Jatinder S. Luthra
Anatomy, Radiographic evaluation &
Classification of Pelvic Ring Fractures

Pelvic Fractures: Epidemiology
Majority due to high impact blunt trauma (MVA, pedestrian vs. vehicle etc.) but also secondary to falls in frail elderly
Mortality overall = 10% Mortality 50% if open #

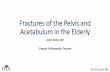
Pelvic Anatomy Pelvis = sacrum,
coccyx + 2 innominate bones
Innominate bones = ilium, ischium, pubis
Sacrum + innominate bones form a ring
Strength from ligamentous supports (largely posterior aspect of ring)

Pelvic Anatomy 5 joints: Lumbosacral Sacroiliac (x2) Sacrococcygeal Symphysis

Anterior Support:– Symphysis pubis
Fibrocartilaginous joint covered by ant & post symphyseal ligaments
– Pubic rami Posterior Support:
– ~majority of stability Iliolumbar
ligaments Sacroiliac
ligaments Sacrospinous
ligament Sacrotuberous
ligament

Vascular Anatomy Vessels lie
close to posterior pelvic walls
Venous bleeding most common (sacral plexus)
Most commonly injured arteries are superior gluteal and internal pudendal

Pelvic Anatomy Nerve supply through the pelvis
derived from lumbar and sacral plexuses
Other structures: lower GI/GU


Imaging – X- rays
X Rays Pelvis AP – part of ATLS protocol

Imaging – X- rays AP VIEW:-Identifies most fractures-Look for disruption in iliopubic and ilioischial
lines, sacral foramina, radiographic U, Shenton’s Lines
Inlet and outlet views
Judet Views

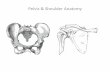
AP Pelvis Radiogram
Acetabular fracture
Posterior Pelvic lesion

S2

Imaging Look for any evidence of damage to
the posterior pelvic structures– Clues on X-rays:
L5 transverse process avulsion (iliolumbar ligament)
Ischial spine avulsion (sacrospinous ligament)
Unable to clearly make out sacral foramina Assymmetry of sacral foramina Avulsion at lower lip of lateral sacrum
(sacrotuberous ligament)

Inlet view– X-ray beam at
40o to plate directed towards feet
Sacral Promontry should overlap anterior border of S1

Posterior displacement
Rotational deformity
Subtle SI joint injury
Sacral Ala fracture

Outlet View Outlet view
– Beam aimed 30o towards head
– Superior border of symphysis at level S2

Outlet View Vertical
displacement
Sacral foramina
Flexion deformity

CT scan Detailed
information of posterior lesion
Sacral Foramina Subtle sacral
impaction. Rotation of
hemipelvis Associated Lesions Dysmorphysisum

Radiological criteria of instability

Displacement instead of impaction in posterior pelvis


Attention Stationary pelvic radiogram do not reflect true
pathology
Apparently stable patient should undergo Examination under anaesthesia
Push Pull film under anaesthesia > 1cm is unstable Contraindicated – Zone 2/3 sacral fracture Haemodynamically unstable

ArteriogramPatients with pelvic fracture – persistent bleeding despite External stabilization
ICE – intravenous contrast extravasation

-Gross haematuria-- Bloody urethral discharge-Inability to void-- swelling / echymosis in perineal region-High riding prostate

Pelvic Fractures 5 General Categories: 1. Pelvic Ring 2. Acetabular 3. Sacral 4. Avulsion type 5. Single bone

Pelvic fracture classification
Bucholz classification – JBJS 1981
Type1 - stable Type II- Open
Book
Type III – Rotaionally and vertically unstable

Pelvic fracture classification
Letournal Classification

Pelvic Ring FracturesYoung Classification System:
Differentiates fracture patterns based on mechanism of injury/direction of causative force
3 major fracture patterns: 1. lateral compression (50%) 2. antero-posterior compression
(25%) 3. vertical shear (5%)

Pelvic fracture classification Young & Burgess
Classification
Modification of tile – Based on mech of inj.

Young & Burgess Anteroposterior compression fracture
External rotation force
Neurovascular structures stretched.
Symphyseal diastasis / Vertical fracture pubic ramus

Young & Burgess Anteroposterior compression fracture - I

Young & Burgess Anteroposterior compression fracture - II

Young APC II

Young & Burgess Anteroposterior compression fracture - III


Young & Burgess LATERAL COMPRESSION - I

Young & Burgess LATERAL COMPRESSION - II
CRESCENT FRACTURE

Young & Burgess LATERAL COMPRESSION – III

Young & Burgess VERTICAL SHEAR

Tile C1/ Young VS

Young & Burgess COMBINED MECHANISM

Summary Classification system - - Assist
surgeon in determining treatment and prognosis
Young & Burgess – - Fluid resuscitation reqd - Solid organ injury Need for acute stabilization Pt. survival
APC type 3 & VS injury – highest transfusion reqd.

THANK YOU