Remove the Mystery from
12 Lead EKG Interpretation for Acute MI
The simple, rapid “12 lead solution” to 12 lead confusion!
A 12 Lead Program for ALL health care professionals!
Copyright Apex Innovations 2003

The Basics…..Let’s do the re-view
Coronary Anatomy
Conduction
Paper and rate basics
Rhythm
Lead placement
Vectors and axis
R wave progression

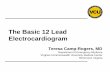
Coronary Anatomy
Right CoronaryArtery (RCA)
Aorta
Circumflex (Cx)
Left AnteriorDecending (LAD)

Conduction:
Normal P-QRS-T Constant, Continuous Conduction….the beat goes
onP wave
Depolarization & contraction of
both atria
QRS..
Ventricular
depolarization
T wave…
Ventricular
repolarization
Iso-electric Line

Conduction:
Normal P-QRS-T Constant, Continuous Conduction….the beat goes
on
Q-First down slope
R-Upward slope
S-Down slope
Iso-electric Line

Normal P-QRS-T
P Wave PR Interval QRS Complex ST Segment
Represents Atrial depolarization
Time between onset of atrial depolarization and onset of ventricular depolarization (AV conduction time)
Ventricular depolarization
Interval between ventricular
depolarization and repolarization
Duration < 0.12 seconds
0.12 - 0.20 seconds 0.04 - 0.10 seconds Measure from end of QRS to J-point, the
beginning of T wave
Height < 2.5 mm Measure start of P wave to start of QRS
Q- First negative deflection R- First positive deflectionS- Negative deflection after R wave
Shape Smooth Prolonged indicates a conduction block
Shortened indicates accelerated conduction or junctional in origin
In relation to iso-electric line:Depression/
Negative indicates ischemia
Elevation/Positive indicates injury
Orientation Positive in Leads I,II,aVF,
V4Negative in
aVR

Cardiac Conduction System
LeftBundleBranch
Purkinjefibers
RightBundle Branch
Bundle of His
AV node
Internodalpathways
Sinus node

Cardiac Conduction System
Relationship of ECG to anatomy

One Small Block = .04 Seconds
Standard paper speed = 25mm per secondNote calibration on side of EKG - 2 Large
Blocks tall
One Large Block = .20 Seconds
-Increased paper speed makes complexes wider-Decreased paper speed makes the complexes
narrower
Rate: EKG Paper Basics
One small Block = 1mm Voltage
One Large Block = 5mm Voltage

Rate: Calculation Options
1. RATE = # of R waves in a 6 second strip X 10
2. RATE = 300 # large squares between R waves
3. RATE Count = Count from a QRS complex on any bold line to the next QRS complex. Count “300, 150, 100, 75, 60, 50” for each bold line after first complex.
300 150 100 75 60 50
Start End
Rate = 82 BPM

Rhythms
• Normal Sinus
• Sinus Bradycardia
• Sinus Tachycardia
• Sinus Arrhythmia
• Sick Sinus Syndrome
• Wandering Atrial Pacemaker
• Sinus Block
• Sinus Arrest
Sinus (SA Node)

Rhythms Continued
• Premature Atrial Contraction (PAC)
• Paroxysmal Atrial Tachycardia (PAT)
• Multifocal Atrial Tachycardia
• Atrial Flutter
• Atrial Fibrillation
Atrial Rhythms

Rhythms Continued
• Premature Junctional Contraction (PJC)
• Paroxysmal Junctional Tachycardia (PJT)
• Junctional Flutter
• Junctional Fibrillation
Junctional (AV)

Rhythms Continued
• Premature Ventricular Contraction (PVC)
- Bigeminy Trigeminy, Quadrageminy
• Paroxysmal Ventricular Tachycardia (PVT)
• Multifocal Ventricular Tachycardia
• Ventricular Flutter
• Ventricular Fibrillation
Ventricular

Rhythms Continued
• 1 Prolonged PRI
• 2 Type I - Wenchebach
• 2 Type II - Mobitz II
- 2:1, 3:1 Conduction
• 3 Complete Heart Block
• Bundle Branch
- Right BB
- Left BB
AV Blocks

The 12 Lead EKG…
6 Limb Leads 6 Chest or Pre-cordial Leads
IIIIII
AVRAVLAVF
V1V2V3
V4V5V6
12 angles or pictures
of the electrical activity of the heart

Looking and Learning: Vectors and Axis ~the hard way~
A panoramic view
of the heart’s
electrical activity from
12 different angles
The sum of all vectors determines the axis

Lead Placement - Lead I, II, III
RA LA
LL
+-LEAD I Bipolar Limb Lead• Looks from Right to Left Shoulder
• Looks at high lateral wall of
left ventricle
• Supplied by circumflex artery–CX
• Positive/upright P QRS T

Lead Placement - Lead I, II, III
RA LA
LL
+-
LEAD II Bipolar Limb Lead• Looks from R Shoulder to Left Leg• Looks at inferior wall of left ventricle
• Supplied by right coronary artery–RCA
• Positive/upright P QRS T
+
-

Lead Placement - Lead I, II, III
RA LA
LL
+-
+
-
LEAD III Bipolar Limb Lead• Looks from Left Shoulder to Left Leg• Looks at inferior wall of left ventricle • Supplied by right coronary artery-RCA• A biphasic QRS complex is expected
-
+

Augmented Limb Leads
LA RA
LL
+ +
+
AVR Augmented Voltage Right Arm • All complex waves are negative• Typically, this lead not used for diagnosing!
AVL Augmented Voltage Left Arm • Looks at lateral wall of left ventricle • Supplied by circumflex artery - CX• All complexes should be positive
AVF Augmented Voltage (left) Foot • Cross between Leads I and II • Looks at inferior wall of left ventricle • Supplied by right coronary artery-RCA• All complexes should be positive

Lead Placement – V-Leads
V1-V2 = Septal
V3-V4 = Anterior
V5-V6 = Lateral
V1-V3 = Posterior
V1 – 4th ICS, right of sternum
V2 – 4th ICS, left of sternum
V3 – Midpoint between V2 and V4
V4 – 5th ICS, mid-clavicular line
V5 – Level with V4 , anterior to axillary line
V6 – Level with V4, mid-axillary line

V-Lead R Wave Progression
- V1 - R wave is generally smallest or most negative
- V4 - R wave is typically the tallest or most positive
- Lack of R wave progression may mean :
Pathology- Disease state, CAD, Septal wall MI
Normal- A patient with Congenital state, Rotated heart, Obesity, COPD
Other- Breast tissue, poor lead placement
The progression or increasing in R wave amplitude from
negative to positive in leads V1 to V4 is expected and
normal!

R Wave Progression in the V Leads
V1 – PQRST All negative
V2 – PQRST Should be mostly negative but
start progression
V3 – PQRST Biphasic with upright T waves
V4 – PQRST Nearly completely upright
V5 – PQRST Upright
V6 – PQRST Upright

Myocardial Infarction
Ischemia
Injury
Recognition
Criteria
Infarct Location Template
AMI Evolution
Practice EKG’s
Bumps, elevations and tombstones…

Myocardial Infarction
Occurs when a coronary artery is narrowed and occludes, terminating the blood and oxygen supply. This results in
cardiac hypoxia and irritability which may cause fatal arrhythmias. Without a blood supply to the cardiac muscle, depolarization cannot happen and renders the muscle, electrically dead.
An EKG can diagnose AMI location, identify the culprit artery and reveal any blocks in
ventricular conduction.

ST Depression = Ischemia
• Inverted T waves, sometimes peaked
• T wave deflection is opposite from QRS (Normally T wave is upright when QRS is upright and vice versa)
• T wave inversion is usually in same leads that demonstrates signs of acute infarction
(Q waves, ST elevation)

Causes for ST depression
• Ischemia• Digoxin Toxicity• Pulmonary Embolism• Ventricular Hypertrophy• Left Bundle Branch
Block

ST Elevation = Current Injury
• Depicts current myocardial injury
• Measure J-point to beginning of ventricular repolarization
• May be elevated >1mm in limb leads and >2mm in precordial leads
• Will see reciprocal ST depression in other leads

Causes for ST elevation
• Pericarditis• Ventricular aneurysm• Drug induced• Myocardial Infarction

Recognition of AMI
• Know what to look for:– ST elevation >1 mm– 3 contiguous leads
PR baseline
ST-segment deviation= 4.5 mm
J point

AMI Requires at least 2 of these criteria:
1. History of characteristic chest pain Crushing-pressure in chest, pain
radiation to jaw, arms, back, N/V, SOB, diaphoresis
2. Evolutionary EKG changes ST depression (ischemia) ST elevation (injury) Q wave development (muscle
death)3. Elevated cardiac enzymes Troponin, CKMB-CK, Myoglobin

Understanding infarct location
Here’s the trick!
The 12 Lead Solution
to
12 Lead Confusion!

Simple - Rapid!!
Finally…….
Remove the mystery!Location, Location,
Location!

AMI Location Correlation
aVF InferiorIII Inferior V3 Anterior V6 Lateral
aVL LateralII Inferior V2 Septal V5 Lateral
aVRI Lateral V1 Septal V4 Anterior

Lateral Lead ST Elevation in AMI
LEAD I AVL V5 V6
Lateral: Usually supplied by Circumflex (CX)Look for reciprocal changes in Lead V1
“High Lateral” Wall

Normal EKG
Lateral
Lateral Lateral
Lateral
ReciprocalChange

Inferior Lead ST Elevation in AMI
LEAD II AVFLEAD III
Inferior: Usually supplied by Right Coronary Artery (RCA)Look for reciprocal changes in Leads I, AVL

Normal EKG
Inferior
Inferior
Inferior
Reciprocal Change
Reciprocal Change

Septal Lead ST Elevation in AMI
V1 V2
Septal: Usually supplied by Left Anterior Descending (LAD)Look for reciprocal changes in Leads V3, AVF

Normal EKG
Septal
Septal
Reciprocal Change
Reciprocal Change

Anterior Lead ST Elevation in AMI
V3 V4
Usually supplied by Left Anterior Descending (LAD)Look for reciprocal changes in Leads V2, AVF

Normal EKG
Anterior
Anterior
Reciprocal Change
Reciprocal Change

12 Lead-Paper Heart
To better understand rhythm location:
1. Hold left upper corner and right lower corner of EKG2. Roll EKG to note: inferior leads at apex lateral leads on sides anterior and septal leads in front

• Height is 1/3 the size of entire QRS complex• Width is at least one square or 0.04 seconds in duration • Q waves in V1,V2,V3 or V4 indicate anterior or antero- septal infarction• Damage from old infarcts cause Q waves that last a lifetime • Abnormal if thick on tracing• Q wave may be normal in AVR
Significant Q Wave Characteristics

ST segment Evolution and Q wave development with AMI
A

Differentiating Between Acute and Old MI
• Q wave with no other morphology = old MI
• Q wave and ST segment elevation (with or without T wave inversion) = AMI
• Q wave and inverted T wave = age undetermined

Evolutional Changes of an Acute Myocardial Infarction

Identify infarct location using a systematic
approach Rhythm
ST Depression
ST Elevation
R Wave Progression
Q Waves

Let’s take a look at…
the Good, the Bad and
the Ugly!
~EKG Review~

Review #1 What Does This 12-Lead ECG Show?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
INFERIOR
INFERIOR INFERIOR

Review #2 What Does This 12-Lead ECG Show?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
LATERAL ANTERIOR
LATERAL LATERAL
ANTERIOR LATERAL

Review #3 What Does This 12-Lead ECG Show?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
LATERAL ANTERIOR
LATERAL LATERAL
ANTERIOR LATERAL

Appearances and History are Important!
Your patient, a 58 y/o male, was diagnosed with cancer 2 weeks ago and was scheduled to receive his first chemotherapy treatment this morning. Instead, he was delivered in a wheelchair hurriedly (by his oncologist), to the emergency department in distress. He presents complaining of intense chest pain described as a “10”, is very restless, nauseated, diaphoretic and pale. You order the usual cardiac work-up. Here is what his EKG showed…

Review #4 What Does This 12-Lead ECG Show?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL

Later that day…
This patient’s cardiac workup returned within normal limits and was
diagnosed with anxiety and released to begin his chemotherapy.

Review #5 What Does This 12-Lead ECG Show?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
LATERAL ANTERIOR
LATERAL LATERAL
ANTERIOR LATERAL

Review #6 What Does This 12-Lead ECG Show?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
INFERIOR LATERAL
INFERIOR INFERIOR LATERAL

Review #7 What Does This 12-Lead ECG Show?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
LATERAL ANTERIOR
LATERAL LATERAL
ANTERIOR LATERAL

Appearances and History are Important!
Your patient, a 62 year old male pharmacist, presents at 6:00AM with chest pressure radiating to his neck, jaw and left arm. He is mildly short of breath and says he’s had indigestion all night. You order the usual cardiac work-up. Here is what his EKG showed…

Review #8 What Does This 12-Lead ECG
Show?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
LATERAL SEPTAL ANTERIOR
LATERAL SEPTAL LATERAL
ANTERIOR LATERAL

Later that day…
The Inferolateral/Anteroseptal MI
caused massive injury and tissue death,
and the patient subsequently died.

Review #9 What Does This 12-Lead ECG Show?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
INFERIOR
INFERIOR INFERIOR

Review #10 What Does This 12-Lead ECG Show?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
SEPTAL
SEPTAL

Posterior MI’s can be tricky!
EKG changes are seen in V1-V3 (the anterior precordial leads)
and are a mirror image of an anteroseptal MI
Posterior MI HINT: R waves in V1 and V2?Suspect Posterior MI!
You will see:Increased R wave amplitude and duration
R wave is more prominent than S wave in V1 and V2ST depression and large inverted T waves V1-V3

Review #11 What Does This 12-Lead ECG Show?
LATERAL SEPTAL? ANTERIOR
INFERIOR LATERAL SEPTAL? LATERAL
INFERIOR INFERIOR ANTERIOR? LATERAL
POSTERIOR
POSTERIOR
POSTERIOR

LATERAL SEPTAL? ANTERIOR
INFERIOR LATERAL SEPTAL? LATERAL
INFERIOR INFERIOR ANTERIOR? LATERAL
POSTERIOR
INFERIOR POSTERIOR
INFERIOR INFERIOR POSTERIOR
Review #12 What Does This 12-Lead ECG Show? Look at those R waves!!!

~~ Time is Muscle! ~~
Tick-Tock

~Test Time~
Please stop here!1.Answer the Self Assessment
Sheet’s
first 8 questions.
2. Next proceed to the remaining
slides and record the infarct location
for each EKG on the self assessment.

Quiz #1 Where is the elevation or infarct?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
INFERIOR
INFERIOR INFERIOR

Quiz #2 Where is the elevation or infarct?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
SEPTAL ANTERIOR
SEPTAL
ANTERIOR

Quiz #3 Where is the elevation or infarct?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
LATERAL
LATERAL LATERAL
LATERAL

LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
SEPTAL ANTERIOR
SEPTAL
ANTERIOR
Quiz #4 Where is the elevation or infarct?

Quiz #5 Where is the elevation or infarct?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
LATERAL ANTERIOR
LATERAL LATERAL
ANTERIOR LATERAL

Quiz #6 Where is the elevation or infarct?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
SEPTAL ANTERIOR
SEPTAL
ANTERIOR

Quiz #7 Where is the elevation or infarct?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
INFERIOR LATERAL
INFERIOR INFERIOR LATERAL

Quiz #8 Where is the elevation or
infarct?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
LATERAL SEPTAL ANTERIOR
LATERAL SEPTAL LATERAL
ANTERIOR LATERAL

Quiz #9 Where is the elevation or
infarct?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
SEPTAL
SEPTAL

Quiz #10 Where is the elevation or infarct?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
LATERAL ANTERIOR
INFERIOR LATERAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL

Quiz #11 Where is the elevation or infarct?
LATERAL SEPTAL ANTERIOR
INFERIOR LATERAL SEPTAL LATERAL
INFERIOR INFERIOR ANTERIOR LATERAL
SEPTAL ANTERIOR
SEPTAL
ANTERIOR

Thank you for your participation!
Please complete the program and speaker evaluation.
Copyright Apex Innovations 2003