Pediatrics ReviewEmergency
Gina Neto, MD FRCPCDivision of Emergency Medicine
Case 1• 10 yr old boy with asthma, difficulty
breathing today. Cough and runny nose for 3 days.
• T 36.5, RR 40, HR 130, O2 Sat 89%.• Suprasternal and scalene retractions,
decreased air entry, expiratory wheeze.
• Describe your management.
Asthma• Mild Asthma:• Salbutamol MDI x 3 doses prn
• Moderate Asthma:• Salbutamol MDI x 3 doses then prn• Steroids
Dexamethasone 0.15-0.3 mg/kg PO (max 12) Prednisone 1-2 mg/kg PO (max 60 mg)

Asthma• Severe Asthma:• Salbutamol via nebulization with• Ipratropium 250 mcg x 3 doses q20 min• Steroids
Dexamethasone 0.15-0.3 mg/kg PO (max 12) Prednisone 1-2 mg/kg PO (max 60 mg)

Asthma• If not improving within 60 min or signs
of impending respiratory failure:• Magnesium Sulfate 50 mg/kg/dose IV
(max 2g)• Give over 20-30 min• May cause severe hypotension• IV NS 20 bolus ml/kg
• Methylprednisolone 1-2 mg/kg IV
Case 2 • 2 mo male with 2 day hx rhinorrhea, poor
feeding and cough. Few hrs resp distress.
• RR 60 HR 120 T 37C. Pink, well hydrated.• Chest - inspiratory crackles, exp wheezes.
• Diagnosis?• Treatment?

Bronchiolitis• RSV - Respiratory Syncytial Virus most
common• Parainfluenza, Influenza A, Adenovirus,
Human metapneumovirus• Peak in winter• More serious illness• < 2 months• Hx of prematurity < 35 weeks• Congenital heart disease
Bronchiolitis• Treatment • Nebulized Epinephrine – short term relief
• ? Dexamethasone 1 mg/kg on Day 1 0.6 mg/kg for another 5 days
• ? Nebulized Hypertonic Saline

Case 3 • 2 yr old girl awoke tonight with respiratory
distress. Harsh, “barky” cough.
• HR 100 RR 28 T 37 • Mild distress. Stridor at rest.
• Diagnosis? • Treatment?

Croup• Parainfluenza most common• Hoarse voice, barky cough, stridor • Peak fall and spring• Infants and toddlers • Treatment• Dexamethasone (0.6 mg/kg)• Nebulized Epinephrine if in respiratory
distress• Consider Nebulized Budesonide

Steeple Sign

Case 4 • 18 month female with fever x 2 days.
Difficulty swallowing.
• HR130 RR28 T39C• Exam normal except won’t move neck fully.
• What diagnostic test should be performed?


Retropharyngeal Abscess• Complication of bacterial
pharyngitis
• Grp A strep, oral anaerobes and S. aureus
• Treatment• IV Clindamycin and
Cefuroxime• Consult ENT

Retropharyngeal Soft Tissues *Age (yrs) Maximum (mm)0-1 1.5 x C21-3 0.5 x C23-6 0.4 x C26-14 0.3 x C2
Age (yrs) Maximum (mm)0-1 2.0 x C51-2 1.5 x C52-3 1.2 x C53-6 1.2 x C56-14 1.2 x C5
Retrotracheal Soft Tissues *
*
*

Case 5• 5 yr old male fever x 6 hrs. Refusing to eat or
drink. Voice muffled, drooling. Not immunized.
• HR 140 RR 20 T 39.5 • Very quiet, doesn't move. • Slight noise on inspiration. • Chest clear, exam normal.


Epiglottitis• Rarely seen • Strep pneumoniae• H. influenzae uncommon
due to vaccine
• Do not disturb patient• Consult Anesthesia,
intubate • IV Cefuroxime and
Clindamycin
Case 6 • 17 mo male with sudden onset noisy and
abnormal breathing.• Was playing on floor before developing
difficulty breathing.
• VS T36.8, P200 (crying), R28 (crying), O2 sat 99%
• Mild wheezing with mild inspiratory stridor.


What investigation would you do next?

ExpiratoryCXR
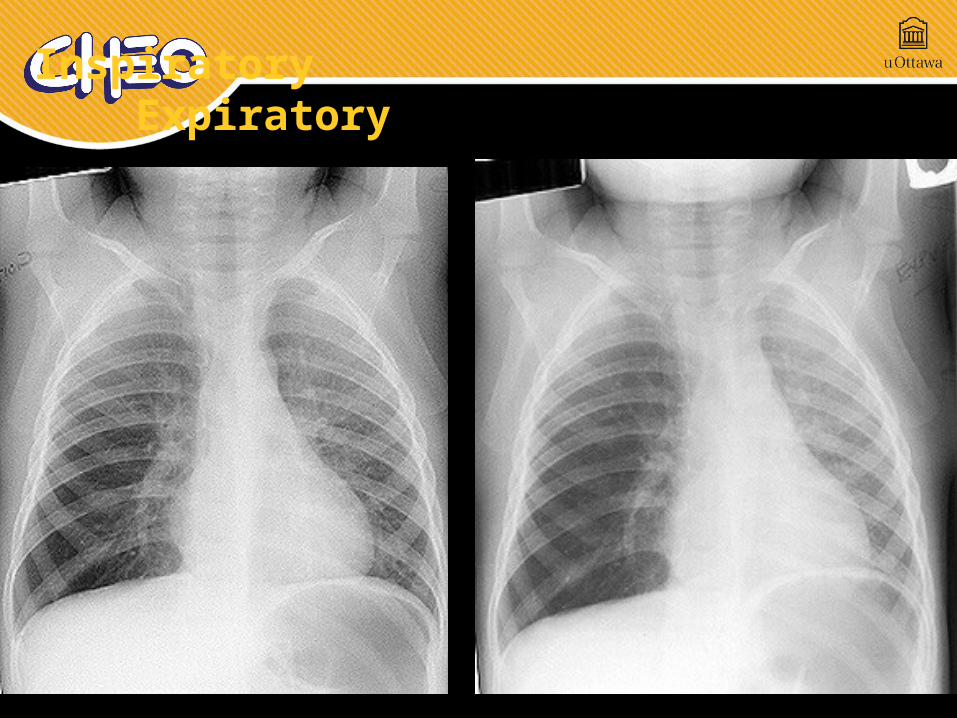
Inspiratory Expiratory
Foreign Body Aspiration
• Highest risk between 1 -3 yrs old Immature dentition, poor food control More common with food than toys
• peanuts, grapes, hard candies, sliced hot dogs
• Acute respiratory distress (resolved or ongoing)• Witnessed choking• Cough, Stridor, Wheeze, Drooling• Uncommonly…. Cyanosis and resp arrest
Case 7 • 9 month old female with fever x 2 days.
Vomiting x 20 today. Diarrhea x 10 today. Voiding scant amounts.
• HR 120 RR 36 BP 100/50 T 38.5• Cap refill 2 sec, pink, decreased skin turgor.• Font sunken, eyes sunken.• Abdo + GU normal.

Case 7• What is the degree of dehydration of this
child?• Management?
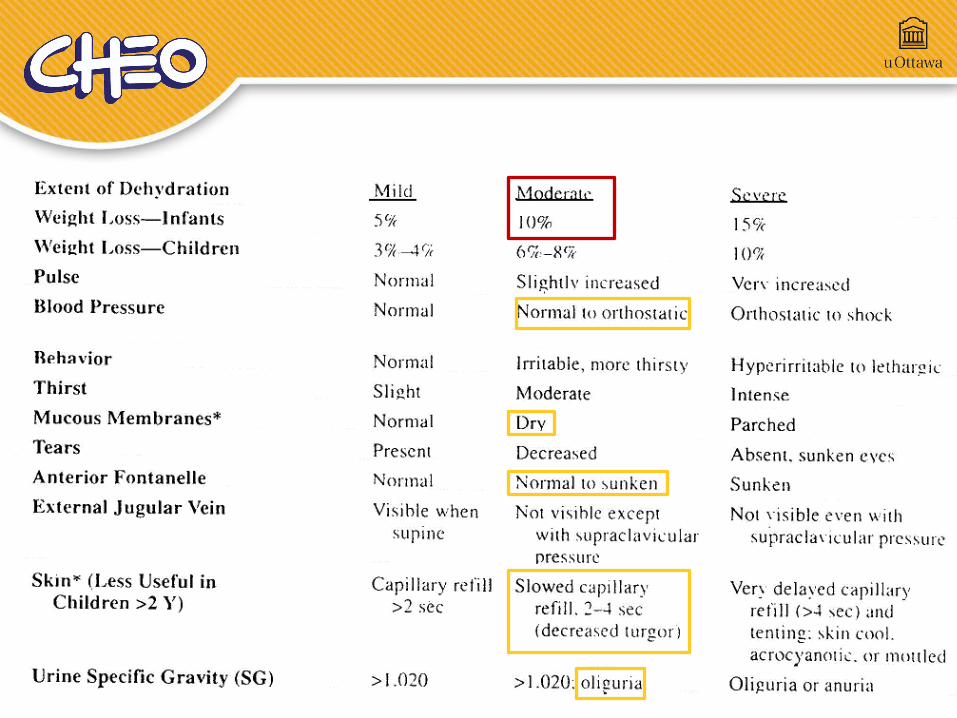
Dehydration
Gastroenteritis• ORT with rehydration solution (eg Pedialyte)• 5 ml/kg/hr divided every 5 min, continue
until appears hydrated
• Consider Ondansetron (0.15 mg/kg)
• Early refeeding (including milk) within 12 hrs
• Rule out UTI
Fluids and Electrolytes• Maintenance (D5NS)
4ml/kg/hr for first 10 kg2ml/kg/hr for second 10 kg1 ml/kg/hr for rest of weight in kg
• Deficit (NS)• If severely dehydrated give NS bolus
20 ml/kg over 15-60 min • Replace over 24 hours
First half over 8hrs, second half over 16 hrs• Ongoing Losses• Diarrhea, Vomiting, Insensible losses with fever

Case 8• 15 month old male with intermittent sudden
severe abdo pain x 24 hrs. Vomiting x 3. Diarrhea with blood and mucus.
• HR130 RR24 T37 • Tender abdomen with fullness in RUQ
• Diagnosis?• Investigations?

Intussusception• 1-3 years• Boys 2:1
• Classic Triad (10-30%)• Vomiting• Crampy abdominal pain• “Red currant jelly” stools
• Lethargy is common

Intussusception• 75% are ileo-colic• Lead point• Peyer's Patches
preceding viral infection• Meckel diverticulum• Polyps• Hematoma (Henoch Schonlein Purpura)• Lymphoma
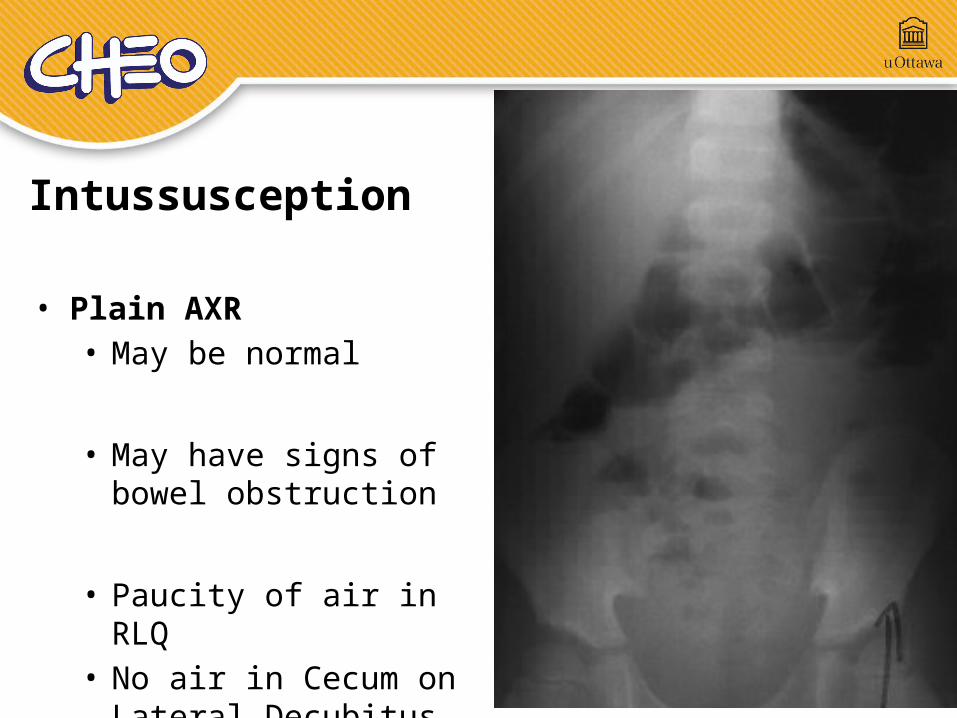
• Plain AXR• May be normal
• May have signs of bowel obstruction
• Paucity of air in RLQ • No air in Cecum on
Lateral Decubitus
Intussusception
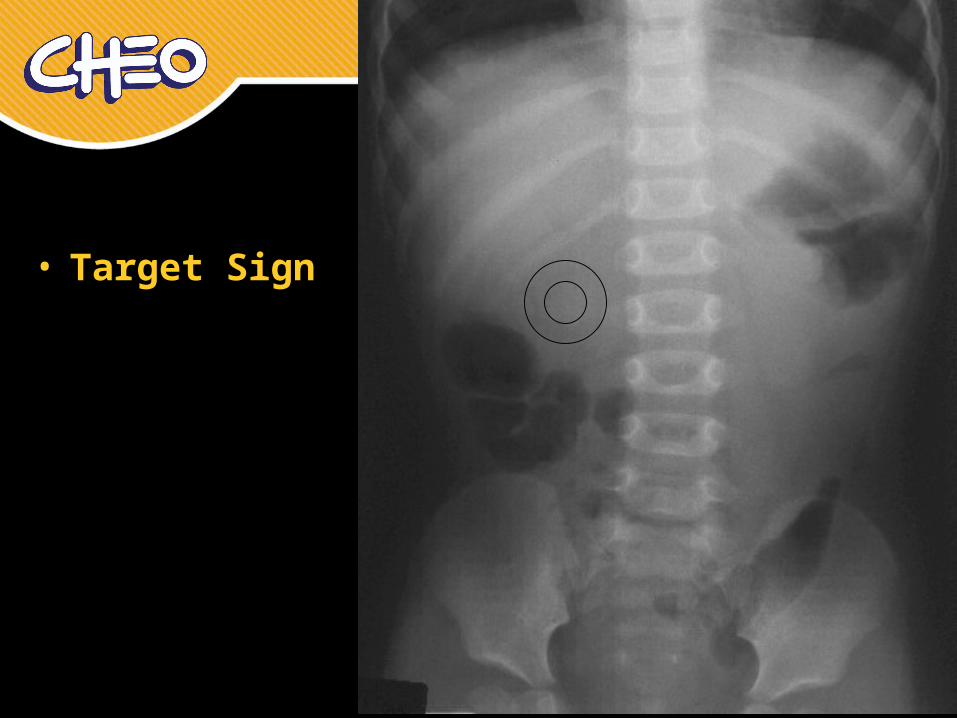
• Target Sign

• Crescent Sign

Intussusception• Air Contrast
Enema
• Success rate >80%• Recurrence 10-15%

Case 9• 4 week old boy with vomiting for past week.
Initially one emesis per day now emesis with every feed. Forceful. No bile.
• No fever. No diarrhea.
• Looks well. Mild dehydration. • Abdomen soft, non tender, BS present.
• DDx?

Case 9
• Na 140 K 3.0 Cl 90 BUN 24 CR 50
• WBC 8.5 Hgb 120 Plts 360
• Venous gas pH 7.50, PCO2 44, HCO3 30

Pyloric Stenosis• Most common surgical condition < 2 mos
• 4-6 wks of age• Ratio male to female is 4:1• Increased in first born males
• Occurs in 5% of siblings and 25% if mother was affected

Pyloric Stenosis• Nonbilious vomiting• Emesis increases in frequency and
eventually becomes projectile
• Classic findings:• Hypertrophied pylorus palpable “olive” in
epigastric area• Peristaltic waves progressing from LUQ to
the epigastrium

Pyloric Stenosis
• Laboratory abnormalities:• Hypokalemia• Hypochloremia• Metabolic alkalosis
• Ultrasound• Thickened pylorus
Case 10• 1 month old with bilious vomiting. Multiple
episodes of yellow green vomiting since this morning. Progressive lethargy and irritability.
• Looks unwell, irritable cry.• Abdomen distended.• Weak pulses, cap refill>5 sec.
• DDx? Management?
Volvulus• Twisting of a loop of bowel
around its mesenteric attachment.
• 80% present by the first month
40% present in the first week
Rarely can be seen in older children.

Volvulus• Sudden onset of bilious
vomiting in a neonate.
• Acute abdomen with shock
• May have more gradual course with episodic vomiting

Volvulus• Evidence of small
bowel obstruction • Dilated loops• Air fluid levels• Paucity of distal air

Volvulus• Upper GI series • “corkscrew”
appearance of the duodenum and jejunum

Case 11• 1 month old girl fever today. Cough and
runny nose. Slightly decreased feeding.
• Looks well, alert and interactive• T 38.9o HR 176 RR 42 BP 100/50 • Font flat, neck supple, exam non remarkable
• What is your approach to this case?

• Well appearing infants 1-3 mos are low risk for serious bacterial infection if:
Previously healthy• Born at term (> 37 weeks)• No hyperbilirubinemia• No hospitalizations • No chronic or underlying diseases
No evidence of focal bacterial infection Laboratory parameters:
• WBC count 5-15/mm3
• Urinalysis WBC count < 5/hpf• Stool WBC count < 5/hpf (if infant has diarrhea)
Low Risk Criteria “Rochester” for Febrile Infants
Case 12• 2 year old boy with generalized tonic clonic
movements. Duration 5 min.
• T 39.2o HR 110 RR 24 BP 110/60 • Awake now, normal neurological exam.• Right TM bulging, neck supple, no rash. • Past med history unremarkable.
• Approach?
Febrile Seizure• Simple Febrile Seizure• T>38.5• 6 mo-5 yr• Generalized seizure, < 15 min• One seizure within 24 hours• Neurologically normal before and after
• Occur in ~ 5% of children• Recurrence in 30%

Febrile Seizure• Risk of epilepsy is 1% • ~ same as general population
• Higher risk (2.4%) if:• Multiple febrile seizures• < 12 mos at the time of first febrile seizure• Family history of epilepsy

Seizure Management• ABC's• IV access• Seizure treatment• 1st Line - Benzodiazepines
• IV/PR Lorazepam or Diazepam• Buccal Midazolam
• 2nd Line Phenytoin, Fosphenytoin Phenobarbitol
Seizure Management• Seizure treatment• 3rd Line
Midazolam infusion Thiopental Paraldehyde Propofol
• Observe in the ED until child returns to normal
• After simple febrile seizure no neurological investigations indicated (eg CT, EEG)

Case 13• 2 yr old boy with fever for 6
days.• Red eyes but no discharge.• Generalized rash.• Erythema of the palms of
hands and soles of feet.• Red, swollen lips.• Enlarged cervical lymph
nodes.
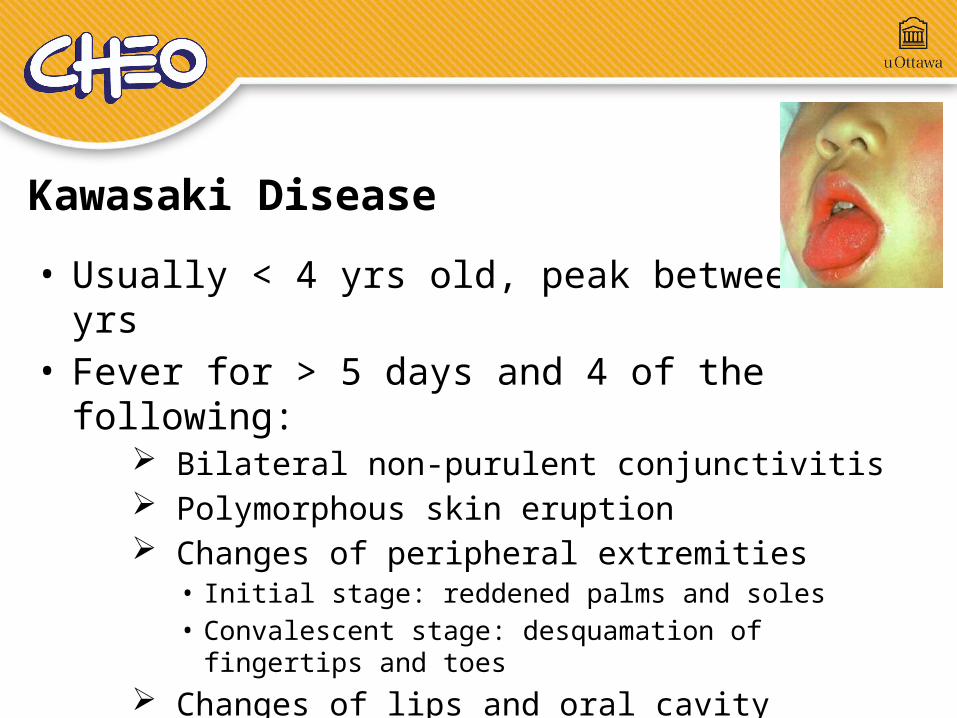
• Usually < 4 yrs old, peak between 1-2 yrs• Fever for > 5 days and 4 of the following:
Bilateral non-purulent conjunctivitis Polymorphous skin eruption Changes of peripheral extremities
• Initial stage: reddened palms and soles• Convalescent stage: desquamation of fingertips and
toes Changes of lips and oral cavity Cervical lymphadenopathy ( >1.5 cm)
Kawasaki Disease

• Subacute phase - Days 11-21• Desquamation of extremities• Arthritis
• Convalescent phase - > Day 21• 25% develop coronary artery aneurysms if
untreated
• Other manifestations:• Uveitis, Pericarditis, Hepatitis, Gallbladder
hydrops• Sterile pyuria, Aseptic meningitis
Kawasaki Disease
• Treatment
• IV Immunoglobulin• Reduces incidence of coronary aneurysms to 3%
if given within 10 days of onset of illness• Defervescence with 48 hrs
• ASA• High dose during acute phase then lower dose for
3 mos
Kawasaki Disease

Case 13 • 3 yr old girl with rash
starting today.
• Recent URTI.
• Swollen ankles and knees. Painful walking.
• Diagnosis?
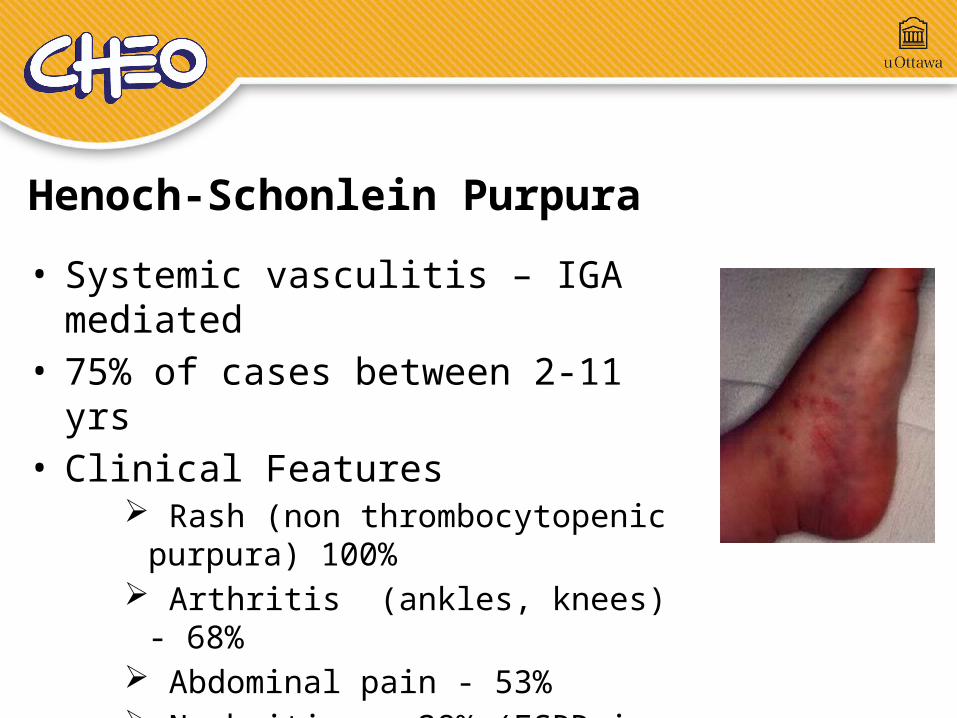
Henoch-Schonlein Purpura• Systemic vasculitis – IGA
mediated• 75% of cases between 2-11 yrs • Clinical Features
Rash (non thrombocytopenic purpura) 100%
Arthritis (ankles, knees) - 68% Abdominal pain - 53% Nephritis - 38% (ESRD in ~1%)
• Intussusception (2-3%)

1 yr old boy with mouth lesions for two days...
• What are the two most likely causes?

Herpes Simplex

Coxsackie

5 yr old girl itchy rash for two days...
Varicella Zoster
• This child comes back to the ED three days later with worsening fever and pain...

Diagnosis?Necrotizing
Fasciitis
• Invasive group A streptococcal infection
• IV Penicillin and Clindamycin
• Consult ID, surgery• MRI
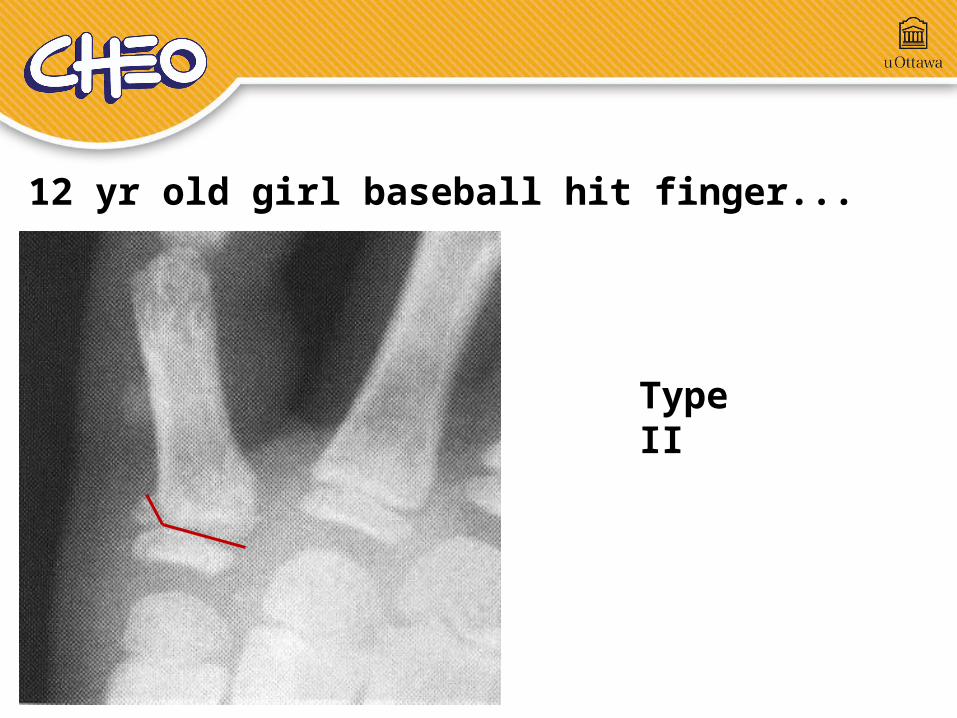
12 yr old girl baseball hit finger...
Type II

Salter-Harris Classification

10 yr old boy fall onto hand...
Type I

Type IV
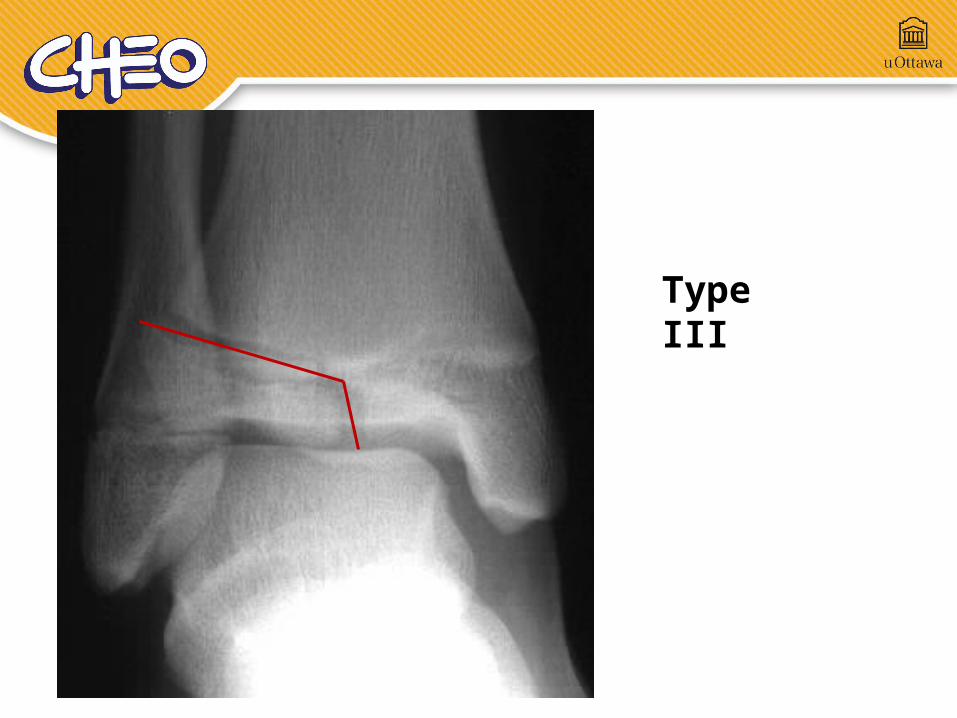
Type III

11 yr old fell off garage...
Type V

• 6 yo boy fall from play structure onto outstretched hand
• Pain and swelling at elbow
• Diagnosis?
Supracondylar Fracture

Radiocapitellar LineLine down middle of radius bisects capitellum in all views
Anterior Humeral LineTransects through posterior 2/3 of capitellum
Elbow Alignment

Elbow Ossification Centers
C
CR R
ET
O
O
I
I
C: Capitellum - 1yR: Radial Head - 3yI: Int(Medial)Epicondyle - 5yT: Trochlea - 7yO: Olecranon - 9yE: Ext(Lateral)Epicondyle - 11y

• 12 yo boy fall from bike
• Painful, swollen elbow

E
R
CT O
Where is the Internal (Medial) Epicondyle?
I ??
I ??

Slipped Capital Femoral Epiphysis• Male, 10-16 yrs, overweight• Acute or subacute pain, decreased internal rotation• Klein line
12 yr old with hip pain


Legg-Calve-Perthe Disease• Avascular necrosis of femoral head• 5-9 yrs, boys > girls• Bilateral in 15%
6 yr old with hip pain

Questions ?