Nephritic Sx & Nephrotic Sx
Case report 1
18 yr old man Bilateral loin pain Macroscopic haematuria Sore throat started one day earlier BP 140/90; euvolaemic Creatinine 120 μmol/l Proteinuria and haematuria on dipstix
Case Report 2
20 yr old ladyCompletely wellHaematuria on dipstixNo proteinuriaNormotensive
Case Report 3
12 year old boyImpetigo two weeks earlierHeadacheOliguricFrothy dark coloured urineHypertensive
Case report 4
15yr old woman 3/12 ankle swelling; face and fingers
swollen in the am BP 130/80; JVP normal; Leg oedema Creatinine 54 μmol/l Cr Cl 140 ml/min Albumin 18 g/l 24 hr u.protein 10 g
Case Report 5
30 year old man,diabetic Known hypertensive Ankle oedema Dipstix: ++++ proteinuria Creatinine 124 μmol/l (80 – 120) Albumin 30 g/l (36 – 45)
Case Report 6
50 year old obese manHypertension 10 yearsNIDDM 3 yearsNo retinopathyCreatinine 124 μmol/l24 hr urine protein 2 gHbA1 9.6%
10
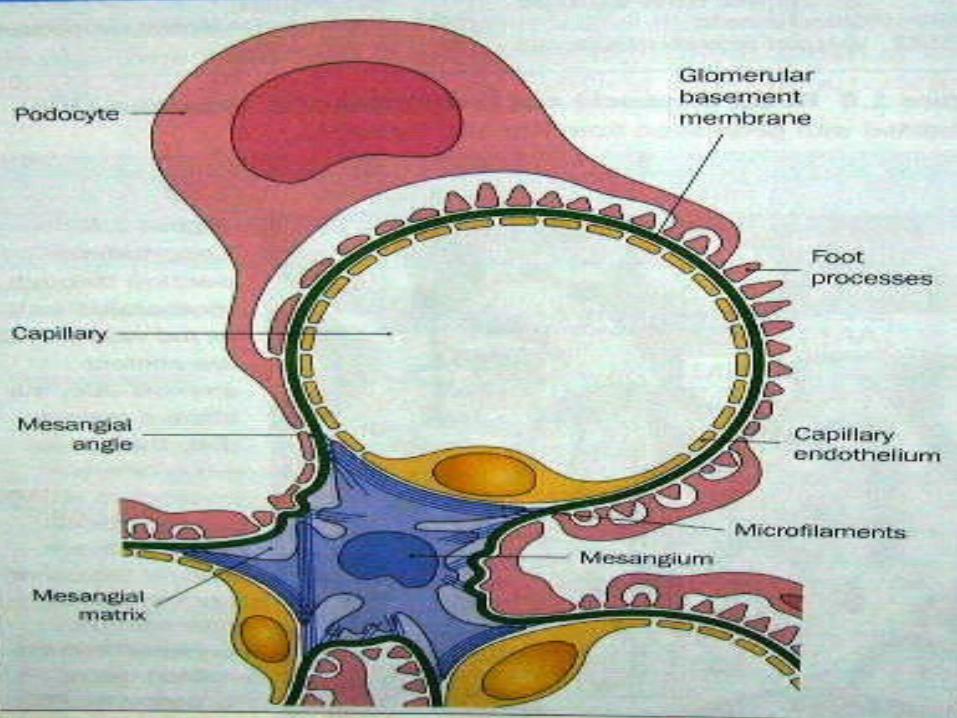
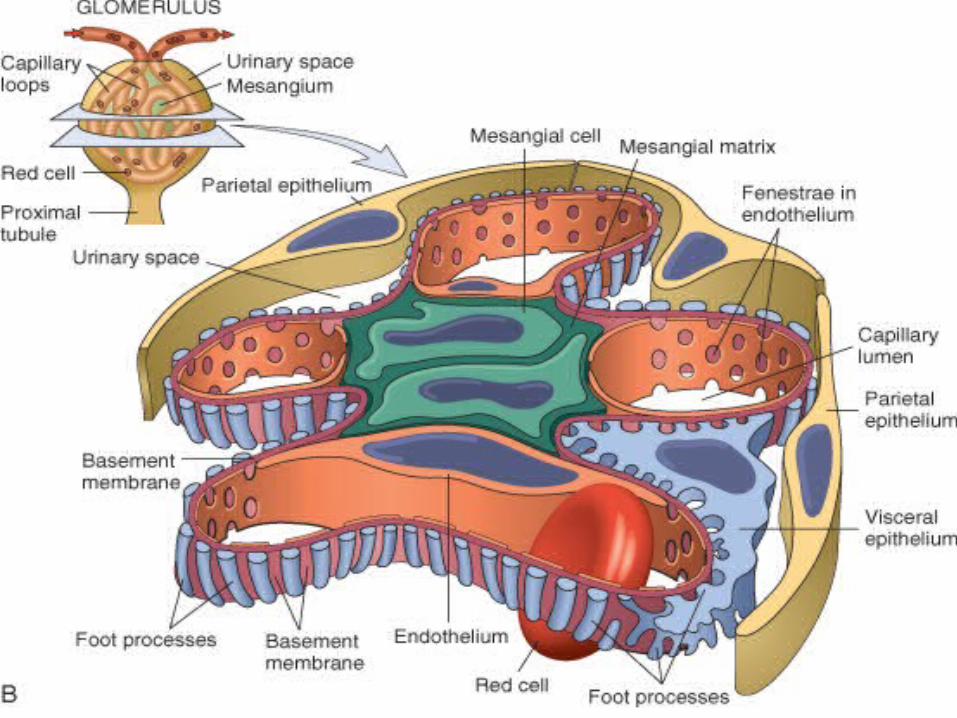
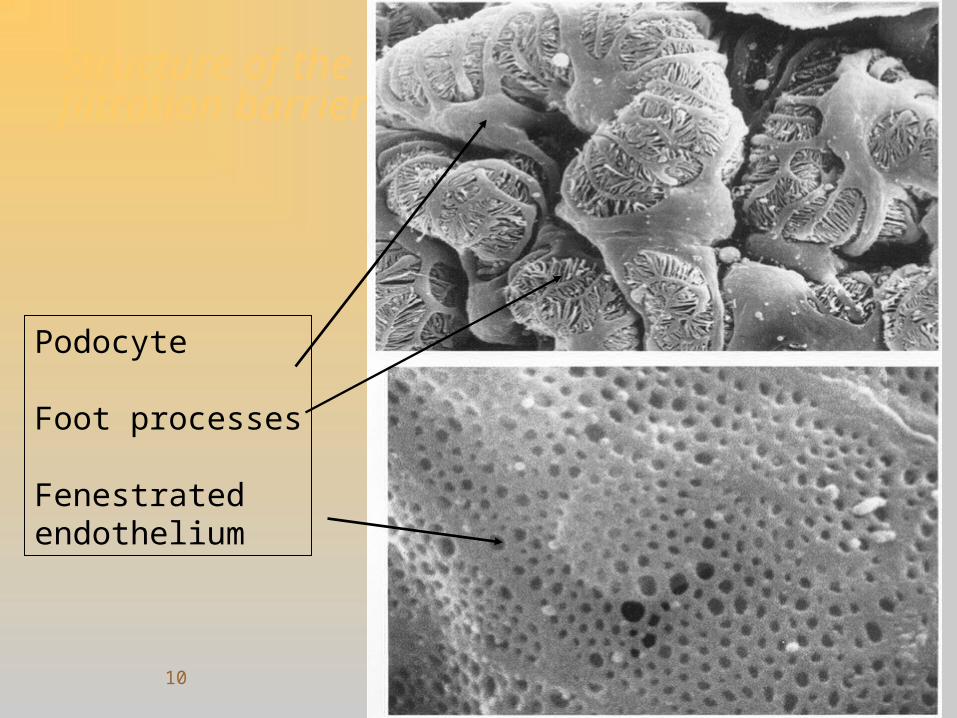
Structure of the filtration barrier
Podocyte
Foot processes
Fenestrated endothelium
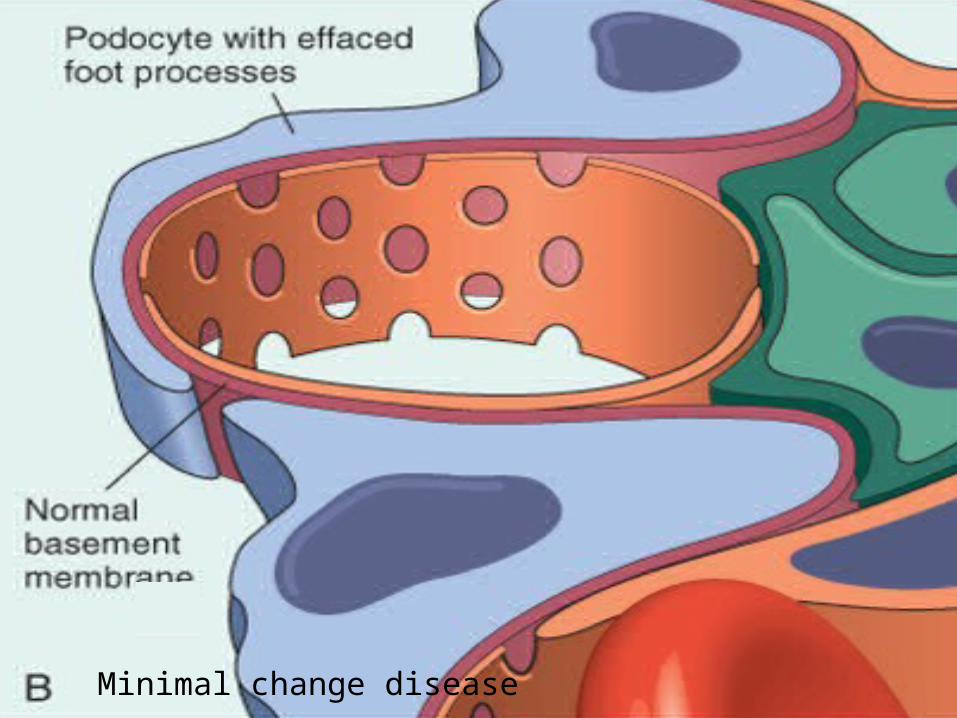
Minimal change disease
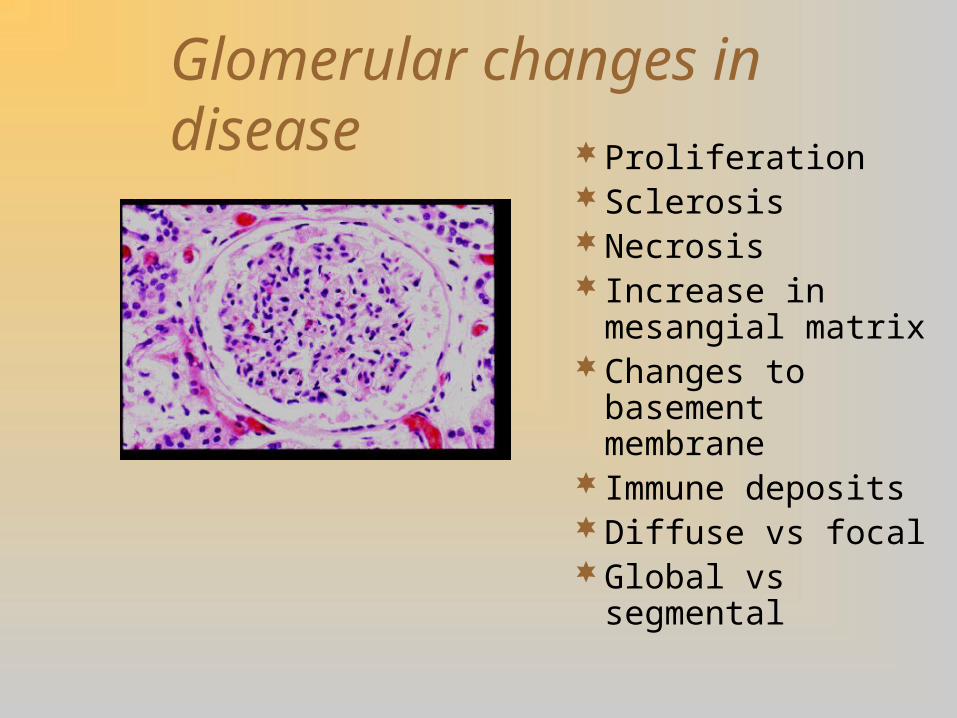
Glomerular changes in diseaseProliferationSclerosisNecrosis Increase in mesangial
matrixChanges to basement
membrane Immune depositsDiffuse vs focalGlobal vs segmental
Common Syndromes
Nephrotic Syndrome
Nephritic Syndrome
Rapidly Progressive GN
Loin Pain Haematuria Syndrome
Features of Glomerular Disease
ProteinuriaHaematuriaRenal FailureSalt and Water RetentionLoin Pain

Salt and Water Retention
Hypertension
Oedema
Oliguria
Loin Pain
Rare
Proteinuria
Marker of renal disease Risk factor for
cardiovascular disease– Dyslipidaemia
– Hypertension
– Something more?
24 hr protein vs urine protein:creatinine ratio
Nephrotic syndrome
Proteinuria > 40 mg/m2*hrHypoalbuminaemia (<2.5mg/dl)OedemaHyperlipidemia
ThrombosesInfection
Learning Points
Clinical features Commonest typesPrognosisCauses Treatments
Nephrotic Syndrome
Causes of primary idiopathic NS– Minimal change disease– Mesangial proliferation– Focal segmental glomerulosclerosis
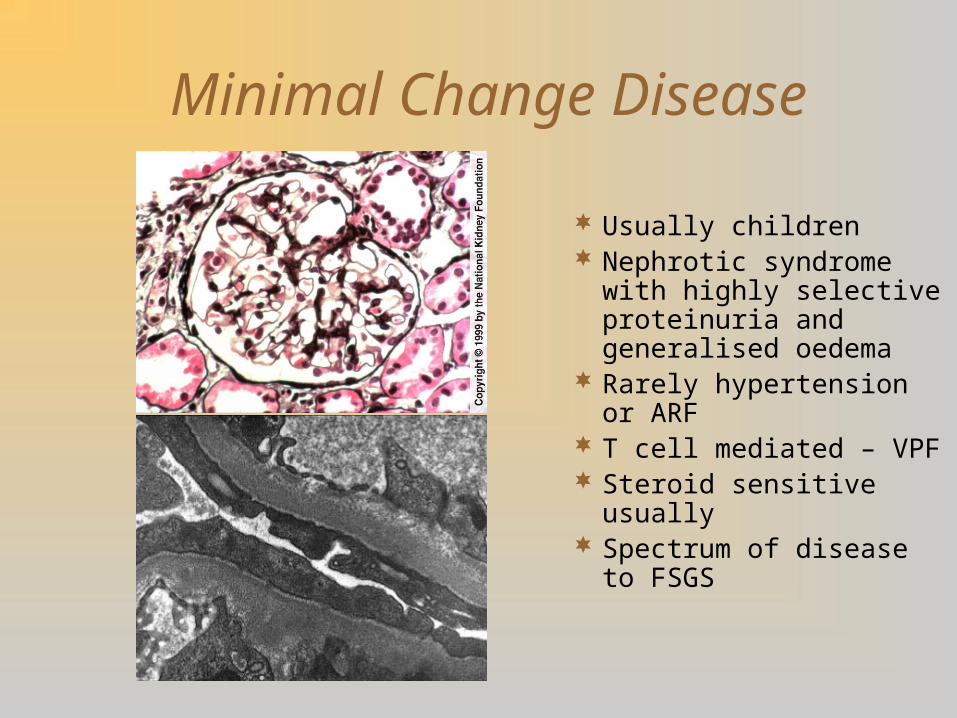
Minimal Change Disease
Usually children Nephrotic syndrome with
highly selective proteinuria and generalised oedema
Rarely hypertension or ARF
T cell mediated – VPF Steroid sensitive usually Spectrum of disease to
FSGS
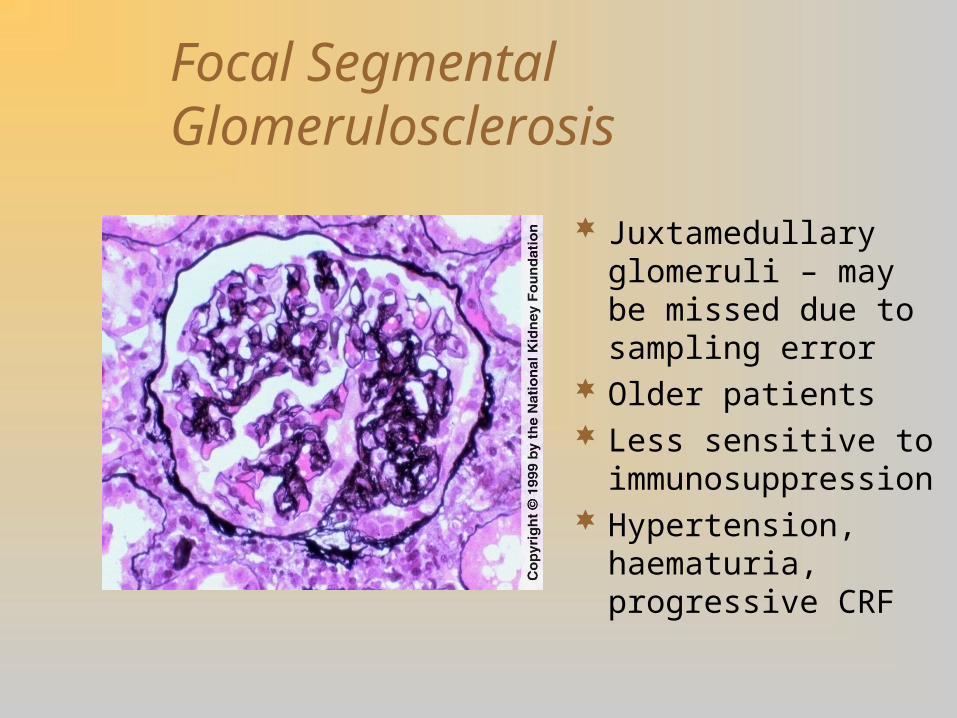
Focal Segmental Glomerulosclerosis
Juxtamedullary glomeruli – may be missed due to sampling error
Older patients Less sensitive to
immunosuppression Hypertension,
haematuria, progressive CRF

FSGS:
Familial
VUR
Drug abuse
Obesity
Common types of GN
PrimaryThin membrane diseaseIgA diseaseMinimal Change / FSGS spectrumMembanous Nephropathy
SecondaryPSGN & Diabetic Glomerulosclerosis
Rarer Types
Diffuse endocapillary proliferative GN (post infectious GN)
Crescentic GNMembanoproliferative / mesangiocapillary
GN
Nephritic Syndrome
Haematuria
Hypertension
Oliguria
Edema
Rapidly progressive GN
Nephritic or nephrotic onset
ESRF in six months
General Treatment of GN
Control BPAngiotensin blockadeStatinLose weightStop smoking(pneumococcal prophylaxis)(anticoagulation)
Help!
I need a volunteer!
30

Case report 1
18 yr old man Bilateral loin pain Macroscopic haematuria Sore throat started one day earlier BP 140/90; euvolaemic Creatinine 120 μmol/l Proteinuria and haematuria on dipstix
Case 1: indicative answers
IgA Disease
Renal failure, proteinuria, haematuria, oedema, hypertension, oliguria, loin pain
All except oedema and oliguria

Mesangial IgA disease
Classical Berger’s Disease Microscopic haematuria Proteinuria (rarely
nephrotic) Hypertension Chronic renal failure ? Failure of hepatic
clearance of IgA Association with GI
disease No specific treatment
Ig A Nephropathy
Ig A nephropathy is the most common primary GN worldwide
Usually present with hematuriaEpisodes of gross hematuria are precipitated by
flu like illness, exerciseUrinary protein excretion usually non-nephroticAssociated with chronic liver ds, psoriasis, IBD
and HIV disease.

Ig A Nephropathy
Only 30% of patients with IgA nephropathy has progressive disease.
In progressive disease, use of fish oil may be beneficial.
Immunosuppressive therapy in patients with Ig A nephropathy has not consistently shown to be of benefit
Case Report 2
20 yr old ladyCompletely wellHaematuria on dipstixNo proteinuriaNormotensive
Case 2: indicative answers
Exclude menstruation! Thin membrane disease (possibly IgA
disease)Commonest cause of isolated microscopic
haematuria in this age group. At this age, urological cause unlikely; nil
to suggest infection / urolithiasis

Thin membrane disease
Most common GNMicroscopic haematuriaFamilialBenignNo treatment neededMost young people with
isolated microscopic haematuria have thin membrane disease
Case Report 3
12 year old boyImpetigo two weeks earlierHeadacheOliguricFrothy dark coloured urineHypertensive
Case 3: indicative answers
Acute nephritic syndromePost-streptococcal glomerulonephritisDiffuse proliferative endocapillary
glomerulonephritisDue to salt and water retention, so salt
restriction or loop diuretic
Acute Post-Infectious GN
Usually occur in childrenPost-streptococcal GN is the most common cause of
post infectious GNOccurs after a streptococcal sore throat or impetigoCaused by Group A, beta-hemolytic streptococci,
particularly nephritogenic strains – Type 1,4,12 (throat) and 2,49(skin)
Acute Post-Infectious GN
Acute onset of gross hematuria (COLA COLORED) or microscopic hematuria after latent period of 10-14 days.
Edema/hypertensionRBC casts on U/AElevated creatinine, increased ASO titerDecreased complement level

Acute Post-Infectious GN
LM – Diffuse proliferative and exudative GN
IF – IgG and C3 “lumpy, bumpy”
EM – Sub epithelial “Hump” or “Flame” like deposits
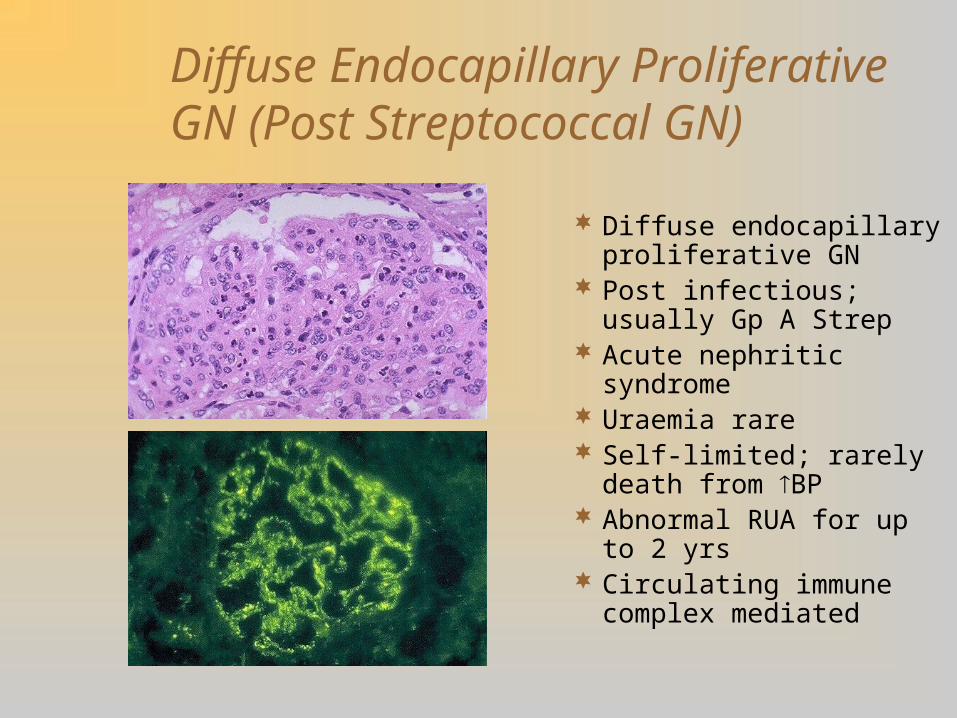
Diffuse Endocapillary Proliferative GN (Post Streptococcal GN)
Diffuse endocapillary proliferative GN
Post infectious; usually Gp A Strep
Acute nephritic syndrome Uraemia rare Self-limited; rarely death
from BP Abnormal RUA for up to 2
yrs Circulating immune
complex mediated
Acute Post-Infectious GN
Renal biopsy is generally not required.
Treatment is supportive and consist of sodium restriction, control of BP and dialysis if this become necessary.
Complications of the Nephritic Syndrome
Hypertensive encephalopathy (seizures, coma)
Heart Failure (pulmonary oedema)
Uraemia requiring dialysis
Prognosis in the Nephritic Syndrome
More than 95% of children make a complete recovery
Chronic renal impairment in the longer term is uncommon in children
Bad prognostic features include severe renal impairment at presentation and continuing heavy proteinuria and hypertension
Adults more likely to have long term sequellae than children

Case report 4
15 yr old girl 3/12 ankle swelling; face and fingers
swollen in the am BP 130/80; JVP normal; Leg oedema Creatinine 54 μmol/l Cr Cl 140 ml/min Albumin 18 g/l 24 hr u.protein 10 g
Case 4: indicative answers
Minimal change – focal segmental glomerulosclerosis spectrum
Very nephrotic Age and borderline BP make FSGS more
likely than MCNEffect of loss of colloid osmotic pressure
gradient across glomerulus causing hyperfiltration
Case Report 5
30year old man,diabetic Known hypertensive Ankle oedema Dipstix: ++++ proteinuria Creatinine 124 μmol/l (80 – 120) Albumin 30 g/l (36 – 45)

Case 5: indicative answers
Nephrotic syndrome secondary to diabetes / membranous disease
Refer urgently to nephrology
Diabetic glomerulosclerosis
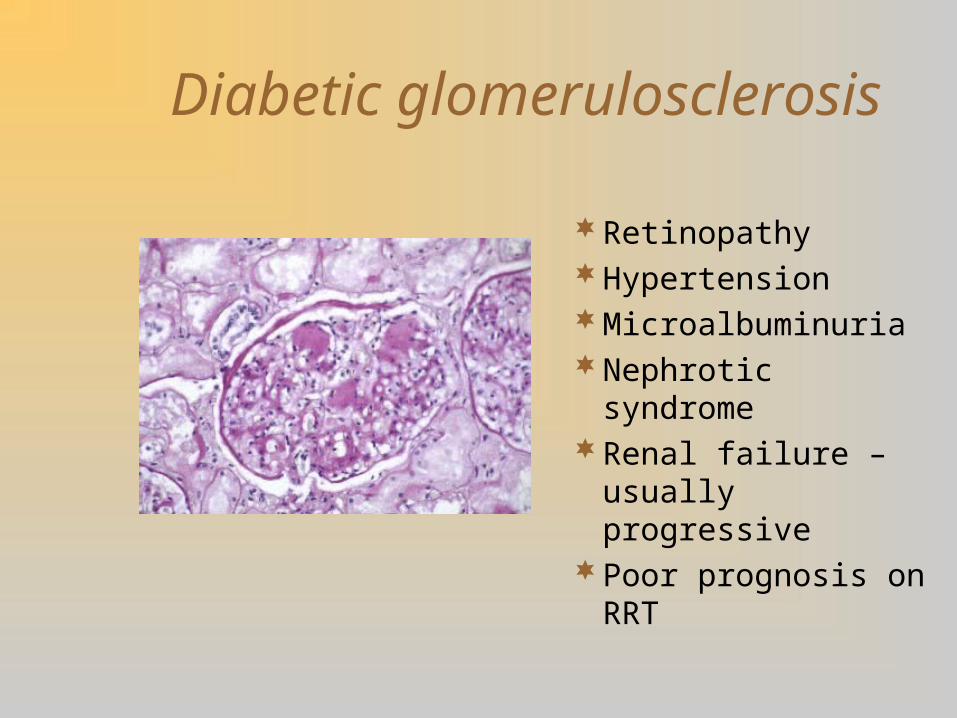
RetinopathyHypertensionMicroalbuminuriaNephrotic syndromeRenal failure –
usually progressivePoor prognosis on
RRT
What we’d like!
Demography including tel no and occupationReason for referral: presenting complaint,
expectationsCo-morbidities, incl other diagnoses, smoking,
alcohol and BMI, social care needsExaminationMedications (incl recently stopped), allergies etcTreatment and investigations to dateSpecial requirements (eg interpreter)
Case Report 6
50 year old obese manHypertension 10 yearsNIDDM 3 yearsNo retinopathyCreatinine 124 μmol/l24 hr urine protein 2 gHbA1 9.6%
Case 6: indicative answers
Obesity-related FSGS more likely than diabetic nephropathy (duration diabetes, absence of retinopathy)
Worsening nephrotic syndrome and progressive renal failure; Death from cardiovascular cause before reaches ESRF
Stop smoking, lose weight, improve glycaemic control, regular exercise, healthy diet, moderate alcohol in that order
Case 6: indicative answers contd
Lack of ownership of responsibility for own healthWithdrawal symptoms (smoking) Denial of calorie intakeDifficulty exercising due to immobilityNo!
– Problems with MDRD equation– No evidence of benefit of ACE inhibitors in absence proteinuria– Dangers of ACE inhibitors in patients with angioneurotic
oedema, hypotension or bilateral renal artery stenosis
Lessons
Not all abnormal urinalysis is a UTI
Acute pyelonephritis is very rarely bilateral
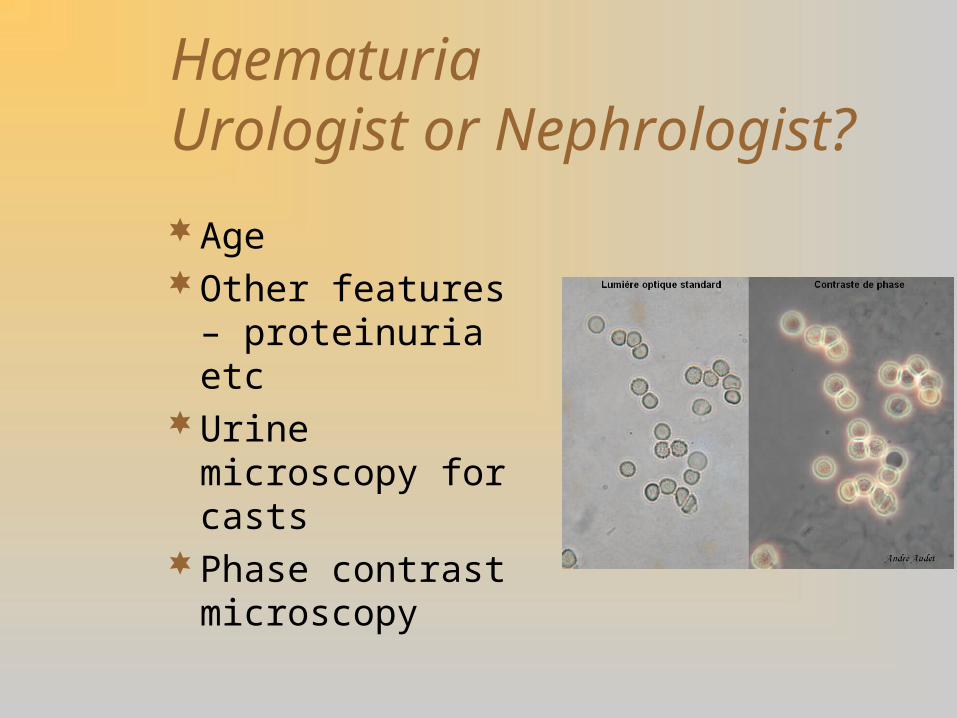
Haematuria Urologist or Nephrologist?
AgeOther features –
proteinuria etcUrine microscopy for
castsPhase contrast
microscopy

Non-dysmorphic vs dysmorphic
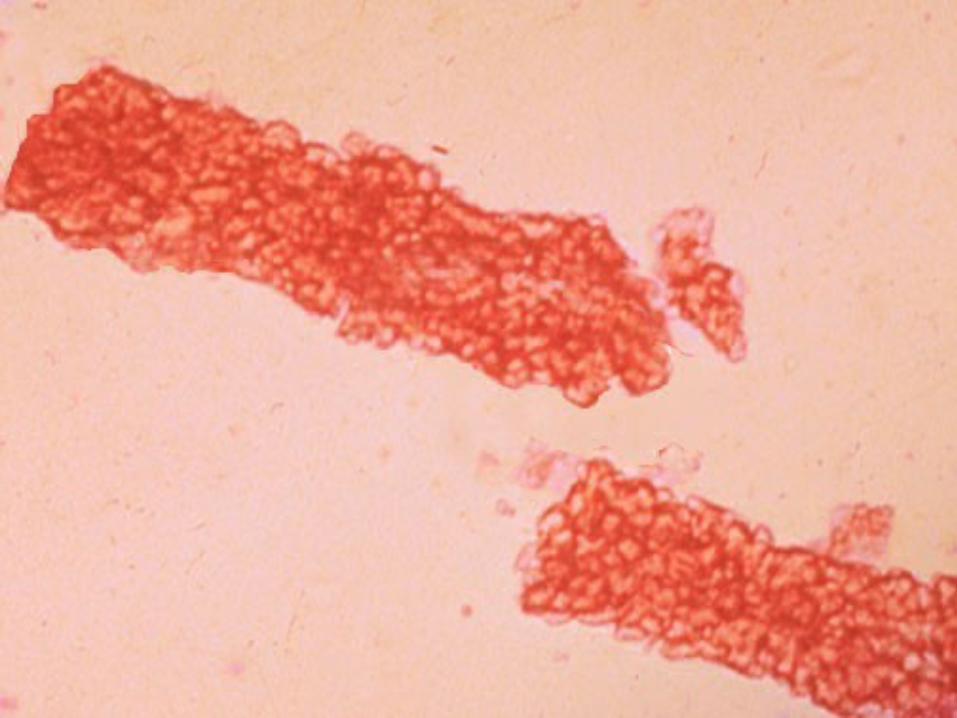
RBC Cast
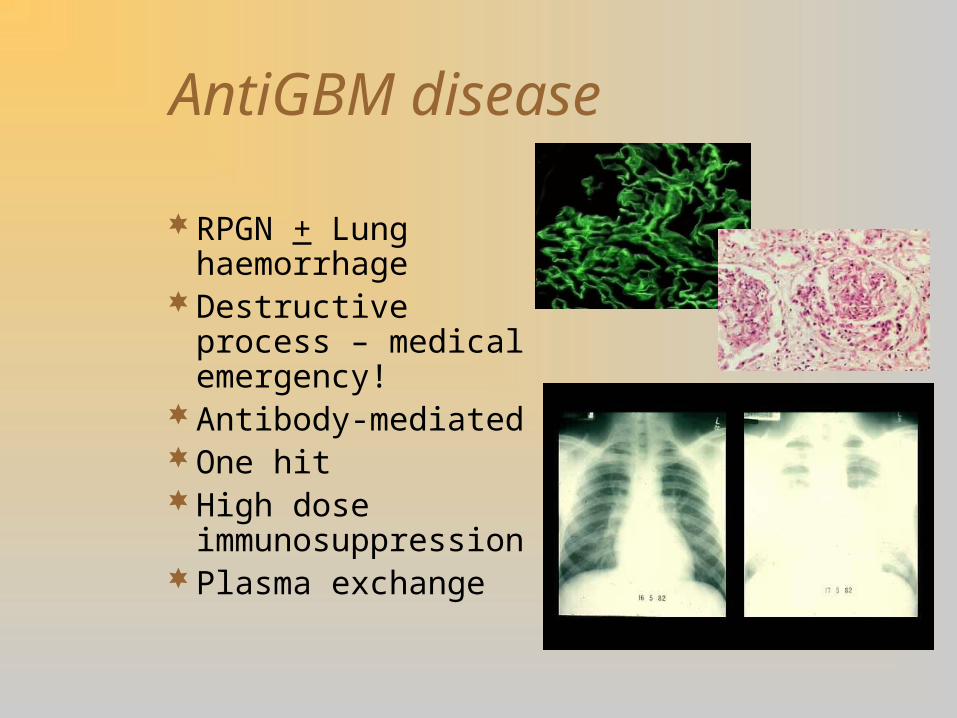
AntiGBM disease
RPGN + Lung haemorrhage
Destructive process – medical emergency!
Antibody-mediatedOne hitHigh dose
immunosuppressionPlasma exchange
Any Questions?
Whoopee! It’s .........
….Coffee Time