluid following dosing and usually have similar
time-courses to that in plasma. Following common doses peak oral fluid concentrations exceed 0.1 mg/mL and often even 1 mg/
mL. The drug concentration will depend on whether a dilution step occurs with buffer as part of the sampling procedure. The
uses of collectors that stimulate oral fluid usually reduce the drug concentration compared to a non-stimulated manner. This
reduction will not disadvantage the recipient since it will potentially reduce the detectablity of drug in oral fluid compared to
non-stimulated collections. Only one recent study has been reported for a benzodiazepine. This showed nanogram per milliliter
concentrations for flunitrazepam. More studies are required for benzodiazepines and indeed for other drugs, particularly in
multiple drug situations and where disease may affect the pharmacokinetics of drugs.
# 2005 Elsevier Ireland Ltd. All rights reserved.
Keywords: Pharmacokinetics; Oral fluid; Drugs of abuse; Review
1. Introduction
The use of oral fluid (OF) to detect the presence of illicit
drugs has become increasingly popular as a non-invasive
specimen to detect drug-use [1].
A number of devices are now available to screen OF for
the presence of recreational drugs. The drugs of most interest
are amphetamines, ecstasy (MDMA), cocaine, opiates (mor-
phine, codeine), benzodiazepines and cannabis [1,2].
For the most part studies have shown that OF contains
predominately the parent drug. For example, cocaine is the
major species present in OF following the use of cocaine
[3–5], heroin and 6-acetylmorphine are dominant species
following use of heroin [6], while tetrahydrocannabinol
(THC) is the predominant species following smoking of
cannabis products [7,8].
* Tel.: +61 3 9684 4334; fax: +61 3 9682 7353.
E-mail address: [email protected].
0379-0738/$ – see front matter # 2005 Elsevier Ireland Ltd. All rights r
doi:10.1016/j.forsciint.2004.11.022
Schramm et al. [9] has provided an early review on
detection times and early studies pre 1990s. Other reviews
on the testing for drugs of abuse in OF also exist [10,11].
Pharmacokinetic studies provide an ability to determine
the concentration of target drugs following known doses, and
therefore provide an ability to assess the required sensitivity
of oral fluid drug-detecting devices. A number of these have
been conducted over the last 15 years.
This paper reviews published works that have measured
the concentration of recreational drugs in oral fluid follow-
ing a known dose of drug in volunteers.
2. Methods
Published peer-reviewed studies from 1990 were identi-
fied through references listed in known published studies.
Other studies were identified by using the public MedLine
database PubMed using the search string ‘‘pharmacokinetics
eserved.
O.H
.D
rum
mer
/Fo
rensic
Scien
ceIn
terna
tion
al
15
0(2
00
5)
13
3–
14
21
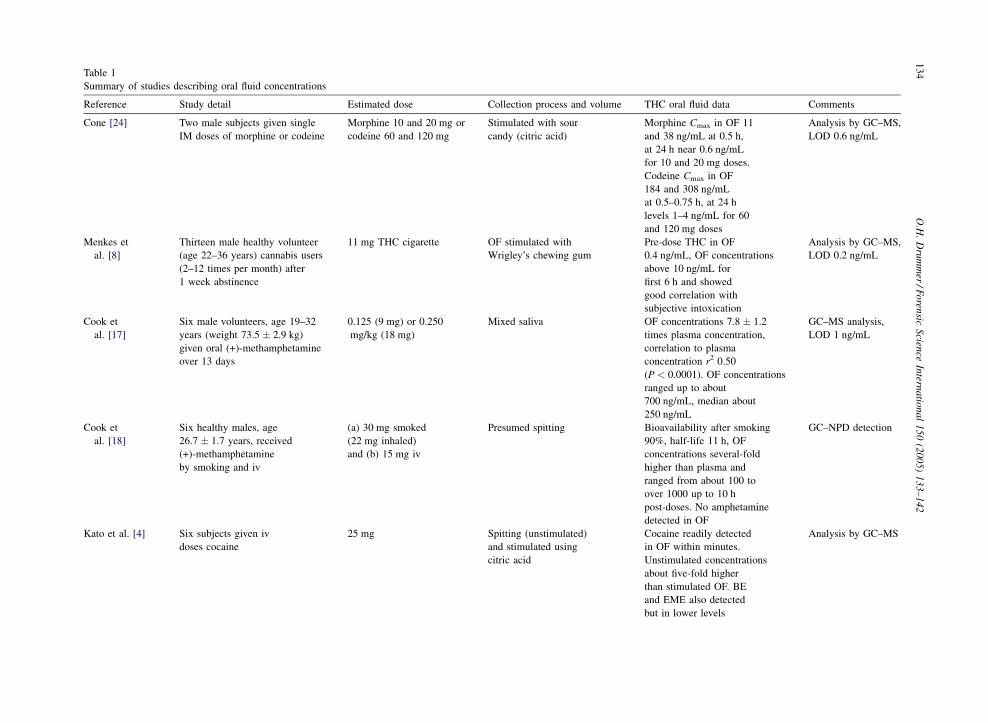
34Table 1
Summary of studies describing oral fluid concentrations
Reference Study detail Estimated dose Collection process and volume THC oral fluid data Comments
Cone [24] Two male subjects given single
IM doses of morphine or codeine
Morphine 10 and 20 mg or
codeine 60 and 120 mg
Stimulated with sour
candy (citric acid)
Morphine Cmax in OF 11
and 38 ng/mL at 0.5 h,
at 24 h near 0.6 ng/mL
for 10 and 20 mg doses.
Codeine Cmax in OF
184 and 308 ng/mL
at 0.5–0.75 h, at 24 h
levels 1–4 ng/mL for 60
and 120 mg doses
Analysis by GC–MS,
LOD 0.6 ng/mL
Menkes et
al. [8]
Thirteen male healthy volunteer
(age 22–36 years) cannabis users
(2–12 times per month) after
1 week abstinence
11 mg THC cigarette OF stimulated with
Wrigley’s chewing gum
Pre-dose THC in OF
0.4 ng/mL, OF concentrations
above 10 ng/mL for
first 6 h and showed
good correlation with
subjective intoxication
Analysis by GC–MS,
LOD 0.2 ng/mL
Cook et
al. [17]
Six male volunteers, age 19–32
years (weight 73.5 � 2.9 kg)
given oral (+)-methamphetamine
over 13 days
0.125 (9 mg) or 0.250
mg/kg (18 mg)
Mixed saliva OF concentrations 7.8 � 1.2
times plasma concentration,
correlation to plasma
concentration r2 0.50
(P < 0.0001). OF concentrations
ranged up to about
700 ng/mL, median about
250 ng/mL
GC–MS analysis,
LOD 1 ng/mL
Cook et
al. [18]
Six healthy males, age
26.7 � 1.7 years, received
(+)-methamphetamine
by smoking and iv
(a) 30 mg smoked
(22 mg inhaled)
and (b) 15 mg iv
Presumed spitting Bioavailability after smoking
90%, half-life 11 h, OF
concentrations several-fold
higher than plasma and
ranged from about 100 to
over 1000 up to 10 h
post-doses. No amphetamine
detected in OF
GC–NPD detection
Kato et al. [4] Six subjects given iv
doses cocaine
25 mg Spitting (unstimulated)
and stimulated using
citric acid
Cocaine readily detected
in OF within minutes.
Unstimulated concentrations
about five-fold higher
than stimulated OF. BE
and EME also detected
but in lower levels
Analysis by GC–MS
O.H
.D
rum
mer
/Fo
rensic
Scien
ceIn
terna
tion
al
15
0(2
00
5)
13
3–
14
21
35
Cone et al. [5] Male volunteers with a history
of cocaine abuse, given cocaine
by iv, intranasal, smoking
25 mg iv, 42 mg smoking Spitting with citric acid
stimulation
Readily detectable
concentrations on OF,
BE and EME also present
after all routes. S/P ratio
cocaine 3
Analysis by GC–MS,
citric acid stabilizes
cocaine loss with
NaF. LOD 1 ng/mL
Wang et al. [23] One subject received
intranasal heroin
12 mg heroin HCl Presumed spitting Heroin detected in OF
at 5 min, peak at 10 min
(308 ng/mL) and detectable
to about 1 h. 6-AM detected
at 5 min, peak concentration
at 10 min (59 ng/mL) and
detectable to about 6 h,
morphine detectable from
5 min to 4 h (peak
25 ng/mL at 1 h)
GC–MS, LOD
about 1 ng/mL
Jenkins et al. [6] Two subjects each received
smoked or iv doses of heroin
or cocaine in separate studies
Cocaine 44.8 mg iv or
40 mg smoked, heroin
5–20 mg iv or 2.6–12 mg
base smoked
Spitting with citric acid
stimulation 4 mL
Cmax heroin >3000 ng/mL
at 2–5 min after smoking,
and after iv Cmax was
6–20 ng/mL (3–12 mg
doses). Not detectable
after 5–30 min with lower
doses, but detectable to
24 h after 12 mg dose.
6-AM and morphine also
detected. Peak morphine
<16 ng/mL after iv. S/P
ratio for morphine about
1. Cmax cocaine 428–1927
at 5–30 min after iv doses.
BE also detected at lower
concentrations after iv
and smoked doses.
AEME detected after
smoking. Detection time
in OF about 8 h
Analysis by GC–
MS, LOD 1 ng/mL
for all analytes
Kintz [21] Single dose of MBDB to
one volunteer
100 mg MBDB No details provided Cmax 1083 ng/mL at 2 h.
MDBD detected to 17 h
with LOD 2 ng/mL. BDB
also detected, Cmax
146 ng/mL at 2 h
Analysis by GC–
MS, LOD 2 ng/mL

O.H
.D
rum
mer
/Fo
rensic
Scien
ceIn
terna
tion
al
15
0(2
00
5)
13
3–
14
21
36
Table 1 (Continued )
Reference Study detail Estimated dose Collection process and volume THC oral fluid data Comments
Moolchan et
al. [22]
Self-reported recent users of
cocaine studied
0.1–2 g daily, median
1.0 g
Spitting with citric acid
stimulation
Admission OF cocaine
31 � 50 (range 5–171),
BE 54 � 45 (4–144),
EME 69 � 112 (5–337).
T1/2 7.9 h longer than
plasma at 3.8 h
Analysis by GC–MS
after SPE, LOD 1
ng/mL
O’Neal et al. [26] Five volunteers given codeine
and OF collected at various
times with different collectors
Single 30 mg liquid
codeine phosphate
Spitting, sugarless gum,
lemon drop
stimulation, Salivette,
Finger Collector and
Orasure device
Cmax of OF after spitting
was 3542 � 1625 ng/mL
at 0.25 h. At 6 h level was
38 � 11 ng/mL. Stimulated
collection gave lower OF
concentrations: �3.6
(acidic), �2.0 (non-acidic),
�1.3 (Salivette), X � 0.3
(finger collector)
Analysis by GC–MS,
LOD 1 ng/mL
Navarro et
al. [20]
Twelve prior users screened
as extensive metabolizers
given oral MDMA
100 mg MDMA Spitting Cmax OF 3375 � 1812 ng/mL at
1.5 h and detectable to
about 24 h, S/P ratio
variable, average about
7 in post-absorption phase
Analysis
by GC–MS, LOQ
50 ng/mL
Skopp et al. [30] Six Subjects on dihydrocodeine,
single dose 20 subjects with
repeat dosing
60 mg single or once
daily repeat dosing
Salivette At 2 h OF level mean
784 � 346 ng/mL, at 12 h
mean OF level was 176 � 268.
Saliva/plasma ratio 1.2–17.
Mean OF levels in chronic use
were 10.8 � 14.9 mg/mL
(range 0.1–66 mg/mL)
Analysis by HPLC,
LOD 5, LOQ
20 ng/mL
Niedbala et
al. [12]
Eighteen prior users of cannabis,
age 19–25 years smoked for
20–30 min, two control subjects
were tested for passive intake,
three subjects consumed one
brownie
2–25 mg per cigarette
(dose), 20–25 mg
per brownie
Intercept cotton fiber
with 0.8 mL diluent—
0.4 mL average
Cmax THC �70 ng/mL
THC in OF above 1 ng/mL
for at least 16 h, at 1 h
THC was �25 ng/mL.
Two control subjects
had no GC–MS positive
THC in OF. Oral marijuana
gave Cmax THC 4 ng/mL
at 1–2 h
Cannabinoids screened
by microplate EIA
with a 1.0-ng/mL
cut-off and confirmed
for THC by GCMS–MS
with a 0.5-ng/mL cut-off
O.H
.D
rum
mer
/Fo
rensic
Scien
ceIn
terna
tion
al
15
0(2
00
5)
13
3–
14
21
37
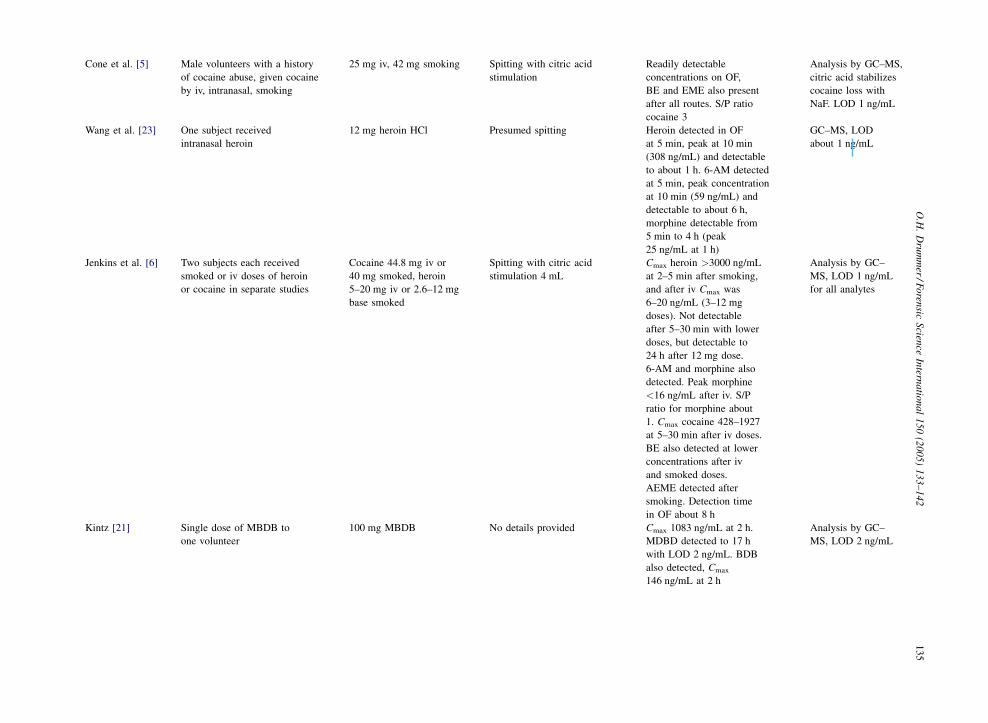
Kim et al. [27] Twelve males and seven female
healthy volunteers
(age 23–43 years) given codeine
sulfate orally
60 and 120 mg, three
doses each
Spitting with citric acid
stimulation
Cmax 639 � 64 ng/mL
(range 184–1288) and
1599 � 241 ng/mL
(range 620–3350) after
60 and 120 mg at 0.5–4 h.
S/P ratio 4. Detection
times were 7 and 21 h
after either dose using
cut-offs of 40 and 2.5
ng/mL. Some norcodeine
also detected.
Analysis by GC–MS
after SPE
Samyn et al. [19] Study 1: 12 healthy volunteers,
age 21–30 years given oral
MDMA. Study 2: users declare
amount of MDMA use before a
test drive
Study 1: 75 mg, Study 2:
25–95 mg initially and
from 0 to 4.5 additional
tablets
Spitting Study 1: Cmax 1215 � 944
ng/mL at 2 h. S/P ratios
ranged from 0.8 to 24. Study 2:
OF concentrations of MDMA
ranged from 55 to 3533 ng/mL
and up to 7077 ng/mL after
additional self-use
In study 1 showed
similar time-course
to plasma. Analysis
by LC–MS
Samyn et al. [31] Four subjects (age 30–40) tested with
single oral dose of flunitrazepam
1 mg Spitting Cmax FLU 0.57 and 2.4 ng/mL
at 2 and 4.5 h in two subjects,
corresponding 7-AF 0.58 and
0.94 ng/mL at 2 and 4.5 h.
FLU detectable to at least 6 h.
Drug unstable, required 2%
NaF for stability
Analysis by negative
ion CI–GC–MS,
LOD FLU 0.05 ng/mL,
7-AF 0.1 ng/mL
Rohrig and
Moore [25]
Consumption of (a) three bagels
and (b) one bagel and ab lib
poppy seeds for 1 h
Unknown Epitope—1 mL (a) No morphine or codeine
detected at 1 h, LOD 3 ng per
device, (b) peak morphine at
15 min (130–205 ng/mL)
and was above 40 ng/mL
to about 1 h
Schepers et
al. [16]
Eight volunteers (four males age
26–40 years) received
(+)-methamphetamine sustained
release tablets
(a) 10 mg and (b) 20 mg Salivette cotton swab
with and without citric
acid
(a) Cmax MA 106 � 101
ng/mL (range 25–313) at 5 h,
Cmax AM 9 � 3 ng/mL, (b)
Cmax MA 192 � 121 ng/mL
(range 75–322) at 4.7 h,
Cmax AM 14 � 6 ng/mL.
Mean OF level was two
times plasma concentration,
95% range 2.3–4.3, neutral
collection gave 1.9 times
level than with citric acid
Analysis by SPE and
GC–MS, LOD
2.5 ng/mL
O.H
.D
rum
mer
/Fo
rensic
Scien
ceIn
terna
tion
al
15
0(2
00
5)
13
3–
14
21
38
Table 1 (Continued )
Reference Study detail Estimated dose Collection process and volume THC oral fluid data Comments
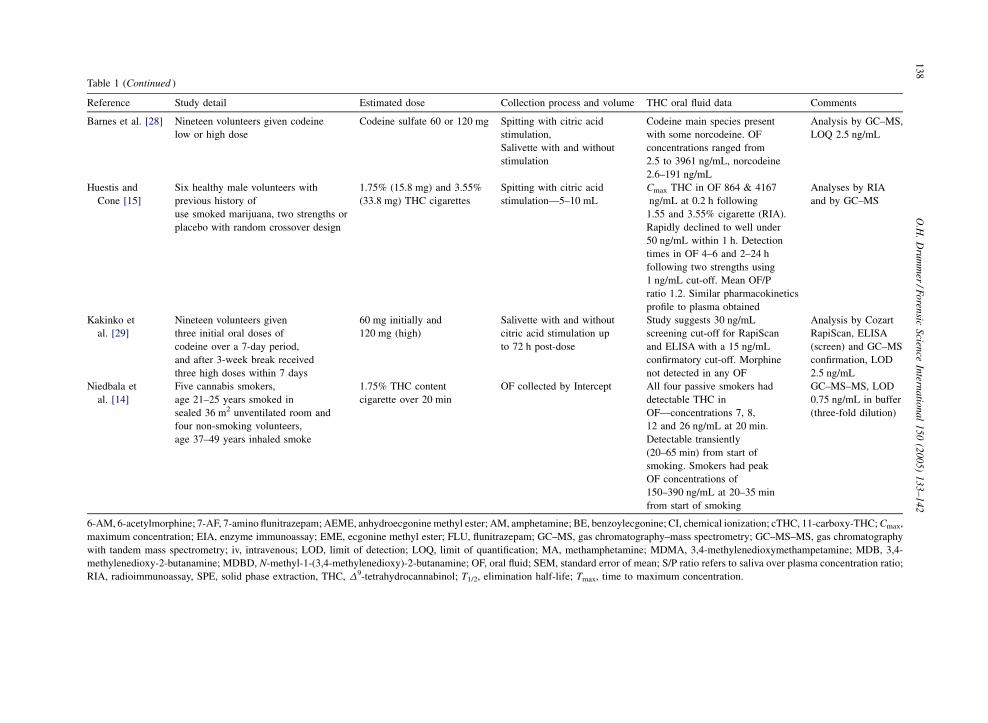
Barnes et al. [28] Nineteen volunteers given codeine
low or high dose
Codeine sulfate 60 or 120 mg Spitting with citric acid
stimulation,
Salivette with and without
stimulation
Codeine main species present
with some norcodeine. OF
concentrations ranged from
2.5 to 3961 ng/mL, norcodeine
2.6–191 ng/mL
Analysis by GC–MS,
LOQ 2.5 ng/mL
Huestis and
Cone [15]
Six healthy male volunteers with
previous history of
use smoked marijuana, two strengths or
placebo with random crossover design
1.75% (15.8 mg) and 3.55%
(33.8 mg) THC cigarettes
Spitting with citric acid
stimulation—5–10 mL
Cmax THC in OF 864 & 4167
ng/mL at 0.2 h following
1.55 and 3.55% cigarette (RIA).
Rapidly declined to well under
50 ng/mL within 1 h. Detection
times in OF 4–6 and 2–24 h
following two strengths using
1 ng/mL cut-off. Mean OF/P
ratio 1.2. Similar pharmacokinetics
profile to plasma obtained
Analyses by RIA
and by GC–MS
Kakinko et
al. [29]
Nineteen volunteers given
three initial oral doses of
codeine over a 7-day period,
and after 3-week break received
three high doses within 7 days
60 mg initially and
120 mg (high)
Salivette with and without
citric acid stimulation up
to 72 h post-dose
Study suggests 30 ng/mL
screening cut-off for RapiScan
and ELISA with a 15 ng/mL
confirmatory cut-off. Morphine
not detected in any OF
Analysis by Cozart
RapiScan, ELISA
(screen) and GC–MS
confirmation, LOD
2.5 ng/mL
Niedbala et
al. [14]
Five cannabis smokers,
age 21–25 years smoked in
sealed 36 m2 unventilated room and
four non-smoking volunteers,
age 37–49 years inhaled smoke
1.75% THC content
cigarette over 20 min
OF collected by Intercept All four passive smokers had
detectable THC in
OF—concentrations 7, 8,
12 and 26 ng/mL at 20 min.
Detectable transiently
(20–65 min) from start of
smoking. Smokers had peak
OF concentrations of
150–390 ng/mL at 20–35 min
from start of smoking
GC–MS–MS, LOD
0.75 ng/mL in buffer
(three-fold dilution)
6-AM, 6-acetylmorphine; 7-AF, 7-amino flunitrazepam; AEME, anhydroecgonine methyl ester; AM, amphetamine; BE, benzoylecgonine; CI, chemical ionization; cTHC, 11-carboxy-THC; Cmax,
maximum concentration; EIA, enzyme immunoassay; EME, ecgonine methyl ester; FLU, flunitrazepam; GC–MS, gas chromatography–mass spectrometry; GC–MS–MS, gas chromatography
with tandem mass spectrometry; iv, intravenous; LOD, limit of detection; LOQ, limit of quantification; MA, methamphetamine; MDMA, 3,4-methylenedioxymethampetamine; MDB, 3,4-
methylenedioxy-2-butanamine; MDBD, N-methyl-1-(3,4-methylenedioxy)-2-butanamine; OF, oral fluid; SEM, standard error of mean; S/P ratio refers to saliva over plasma concentration ratio;
RIA, radioimmunoassay, SPE, solid phase extraction, THC, D9-tetrahydrocannabinol; T1/2, elimination half-life; Tmax, time to maximum concentration.
O.H. Drummer / Forensic Science International 150 (2005) 133–142 139
and drugs’’ in ‘‘oral fluid’’ or ‘‘saliva’’ for each of the
relevant drug types and through Science Direct (Elsevier).
For abbreviation for terms, see table legend of Table 1.
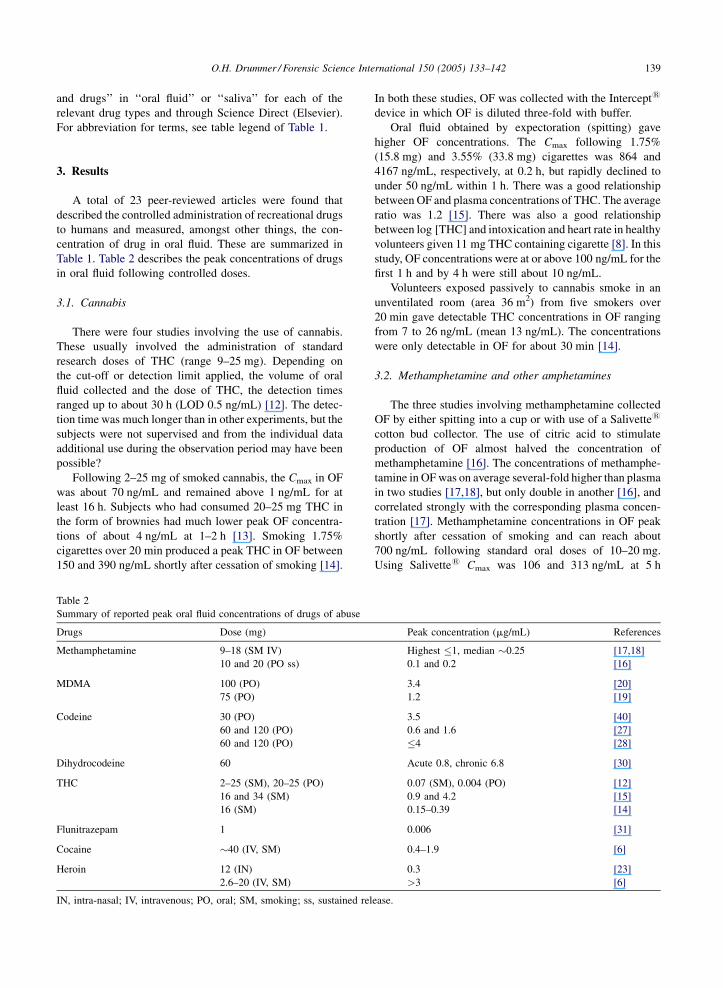
3. Results
A total of 23 peer-reviewed articles were found that
described the controlled administration of recreational drugs
to humans and measured, amongst other things, the con-
centration of drug in oral fluid. These are summarized in
Table 1. Table 2 describes the peak concentrations of drugs
in oral fluid following controlled doses.
3.1. Cannabis
There were four studies involving the use of cannabis.
These usually involved the administration of standard
research doses of THC (range 9–25 mg). Depending on
the cut-off or detection limit applied, the volume of oral
fluid collected and the dose of THC, the detection times
ranged up to about 30 h (LOD 0.5 ng/mL) [12]. The detec-
tion time was much longer than in other experiments, but the
subjects were not supervised and from the individual data
additional use during the observation period may have been
possible?
Following 2–25 mg of smoked cannabis, the Cmax in OF
was about 70 ng/mL and remained above 1 ng/mL for at
least 16 h. Subjects who had consumed 20–25 mg THC in
the form of brownies had much lower peak OF concentra-
tions of about 4 ng/mL at 1–2 h [13]. Smoking 1.75%
cigarettes over 20 min produced a peak THC in OF between
150 and 390 ng/mL shortly after cessation of smoking [14].
Table 2
Summary of reported peak oral fluid concentrations of drugs of abuse
Drugs Dose (mg)
Methamphetamine 9–18 (SM IV)
10 and 20 (PO ss)
MDMA 100 (PO)
75 (PO)
Codeine 30 (PO)
60 and 120 (PO)
60 and 120 (PO)
Dihydrocodeine 60
THC 2–25 (SM), 20–25 (PO)
16 and 34 (SM)
16 (SM)
Flunitrazepam 1
Cocaine �40 (IV, SM)
Heroin 12 (IN)
2.6–20 (IV, SM)
IN, intra-nasal; IV, intravenous; PO, oral; SM, smoking; ss, sustained rel
In both these studies, OF was collected with the Intercept1
device in which OF is diluted three-fold with buffer.
Oral fluid obtained by expectoration (spitting) gave
higher OF concentrations. The Cmax following 1.75%
(15.8 mg) and 3.55% (33.8 mg) cigarettes was 864 and
4167 ng/mL, respectively, at 0.2 h, but rapidly declined to
under 50 ng/mL within 1 h. There was a good relationship
between OF and plasma concentrations of THC. The average
ratio was 1.2 [15]. There was also a good relationship
between log [THC] and intoxication and heart rate in healthy
volunteers given 11 mg THC containing cigarette [8]. In this
study, OF concentrations were at or above 100 ng/mL for the
first 1 h and by 4 h were still about 10 ng/mL.
Volunteers exposed passively to cannabis smoke in an
unventilated room (area 36 m2) from five smokers over
20 min gave detectable THC concentrations in OF ranging
from 7 to 26 ng/mL (mean 13 ng/mL). The concentrations
were only detectable in OF for about 30 min [14].
3.2. Methamphetamine and other amphetamines
The three studies involving methamphetamine collected
OF by either spitting into a cup or with use of a Salivette1
cotton bud collector. The use of citric acid to stimulate
production of OF almost halved the concentration of
methamphetamine [16]. The concentrations of methamphe-
tamine in OF was on average several-fold higher than plasma
in two studies [17,18], but only double in another [16], and
correlated strongly with the corresponding plasma concen-
tration [17]. Methamphetamine concentrations in OF peak
shortly after cessation of smoking and can reach about
700 ng/mL following standard oral doses of 10–20 mg.
Using Salivette1 Cmax was 106 and 313 ng/mL at 5 h
Peak concentration (mg/mL) References
Highest �1, median �0.25 [17,18]
0.1 and 0.2 [16]
3.4 [20]
1.2 [19]
3.5 [40]
0.6 and 1.6 [27]
�4 [28]
Acute 0.8, chronic 6.8 [30]
0.07 (SM), 0.004 (PO) [12]
0.9 and 4.2 [15]
0.15–0.39 [14]
0.006 [31]
0.4–1.9 [6]
0.3 [23]
>3 [6]
ease.

O.H. Drummer / Forensic Science International 150 (2005) 133–142140
following 10 and 20 mg doses of sustained release metham-
phetamine, respectively [16]. The half-life in OF was about
11 h on average [18].
Amphetamine was not always detected in OF following
administration of methamphetamine [16,18]. When present,
concentrations were about one-tenth that of methampheta-
mine [16].
There were three studies involving the administration of
designer amphetamines. Two MDMA studies showed OF
(direct expectoration) to plasma concentration ratios of
0.8–24 [19] with an average of about 7 in the post-absorption
phase [20]. Following 75 and 100 mg oral doses, Cmax was
about 1.2 and 3 mg/mL at 1–2 h [19,20]. Drug was detectable
to about 24 h using a cut-off of 50 ng/mL. When subjects were
allowed to freely use MDMA at a declared rate (25–95 mg)
OF concentrations ranged from 55 to over 3500 ng/mL, and
with additional recreational use to over 7 mg/mL. The time-
course to plasma concentration was very similar [19].
A single dose of MDBD to one volunteer gave a Cmax of
1 mg/mL at 2 h and was detectable to 17 h with a LOD of 2 ng/
mL. BDB was also detected in small concentrations [21].
3.3. Cocaine
Four studies investigated the formation and disappearance
of cocaine and metabolites in oral fluid. Cocaine was readily
detectable in OF, but concentrations were about five-fold
higher in unstimulated versus citric acid stimulated collection
[4]. Citric acid does stabilize cocaine from loss [5]. Both BE
and EME were detectable in OF after smoking or intravenous
administration [5]. The OF to plasma ratio is about 3 [5].
Self-reported users of cocaine (0.1–2 g daily) had OF
concentrations of cocaine, BE and EME of 31, 54 and 69 ng/
mL, respectively, at an average time of 17 h since last dose
and a longer terminal elimination half-life (7.9 h) than in
plasma [22]. Forty milligrams smoked cocaine gave Cmax
0.4–1.9 mg/mL within minutes of smoking. Detection time
in OF (citric acid stimulation) using a LOD 1 ng/mL was
about 8 h [6].
3.4. Opiates
Limited studies are available for heroin. Heroin is
detected within minutes in OF following nasal insufflation
(snorting). In an early experiment on one volunteer, a 12 mg
dose gave a peak heroin concentration of 0.3 mg/mL and was
detectable for about 1 h at a 1 ng/mL LOD. 6-AM and
morphine were rapidly found in OF peaking at about 60
and 25 ng/mL at 10 and 60 min, respectively [23]. Two
subjects given 2.6–10.5 mg smoked gave Cmax of heroin
greater than 3 mg/mL, but was less than 10 ng/mL beyond
60–120 min. Intravenous heroin gave lower Cmax up to
30 ng/mL after 3–12 mg doses. Mean OF:plasma ratio
was about 1 [6].
Intramuscular (IM) morphine sulfate at doses of 10 and
20 mg gave a Cmax of 11 and 38 ng/mL in two subjects,
respectively, using a stimulated collection process [24]. At
24 h concentrations were barely detectable.
Consumption of poppy seeds from bagels either gave no
detectable morphine or it was up to about 0.2 mg/mL for a
short time (�1 h). Morphine concentrations were about
40 ng/mL at 1 h. [25].
Codeine presence in OF has been studied in five studies.
The administration of 30 mg liquid codeine phosphate to five
volunteers gave a Cmax of 3.5 mg/mL at 0.25 h. At 6 h
concentration had rapidly declined to 38 ng/mL. The con-
centration was dependent on the manner of collection;
stimulated OF reduced concentrations by up to a factor of
three [26].
IM administration of 60 and 120 mg codeine phosphate
produced a maximum OF concentration of 184 and 308 ng/
mL in two subjects, respectively, using a stimulated collec-
tion process. [24]. By 24 h, OF concentrations were detect-
able but were quite low.
Similarly, oral administration of 60 and 120 mg codeine
sulfate gave Cmax 0.6 and 1.6 mg/mL, respectively, at
between 1/2 and 4 h. The average OF:plasma ratio was 4
[27]. Similarly, 60 and 120 mg codeine sulfate produced OF
concentrations ranging up to 4 mg/mL. Norcodeine was also
detected in small amounts in OF [28]. Screening and con-
firmation cut-off of 30 and 15 ng/mL have been proposed
based on another study on volunteers given 60 and 120 mg
codeine [29].
Dihydrocodeine 60 mg single dose gave a peak OF
concentration of 0.8 mg/mL at 2 h and a OF:plasma con-
centration ratio of 1.3–17 [30]. Following chronic use of 0.4
to 2.6 g daily OF concentrations in 20 subjects ranged up to
66 mg/mL (mean: 10.8 � 14.9 mg/mL). Dihydrocodeine
was detectable until about 24 h after last use using a limit
of detection of 5 ng/mL. Two subjects gave no detectable
dihydrocodeine in OF and plasma suggesting non-compli-
ance [30].
3.5. Benzodiazepines
Only one study has examined the presence of benzodia-
zepines in OF. This involved administration of 1 mg fluni-
trazepam to four subjects. Cmax of flunitrazepam and 7-
aminometabolite ranged from 0.6 to 4 ng/mL and from 0.9 to
2 ng/mL at 1–4.5 h. NaF preservative was required to reduce
conversion to the 7-amino metabolite [31]. Several other
studies were performed earlier and are discussed in the
review by Kidwell et al. [10].
4. Discussion
A review of the literature over the last 15 years has shown
a number of pharmacokinetic studies aimed at examining the
presence of drugs of abuse in oral fluid. Most of these studies
have been aimed at the amphetamines, cannabis, cocaine and
the opiate class of drugs.

O.H. Drummer / Forensic Science International 150 (2005) 133–142 141
Collectively they show that with the possible exception
of benzodiazepines, these drugs of abuse are readily detect-
able in oral fluid and can show similar pharmacokinetics to
plasma. This relationship to plasma is important if oral fluid
is to be used as a surrogate to plasma, particularly in
situations, where invasive collection procedures are too
difficult, i.e. at the roadside for drug-using drivers. This
relationship is perhaps not surprising since there is a known
relationship between OF and plasma concentrations depend-
ing on the pH of the two specimens, the degree of protein
binding in plasma and the pKa of the drug [32]. For basic
drugs such as the amphetamines OF concentrations are much
higher than the corresponding plasma concentration
[16,17,19,20]. This increases the detectability of this class
of drugs. In contrast, there is very little partitioning of THC
between plasma and OF due to the high lipophilicity of the
drug, yet similarity in time profiles occurs. This is due
possibly to reserves of THC deposited in the oral mucosa
that is leached out with time [8,15].
The process of collection of oral fluid can lead to
alterations in the drug concentration. All studies that have
compared collection processes have shown that stimulated
saliva (citric acid) reduces the concentration of drug
[4,16,26]. Deceases can amount to two to three-fold for
codeine [26], methamphetamine [16] or even five-fold for
cocaine [4]. These changes are due to a dilution effect by the
increased output of oral fluids as well as a possible pH effect.
This suggests that collecting oral fluid from drivers unable to
provide a quick specimen may not disadvantage them in
terms of increasing the detectability of drug in this specimen.
With the exception of flunitrazepam, peak concentrations
of drugs in OF easily exceed 100 ng/mL, and many are
above 1 mg/mL (codeine, dihydrocodeine, heroin, cocaine,
MDMA). The longer half-life amphetamines will remain
high for some period due to their slow elimination from the
body, whereas THC, cocaine and heroin remain at relatively
high concentrations for a short period of time (see Tables 1
and 2). Chronic use will lead to an accumulation of drug in
OF. This is typified by dihydrocodeine in which OF con-
centrations rise over 10-fold with repeated use [30].
In uncontrolled situations OF concentrations tend to be
similar to or higher than the controlled dose studies. Drug-
users observed to be impaired have shown amphetamine
concentrations in OF range up to12 mg/mL (median 2.7,
n = 12). MDMA was also detected in nine volunteers, six of
whom were also positive for amphetamine. The MDMA
concentration range in OF was 0.4–6.3 mg/mL (median
1.8 mg/mL). There were 11 cases positive to THC in OF
with a concentration range of 1.4–42 ng/mL (median 10 ng/
mL). There were five cases positive to morphine in OF. The
concentration range was 0.09–8 mg/mL (median 0.9 mg/mL)
[33].
Oral fluid taken from impaired drivers gave median THC
concentrations of 6.4 ng/mL (n = 91, greater than 2 ng/mL
cut-off). Amphetamines were detected in 74 drivers at
concentrations greater than the cut-off (50 ng/mL). The
median MDMA and MDEA concentrations were 97 and
315 ng/mL, respectively. Benzoylecgonine was detected in
21 cases greater than the applied cut-off giving a median
concentration of 148 ng/mL. Twenty cases had morphine
detected at greater than the applied cut-off with a median of
32 ng/mL [34].
In OF specimens collected in workplaces using the
Intercept1 collector drugs of abuse were detected in
5.06%. THC prevalence was 3.2% (cut-off 1.5 ng/mL),
cocaine 1.1% (6 ng/mL as BE), opiates 0.23% (30 ng/mL)
and methamphetamine/amphetamine 0.47% (120 ng/mL).
The THC positives were predominately (61%) in the �4–
49.9 ng/mL, although 8.8% were over 50 ng/mL. Ninety-
three percent of the methamphetamine positives were
�160 ng/mL [35,36].
A number of factors may affect the clearance of drugs in
plasma. This includes diseases of the heart, renal and liver
disease, obesity, etc. [37,38]. Similarly, concomitant drug-
use can affect clearance through a competition of binding
sites or through metabolic pathways, or even in persons with
a high degree of fitness [39]. How these factors will affect
drug concentration in OF will need to be established as well
as methods designed to adulterate or change the concentra-
tion of drug in OF.
This review shows that there are a number of studies that
have examined the concentration of selected drugs of abuse
in OF. While this provides much useful information more
studies are required, particularly for some of the other
abused drugs and in situations, where the pharmacokinetics
may be altered by either concomitant drug-use or disease
states.
References
[1] A. Verstraete, Oral fluid testing for driving under the influence
of drugs: history, recent progress and remaining challenges,
Forensic Sci. Int. 150 (2-3) (2005) 143–150.
[2] J.M. Walsh, R. Flegel, D.J. Crouch, L. Cangianelli, J. Baudys,
An evaluation of rapid point-of-collection oral fluid drug-
testing devices, J. Anal. Toxicol. 27 (7) (2003) 429–439.
[3] W. Schramm, P.A. Craig, R.H. Smith, G.E. Berger, Cocaine
and benzoylecgonine in saliva, serum and urine, Clin. Chem.
39 (1993) 481–487.
[4] K. Kato, M. Hillsgrove, L. Weinhold, D.A. Gorelick, W.D.
Darwin, E.J. Cone, Cocaine and metabolite excretion in saliva
under stimulated and nonstimulated conditions, J. Anal. Tox-
icol. 17 (6) (1993) 338–341.
[5] E.J. Cone, M. Hillsgrove, W.D. Darwin, Simultaneous mea-
surement of cocaine, cocaethylene, their metabolites, and
‘‘crack’’ pyrolysis products by gas chromatography-mass
spectrometry, Clin. Chem. 40 (7 Pt 1) (1994) 1299–1305.
[6] A.J. Jenkins, J.M. Oyler, E.J. Cone, Comparison of heroin and
cocaine concentrations in saliva with concentrations in blood
and plasma, J. Anal. Toxicol. 19 (6) (1995) 359–374.
[7] P. Kintz, V. Cirimele, B. Ludes, Detection of cannabis in oral
fluid (saliva) and forehead wipes (sweat) from impaired dri-
vers, J. Anal. Toxicol. 24 (7) (2000) 557–561.
O.H. Drummer / Forensic Science International 150 (2005) 133–142142
[8] D.B. Menkes, R.C. Howard, G.F. Spears, E.R. Cairns, Salivary
THC following cannabis smoking correlates with subjective
intoxication and heart rate, Psychopharmacology (Berl) 103
(2) (1991) 277–279.
[9] W. Schramm, R.H. Smith, P.A. Craig, D.A. Kidwell, Drugs of
abuse in saliva: a review, J. Anal. Toxicol. 16 (1) (1992)
1–9.
[10] D.A. Kidwell, J.C. Holland, S. Athanaselis, Testing for drugs
of abuse in saliva and sweat, J. Chromatogr. B Biomed. Sci.
Appl. 713 (1) (1998) 111–135.
[11] E.J. Cone, Saliva testing for drugs of abuse, Ann. N. Y. Acad.
Sci. 694 (1993) 91–127.
[12] R.S. Niedbala, K.W. Kardos, D.F. Fritch, S. Kardos, T. Fries, J.
Waga, et al. Detection of marijuana use by oral fluid and urine
analysis following single-dose administration of smoked and
oral marijuana, J. Anal. Toxicol. 25 (5) (2001) 289–303.
[13] R.S. Niedbala, H. Feindt, K. Kardos, T. Vail, J. Burton, B.
Bielska, et al. Detection of analytes by immunoassay using up-
converting phosphor technology, Anal. Biochem. 293 (1)
(2001) 22–30.
[14] R.S. Niedbala, K. Kardos, S. Salamone, D. Fritch, M. Brons-
geest, E.J. Cone, Passive cannabis smoke exposure and oral
fluid testing, J. Anal. Toxicol. 28 (2004) 546–552.
[15] M.A. Huestis, E.J. Cone, Relationship of delta-9-tetrahydro-
cannabinol concentrations in oral fluid and plasma after con-
trolled administration of smoked cannabis, J. Anal. Toxicol. 28
(2004) 394–399.
[16] R.J. Schepers, J.M. Oyler, R.E. Joseph Jr., E.J. Cone, E.T.
Moolchan, M.A. Huestis, Methamphetamine and ampheta-
mine pharmacokinetics in oral fluid and plasma after con-
trolled oral methamphetamine administration to human
volunteers, Clin. Chem. 49 (1) (2003) 121–132.
[17] C.E. Cook, A.R. Jeffcoat, B.M. Sadler, J.M. Hill, R.D. Voyks-
ner, D.E. Pugh, et al. Pharmacokinetics of oral methamphe-
tamine and effects of repeated daily dosing in humans, Drug
Metab. Dispos. 20 (6) (1992) 856–862.
[18] C.E. Cook, A.R. Jeffcoat, J.M. Hill, D.E. Pugh, P.K. Patetta,
B.M. Sadler, et al. Pharmacokinetics of methamphetamine
self-administered to human subjects by smoking S-(+)-
methamphetamine hydrochloride, Drug Metab. Dispos. 21
(4) (1993) 717–723.
[19] N. Samyn, G. De Boeck, M. Wood, C.T. Lamers, D. De Waard,
K.A. Brookhuis, et al. Plasma, oral fluid and sweat wipe
ecstasy concentrations in controlled and real life conditions,
Forensic Sci. Int. 128 (1–2) (2002) 90–97.
[20] M. Navarro, S. Pichini, M. Farre, J. Ortuno, P.N. Roset, J.
Segura, et al. Usefulness of saliva for measurement of 3,4-
methylenedioxymethamphetamine and its metabolites: corre-
lation with plasma drug concentrations and effect of salivary
pH, Clin. Chem. 47 (10) (2001) 1788–1795.
[21] P. Kintz, Excretion of MBDB and BDB in urine, saliva, and
sweat following single oral administration, J. Anal. Toxicol. 21
(7) (1997) 570–575.
[22] E.T. Moolchan, E.J. Cone, A. Wstadik, M.A. Huestis, K.L.
Preston, Cocaine and metabolite elimination patterns in
chronic cocaine users during cessation: plasma and saliva
analysis, J. Anal. Toxicol. 24 (7) (2000) 458–466.
[23] W.L. Wang, W.D. Darwin, E.J. Cone, Simultaneous assay of
cocaine, heroin and metabolites in hair, plasma, saliva and
urine by gas chromatography–mass spectrometry, J. Chroma-
togr. B Biomed. Appl. 660 (2) (1994) 279–290.
[24] E.J. Cone, Testing human hair for drugs of abuse. I. Individual
dose and time profiles of morphine and codeine in plasma,
saliva, urine, and beard compared to drug-induced effects on
pupils and behavior, J. Anal. Toxicol. 14 (1) (1990) 1–7.
[25] T.P. Rohrig, C. Moore, The determination of morphine in urine
and oral fluid following ingestion of poppy seeds, J. Anal.
Toxicol. 27 (7) (2003) 449–452.
[26] C.L. O’Neal, D.J. Crouch, D.E. Rollins, A.A. Fatah, The
effects of collection methods on oral fluid codeine concentra-
tions, J. Anal. Toxicol. 24 (7) (2000) 536–542.
[27] I. Kim, A.J. Barnes, J.M. Oyler, R. Schepers, R.E. Joseph Jr.,
E.J. Cone, et al. Plasma and oral fluid pharmacokinetics and
pharmacodynamics after oral codeine administration, Clin.
Chem. 48 (9) (2002) 1486–1496.
[28] A.J. Barnes, I. Kim, R. Schepers, E.T. Moolchan, L. Wilson, G.
Cooper, et al. Sensitivity, specificity, and efficiency in detect-
ing opiates in oral fluid with the Cozart Opiate Microplate EIA
and GC–MS following controlled codeine administration, J.
Anal. Toxicol. 27 (7) (2003) 402–407.
[29] S.L. Kacinko, A.J. Barnes, I. Kim, E.T. Moolchan, L. Wilson,
G.A. Cooper, et al. Performance characteristics of the Cozart(R)
RapiScan Oral Fluid Drug Testing System for opiates in com-
parison to ELISA and GC/MS following controlled codeine
administration, Forensic Sci. Int. 141 (1) (2004) 41–48.
[30] G. Skopp, L. Potsch, K. Klinder, B. Richter, R. Aderjan, R.
Mattern, Saliva testing after single and chronic administration
of dihydrocodeine, Int. J. Legal Med. 114 (3) (2001) 133–140.
[31] N. Samyn, G. De Boeck, V. Cirimele, A. Verstraete, P. Kintz,
Detection of flunitrazepam and 7-aminoflunitrazepam in oral
fluid after controlled administration of Rohypnol, J. Anal.
Toxicol. 26 (4) (2002) 211–215.
[32] N. Samyn, A. Verstraete, C. van Haeren, P. Kintz, Analysis of
drugs of abuse in saliva, Forensic Sci. Rev. 11 (1999) 1–19.
[33] N. Samyn, C. van Haeren, On-site testing of saliva and sweat
with Drugwipe and determination of concentrations of drugs of
abuse in saliva, plasma and urine of suspected users, Int. J.
Legal Med. 113 (3) (2000) 150–154.
[34] N. Samyn, G. De Boeck, A.G. Verstraete, The use of oral fluid
and sweat wipes for the detection of drugs of abuse in drivers,
J. Forensic Sci. 47 (6) (2002) 1380–1387.
[35] E.J. Cone, L. Presley, M. Lehrer, W. Seiter, M. Smith, K.W.
Kardos, et al. Oral fluid testing for drugs of abuse: positive
prevalence rates by Intercept immunoassay screening and GC–
MS–MS confirmation and suggested cut-off concentrations, J.
Anal. Toxicol. 26 (8) (2002) 541–546.
[36] A.G. Verstraete, Detection times of drugs of abuse in blood,
urine, and oral fluid, Ther. Drug Monit. 26 (2) (2004) 200–205.
[37] G. Cheymol, Effects of obesity on pharmacokinetics implica-
tions for drug therapy, Clin. Pharmacokinet. 39 (3) (2000) 215–
231.
[38] D.J. Morgan, A.J. McLean, Clinical pharmacokinetic and
pharmacodynamic considerations in patients with liver dis-
ease. An update, Clin. Pharmacokinet. 29 (5) (1995) 370–391.
[39] A.M. Persky, N.D. Eddington, H. Derendorf, A review of the
effects of chronic exercise and physical fitness level on resting
pharmacokinetics, Int. J. Clin. Pharmacol. Ther. 41 (11) (2003)
504–516.
[40] C.L. O’Neal, D.J. Crouch, D.E. Rollins, A. Fatah, M.L. Che-
ever, Correlation of saliva codeine concentrations with plasma
concentrations after oral codeine administration, J. Anal.
Toxicol. 23 (6) (1999) 452–459.










![Clinical Pharmacokinetics-II [dosing of drugs, tdm]](https://static.cupdf.com/doc/110x72/5563b643d8b42a38198b4e8b/clinical-pharmacokinetics-ii-dosing-of-drugs-tdm.jpg)













![DRUGS AND PREVENTION OF ILLICIT TRAFFIC IN DRUGS … · 1 ___ chapter 95 ___ the drugs and prevention of illicit traffic in drugs act [principal legislation] arrangement of sections](https://static.cupdf.com/doc/110x72/5b491f7d7f8b9af54b8d363c/drugs-and-prevention-of-illicit-traffic-in-drugs-1-chapter-95-the-drugs.jpg)





