45 21/11/2017
number 15+16
Done by
Corrected by
Doctor Dr Hamed Al-Zoubi


Mycobacterium
Dr Hamed Al-Zoubi
Mycobacterium tuberculosis
• 2billions cases
• 3million deaths
• HIV, MDR

Mycobacterium Tuberculosis Complex
Major human pathogens :
1.Mycobacterium tuberculosis (M. tuberculosis (
2.M. Africanum
3.M. Bovis
4.M. Canettii: smooth
Aerobic acid fast rods.
UV, Alcohol, aldehydes S
Alkaline acid and ammonia R
Mycobacterium Tuberculosis Complex

MYCOBACTERIUM / structure
MYCOBACTERIUM
Growth medium :
Lowenstein–Jensen medium (LJ):
Egg-glycerol with malachite green :
Liquid medium :

MYCOBACTERIUM
Pathogenesis: Caused by immune response
Lung
Primary TB:
Macrophages 1 in alveoli > Ghon’s focus
> To hilar lymph nodes > primary TB complex
> PTB attacked by Macrophages 2 (O2 consumption) > surrounding the lesion in granuloma (caseation) > latent
Tuberculosis (TB) in other places: Skin, intestine and lymph nodes
MYCOBACTERIUM• 90 % of primary infections infections > latent <
reactivation or reinfection > post primary TB
• Reactivation of primary TB > Post primary TB (Also dueto REinfection :(
• Same as in primary but tuberculoma instead of granuloma
• Spread to LLL, upper airways, bladder, skin (Lopusvulgaris) and bladder (more spread and infectivity (
• 10 % of primary > secondary TB > meningitis, pott’s disease, urogenital and skin involvement (s.t milliary TB if opened into a blood vessel > disseminated (

MYCOBACTERIUM
Clinically :
• The following factors increase the likelihood that a patient will have tuberculosis (TB :(
• HIV infection
• History of prior TB treatment
• TB exposure, Travel to or emigration from a TBendemic area
• Homelessness, shelter-dwelling, incarceration
MYCOBACTERIUM
• Classic features associated with active TBare as follows :
• Cough
• Weight loss/anorexia
• Fever
• Night sweats
• Hemoptysis
• Chest pain

MYCOBACTERIUM
Diagnosis :
History and Examination
CXR <<<
PPD test
Lab :
Acid fast stain (Ziehl–Neelsen stain (Culture 6-8 Weeks on L J , shorter in liquid medium
Interferon Gamma interferon
PCR
MYCOBACTERIUM
PPD test (Mantoux test):
2-12 Weeks post infection
Given intradermally
Read within 2-3 days
Delayed HS reaction in the skin
Active infection, vaccine, environmental TB
IGRT?interferon gamma release test

MYCOBACTERIUM / PPD test results
MYCOBACTERIUM
Management:
Isolation:?
Combination, DOTs
(1st line anti TB)
RIFINA 6months +Ethambutol and Pyrazinamide first 2months
2nd line treatment in MDR:
Macrolides, Fluroquinilones, aminoglycosides, cycloserine...
3rd line treatment:
Linezolid, rifabutin, arginine, vitamin D..
Prevention: BCG life attenuated vaccine : ?
• BCG vaccine has a documented protectiveeffect against meningitis and disseminatedTB in children .
Mycobacterium leprae
• Acid fast, aerobic, intracellular bacilli similar to M. Tuberculosis (fat in cell wall (
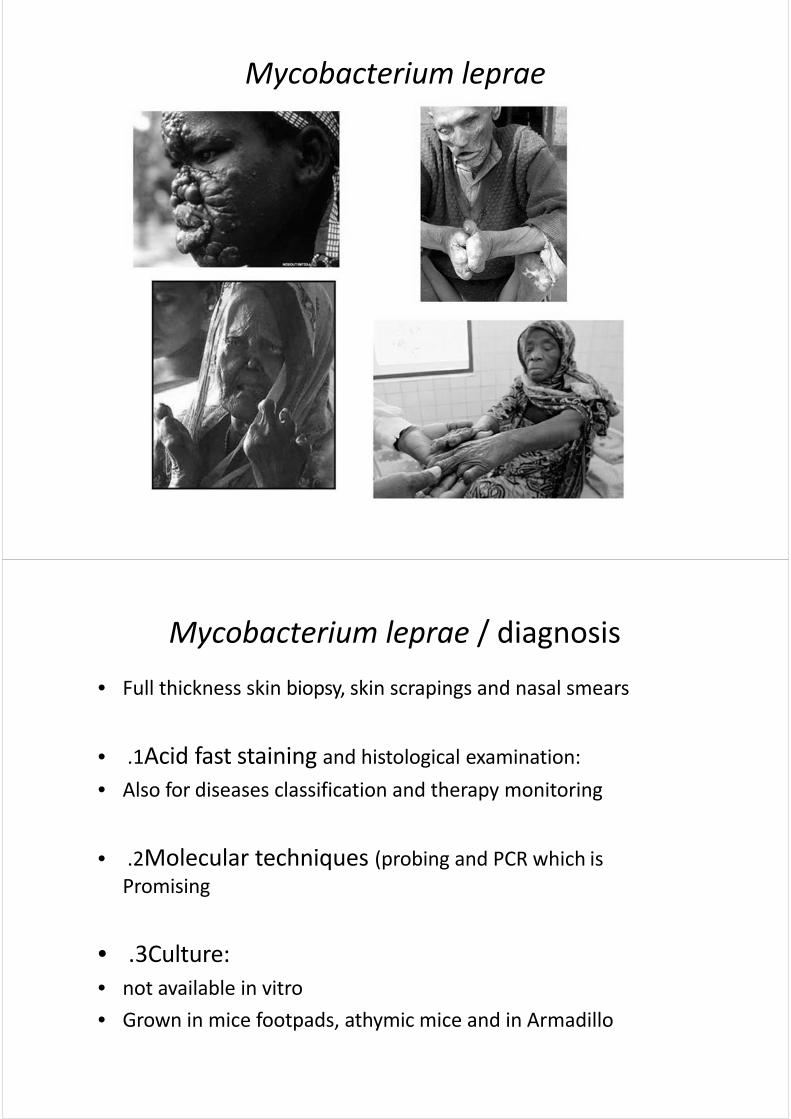
• It causes leprosy (Hansen’s disease (
• Leprosy: chronic granulomatous disease principally affectingthe skin, mucous membrane, peripheral nervous system andanterior chamber of eyes .
• Approximately 2 million cases worldwide; Africa, Asia andsouth America (India, Nepal, Tanzania, Brazil, Madagascar,Mozambique (

Mycobacterium leprae
• MOT :
• Inhalation (respiratory droplets (
• Incubation period on average is 4-8 years (1-30 years (
• Pathogenesis: (determined by the immune response (• Brief bacteraemic phase
• Binds to macrophages and Schwann cells
• immune response
Mycobacterium leprae
• Clinically :
• Thickened lesions of skin / nodules
• Nerve thickening and Loss of sensation (muscle weakness, tissue /organ and nasal septum destruction, ulcers (...
• Disfigurement and mutilation
• classification
1. Tuberculoid (Paucibacillary) leprosy
2. Lepromatous (Multibacillary) leprosy
3. Borderline leprosy

Mycobacterium leprae
• Tuberculoid :• Few skin lesions < 5
• Usually no acid fast bacilli seen in the lesions
• Lepromatous :
• skin lesions > 5
• Many acid fast bacilli seen in lesions
• More in cold areas (nose, ear, knees, elbow and buttocks (
• ‘Leonine facies ’
Mycobacterium leprae
Mycobacterium leprae
Mycobacterium leprae / diagnosis
• Full thickness skin biopsy, skin scrapings and nasal smears
• 1 . Acid fast staining and histological examination :
• Also for diseases classification and therapy monitoring
• 2 . Molecular techniques (probing and PCR which isPromising
• 3 . Culture :• not available in vitro
• Grown in mice footpads, athymic mice and in Armadillo

Armadillo
Mycobacterium leprae / treatment
Effective treatment is available :
1 . Paucibacillary
• Dapsone + Rifampicin
• 6months
2 . Multibcillary
• Dapsone+Rifampicin+Clofazamine
• 12months

Mycobacterium leprae / treatment
Effective treatment is available :
1 . Paucibacillary
• Dapsone + Rifampicin
• 6months
2 . Multibcillary
• Dapsone+Rifampicin+Clofazamine
• 12months
•The End

Spirochaetes
Dr Hamed Al Zoubi
• Treponema
)T. pallidum (
)T. pertenue (
)T.endemicum (
)T. carateum (
orher non pathogenic spp

T. pallidum• Syphilis :• Belongs to spirochetes which are thin – walled ,
flexible spiral rods
• Motile by flagella :
at both sides
wrap around the bacterial cell body .
In contrast to other motile bacteria, these flagella do not protrude into the surrounding medium but are enclosed within the bacterial outer membrane
• Has not been grown on bacteriologic media

Syphilis
• Transmission :1. Sexually2. Contact with skin lesions
3. Congenital (mother to baby (
4. Blood donation during primary and secondarystages
Syphilis• Pathogenesis :
• No toxins
• Multiplication at primary site of infectionleading to a painless ulcer called Chancre
• Widespread via blood to many tissues
• Primary, secondary, latent, late tertiary stages
• Human only
• Infectious dose less than 10 organisms
• Incubation period: 2-10 weeks, 3 wks usually
• Early (primary and secondary), latent andtertiary stages
• Overall and of the early diseases :
• 1/3 will heal without treatment
• 1/3will go into latent
• 1/3into tertiary
Syphilis / clinically1 . Primary :
• Painless Chancre on genitalia, cervix or anogenital area
• Usually single
• Disappear spontaneously in 3 – 6 weeks
• Infectious
• Inguinal LNE
• Exudates used for diagnosis

2 . Secondary syphilis (infectious :(
• 2 -12 weeks after chancre disappeared
• Non specific symptoms (e.g fever malaise, lethargy ,headache, lymph nodeenlargement (
• Maculopapular and pustular rash mainly on trunkand extremities
• Heals spontaneously
• There might be Multiplication and production of lesion in lymph nodes, liver, joints, muscles, skin and mucous membranes

3 . Latent :
• No lesion but serological evidence exists
• Early and late latent
• Early latent phase: may reactivate and manifest as asecondary lesion i.e infectious
4 . Tertiary (3-30 years :(
• Neurosyphilis: e.g Meningoencephalitis and paralysis
• Cardiovascular: aneurysm of ascending aorta, aortitis
• Skin and bone granulomatous lesions (Gummas (
• Congenital syphilis:
• Blood – placenta – fetus
• Intrauterine death, abortion, low birth weight
• Facial abnormalities e.g saddle shape nose
• Diagnosis:
1. Detection of the organism in the exudates and lesions using dark field E.M or phase contrast, Immunofluorescent antibodies
Low sensitivity
2. Serology:
A. Non-specific antibodies (1-2 weeks after the primary chancre appears):
• Rapid plasma regain test (VDRL test): detectinganticardiolipin antibodies
• Cardiolipin?
B. Specific antibody detection:
• These tests should be used to confirm that a positiveresult with a non-specific test is truly due to syphilis.
Syphilis / serology – specific antibody detection
1. FTA-Abs (fluorescent Treponema antibodies-absorption): patient's serum is first absorbed with non-pathogenic treponemes to remove cross-reacting antibodies before reaction with T. pallidum antigens
2.TPHA (Treponema pallidum Haemagglutinin antibodies (

• Treatment :• Penicillin G• If allergic, Doxycycline or erythromycin is a good
alternative• In neurosyphilis use penicillin and Doxycycline together
• Prevention :• No vaccine• Early diagnosis and treatment of case and contact is
important• Sexually transmitted :• Test for syphilis if any STD exists

• Borrelia Burgdorferi: Lyme Disease.. Common USA, Biting Insects (Ticks).. Wild Animals, Rodents, Birds ..Incub. Few Weeks-Months..Single/Multiple Skin Lesions.. Systemic Disease.. Arthritis, CNS.. Cardic Abnormalities..
• B. recurrentis: recurrent fever, can be fatal• Liptospiral diseases: Zoonosis, mild-severe
fatal systemic .. Weils’s disease ..high Fever,Jaundice, vasculitis, Bleeding.
• Diagnosis: Serological Tests, Special culture
Chlamydia

Family: Chlamydiaceae
• Genus: Chlamydia– C. trachomatis - Urogenital infections,
trachoma, conjunctivitis, pneumonia and lymphogranuloma venerium (LGV (
• Genus: Chlamydophilia– C. psittaci - Pneumonia (psittacosis (
– C. pneumoniae - Bronchitis, sinusitis ,pneumonia and possibly atherosclerosis
N.B. New taxonomy, previously three species in one genus - Chlamydia
Chlamydia- Microbiology
• Small obligate intracellular parasites
• Inner and outer membrane
• LPS but no peptidoglycan– Cell wall not well characterized
• Energy parasites– Can’t make ATP

Physiology and Structure
• Elementary bodies (EB (– Extracellular form
– Rigid outer membrane• Disulfide linked proteins
– Resistant to harsh conditions
– Non-replicating, non-metabolically active form
– Infectious form• Bind to columnar epithelial cells (macrophages (
Physiology and Structure
• Reticulate bodies (RB(– Intracellular form
– Fragile membrane• Fewer disulfide bonds
– Metabolically active form
– Replicating form
– Non-infectious
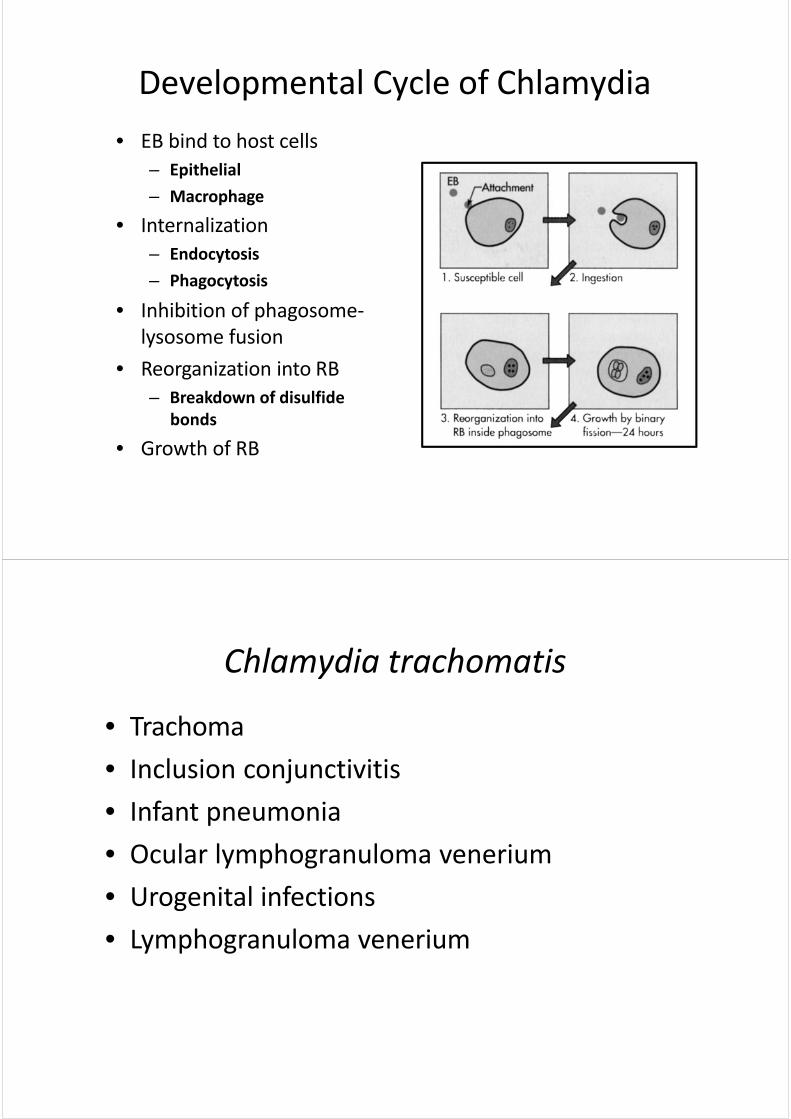
Developmental Cycle of Chlamydia
• EB bind to host cells– Epithelial
– Macrophage
• Internalization– Endocytosis
– Phagocytosis
• Inhibition of phagosome-lysosome fusion
• Reorganization into RB– Breakdown of disulfide
bonds
• Growth of RB
Chlamydia trachomatis
• Trachoma
• Inclusion conjunctivitis
• Infant pneumonia
• Ocular lymphogranuloma venerium
• Urogenital infections
• Lymphogranuloma venerium

C. trachomatis
• Ocular infections– Worldwide
– Poverty and overcrowding
– Endemic in Africa, Middle East, India, SE Asia
– United States - American Indians
– Infection of children
– Transmission: droplets, hands, contaminatedclothing, flies, contaminated birth canal
Clinical Syndrome -Trachoma
From: G. Wistreich, Microbiology Perspectives, Prentice Hall

Clinical Syndrome -Trachoma )C.trachomatis biovar: trachoma (
• Chronic or repeated infection– Follicle formation on conjunctiva
– Scarring of the conjunctiva
Clinical Syndrome -Trachoma
• Eyelids turn in and abrade cornea– Ulceration
– Scarring
– Blood vessel formation

Clinical Syndrome -Trachoma
• Flow of tears impeded–Secondary infections
Clinical Syndrome - Ocular Lymphogranuloma Venereum
(C.trachomatis biovar: LGV)
• Conjunctivitis and associated lymphadenopathy
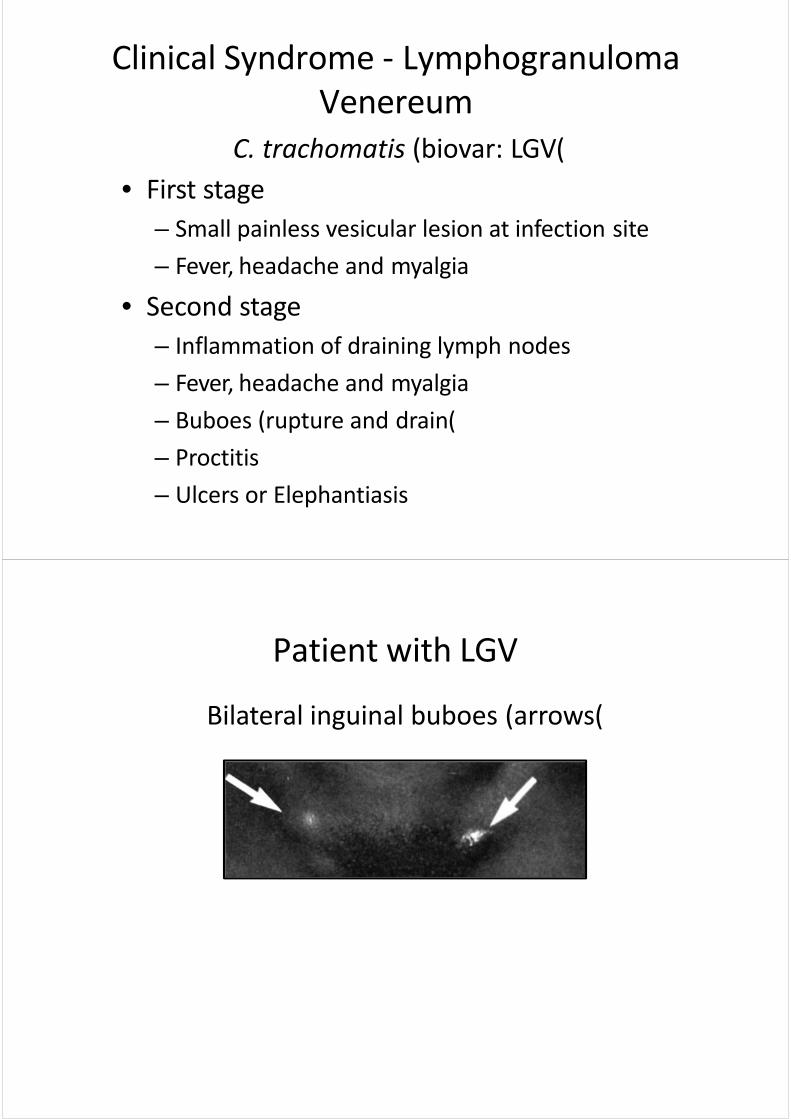
Clinical Syndrome - LymphogranulomaVenereum
C. trachomatis (biovar: LGV (• First stage
– Small painless vesicular lesion at infection site
– Fever, headache and myalgia
• Second stage– Inflammation of draining lymph nodes
– Fever, headache and myalgia
– Buboes (rupture and drain (
– Proctitis
– Ulcers or Elephantiasis
Patient with LGV
Bilateral inguinal buboes (arrows (

C. trachomatis - Diagnosis
• Histo Cytology– Iodine-staining
inclusions
– Not sensitive
• Culture– Iodine staining
inclusions
– Most specific
Iodine-stained inclusion bodies
C. trachomatis - Diagnosis
• Antigen detection (ELISA or IF(– Group specific LPS
– Strain specific outer membrane proteins
• Serology– Can’t distinguish between current or past infection
– Detection of high titer IgM antibodies can be helpful
• Nucleic acid probes– Several kits available
– May eventually replace culture

C. trachomatis - Treatment and Prevention
• Tetracycline, erythromycin and sulfonamides
• Vaccines are of little value
• Treatment coupled with improved sanitation
• Safe sexual practices
• Treatment of patients and their sexual partners
Chlamydophilia (Chlamydia) psittaci
• Psittacosis (Parrot fever (
• Ornithosis

Pathogenesis - C. psittaci
• Inhalation of organisms in bird droppings– Person to person transmission is rare
• Hematogenous spread to spleen and liver– Local necrosis of tissue
• Hematogenous spread to lungs and other organs
• Lymphocytic inflammatory response– Edema, infiltration of macrophages, necrosis and
occasionally hemorrhage
– Mucus plugs may develop in alveoli
• Cyanosis and anoxia
Laboratory Diagnosis - C. psittaci
• Serology (Complement fixation test ( –Fourfold rise in titer
Treatment and Prevention - C. psittaci
• Tetracycline or erythromycin
• Quarantine of imported birds
• Control of bird infection– Antibiotic supplementation of food
Chlamydophilia (Chlamydia) pneumoniae
• Atypical pneumonia
• Atherosclerosis?
Pathogenesis - C. pneumoniae
• Person to person spread –Respiratory droplets
• Bronchitis, sinusitis and pneumonia
Laboratory Diagnosis - C. pneumoniae• Serology
–Fourfold rise in titer

Treatment and Prevention - C. pneumoniae
• Tetracycline or erythromycin
• Difficult to prevent transmission
• No vaccine
The End