




Coarctation of the AortaTrisomy 21
Clinical Case Presentation Presented by: Lynette Barnhart RNC, BSN, SNNP
June 9, 2014
University of Texas Medical Branch at GalvestonNNP Concepts and Practicum II
GNRS 5632
Dr. Debra Armentrout PhD, RN, MSN, NNP-BCDr. Leigh Ann Cates PhD, APRN, NNP-BC,RRT-NPS,CHSE

ObjectivesMaternal HistoryMaternal and Fetal Risks and ComplicationsDelivery and StabilizationAdmission exam and diagnosticsPrimary admission diagnoses Etiology and Pathophysiology of Primary Admission Diagnoses Initial Plan of CareHospital Course by Symptoms Medications Pertinent Theories and Evidence Based Practice Family Interactions Discharge Plan and Follow Up

Maternal History37 yo, married HispanicG6 now P5
1 SAB1994-39 weeks1997-40 weeks2004-39 weeks2009-39 weeks
EDD 6/10/14A+, GBS-, RPR NR, Rubella Immune, HIV NR, HB-Unremarkable Medical historyDenies alcohol, tobacco, and illicit drug use

Maternal & Fetal Risks & Complications
Advanced maternal age37 year old
U/S 12/16/14Nuchal thickness of 3.1
Low AFP 12/31/14+ Trisomy 21
U/S 2/28/14Suspected Coarctation of the aorta
Delivery & StabilizationScheduled induction at 39 weeks
Due to suspected Coarctation of the aortaSpontaneous labor
38 1/7 weeks GASROM 2 ½ hours prior to delivery
Clear fluidVertex presentationNSVDNo maternal medications prior to deliveryApgars
8 at 1 minute8 at 5 minutes
Delivery summaryLusty cry at delivery, cord clamped and cut. Infant taken to radiant warmer. Dried and stimulated. Infant dusky, BBO2 (40%) provided at 5 minutes of life for pre-ductal saturations below 85%. Continued to dry and stimulate. Improvement in color and saturations noted. O2 discontinued at 8 minutes of life. Infant placed skin to skin with mother prior to transfer to NICU for transition.

Admission Assessment Gestational age
38 1/7 weeksMeasurements
Birth weight: 3078gms (10th-50th %tile)Length: 48.5 cm (10th-50th %tile)OFC: 32 cm (10th %tile)
Vital signsTemperature 36.9 CHeart rate 120 bpmRespiratory rate 40 br/minPre-ductal SpO2 94%Post-ductal SpO2 89%
Admission Assessment Physical Exam
General: Habitus of Trisomy 21, No acute distress, active with exam, sucking on pacifierEye: Normal conjunctiva, bilateral red reflexes.HENT: Normocephalic, nares patent, oral mucosa moist with intact palate, anterior fontanelle soft and flat, ears normally set and rotated, flat facial profile.Respiratory: Unlabored respirations with appropriate chest excursion, lung sounds clear and equal bilaterally.Cardiovascular: Heart rate and rhythm regular without murmur, pulses equal in all four extremities, capillary refill less than 3 seconds, pink with acrocyanosis to hands and feet.Gastrointestinal: Soft, non-tender, non distended with active bowel sounds, no organomegaly, 3 vessel umbilical cord, anus appears patent.Genitourinary: Normal male genitalia for age/gestation, testes descended, void at deliveryLymphatic: Fat pad to nape of neckMusculoskeletal: Moves all extremities, no hip clicks, normal Barlow’s and Ortolani’s. Simian creases to both hands, wide gap between first and second toes.Integumentary: Warm, dry, pink, without rashNeurologic: Alert, moves all extremities appropriately.

Admission Diagnostics
Echocardiogram5/28/2014- 1 hour of life
FISH chromosomes5/29/2014- results pending
High resolution chromosomes5/29/2014- results pending
Bedside chemstrip51 @ 1426 (admit)
Primary Admission Diagnoses
38.1 week AGA male infant, 3078gmsSuspected Coarctation of the aortaSuspected Trisomy 21
Etiology and Pathophysiology of Coarctation of the Aorta
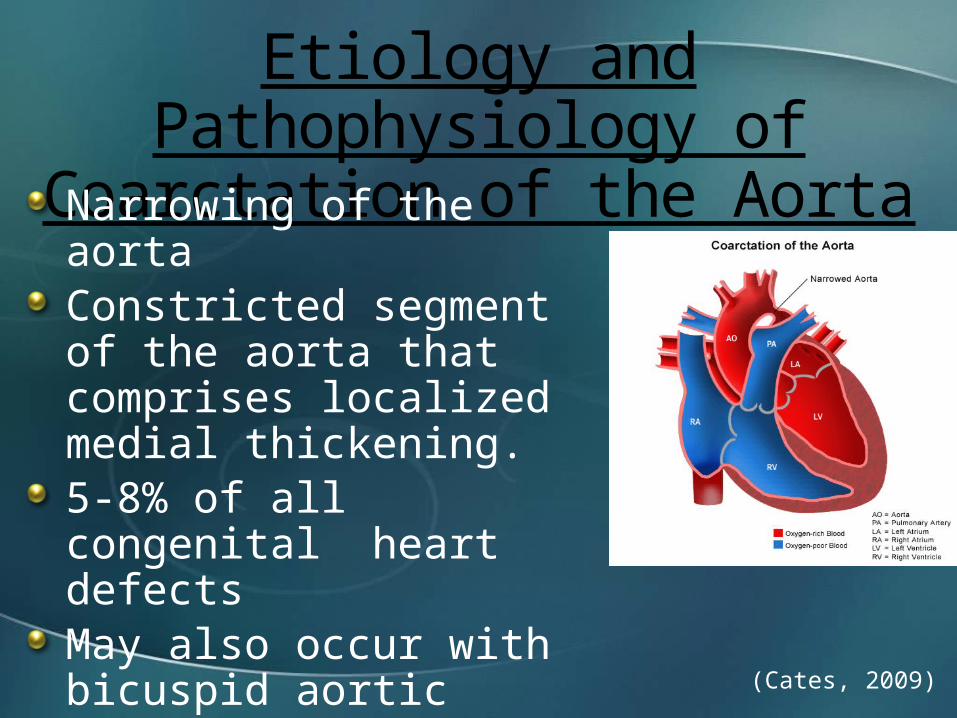
Narrowing of the aortaConstricted segment of the aorta that comprises localized medial thickening.5-8% of all congenital heart defectsMay also occur with bicuspid aortic valve and VSD
(Cates, 2009)

Coarctation of the Aorta
Increased afterload on the left ventricleIncreased wall stress resulting in ventricular hypertrophyAs the PDA closes (may cause rapid CHF and shock)
Causes increased left ventricular pressures, increased left atrial pressure, and opening of the foramen ovale
Resulting in left-to-right shunting and dilation of the right atrium and right ventricle
When the foramen ovale doesn’t open the pulmonary venous and artery pressures increase
Resulting in right ventricular dilation
(Gholampour, et al., 2006)
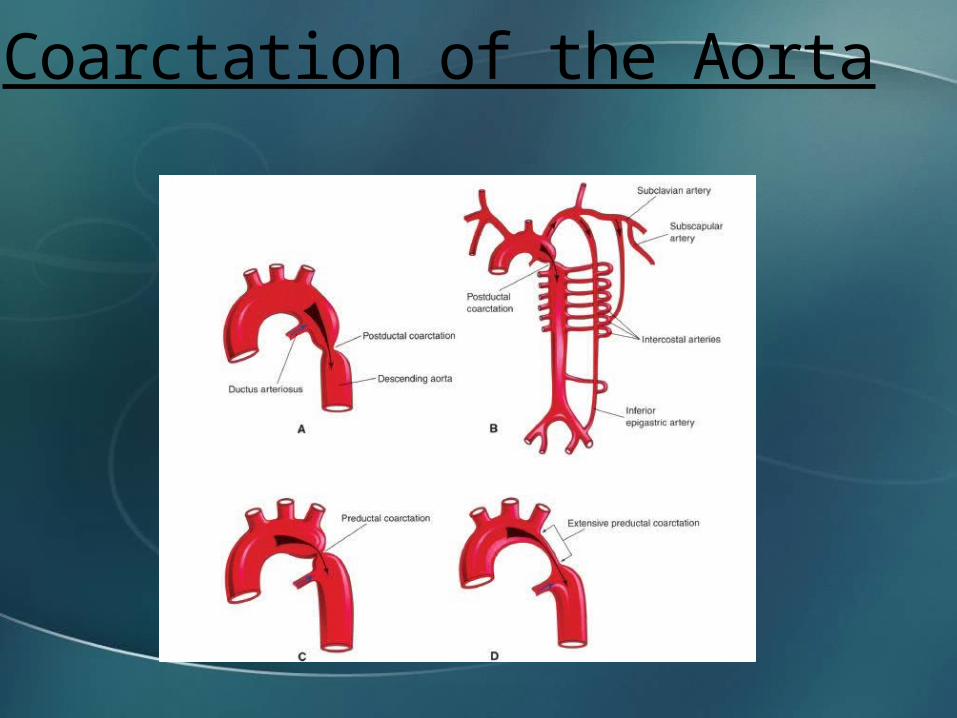
Coarctation of the Aorta

Coarctation of the AortaClinical findings
Systolic ejection murmur that radiates to the apex and is often loudest in the backXray finidngs
Generalized cardiomegaly with normal pulmonary vascular density (Pre-ductal Coarctation)Enlarges left ventricle and left atrium and dilated ascending aorta (Post-ductal Coarctation)
Pre-ductal and post-ductal SpO2 saturation discrepancy Upper and lower extremity BP discrepancyAbsent or decreased lower extremity pulsesTachypneaLethargyPoor feedingShockCyanotic lower extremities (Gomella, 2013)
(Syamasundar, 2012)

Coarctation of the AortaMedical Treatment
Prostaglandin E 0.05-0.15 mcg/kg/min
Ventilatory assistanceTo support increased work of breathing
Inotropic drugsDopamine, Dobutamine, Epinepherine
DiureticsUsed for infants with CHF
Foley CatheterStrict monitoring of urine output and renal perfusion
UACABGs
(Cates, 2009)
Coarctation of the AortaSurgical Treatment
Goal is to bypass the narrowed section of the aorta
Left subclavian aortoplastyResection and end-to-end anastomosisAngioplasty with Dacron patchStentingBalloon angioplasty
(Gholampour, et al, 2004).
Trisomy 21Down SyndromePresence of an extra 21st chromosomeMost common of all multiple congenital anomaly (MCA) syndromesOccurs in ~ 1 in 650 birthsNeonatal mortality is related to severe cardiac anomalies Maternal nondisjunction
Occurring in the first meiotic division accounts for ~65% of casesOccurring in the second meiotic division accounts for ~23% of cases
(Blackburn, 2007)(Gomella, 2013)
Trisomy 211st trimester screening
Ultrasound between 10 4/7 and 13 4/7 weeks gestationMeasurement of the nuchal translucency (increased in Trisomy 21)Detects 70% of Trisomy 21
2nd trimester screeningSerum screening between 15 and 20 6/7 weeks gestation
Alpha fetoprotein (AFP), hCG, and unconjugated estriol (Triple Screen)Alpha fetoprotein (AFP), hCG, unconjugated estriol, and inhibin-A (Quad screen) results in 80% detectionDecreased AFP, increased hCG, decreased PAPP-A, and increased Inhibin A
(Bajaj & Gross, 2011)

Trisomy 21Physical findings
Hypotonia, poor or absent moro reflex, flat facial profile, protruding tongue, up slanting palperbral fissures, Brushfield spots, anomalous auricles, joint hyperextensibility, excess nuchal skin, fifth-digit brachydactyly/clinodactyly, and single transverse palmar crease.
Associated AnomaliesCongenital heart defects in 40% of infants (most common ASD or VSD), PDA, endocardial cushion defect, aberrant subclavian artery.Hirschsprung disease, duodenal or esphageal atresia, imperforate anus, hearing loss (66%), mental deficiency, and renal and urinary tract anomalies. (Gomella, 2013)
(Jones, 2006)

Trisomy 21
TreatmentThere is no cure for Down’s syndromeSupportive care
Early intervention is essential to assist in the progression of developmental milestones.
(Heyn & Perlstein, 2014)
Initial Plan of CareAdmit to NICU, place on continuous cardio/resp monitoringDaily weight, OFC and Length Q SundayErythromycin ointment to eyes bilaterally within 1 hour of birthVitamin K 1mg IM x1 within 1 hour of birthPlace PIV Infuse D10W at 10cc/hr (80ml/kg/day)Strict Intake and OutputCardiac ECHO stat to evaluate fetal diagnosis of suspected Coarctation of the AortaPre and post-ductal SpO2 monitoringObtain 4 point Blood pressures
Initial Plan of CareChemstick on admission and then per policyObtain Metabolic Screen at 24-48 hoursObtain Metabolic screen #2 at 5-10 days of ageMay breast feed ad lib on demandSocial service consult

Hospital Course by Systems
Respiratory: Mild respiratory insufficiency
At 3 hours of life infant noted to have frequent desaturations (75-85%) Nasal Cannula started at 1 L @ 21%
Discontinued on DOL 1 (24 hours after start)Intermittent nasal stuffiness without increase work of breathing
On DOL 4 Treated with little noses Q 4 hours x 24 hours with some improvementNo further intervention required
Discharged on room air on DOL 6Pre and post ductal saturation monitoring continued until dischargeRespiratory rate 23-77 during stay

Hospital Course by Systems
Cardiovascular: Suspected Coarctation of the Aorta
Hemodynamically stable without murmur. Peripheral pulses equal x 4DOL 0 @ 1 hour of life ECHO obtained
Study limited by technical limitations. Atrial level shunt, quantitatively normal biventricular size and systolic function. Ventricular level shunting cannot be excluded. Greater than ½ systemic right ventricular systolic pressures. Tapering of the transverse aorta without evidence of discrete narrowing or stenosis; coarctation cannot be excluded in the presence of a ductus.
DOL 1 Pre ductal sats 94-99% Post ductal sats 94-97%Left upper extremity BP 81/45 (58)Left lower extremity BP 70/41 (51)Heart rate 108-138 bpm

Hospital Course by SystemsCardiovascular continued
DOL 2 repeat ECHOSmall superior atrial level communication with left-to-right flow. Mild to moderate right heart enlargement as well as right ventricular hypertrophy with normal right ventricular systolic function. Structurally normal-appearing mitral valve with mild mitral regurgitation. Normal left ventricular size and systolic function in the presence of flattened interventricular septal wall motion. Moderate sized patent ductus arteriosus with bidirectional flow. This is a left arch with a common brachiocephalic trunk as the first arch vessel. The transverse aortic arch is diffusely narrowed measuring approximately 3.5mmfor a Z-score of negative 2.5. There is mildly turbulent color low through the transverse aortic arch and there is a peak gradient of 8mmHg in the descending aorta. There does not appear to be a further discrete narrowing of the aortic isthmus. However, cannot completely rule out coarctation in the presence of a PDA. Normal left coronary artery origin. Right coronary artery origin not well visualized. Systemic to supersystemic RV pressure by septal position, TR jet, and PDA flow.
DOL 6Discharge home with parents. Follow up with Cardiologist in 1-2 weeks.
Hospital Course by SystemsFEN/GI:
DOL 0PIV with D10W @ 80ml/kg/day
DOL 1PIV continues @ 80ml/kg/dayBF or Similac Advance 20 Infant directed Q 2-4 hours
DOL 2PIV at 117ml/kg/dayBF or Similac Advance 20 15cc Q 3 hours Nipple or gavage
DOL 3PIV at 125ml/kg/dayBF of Similac Advance 20 15cc Q 3 hours
DOL 4PIV D10W with lytes at 125ml/kg/dayBF/EBM/Similac Advance 20 Ad lib minimum 15cc Q 3 hours
DOL 5Discontinue PIVBF/EBM/Similac Advance 20 Ad lib Q 2-4 hours
Hospital Course by SystemsHeme
Physiologic Jaundice of the newbornMother A+, ABS negativeInfant blood type unknown
At 49 hours-Transcutaneous Bilirubin 12.4DOL 3 - Total Bilirubin 12.8, Direct 0.2
Bili blanket startedDOL 5 - Bili blanket discontinued DOL 6 - Transcutaneous Bilirubin 10.5

Hospital Course by SystemsNeuro
Suspected Trisomy 21 (Intrauterine Diagnosis)DOL 1 –FISH probe sent
Confirmed Trisomy 21 DOL 5DOL 1- High resolution chromosomes sent
Pending results at discharge on DOL 6Discharge
Information given on Sharing Down Syndrome AZ
Infectious DiseaseNo issues. Mom GBS -, ROM at delivery
Medications
Vitamin K IM injection, 1 mg x 1 within 1 hour of birthErythromycin ophthalmic eye ointment to both eyes x 1 within 1 hour of birthD10W @ 10cc/hr (80ml/kg/day)Hepatitis B vaccine 5mcg IM x 1 Little noses Q 4 hours x 24 hours
Pertinent Theories and EBPCOARCTATION OF THE AORTA
Until surgery can be performed PGE is needed. Surgical correction has the lowest risk of restenosis then any other treatment.Although surgical correction reduces the morbidity and mortality rate. These infant’s still have a decreased life expectancy related to poor blood pressure control.Outcome is worse when there is also a hypoplastic arch present. If the ECHO is performed by someone whom is not experienced in neonates and small children a CT or cardiac MRI should be performed to officially adequately assess the aortic arch.Surgical intervention is the preferred method of treatment because those whom have a balloon dilation will almost always need a repeat dilation and/or surgery.
(Shah, 2014)(Panzer & Dewolf, 2014)
Pertinent Theories and EBPTRISOMY 21
Currently there is no cure for Down’s syndrome. Genetic studies are focuses on finding therapies to improve learning and potential therapies.Early intervention programs, physical therapy, occupational therapy, and speech therapy can improve outcomes.At greater risk for hearing, vision, and learning deficits. Leukemia is more common with Trisomy 21 patients then those without.
(Heyn & Perlstein, 2014)

Family Interactions
Mother and father were concerned immediately after birth, questions answered and plan of care explained. Infant skin to skin with mother prior to transfer to NICU for further evaluation. Father accompanied infant to NICU and further questions answered. After recovery mother visited infant in the NICU, asked appropriate questions regarding suspected Coarctation and Trisomy 21.
Discharge Plan and Follow-upDischarge home with parents 6/3/14 DOL 6Diet: EBM/ Similac Advance 20cal/oz ad lib q 2-4 hours1st Newborn screen sent 5/29 results pending2nd Newborn screen sent 6/1 results pendingABR hearing screen passed on 6/2/14Hepatitis B Vaccine given on 6/1/14Follow up with Primary Care Physician in 2daysFollow up with Pediatric Cardiologist in 1-2 weeks

ConclusionCoarctation is a constricted segment of the aorta that comprises localized medial thickening and can be life threatening if not diagnosed and treated. A prenatal diagnosis of Coarctation of the aorta can assist the medical professionals in the preparation for treatment.Trisomy 21 is a genetic defect that may have multiple associated anomalies. Confirmation of a prenatal diagnosis is important to assist the family in the acceptance of a child with a chronic disorder and/or a genetic disorder. Although it is common for a Trisomy 21 infant to have an associated heat defect it is not commonly associated with coarctation of the aorta.
ReferencesBajaj, K & Gross, S. (2011). Genetic aspects of perinatal disease and prenatal diagnosis. In R. J. Martin, A.A. Fanaroff, & M.C. Walsh. Neonatal-Perinatal medicine: Diseases of the fetus and infant (9th edition pp.129-145). Volume 1. St. Louis, Missouri: Elsevier MosbyBlackburn, S. (2007). Maternal, Fetal, & Neonatal Physiology (3rd edition). St. Louis, Missouri: Saunders Elsevier. Cates, L.A. (2009). The basics about acyanotic heart disease (Powerpoint presentation). Gholampour, D.M., Givtaj, N., Omrani, G.H., Sadeghpour, T.A., & Yaghoobi, A. (2006) Evaluation of results of surgical correction for coarctation of aorta by suclavian flap aortoplasty (SCFA) and other methods in Rajaee Heart Center. Retrieved May 31, 2014, from, http://www.plan.sid.ir/en/ViewPaper.asp?ID=40885&vRadif=17&vWriter=GHOLAMPOUR%20DEHAKI%20M.,GIVTAJ%20NADER,OMRANI%20GH.,SADEGHPOUR%20TABAEI%20A.,YAGHOOBI%20A.&vJournal=RAZI+JOURNAL+OF+MEDICAL+SCIENCES+%28JOURNAL+OF+IRAN+UNIVERSITY+OF+MEDICAL+SCIENCES%29&vDate=Winter%202006&vVolume=12&vNo=49&vStart=0&vEnd=0Gomella, T.L. (2013) Neonatology: Management, procedures, on-call problems, diseases, and drugs (7th edition). New York: McGraw Hill Education.
ReferencesHeyn, S.N. & Perlstein, D (2014). Down Syndrom. Retrieved June 6, 2014 , from http://www.onhealth.com/down_syndrome/article.htmJones, K.L. (2006) Smith’s recognizable patterns of human malformation. (5th edition) Philadelphia, Pennyslvania: Saunders Elsevier. Panzar, J. & Dewolf, D. (2014) Hypertension after Coarctation repair. Retrieved June 6, 2014, from, http://cardiologyacademicpress.com/soap/pdf/delme_427_535c2c62225e71.97600142.pdfShah, S. N. (2014). Aortic coarctation treatment & management. Retrieved June 6, 2014, from, http://emedicine.medscape.com/article/150369-overviewSyamasundar Rao, P. (2012, February 1) Coarctation of the aorta. Medscape. Retrieved May 31, 2014 from http://emedicine.medscape.com/article/895502-overview





























