Motor Control Exercise for Persistent,Nonspecific Low Back Pain:A Systematic ReviewLuciana G Macedo, Christopher G Maher, Jane Latimer, James H McAuley
Background. Previous systematic reviews have concluded that the effectivenessof motor control exercise for persistent low back pain has not been clearlyestablished.
Objective. The objective of this study was to systematically review randomizedcontrolled trials evaluating the effectiveness of motor control exercises for persistentlow back pain.
Methods. Electronic databases were searched to June 2008. Pain, disability, andquality-of-life outcomes were extracted and converted to a common 0 to 100 scale.Where possible, trials were pooled using Revman 4.2.
Results. Fourteen trials were included. Seven trials compared motor control ex-ercise with minimal intervention or evaluated it as a supplement to another treat-ment. Four trials compared motor control exercise with manual therapy. Five trialscompared motor control exercise with another form of exercise. One trial comparedmotor control exercise with lumbar fusion surgery. The pooling revealed that motorcontrol exercise was better than minimal intervention in reducing pain at short-termfollow-up (weighted mean difference14.3 points, 95% confidence interval[CI]20.4 to 8.1), at intermediate follow-up (weighted mean difference13.6points, 95% CI22.4 to 4.1), and at long-term follow-up (weighted mean differ-ence14.4 points, 95% CI23.1 to 5.7) and in reducing disability at long-termfollow-up (weighted mean difference10.8 points, 95% CI18.7 to2.8). Motorcontrol exercise was better than manual therapy for pain (weighted mean differ-ence5.7 points, 95% CI10.7 to 0.8), disability (weighted mean differ-ence4.0 points, 95% CI7.6 to 0.4), and quality-of-life outcomes (weightedmean difference6.0 points, 95% CI11.2 to 0.8) at intermediate follow-upand better than other forms of exercise in reducing disability at short-term follow-up(weighted mean difference5.1 points, 95% CI8.7 to 1.4).
Conclusions. Motor control exercise is superior to minimal intervention andconfers benefit when added to another therapy for pain at all time points and fordisability at long-term follow-up. Motor control exercise is not more effective thanmanual therapy or other forms of exercise.
LG Macedo, PT, MSc, is a PhD stu-dent at The George Institute forInternational Health, The Univer-sity of Sydney, PO Box M201, Mis-senden Rd, Camperdown, Syd-ney, New South Wales, 2050Australia. Address all correspon-dence to Ms Macedo at:[email protected].
CG Maher, PT, PhD, is Director,Musculoskeletal Division, TheGeorge Institute for InternationalHealth, The University of Sydney.
J Latimer, PT, PhD, is AssociateProfessor, The George Institute forInternational Health, The Univer-sity of Sydney.
JH McAuley, PhD, is ResearchManager, The George Institute forInternational Health.
[Macedo LG, Maher CG, Latimer J,McAuley JH. Motor control exer-cise for persistent, nonspecific lowback pain: a systematic review.Phys Ther. 2009;89:925.]
2009 American Physical TherapyAssociation
Research Report
Post a Rapid Response orfind The Bottom Line:www.ptjournal.org
January 2009 Volume 89 Number 1 Physical Therapy f 9
Low back pain (LBP) is one of themain causes of disability, and,despite its high prevalence, thesource of pain is not established inthe majority of cases and the termnonspecific low back pain isused.14 One factor that has beenproposed as important in the genesisand persistence of nonspecific LBP isstability and control of the spine.4
Studies of individuals with LBP haveidentified impairments in the controlof the deep trunk muscles (eg, trans-versus abdominis and multifidus) re-sponsible for maintaining the stabil-ity of the spine.58 For example,activity of the transversus abdominismuscles9 and the multifidus muscles7
is delayed during arm movements(that challenge the stability of thespine) in individuals with LBP. Fur-thermore, there is evidence of de-creased cross-sectional area10 andincreased fatiguability11 and a sug-gestion of increased intramuscularfat in the paraspinal muscles of indi-viduals with LBP.12 Therefore, theo-retically, an intervention that aims tocorrect the changes occurring in thedeep trunk muscles and that targetsthe restoration of control and coor-dination of these muscles should beeffective in the management of per-sistent LBP.
Motor control exercise was devel-oped based on the principle that in-dividuals with LBP have a lack ofcontrol of the trunk muscles. Theidea is to use a motor learning ap-proach to retrain the optimal controland coordination of the spine. Theintervention involves the training ofpreactivation of the deep trunk mus-cles, with progression toward morecomplex static, dynamic, and func-tional tasks integrating the activationof deep and global trunk muscles.13,14
Although a number of laboratorystudies supporting the underlyingmechanism of action of motor con-trol exercises have been published inthe last decades,5,9,15 the clinical ef-
fectiveness of motor control exer-cise for persistent LBP is still un-clear.5,9,15 Three systematic reviewsof motor control exercise have beenpublished1618; however, the authorsof these reviews searched the litera-ture only up until October 2005.Hauggaard and Persson,17 the au-thors of the latest published review,included 10 trials testing the efficacyof motor control for acute, subacute,and chronic LBP. The review used asimple descriptive approach to sum-marize the results of each individualtrial. Rackwitz et al18 summarizedthe results of 7 randomized con-trolled trials of acute, subacute, andchronic LBP, and although they useda better approach to summarize theavailable evidence, no meta-analytical analysis with pooling ofthe data was used. Ferreira et al16
summarized the results of 13 ran-domized controlled trials of recur-rent, acute, subacute, and chronicLBP and cervical pain. This reviewwas the only one that included ameta-analytical approach; however,only a few trials were pooled, limit-ing the generalization of the re-sults. A meta-analytical approach issuperior to the other forms of analy-sis for systematic reviews because itprovides a treatment effect size with95% confidence interval (CI).
Consistent with the Cochrane Col-laboration,19 we felt that an updatedreview incorporating new random-ized controlled trials would make auseful contribution to the literature.In addition, a meta-analytical ap-proach, which has not been widelyused in the previous published sys-tematic reviews, can potentially adduseful information about the magni-tude of the effect of motor controlexercises. Because our main interestwas to study persistent LBP andguidelines suggest that persistentand acute LBP should be consideredseparately,1921 we included only tri-als studying patients with LBP thatpersisted beyond the acute phase.
The term persistent low back painis used to describe subacute,chronic, and recurrent pain. Thus,the objective of this study was tosystematically review randomizedcontrolled trials testing the effect ofmotor control exercise in patientswith persistent, nonspecific LBP.
MethodData Sources and SearchesA computerized electronic searchwas performed to identify relevantarticles. The search was conductedon MEDLINE (1950 to June 2008),CINAHL (1982 to June 2008), AMED(1985 to June 2008), PEDro (to June2008), and EMBASE (1988 to June2008). Key words relating to the do-mains of randomized controlled tri-als and back pain were used, as rec-ommended by the Cochrane BackReview Group.19 Terms for motorcontrol and specific stabilizationexercises were extracted from thereview by Ferreira et al.16 Subjectsubheadings and word truncations,according to each database, wereused. There was no languagerestriction.
One reviewer (LGM) screenedsearch results for potentially eligiblestudies, and 2 reviewers (LGM,CGM) independently reviewed arti-cles for eligibility. A third indepen-dent reviewer (JL) resolved any dis-agreement about inclusion of trials.Authors were contacted if more in-formation about the trial was neededto allow inclusion of the study. Re-searchers who published in the areawere contacted to help identify grayliterature and articles in press. Cita-tion tracking was performed usingISI Web of Science, and a manualsearch of the reference lists of previ-ous reviews and the eligible trialswas performed.
Study SelectionThe reviewers followed a researchprotocol, developed prior to the be-ginning of the review, that included
Motor Control Exercise for Persistent, Nonspecific LBP
10 f Physical Therapy Volume 89 Number 1 January 2009
a checklist for inclusion criteria. Ar-ticles were eligible for inclusionif they were randomized or quasi-randomized controlled trials compar-ing motor control exercise with aplacebo treatment, no treatment, oranother active treatment or whenmotor control exercise was added asa supplement to other interventions.When motor control exercise wasused in addition to other treatments,motor control exercises had to rep-resent at least 40% of the total treat-ment program. This criterion wasjudged by reading the description ofthe treatment with the reviewermaking a global yes/no judgment.
Trials were considered to have eval-uated motor control exercise if theexercise treatment was described asmotor control or specific spinal sta-bilization or core stability exerciseand where the protocol describedexercise targeting specific trunkmuscles in order to improve controland coordination of the spine andpelvis.
Randomized or quasi-randomizedcontrolled trials were included ifthey explicitly reported that a crite-rion for entry was nonspecific LBP(with or without leg pain) of at least6 weeks duration (nonacute LBP) orrecurrent LBP. Studies evaluating in-dividuals of all age groups of eithersex were included. Trials were in-cluded if one of the following out-come measures had been reported:pain, disability, quality of life, returnto work, or recurrence.
Data Extraction and QualityAssessmentThe methodological quality of the tri-als was assessed using the PEDroscale,22 with scores extracted fromthe PEDro database. Assessment ofquality of trials in the PEDro databasewas performed by 2 trained inde-pendent raters, and disagreementswere resolved by a third rater.23 Onestudy24 was extracted from a confer-
ence proceeding, and, therefore, thePEDro score was not available inthe database. However, 2 PEDro rat-ers evaluated the information avail-able in the abstract and in an initialversion of a manuscript, and a PEDroscore was given. Methodologicalquality was not an inclusioncriterion.
Three independent reviewers (LGM,CGM, JL) extracted data from eachincluded study using a standardizedextraction form. Mean scores, stan-dard deviations, and sample sizeswere extracted from the studies.When this information was not pro-vided in the trial, the values werecalculated or estimated using meth-ods recommended in the CochraneHandbook for Systematic Reviewsof Interventions.25 When there wasinsufficient information about out-comes to allow data analysis, the au-thors of the study were contacted,and all authors replied to ourinquiries.24,2628
Outcomes were extracted for painand disability for short-termfollow-up (less than 3 monthsafter randomization), intermediatefollow-up (at least 3 months but lessthan 12 months after randomiza-tion), and long-term follow-up (12months or more after randomiza-tion). When there were multipletime points that fell within the samecategory, the one that was closer tothe end of the treatment for theshort-term follow-up, closer to 6months for the intermediate follow-up, and closer to 12 months for thelong-term follow-up was used. Thesereferences for time points werebased on guidelines from the Coch-rane Back Review Group. Scores forpain and disability were converted toa 0 to 100 scale.29
Data Synthesis and AnalysisThe studies were grouped into 4treatment contrasts: (1) motor con-trol versus minimal intervention (no
intervention, general practitionercare, education) or motor control asa supplement, (2) motor control ver-sus spinal manipulative therapy, (3)motor control versus exercise, and(4) motor control versus surgery(lumbar fusion). Results were pooledwhen trials were considered suffi-ciently homogenous with respect toparticipant characteristics, interven-tions, and outcomes. I2 was calcu-lated using RevMan 4.2* to analyzestatistical heterogeneity. I2 describesthe percentage of the variability ineffect estimates that is due to heter-ogeneity rather than sampling error(chance). A value greater than 50%may be considered substantial heter-ogeneity.25 When trials were statisti-cally homogeneous (I250%),pooled effects (weighted mean dif-ference) were calculated using afixed-effect model. When trials werestatistically heterogeneous (I250%)pooled estimates of effect (weightedmean difference) were obtained us-ing a random-effects model.25 Whenthere was a single trial for the com-parison, results were expressed asmean differences and 95% CI.
ResultsStudy SelectionThe initial electronic database searchresulted in a total of 1,052 articles.Of these, 42 were selected as poten-tially eligible based on their title andabstract. Through a Web of Sciencesearch of these articles, 3 other po-tentially eligible articles were identi-fied. A total of 45 potentially eligiblearticles were considered for inclu-sion, with only 14 eligible for inclu-sion in this review (Fig. 1). Reasonsfor exclusion are shown in Figure 1for those articles2,3,15,3057 that wereexcluded from this review. Only 1 ofthe 26 experts contacted sent infor-mation to us on a new trial forinclusion.
* Copenhagen, Denmark: The Nordic Coch-rane Centre, The Cochrane Collaboration,2003.
Motor Control Exercise for Persistent, Nonspecific LBP
January 2009 Volume 89 Number 1 Physical Therapy f 11
A number of randomized controlledtrials that were included in previoussystematic reviews of motor controlexercises were not included in thisreview. Reasons for exclusion in-cluded: patients had acute but notpersistent back pain,15,51,53 patientshad neck pain and headache but notback pain,58 the trial did not use amotor control intervention accord-ing to our review definition,56 and
the trial did not have the outcomesof interest.59,60 Four new tri-als13,24,26,61 that were not included inany of the previously published re-views were included in this review,accounting for the addition of 560patients.
Methodological QualityThe methodological quality assess-ment using the PEDro scale revealed
a mean score of 6 (range28).Blinding of the therapist and blind-ing of the subject were not used inany of the trials, as would be ex-pected for an exercise therapy study.An intention-to-treat analysis wasused in 36% of the trials, and alloca-tion concealment was present in58% of the trials. One of the articles24
included in the review was from aconference proceeding, and, there-
Figure 1.Flow chart of systematic review inclusion and exclusion. RCTrandomized controlled trial.
Motor Control Exercise for Persistent, Nonspecific LBP
12 f Physical Therapy Volume 89 Number 1 January 2009
fore, not much information on theconduct of the trial was available.With the limited information avail-able, this trial received a score of 2on the PEDro scale and was the onlytrial that was a quasi-randomizedcontrolled trial.24
Study CharacteristicsThe 14 randomized controlled trialsincluded in this review comparedmotor control exercise against an-other treatment or against no treat-ment (Tabs. 1 and 2). No placebo-controlled trials were identified.Trials were grouped into 4 treatmentcontrasts: (1) motor control exerciseversus minimal intervention or mo-tor control exercise as a supplement,(2) motor control exercise versusmanual therapy, (3) motor controlexercise versus other forms of exer-cise, and (4) motor control exerciseversus surgery.
Seven trials (603 patients) were in-cluded in the first treatment con-trast: 4 trials (343 patients) that com-pared motor control exercise withminimal intervention (no interven-tion, general practitioner care, or ed-ucation)14,27,62,63 and 3 trials (260 pa-tients) that used motor controlexercise as a supplement to othertreatment (general exercise or usualphysical therapy.28,64,65 Four trials(523 patients) compared motor con-trol exercise with manual therapy(high- or low-velocity trust).13,26,64,66
Five trials (508 patients) comparedmotor control exercise with anotherform of exercise therapy (pain man-agement, general exercises, or theMcKenzie approach).13,24,26,61,67 Onetrial (61 patients) compared motorcontrol exercise with lumbar fusionsurgery.68 The characteristics of themotor control exercise programsthat were evaluated in each trial areprovided in Table 2.
Motor Control Exercise VersusMinimal Intervention or MotorControl Exercise as a SupplementOf the 7 studies included in thistreatment contrast, 4 compared mo-tor control exercise with a minimalintervention program (usual generalpractitioner care or no interven-tion)14,27,62,63 and 3 compared motorcontrol exercise as a supplement toanother intervention versus thisother intervention alone.28,64,65
Methodological quality of the articlesranged from 4 to 8. Data for pain,disability, and quality of life wereavailable for pooling at short-term,intermediate, and long-term follow-up. Data were pooled using arandom-effects model for all compar-isons except for quality of life at in-termediate and long-term follow-ups,where a fixed-effects model wasused because I2 was smaller than50%.
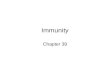
The pooled results favored motorcontrol exercise for pain and disabil-ity outcomes at each follow-up, with4 of the 6 estimates of treatmenteffect being statistically significant.The random-effects model showed astatistically significant decrease inpain favoring motor control exerciseat short-term follow-up (weightedmean difference [on a 0100scale]14.3 points, 95%CI20.4 to 8.1), intermediatefollow-up (weighted mean differ-ence13.6 points, 95% CI22.4 to4.1), and long-term follow-up(weighted mean difference14.4points, 95% CI23.1 to 5.7) andin reducing disability at long-termfollow-up (weighted mean differ-ence10.8 points, 95% CI18.7to 2.8) (Fig. 2). There was no evi-dence that motor control exercisewas effective for improving qualityof life.
Motor Control Exercise VersusManual TherapyFour trials13,26,64,66 compared motorcontrol exercise with manual ther-
apy, with pain and disability out-comes measured at short-term, inter-mediate, and long-term follow-upsand quality of life measured at inter-mediate and long-term follow-ups.The methodological quality of the ar-ticles ranged from 4 to 8. Because I2
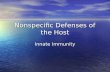
was smaller than 50% for all timepoints, a fixed-effects model wasused to pool the results. The pooledeffects for pain and disability out-comes favored motor control exer-cise, but the effects were alwayssmall and reached statistical signifi-cance for only 2 of the 6 estimates.There was a significant difference be-tween treatment groups favoringmotor control exercise for pain anddisability at intermediate follow-up(weighted mean difference5.7points, 95% CI10.7 to 0.8 forpain and weighted mean differ-ence4.0 points, 95% CI7.6 to0.4 for disability) (Fig. 3). Thepooled estimates of treatment effectson quality of life were small, favoringmotor control exercise at short-termfollow-up and favoring manual ther-apy at long-term follow-up.
Motor Control Exercise VersusOther Forms of ExerciseFive trials13,24,26,61,67 compared mo-tor control exercise with anotherform of exercise therapy. The meth-odological quality of the trials rangedfrom 2 to 8. The trial with a method-ological quality score of 2 had itsPEDro score assessed from a confer-ence proceeding and some informa-tion given by the authors.24 Resultswere pooled for pain and disabilityat short-term, intermediate, and long-term follow-ups. Because I2 wasgreater than 50% for pain at short-term follow-up and for disability atlong-term follow-up, pooled effectsfor these time points were calculatedusing a random-effects model. Allother pooled effects were calculatedusing a fixed-effects model. All esti-mates of treatment effect were small.Five of the 6 estimates favored motorcontrol exercise; however, only one
Motor Control Exercise for Persistent, Nonspecific LBP
January 2009 Volume 89 Number 1 Physical Therapy f 13
Table
1.Detailsof
theInclud
edRa
ndom
ized
Con
trolledTrialsa
Article
PatientCharacteristics,Sample
Size,an
dDurationofComplaint
Interven
tions
Outcomes
(Measure)
PED
roScore
Article
Included
inPreviousReviews
Motorcontrolexercisesversusminim
alinterven
tionormotorcontrolexercisesas
asupplemen
t
Niemisto
etal,62
2003
Patie
ntsrecruitedfrom
adve
rtisem
ent
Age
d24
46y
Mainex
clusioncrite
rion:
neurolog
ical
sign
sor
prio
rba
cksurgery
N20
4Durationof
LBP3mo
Motor
controle
xercises
muscleen
ergy
vsusua
lge
neralp
ractition
ercare
(edu
catio
n)
Pain
(VAS)
Disab
ility
(ODI)
Qua
lityof
life(hea
lth-related
qua
lity
oflife)
8Includ
edin
Ferreira
etal,16
2006
;Ra
ckwitz
etal,1820
06;
andHau
ggaa
rdet
al,1720
07
Koum
antakiset
al,65
2005
Patie
ntsfrom
anorthop
edic
clinic
inaho
spita
land
gene
ral
practition
ers
Mainex
clusioncrite
rion:
prio
rba
cksurgeryor
radiolog
ical
sign
sof
spinal
instab
ility
N55
Durationof
LBP6wk
Motor
controle
xercises
gene
rale
xercises
vsge
neral
exerciseson
ly
Pain
(VAS)
Disab
ility
(RM-24)
7Includ
edin
Ferreira
etal,16
2006
;an
dHau
ggaa
rdet
al,17
2007
OSullivan
etal,14
1997
Patie
ntswith
spon
dylolysisor
spon
dylolisthesis
Age
d16
49y
Mainex
clusioncrite
rion:
neurolog
ical
sign
sor
infla
mmatoryjointdisease
N42
Durationof
LBP3mon
ths
Motor
controle
xercises
vsusua
lgen
eral
practition
ercare
Pain
(sho
rt-form
McG
illVA
S)Disab
ility
(ODI)
7Includ
edin
Ferreira
etal,16
2006
;Ra
ckwitz
etal,1820
06;
andHau
ggaa
rdet
al,1720
07
Stug
eet
al,2820
04Pa
tientsfrom
health
care
practition
ers
Pelvic
girdle
painlateraltoL5
S1
Mainex
clusioncrite
rion:
neurolog
ical
sign
sN81
Durationof
LBP6wk
Motor
controle
xercises
usua
lphy
sicalthe
rapyvs
usua
lphy
sicalthe
rapyon
ly
Pain
(VASpainev
ening)
Disab
ility
(ODI)
7Includ
edin
Ferreira
etal,1620
06
Moseley
,2720
02Pa
tientsfrom
gene
ralp
ractition
ersan
dphy
sicalthe
rapy
clinics
Mainex
clusioncrite
rion:
worsening
neurolog
ical
sign
sN57
Durationof
LBP2mo
Motor
controle
xercises
man
ualthe
rapy
educ
ationvs
usua
lgen
eral
practition
ercare
Pain
(backpainNRS
010
)Disab
ility
(RM-18)
6Includ
edin
Ferreira
etal,16
2006
;an
dRa
ckwitz
etal,18
2006
Shau
ghne
ssyet
al,63
2004
Patie
ntsfrom
orthop
edic
clinics
Age
d20
60y
Mainex
clusioncrite
rion:
neurolog
ical
sign
sor
infla
mmatoryjointdisease
N41
Durationof
LBP3mo
Motor
controle
xercises
vsno
interven
tion
Pain
(SF-36
bodily
pain)
Disab
ility
(RM-24)
Qua
lityof
life(SF-36
gene
ral
health)
5Includ
edin
Hau
ggaa
rdet
al,17
2007
Goldb
yet
al,64
2006
19
Patie
ntsfrom
phy
sicalthe
rapyde
partm
entof
aho
spita
lAge
d18
65y
Mainex
clusioncrite
rion:
neurolog
ical
sign
sor
prio
rba
cksurgery
N12
4Durationof
LBP3wk
Motor
controle
xercises
educ
ationvs
educ
ationon
lyPa
in(backpainNRS
010
0)Disab
ility
(ODI)
Qua
lityof
life(N
othing
ham
Hea
lthProfi
le)
4Includ
edin
Ferreira
etal,16
2006
;an
dHau
ggaa
rdet
al,17
2007
(Con
tinued)
Motor Control Exercise for Persistent, Nonspecific LBP
14 f Physical Therapy Volume 89 Number 1 January 2009
Table
1.Con
tinue
d
Article
PatientCharacteristics,Sample
Size,an
dDurationofComplaint
Interven
tions
Outcomes
(Measure)
PED
roScore
Article
Included
inPreviousReviews
Motorcontrolexercisesversusman
ual
therap
y
Ferreira
etal,1320
07Pa
tientsseekingcare
from
phy
sicalthe
rapyde
partm
ents
ofpub
licho
spita
lsAge
d18
80y
Mainex
clusioncrite
rion:
neurolog
ical
sign
sor
prio
rba
cksurgery
N16
0Durationof
LBP3mo
Motor
controle
xercises
vsspinal
man
ipulativetherap
yPa
in(VAS)
Disab
ility
(RM-24)
8Not
includ
edin
previou
sreview
s
Critch
leyet
al,26
2007
Patie
ntsrecruitedfrom
referralsby
spec
ialists
orprim
ary
care
practition
ersto
phy
sicalthe
rapyde
partm
ents
ofho
spita
lsAge
d18
yor
olde
rWith
orwith
outlegsymptomsor
neurolog
icsign
sMainex
clusioncrite
rion:
prio
rspinal
surgery,
hematolog
icdisease,
orha
dphy
sicalthe
rapyin
thelast
6mo
N14
3Durationof
LBP12
wk
Motor
controle
xercises
vsman
ualthe
rapy
home
exercisesvs
pain
man
agem
entprogram
Pain
(VAS)
Disab
ility
(RM-24)
Qua
lityof
life(EQ-5D)
7Not
includ
edin
previou
sreview
s
Rasm
ussen-Ba
rret
al,6620
03N47
Durationof
LBP6wk
Motor
controle
xercises
vsspinal
man
ipulativetherap
yPa
in(VAS)
Disab
ility
(ODI)
5Includ
edin
Ferreira
etal,16
2006
;an
dRa
ckwitz
etal,18
2006
Goldb
yet
al,6420
06Pa
tientsfrom
phy
sicalthe
rapyde
partm
entof
aho
spita
lAge
d18
65y
Mainex
clusioncrite
rion:
neurolog
ical
sign
sor
prio
rba
cksurgery
N17
3Durationof
LBP3wk
Motor
controle
xercises
educ
ationvs
spinal
man
ipulativetherap
y
educ
ation
Pain
(backpainNRS
010
0)Disab
ility
(ODI)
Qua
lityof
life(N
othing
ham
Hea
lthProfi
le)
4Includ
edin
Ferreira
etal,16
2006
;an
dHau
ggaa
rdet
al,17
2007
Motorcontrolexercisesversusother
form
sofexercise
Ferreira
etal,1320
07Pa
tientsseekingcare
from
phy
sicalthe
rapyde
partm
ents
ofpub
licho
spita
lsAge
d18
80y
Mainex
clusioncrite
rion:
neurolog
ical
sign
sor
prio
rba
cksurgery
N16
0Durationof
LBP3mo
Motor
controle
xercises
vsge
nerale
xercises
Pain
(VAS)
Disab
ility
(RM-24)
8Not
includ
edin
previou
sreview
s
Critch
leyet
al,26
2007
Patie
ntsrecruitedfrom
referralsby
spec
ialists
orprim
ary
care
practition
ersto
phy
sicalthe
rapyde
partm
ents
ofho
spita
lsAge
d18
yor
olde
rWith
orwith
outlegsymptomsor
neurolog
icsign
sMainex
clusioncrite
rion:
prio
rspinal
surgery,
hematolog
ical
disease,
orha
dphy
sicalthe
rapyin
thelast
6mo
N14
1Durationof
LBP12
wk
Motor
controle
xercises
vsman
ualthe
rapy
home
exercisesvs
pain
man
agem
entprogram
Pain
(VAS)
Disab
ility
(RM-24)
Qua
lityof
life(EQ-5D)
7Not
includ
edin
previou
sreview
s
(Con
tinued)
Motor Control Exercise for Persistent, Nonspecific LBP
January 2009 Volume 89 Number 1 Physical Therapy f 15
Table
1.Con
tinue
d
Article
PatientCharacteristics,Sample
Size,an
dDurationofComplaint
Interven
tions
Outcomes
(Measure)
PED
roScore
Article
Included
inPreviousReviews
Klad
nyet
al,6720
03Pa
tientssent
totheou
tpatient
reha
bilitationde
partm
ent
dueto
back
pain
Age
d18
55y
Patie
ntswith
orwith
outradiationor
with
orwith
outdisk
hernia
orprotrusion
Mainex
clusioncrite
ria:prio
rspinal
surgery,
arthritisof
the
joints,injurie
s,or
trau
ma
N99
Suba
cute
andch
ronic
Motor
controle
xercises
gene
rale
xercises
vsge
neral
exercises
man
ualthe
rapy
Pain
(backpainNRS
)Disab
ility
(ODI)
5Includ
edin
Ferreira
etal,16
2006
;Ra
ckwitz
etal,1820
06;
andHau
ggaa
rdet
al,1720
07
Miller
etal,6120
05Pa
tientsfrom
anou
tpatient
phy
sicalthe
rapyclinic
Age
dab
ove18
yMainex
clusioncrite
rion:
morethan
oneba
cksurgeryor
system
icinfla
mmatorydisease
N30
Durationof
LBP7wk
Motor
controle
xercises
vsMcK
enzieap
proach
Pain
(VAS)
Disab
ility
(fun
ctiona
lstatus0
100)
5Not
includ
edin
previou
sreview
s
Stev
enset
al,24
2007
Patie
ntswith
nonspec
ificLB
Pfrom
thephy
sicalm
edicine
andorthop
edic
surgeryde
partm
entof
aho
spita
lAge
d18
65y
Mainex
clusioncrite
ria:spec
ificLB
P,radicu
larsymptoms,
back
surgery,
andne
urolog
icor
system
icco
ndition
N78
Durationof
LBP3moor
recu
rren
t
Motor
controle
xercises
man
ualthe
rapy(10%
)vs
gene
rale
xercises
oftrun
kmusclefunc
tionan
dco
ordina
tion
Pain
(VAS)
Disab
ility
(QBP
DS)
Qua
lityof
life(SF-36
gene
ral
health)
2Not
includ
edin
previou
sreview
s
Motorcontrolexercisesversussurgery
Brox
etal,6820
03Pa
tientsfrom
departm
ents
oforthop
edic
surgery,
neurosurge
ry,phy
sicalm
edicine,
andreha
bilitation
Age
d25
60y
Spinede
gene
ratio
nor
spon
dylosisha
dto
bepresent
Mainex
clusioncrite
rion:
neurolog
ical
sign
sor
prio
rba
cksurgery
N61
Durationof
LBP1y
Motor
controle
xercises
cogn
itive
beha
vioral
therap
yvs
surgery
Pain
(backpain0
100scale)
Disab
ility
(ODI)
Qua
lityof
life(life
satisfactionscale)
8Includ
edin
Ferreira
etal,1620
06
aLB
Plow
back
pain,
ODI
Osw
estryDisab
ility
Inde
x,VA
Svisual
analog
scale,
RM-18
18-item
Roland
-Morris
Disab
ility
Que
stionn
aire,RM
-24
24-item
Roland
-Morris
Disab
ility
Que
stionn
aire,
NRSnu
merical
ratin
gscale,
SF-36
Med
ical
Outco
meStud
y36
-Item
Short-Fo
rmHea
lthSu
rvey
,QBP
DS
Que
becBa
ckPa
inDisab
ility
Scale,
EQ-5DEu
roQol
que
stionn
aire.
Motor Control Exercise for Persistent, Nonspecific LBP
16 f Physical Therapy Volume 89 Number 1 January 2009
Table
2.Detailsof
theMotor
Con
trol
Exercises
Article
DurationofMotor
ControlInterven
tion
ProgressionRule
HomeProgram
Adheren
ceMean(SD)
Feed
back
Brox
etal,6820
035-wkinterven
tion(1
sessionin
thefirst
wee
k,2wkof
homeprogram
,an
dan
othe
r2wkof
trea
tmen
t)Ave
rage
duratio
nwas
abou
t25
hper
wee
k
Not
stated
2wkof
homeprogram
Adh
eren
cewas
3(7)
sessions
per
patient
Not
stated
Critch
leyet
al,26
2007
8sessions
of90
min
Prog
ressionwas
basedon
theab
ility
ofthe
patientsto
maintainastab
lean
dminim
ally
painful
spine.
Theex
ercisesaimed
toim
prove
musclemotor
controltoprovide
dyna
mic
segm
entalstabilityforthelumba
rspine.
Not
stated
Not
stated
Not
stated
Ferreira
etal,13
2007
12sessions
in8wk
Prog
ressionby
inco
rporatingmorefunc
tiona
lposition
san
dtraining
theco
ordina
tionof
all
trun
kmuscles
durin
gthosefunc
tiona
ltasks
Not
stated
Adh
eren
cewas
9.2(3.4)
sessions
per
patient
Real-tim
eultrasou
nd
Goldb
yet
al,6420
061sessionof
112hper
wee
kfor10
wk
Not
stated
Not
stated
Not
stated
Not
stated
Klad
nyet
al,6720
03Not
stated
Not
stated
Not
stated
Stated
only
that
patients
did16
.4(4.8)dof
motor
control
9.5
(3.4)dof
gene
ral
exercises
Real-tim
eultrasou
nd
Koum
antakiset
al,65
2005
2sessions
of30
to45
min
per
wee
kfor8wk
Prog
ressiontowardthego
alof
10co
ntractions
of10
sdu
ratio
n(12
wk).Prog
ressionto
func
tiona
lactivities
whe
npatientswereab
leto:(1)co
ntract
musclein
aspec
ificpattern
and(2)perform
10co
ntractions
of10
sho
lds(35
wk).Hea
vier-lo
adfunc
tiona
ltasks
wereprogressive
lyintrod
uced
inthelast
3wkof
theprogram
.
Hom
eex
ercisesinclud
edAdh
eren
cewas
12.12
(2.69)
sessions
per
patient,an
dho
me
exercisesha
dmed
ianof
23.5
sessions
Tactile
andpressure
cues
Miller
etal,6120
056wk
Trea
tmen
twas
divide
dinto
3pha
ses.
Phase1
goal
was
toperform
10repetition
sof
10-s
holdsin
diffe
rent
position
s.Ph
ase2go
alwas
contractionof
thetran
sversusab
dominisan
dmultifi
dusmuscles
with
load
ingof
thelim
bsin
diffe
rent
position
s.Ph
ase3go
alwas
more
complexload
ingex
ercises.
Patie
ntswereaskedto
perform
approximately10
15min
ofho
meex
ercises
Not
stated
Verbal,tactile,an
dpressurega
uge
Moseley
,2720
022sessions
per
wee
kfor4wk
Not
stated
Stan
dard
homeex
ercises
Not
stated
Not
stated
Niemisto
etal,62
2003
1sessionper
wee
kfor4wk
Prog
ressionwas
perform
edby
instructingthe
patientsto
perform
exercisesin
amore-
func
tiona
lman
neran
dfurthe
rintegrate
them
inda
ilyactiv
ities.
Verbal,visual,
tactile,an
dpressurega
uge
(Con
tinued)
Motor Control Exercise for Persistent, Nonspecific LBP
January 2009 Volume 89 Number 1 Physical Therapy f 17
Table
2.Con
tinue
d
Article
DurationofMotor
ControlInterven
tion
ProgressionRule
HomeProgram
Adheren
ceMean(SD)
Feed
back
OSullivan
etal,14
1997
1sessionper
wee
kfor10
wk
Holding
timeof
exerciseswas
increa
sed
grad
ually,as
wella
sthepressureon
biofee
dbackmon
itor.Goa
lwas
10co
ntractions
of10
-sho
lds.
Furthe
rlow
load
swereap
pliedby
adding
leve
rage
throug
hlim
bs.Whe
naccu
rate
activ
ationof
theco
-co
ntractionpattern
was
achiev
ed,ex
ercises
wereprogressedto
func
tiona
lholding
ofposturesan
dactiv
ities
know
nto
previou
sly
aggrav
atepatients
symptoms.
Patie
ntswereaskedto
doda
ilyex
ercisesof
approximately
101
5min
Patie
ntsco
mpletedada
ilyex
ercisesshee
tto
mon
itorad
herenc
e,bu
tresults
wereno
tpresented
Pressure
gaug
e
Rasm
ussen-Ba
rret
al,6620
031sessionof
45min
per
wee
kfor6wk
Exerciseswereprogressedby
applyinglow
load
tothemusclethroug
hthelim
bsin
diffe
rent
position
s.Pa
tientswereinstructed
inho
wto
useco
ntractionof
themuscles
durin
gactiv
ities
ofda
ilylivingan
din
situations
that
setoffpain.
Patie
ntswereaskedto
doda
ilyex
ercisesof
approximately
101
5min
Not
stated
Tactile
andpressure
gaug
e
Shau
ghne
ssyet
al,63
2004
10sessions
in10
wk
Thisco
nsistedof
two1-h
sessions
durin
gwee
k1,
two
30-m
insessions
durin
gwee
k2,
one30
-min
session
durin
gea
chof
wee
ks3
6,an
don
e30
-min
session
durin
gwee
ks8an
d10
.
Con
tractio
nswerefirst
perform
edwith
thego
alto
achiev
e10
contractions
of10
-sho
lds.
Onc
epatientswereab
leto
perform
sustaine
dco
ntractions
inlow-lo
adpostures,
theregimen
was
progressedby
adding
leve
rage
throug
hlim
bmov
emen
ts.
Patie
ntsperform
edda
ilymainten
ance
exercisesat
home
Not
stated
Verbal,visual,
tactile,an
dpressurega
uge
Stev
enset
al,24
2007
18individu
alsessions
of45
min
in12
wk(2
times
per
wee
kin
thefirst
6wkan
d1
timeper
wee
kin
thene
xt6wk)
Exerciseswerepracticed
indiffe
rent
environm
ents
andco
ntex
tsto
max
imize
tran
sfersto
daily
situations.Th
ephy
sical
therap
istwas
free
toch
oose
thetypeof
exercise
andtheprogression
hefeltmost
suita
bleforindividu
alpatient.Ba
sedon
continuo
usclinical
exam
ination,
the
trea
tmen
tproce
ssco
ntaine
daclea
rlin
eof
progression
achiev
edby
chan
ging
param
eterssuch
asposturalloa
d,redu
ction
ofattentionde
man
ds,redu
ctionof
spee
d,or
additio
nalstrateg
iesto
augm
ent
perform
ance
,with
thefin
algo
alto
obtain
func
tiona
limprove
men
t.
Daily
homeex
erciseswere
enco
urag
ed;ho
wev
er,
adhe
renc
ewas
notassessed
Not
stated
Not
stated
Stug
eet
al,2820
04Se
ssions
of30
to60
min,
3da
ysper
wee
k,for18
to20
wk
First,thefocu
swas
onthespec
ificco
ntraction
ofthetran
sversely
oriented
abdo
minal
muscle.
After
approximately4wk,
load
ing
was
progressive
lyincrea
sed.
Exercisesweremainly
perform
edat
home.
Patie
ntswereen
courag
edto
activ
atethetran
sversus
abdo
minismuscles
regu
larly
durin
gda
ilyactiv
ities.
Adh
eren
cewas
11sessions
per
patient.
80%
ofpatientsdidtheir
exercise
program
3tim
esper
wee
k,either
attheclinic
orat
home.
Not
stated
Motor Control Exercise for Persistent, Nonspecific LBP
18 f Physical Therapy Volume 89 Number 1 January 2009
Figure 2.Forest plot of the results of randomized controlled trials comparing motor control exercises with minimal intervention or motorcontrol exercises as a supplement. Values presented are effect size (weighted mean difference) and 95% confidence interval. Thepooled effect sizes were calculated using a random-effects model except for quality of life at intermediate and long-term follow-ups.
Motor Control Exercise for Persistent, Nonspecific LBP
January 2009 Volume 89 Number 1 Physical Therapy f 19
Figure 3.Forest plot of the results of randomized controlled trials comparing motor control exercises with spinal manipulative therapy. Valuesrepresent effect size (weighted mean difference) and 95% confidence interval. The pooled effect size was calculated using afixed-effect model.
Motor Control Exercise for Persistent, Nonspecific LBP
20 f Physical Therapy Volume 89 Number 1 January 2009
effect was statistically significant.The results showed that motor con-trol exercise was better than otherforms of exercises only for reduc-ing disability at short-term follow-up(weighted mean difference5.1points, 95% CI8.7 to 1.4) (Fig. 4).The results of a single trial26 showedno difference between treatmentgroups for quality of life at short-term follow-up.
Motor Control Exercise VersusSurgeryOnly one study68 compared motorcontrol exercise with surgery, with amethodological quality score of 8.Surgery consisted of lumbar fusionwith transpedicular screws of theL4L5 segments or the L5S1 seg-ments. Brox et al68 found no statisti-cally significant differences for pain(mean difference [on a 0100scale]9 points, 95% CI22.1 to3.5), disability (mean difference
3.3 points, 95% CI12.8 to 6.2),and quality of life (mean difference0.4 points, 95% CI1.6 to 0.8) atthe long-term follow-up (Fig. 5).
DiscussionThis systematic review provides evi-dence that motor control exercise,alone or as a supplement to anothertherapy, is effective in reducing painand disability in patients with persis-tent, nonspecific LBP. We did notfind convincing evidence that motor
Figure 4.Forest plot of the results of randomized controlled trials comparing motor control exercises with other forms of exercise. Valuesrepresent effect size (weighted mean difference) and 95% confidence interval. The pooled effect size was calculated using arandom-effects model for pain at short-term follow-up and for disability at long-term follow-up and using a fixed-effect model forall other comparisons.
Motor Control Exercise for Persistent, Nonspecific LBP
January 2009 Volume 89 Number 1 Physical Therapy f 21
control exercise was superior tomanual therapy, other forms of exer-cise, or surgery.
Figure 2 shows that there was somevariation among studies in the effectsizes for motor control exercise. Fea-tures that could influence the treat-ment effect sizes are characteristicsof the patients (eg, symptom dura-tion), characteristics of treatment im-plementation (eg, program duration,experience of the therapist), and themethodological quality of the trial.Unfortunately, there are too few tri-als to systematically evaluate the ef-fects of these features using tech-niques such as meta-regression.
An intriguing finding of this reviewwas that motor control exercise wasas effective in reducing pain and in-creasing quality of life as a less-complex form of exercise therapythat did not incorporate the retrain-ing of specific muscles that often istime consuming to therapists and pa-tients. When taking in considerationthe results for disability, motor con-trol exercise was more effective thanother forms of exercise only at short-term follow-up, but the point esti-mate was small (5.1 out of 100),showing differences between inter-ventions that may not be clinicallyimportant.
The results of a single trial68 showedthat motor control exercise was notmore effective than surgery. Thisfinding is interesting because bothinterventions target the restoration
of spinal stability, and although spi-nal stability was not directly mea-sured, the findings suggest that themotor control approach is as effec-tive in maintaining stability as an in-vasive intervention that creates sta-bility by fusing the spine. However,this was the finding of a single trial,and more research is needed to con-firm the results.
Although a motor control interven-tion has been shown to reduce pain,it is still unknown whether thesechanges are accompanied by im-provements in measures of motorcontrol. Tsao and Hodges69 haveshown improvements in motor con-trol (anticipatory contraction of thetransversus abdominis muscle duringarm movement) after a single treat-ment session where the isolation ofthe transversus abdominis musclewas trained. In a different trial, Halland colleagues70 did not find thatmotor control (anticipatory contrac-tion of the transversus abdominismuscle during arm movement and awalking task) changed after trainingthe trunk muscles in a nonisolatedmanner. Therefore, the results ofthese 2 studies support the princi-ples of a motor control interventionwhere the isolated training of thedeep trunk muscles is emphasized.However, there has not been a pub-lished randomized controlled trialthat used clinical and physiologicalmeasures to detect improvements inmotor control that can be associatedwith improvements in pain and dis-
ability and the maintenance of thesechanges.
One question that is still to be an-swered is whether individuals withreduced motor control respond bestto this intervention or whether thereare other clinical features that can beused to define a subgroup of patientswho will respond best to this type ofintervention.
A standard protocol and definitionsfor motor control exercise are yet tobe established, and this is reflectedin the wide variation among trials inhow the exercise was named andimplemented (Tab. 2). Although inmost cases OSullivan et al14 and Ri-chardson et al71 were cited as refer-ences, it is apparent from inspectionof the articles that the interventionsin the trials were quite heteroge-neous. There was variation in theduration of the exercise program,progression rule, use of home exer-cise programs, and type of feedbackused with the motor control inter-vention. As an illustration, the pro-gram lasted 10 weeks in the trial byOSullivan et al, whereas the pro-gram lasted 18 to 20 weeks in thetrial by Stuge et al.28 In the trial byFerreira et al,13 ultrasound was usedfor feedback, and Stuge et al28 usedTerapi Master exercise equipment:2 elements missing from the trial byOSullivan and colleagues.
Nordisk Terapi A/S, Kilsund 4290, Staubo,Norway.
Figure 5.Forest plot of the results of a randomized controlled trials comparing motor control exercises with surgery. Values represent meandifference and 95% confidence interval.
Motor Control Exercise for Persistent, Nonspecific LBP
22 f Physical Therapy Volume 89 Number 1 January 2009
Detailed comparison among trials isdifficult because in many trials theauthors did not thoroughly describethe motor control intervention thatwas evaluated. Accordingly, al-though we can conclude from thisreview that motor control exercise isan effective treatment for persistentLBP, the optimal way to implementthis intervention is not yet clear.
When looking at the quality of thetrials included in this review, a meanscore of 6 can be considered a highscore because these trials were exer-cise trials where it is impossible toblind the treatment provider andsubjects, and, therefore, the maxi-mum PEDro score that can beachieved is 8. However, becausesome trials were of lower method-ological quality, they potentiallypresent biased (and overly optimis-tic) estimates of treatment effects.To assess the impact of the lower-quality studies on the review conclu-sions, a sensitivity analysis with ex-clusion of trials with scores lowerthan 524,64 was performed. When thelower-quality studies were deleted,the effect size unexpectedly in-creased slightly for pain and disabil-ity outcomes (we did not conduct asensitivity analysis for quality of lifebecause the exclusion of these trialswould leave only one trial in thetreatment contrast). Therefore, wedo not believe that our conclusionthat motor control exercise is effec-tive (compared with minimal inter-vention or when used as a supple-ment) is an artifact of the inclusionof low-quality trials.
This review not only includes 4 newtrials that were not included in pre-vious reviews, accounting for theaddition of 560 patients, but also al-lowed the use of a meta-analyticalapproach with the inclusion of agreater number of articles into eachtreatment contrast. The pooled re-sults of this systematic reviewshowed smaller and more-precise es-
timates of treatment effects whencompared with the pooled results ofFerreira et al.13 This differenceamong studies can be seen whenlooking, for example, at the motorcontrol exercise versus minimal in-tervention contrast. For this con-trast, Ferreira et al13 included 2 trialsand found an effect of 21 on a 0 to100 scale (95% CI32 to 9) forpain, whereas we found, based on 5trials, an effect of 14.3 (95%CI20.4 to 8.1).
Although it has been only recentlythat reviews of motor control exer-cises have been published, this typeof intervention is widely acceptedand used in the clinical field aroundthe world. Therefore, it is still crucialthat further studies in the area bedeveloped, such as a placebo-controlled trial and trials aiming toidentify subgroups of patients whowill benefit more from a motor con-trol intervention. More fundamentalstudies in LBP to establish reliableand valid clinical assessment tools toidentify deficits in motor control alsoare needed.
ConclusionThe results of this systematic reviewsuggest that motor control exerciseis more effective than minimal inter-vention and adds benefit to anotherform of intervention in reducingpain and disability for people withpersistent LBP. The optimal imple-mentation of motor control exerciseat present is unclear. Future trialsevaluating issues such as dosage pa-rameters, feedback approaches, andeffects in defined subgroups are ahigh priority.
Ms Macedo, Dr Maher, and Dr Latimer pro-vided concept/idea/research design anddata collection. Ms Macedo and Dr Maherprovided writing and data analysis. MsMacedo, Dr Maher, and Dr McAuley pro-vided project management. Dr Latimer pro-vided clerical support and consultation (in-cluding review of manuscript beforesubmission).
Ms Macedo holds a PhD scholarship jointlyfunded by The University of Sydney and theAustralian Government. Dr Mahers researchfellowship is funded by Australias NationalHealth and Medical Research Council.
This article was received April 3, 2008, andwas accepted October 10, 2008.
DOI: 10.2522/ptj.20080103
References1 Hancock MJ, Maher CG, Latimer J, et al.
Systematic review of tests to identify thedisc, SIJ or facet joint as the source oflow back pain. Eur Spine J. 2007;16:15391550.
2 Niemisto L, Rissanen P, Sarna S, et al. Cost-effectiveness of combined manipulation,stabilizing exercises, and physician consul-tation compared to physician consultationalone for chronic low back pain: a pro-spective randomized trial with 2-yearfollow-up [with consumer summary].Spine. 2005;30:11091115.
3 Niemisto L, Sarna S, Lahtinen-Suopanki T,et al. Predictive factors for 1-year outcomeof chronic low back pain following manip-ulation, stabilizing exercises, and physi-cian consultation or physician consulta-tion alone. J Rehabil Med. 2004;36:104109.
4 Panjabi MM. Clinical spinal instability andlow back pain. J Electromyogr Kinesiol.2003;13:371379.
5 Hodges PW, Richardson CA. Delayed pos-tural contraction of transversus abdominisin low back pain associated with move-ment of the lower limb. J Spinal Disord.1998;11:4656.
6 Hodges PW, Richardson CA. Relationshipbetween limb movement speed and asso-ciated contraction of the trunk muscles.Ergonomics. 1997;40:12201230.
7 MacDonald D, Moseley GL, Hodges PW.The function of the lumbar multifidus inunilateral low back pain. Presented at:World Congress of Low Back and PelvicPain; 2004; Melbourne, Australia.
8 Moseley GL, Hodges PW, Gandevia S.Deep and superficial fibers of the lumbarmultifidus muscle are differentially activeduring voluntary arm movements. Spine.2002;27:E29E36.
9 Hodges PW, Richardson CA. Inefficientmuscular stabilisation of the lumbar spineassociated with low back pain: a motorcontrol evaluation of transversus abdomi-nis. Spine. 1996;21:26402650.
10 Hides JA, Stokes MJ, Saide M, et al. Evi-dence of lumbar multifidus muscle wast-ing ipsilateral to symptoms in patientswith acute/subacute low back pain. Spine.1994;19:165177.
11 Roy SH, DeLuca CJ, Casavant DA. Lumbarmuscle fatigue and chronic low back pain.Spine. 1989;14:9921001.
12 Alaranta H, Tallroth K, Soukka A, et al. Fatcontent of lumbar extensor muscles inlow back disability: a radiographic andclinical comparison. J Spinal Disord.1993;6:137140.
Motor Control Exercise for Persistent, Nonspecific LBP
January 2009 Volume 89 Number 1 Physical Therapy f 23
13 Ferreira ML, Ferreira PH, Latimer J, et al.Comparison of general exercise, motorcontrol exercise and spinal manipulativetherapy for chronic low back pain: a ran-domized trial. Pain. 2007;131:3137.
14 OSullivan PB, Phyty GD, Twomey LT,et al. Evaluation of specific stabilizing ex-ercise in the treatment of chronic lowback pain with radiologic diagnosis ofspondylolysis or spondylolisthesis. Spine.1997;22:29592967.
15 Hides JA, Richardson CA, Jull GA. Multifi-dus muscle recovery is not automatic afterresolution of acute, first-episode low backpain. Spine. 1996;21:27632769.
16 Ferreira PH, Ferreira ML, Maher CG, et al.Specific stabilisation exercise for spinaland pelvic pain: a systematic review. AustJ Physiother. 2006;52:7988.
17 Hauggaard A, Persson A. Specific spinalstabilisation exercises in patients with lowback pain: a systematic review. Phys TherRev. 2007;12:233248.
18 Rackwitz B, de Bie R, Limm H, et al. Seg-mental stabilizing exercises and low backpain. What is the evidence? A systematicreview of randomized controlled trials.Clin Rehabil. 2006;20:553567.
19 Bombardier C, van Tulder MW, Pennick V,et al. Cochrane Back Group. About theCochrane Collaboration (Cochrane Re-view Groups [CRGs]). 2006:4.
20 Airaksinen O, Brox JI, Cedraschi C, et al.Chapter 4: European guidelines for themanagement of chronic nonspecific lowback pain. Eur Spine J. 2006;15(Suppl2):S192S300.
21 van Tulder MW, Becker A, Bekkering T,et al. Chapter 3: European guidelines forthe management of acute nonspecific lowback pain in primary care. Eur Spine J.2006;15(Suppl 2):S169S191.
22 Maher CG, Sherrington C, Herbert RD,et al. Reliability of the PEDro scale for rat-ing quality of randomized controlled trials.Phys Ther. 2003;83:713721.
23 Sherrington C, Herbert RD, Maher C, et al.PEDro: a database of randomised con-trolled trials and systematic reviews inphysiotherapy. Man Ther. 2000;5:223226.
24 Stevens V, Crombez G, Parlevliet T, et al.The effectiveness of specific exercise ther-apy versus device exercise therapy in thetreatment of chronic low back pain pa-tients. In: Proceedings of the 6th Interdis-ciplinary World Congress of Low Back andPelvic Pain; 2007; Barcelona, Spain; 2007:177.
25 Higgins J, Green S. Cochrane Handbookfor Systematic Reviews of Interventions4.2.6 [updated September 2006]. In: TheCochrane Library, issue 4, 2006. Chiches-ter, United Kingdom: John Wiley & SonsLtd; 2006.
26 Critchley DJ, Ratcliffe J, Noonan S, et al.Effectiveness and cost-effectiveness ofthree types of physiotherapy used to re-duce chronic low back pain disability: apragmatic randomized trial with eco-nomic evaluation [with consumer summa-ry]. Spine. 2007;32:14741481.
27 Moseley L. Combined physiotherapy andeducation is efficacious for chronic lowback pain. Aust J Physiother. 2002;48:297302.
28 Stuge B, Laerum E, Kirkesola G, et al. Theefficacy of a treatment program focusingon specific stabilizing exercises for pelvicgirdle pain after pregnancy: a randomizedcontrolled trial. Spine. 2004;29:351359.
29 van Tulder MW, Furlan A, Bombardier C,et al. Updated method guidelines for sys-tematic reviews in Cochrane Collabora-tion Back Review Group. Spine. 2003;28:12901299.
30 Bendix AF, Bendix T, Lund C, et al. Com-parison of three intensive programs forchronic low back pain patients: a prospec-tive, randomized, observer-blinded studywith one-year follow-up. Scand J RehabilMed. 1997;29:8189.
31 Bentsen H, Lindgarde F, Manthorpe R. Theeffect of dynamic strength back exerciseand/or a home training program in 57-year-old women with chronic low backpain: results of a prospective randomizedstudy with a 3-year follow-up period.Spine. 1997;22:14941500.
32 Cambron JA, Gudavalli MR, Hedeker D,et al. One-year follow-up of a randomizedclinical trial comparing flexion distractionwith an exercise program for chronic low-back pain. J Altern Complement Med.2006;12:659668.
33 Friedrich M, Gittler G, Halberstadt Y, et al.Combined exercise and motivation pro-gram: effect on the compliance and levelof disability of patients with chroniclow back paina randomized controlledtrial. Arch Phys Med Rehabil. 1998;79:475487.
34 Frost H, Lamb SE, Doll HA, et al. Random-ised controlled trial of physiotherapy com-pared with advice for low back pain. BMJ.2004;329:708713.
35 Gudavalli MR, Cambron JA, McGregor M,et al. A randomized clinical trial and sub-group analysis to compare flexion-distraction with active exercise forchronic low back pain. Eur Spine J.2006;15:107082.
36 Helewa A, Goldsmith CH, Lee P, et al.Does strengthening the abdominal mus-cles prevent low back pain: a randomizedcontrolled trial. J Rheumatol. 1999;26:18081815.
37 Koes BW, Bouter LM, van Mameren H,et al. The effectiveness of manual therapy,physiotherapy, and treatment by the gen-eral practitioner for nonspecific back andneck complaints: a randomized clinical tri-al. Spine. 1992;17:2835.
38 Lie H, Frey S, Lie H, et al. Mobilizing orstabilizing exercise in degenerative diskdisease in the lumbar region? [in Norwe-gian]. Tidsskrift for Den Norske Laege-forening. 1999;119:20512053.
39 Mannion AF, Muntener M, Taimela S, et al.Comparison of three active therapies forchronic low back pain: results of a ran-domized clinical trial with one-year follow-up. Rheumatology. 2001;40:772778.
40 Nelson BW, OReilly E, Miller M, et al. Theclinical effects of intensive, specific exer-cise on chronic low back pain: a con-trolled study of 895 consecutive patientswith 1-year follow up. Orthopedics. 1995;18:971981.
41 Shaughnessy A. Can a specific exerciseprogram combined with brief counselingby a physical therapist offer benefits overusual care? Evidence-Based Practice.1999;2:12.
42 Suni J, Rinne M, Natri A, et al. Control ofthe lumbar neutral zone decreases lowback pain and improves self-evaluatedwork ability: a 12-month randomized con-trolled study. Spine. 2006;31:E611E620.
43 Timm KE. A randomized-control study ofactive and passive treatments for chroniclow back pain following L5 laminectomy.J Orthop Sports Phys Ther. 1994;20:276286.
44 Freburger JK, Carey TS, Holmes GM, et al.Effectiveness of physical therapy for themanagement of chronic spine disorders: apropensity score approach. Phys Ther.2006;86:381394.
45 Hicks GE, Fritz JM, Delitto A, et al. Prelim-inary development of a clinical predictionrule for determining which patients withlow back pain will respond to a stabiliza-tion exercise program. Arch Phys Med Re-habil. 2005;86:17531762.
46 Kasai R. Current trends in exercise man-agement for chronic low back pain: com-parison between strengthening exerciseand spinal segmental stabilization exer-cise. J Phys Med Sci. 2006;18:97105.
47 Ljungkvist I, Ljungkvist I. Short- and long-term effects of a 12-week intensive func-tional restoration programme in individu-als work-disabled by chronic spinal pain.Scand J Rehabil Med Suppl. 2000;40:114.
48 Weinhardt C, Heller KD, Weh L, et al.Non-operative treatment of chronic lowback pain: specific back muscular strengthtraining versus improvement of physicalfitness. Zeitschrift fur Orthopadie undIhre Grenzgebiete. 2001;139:490495.
49 Koumantakis GA, Watson PJ, Oldham JA,et al. Supplementation of general endur-ance exercise with stabilisation trainingversus general exercise only: physiologicaland functional outcomes of a randomisedcontrolled trial of patients with recurrentlow back pain. Clin Biomech. 2005;20:474482.
50 Stuge B, Veierod MB, Laerum E, et al. Theefficacy of a treatment program focusingon specific stabilizing exercises for pelvicgirdle pain after pregnancy: a two-yearfollow-up of a randomized clinical trial.Spine. 2004;29:E197E203.
51 Cairns MC, Foster NE, Wright C, et al. Ran-domized controlled trial of specific spinalstabilization exercises and conventionalphysiotherapy for recurrent low backpain. Spine. 2006;31:E670E681.
52 Gagnon LH. Efficacy of Pilates Exercisesas Therapeutic Intervention in TreatingPatients With Low Back Pain [disserta-tion]. Knoxville, TN: University of Tennes-see; 2005:119.
Motor Control Exercise for Persistent, Nonspecific LBP
24 f Physical Therapy Volume 89 Number 1 January 2009
53 Hides JA, Jull GA, Richardson CA. Long-term effects of specific stabilizing exer-cises for first-episode low back pain.Spine. 2001;26:E243E248.
54 Aure OF, Nilse JH, Vasseljen O. Manualtherapy and exercise therapy in patientswith chronic low back pain. Spine.2003;28:525532.
55 Monticone M, Barbarino A, Testi C, et al.Symptomatic efficacy of stabilizing treat-ment versus laser therapy for sub-acutelow back pain with positive tests for sac-roiliac dysfunction: a randomized clinicalcontrolled trial with 1-year follow-up. Eu-ropa Medicophysica. 2004;40:263268.
56 Lewis JS, Hewitt JS, Billington L, et al. Arandomized clinical trial comparing twophysiotherapy interventions for chroniclow back pain. Spine. 2005;30:711721.
57 Riipinen M, Niemisto L, Lindgren KA, et al.Psychosocial differences as predictors forrecovery from chronic low back pain fol-lowing manipulation, stabilizing exercisesand physician consultation or physicianconsultation alone. J Rehabil Med. 2005;37:152158.
58 Jull GA, Trott P, Potter H, et al. A random-ized controlled trial of exercises and ma-nipulative therapy for cervicogenic head-ache. Spine. 2002;27:18351843; discus-sion 1843.
59 Danneels LA, Cools AM, VanderstraetenGG, et al. The effects of three differenttraining modalities on the cross-sectionalarea of the paravertebral muscles. ScandJ Med Sci Sports. 2001;11:335341.
60 Danneels LA, Vanderstraeten GG, CambierDC, et al. Effects of three different trainingmodalities on the cross-sectional area ofthe lumbar multifidus muscle in patientswith chronic low back pain. Br J SportsMed. 2001;35:186191; comment in 2001;35:186191.
61 Miller ER, Schenk RJ, Karnes JL, et al. Acomparison of the McKenzie approach toa specific spine stabilization program forchronic low back pain. Journal of Man-ual and Manipulative Therapy. 2005;13:103112.
62 Niemisto L, Lahtinen-Suopanki T, RissanenP, et al. A randomized trial of combinedmanipulation, stabilizing exercises, andphysician consultation compared to phy-sician consultation alone for chronic lowback pain. Spine. 2003;28:21852191.
63 Shaughnessy M, Caulfield B, ShaughnessyM, et al. A pilot study to investigate theeffect of lumbar stabilisation exercisetraining on functional ability and quality oflife in patients with chronic low backpain. Int J Rehabil Res. 2004;27:297301.
64 Goldby LJ, Moore AP, Doust J, et al. A ran-domized controlled trial investigating theefficiency of musculoskeletal physiother-apy on chronic low back disorder. Spine.2006;31:10831093.
65 Koumantakis GA, Watson PJ, Oldham JA.Trunk muscle stabilization training plusgeneral exercise versus general exerciseonly: randomized controlled trial of pa-tients with recurrent low back pain. PhysTher. 2005;85:209225.
66 Rasmussen-Barr E, Nilsson-Wikmar L,Arvidsson I, et al. Stabilizing training com-pared with manual treatment in sub-acuteand chronic low-back pain. Man Ther.2003;8:233241.
67 Kladny B, Fischer FC, Haase I, et al. Eval-uation of specific stabilizing exercise inthe treatment of low back pain and lumbardisk disease in outpatient rehabilitation.Zeitschrift fur Orthopadie und Ihre Gren-zgebiete. 2003;141:401405.
68 Brox JI, Srensen R, Friis A, et al. Random-ized clinical trial of lumbar instrumentedfusion and cognitive intervention and ex-ercise in patients with chronic low backpain and disc degeneration. Spine. 2003;28:19131921; comment in 2004;29:19131921.
69 Tsao H, Hodges PW. Immediate changes infeedforward postural adjustment follow-ing voluntary motor training. Exp BrainRes. 2007;181:537546.
70 Hall L, Tsao T, MacDonald D, et al. Imme-diate effects of co-contraction training onmotor control of the trunk muscles in peo-ple with recurrent low back pain. J Elec-tromyogr Kinesiol. 2007 Nov 21 [Epubahead of print].
71 Richardson CA, Jull GA, Hodges PW. Ther-apeutic Exercise for Spinal SegmentalStabilization in Low Back Pain. Edin-burgh, Scotland: Churchill Livingstone;1999.
Motor Control Exercise for Persistent, Nonspecific LBP
January 2009 Volume 89 Number 1 Physical Therapy f 25