




Robert O. Bonow, MD, MS
No Relationships to Disclose
Northwestern University Feinberg School of Medicine
Bluhm Cardiovascular Institute
Northwestern Memorial Hospital
Management of
Valvular Heart Disease
2016


www.acc.org
www.americanheart.org
Evidence-based guidelines?
The majority of recommendations
are Level of Evidence C

Stages of Valvular Heart Disease
Stage
A
B
C
D
Definition
Risk of valve disease
Mild - moderate asymptomatic disease
Severe valve disease but asymptomatic
C1: Normal LV function
C2: Depressed LV function
Severe, symptomatic valve disease

Mitral regurgitation
Degenerative MR: primary valve disease
Functional MR: primary myocardial disease

Mitral regurgitation
Primary mitral regurgitation
Secondary mitral regurgitation

Mitral regurgitation
Primary mitral regurgitation
Secondary mitral regurgitation
Chronic Mitral Regurgitation
Echo findings:
• Dilated left ventricle
• Normal LV systolic function
• Myxomatous leaflets with MVP
• Dilated left atrium
• Normal pulmonary artery pressure
• Severe mitral regurgitation
56 year old healthy man

Chronic Mitral Regurgitation
56 year old healthy man
Issues:
• Surgery?
• Medical therapy?
• Transcatheter repair?

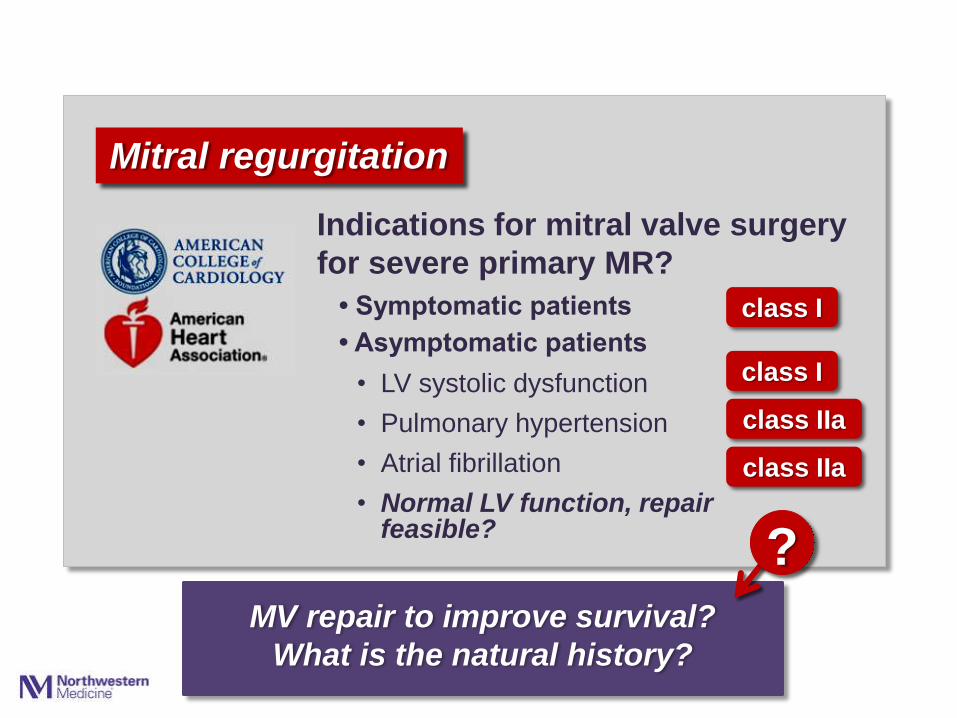
Mitral regurgitation
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
• Atrial fibrillation
• Normal LV function, repair feasible?
?
class I
class I
class IIa
class IIa
Indications for mitral valve surgery
for severe primary MR?
Mitral regurgitation
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
• Atrial fibrillation
• Normal LV function, repair feasible?
class I
class I
class IIa
class IIa
Indications for mitral valve surgery
for severe primary MR?
MV repair to improve survival?
What is the natural history?
?

Mitral regurgitation
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
• Atrial fibrillation
• Normal LV function, repair feasible?
class I
class I
class IIa
class IIa
Indications for mitral valve surgery
for severe primary MR?
66% come to surgery in 5 years because of symptoms,
LV dysfunction, pulmonary hypertension or AF
Asymptomatic severe primary MR:

Mitral regurgitation
• Symptomatic patients
• Asymptomatic patients
• LV systolic dysfunction
• Pulmonary hypertension
• Atrial fibrillation
• Normal LV function, repair feasible?
class I
class I
class IIa
class IIa
Indications for mitral valve surgery
for severe primary MR?
Severe primary MR:
Long-term postoperative survival is worse if surgery
is performed after patients become symptomatic

J Thorac Cardiovasc Surg 2003;125:1143-1152
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11
Mitral Regurgitation Survival After Mitral Valve Surgery
40
20
0
Surv
ival (p
erc
ent)
0 2 4 6 8 10 12
Time (years)
Expected
64%
n=488
p<0.001
Surgery for
Acquired
Cardiovascular
Disease
14
100
80
60
David et al, J Thorac Cardiovasc Surg 2003;126:1143-1152

J Thorac Cardiovasc Surg 2003;125:1143-1152
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11
Mitral Regurgitation Survival After Mitral Valve Surgery
40
20
0
Surv
ival (p
erc
ent)
0 2 4 6 8 10 14 12
Time (years)
David et al, J Thorac Cardiovasc Surg 2003;126:1143-1152
FC I-II
58%
FC III-IV
81%
n=488
p<0.001
Surgery for
Acquired
Cardiovascular
Disease
100
80
60

J Thorac Cardiovasc Surg 2003;125:1143-1152
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11
Mitral Regurgitation Survival After Mitral Valve Surgery
40
20
0
Surv
ival (p
erc
ent)
2 4 6 8 10 20 12
Time (years)
David et al, Circulation 2013;127:1485-1492
FC I
32%
75%
n=840
p<0.001
0 14 16 18
52%
66% 60
80
100
FC IV
FC III
FC II

Mitral regurgitation
class IIa
class I !
Indications for MV repair for
asymptomatic primary MR:
• Repair better than mitral valve replacement
• Patients should be referred to centers experienced in repair
• Chronic severe MR
• Preserved LV function
• Experienced surgical center
• Likelihood of durable repair without residual MR > 95%.


Mitral regurgitation
Primary mitral regurgitation
Secondary mitral regurgitation
• Diagnostic dilemmas
• Therapeutic dilemmas

Imprecision in grading severity of secondary MR
What is “severe”
secondary MR?

0
20
40
60
80
100
1 2 3 4 5 6 7 8
Surv
ival (p
erc
ent)
40
20
0
Grigioni et al. Circulation 2001;103:1759-1764
Time (years)
0 1 2 3 4 5
61%
47%
p<0.001 29%
Survival After MI
MI without MR
100
80
60 ERO 1-19
ERO ≥20

Deja et al. Circulation 2012
p<0.001
0
200
400
600
800
1 2 3 4 5 6 7 8
Ischemic Cardiomyopathy 80
0
Time (years)
0
60
40
20
Mort
alit
y (
perc
ent)
1 2 3 4 5 6
p<0.001
55%
47%
30%
Deja et al. Circulation 2012;125:2639-2648
No MR
Mild MR
Mod-Severe MR

Prevalence of MR in Patients with LV Dysfunction
Prevalence
N MR
Yiu et al Circulation 2000 128 63%
Grigioni et al Circulation 2001 303 64%
Koelling et al Am Heart J 2002 1436 49%
Trichon et al Am J Cardiol 2003 2057 56%
Robbins et al Am J Cardiol 2003 221 59%
Cleland et al N Engl J Med 2004 605 50%
Grayburn et al J Am Coll Cardiol 2005 336 77%
Bursi et al Circulation 2005 303 50%
Acker et al J Thorac CV Surg 2006 300 66%
Di Mauro et al Ann Thorac Surg 2006 239 75%
Rossi et al Heart 2011 1300 74%
Deja et al Circulation 2012 599 63%
Onishi et al Circ Heart Fail 2013 277 48%
Patients with moderate to severe MR *
*
*
*

Secondary mitral regurgitation:
…a marker of a sicker LV
- or -
…a contributor to a sicker LV?

Secondary mitral regurgitation:
…a marker of a sicker LV
- or -
…a therapeutic target?
Therapies that produce beneficial
reverse remodeling also reduce
severity of functional MR

Secondary mitral regurgitation
can be repaired.
But should it be repaired?
… or replaced?
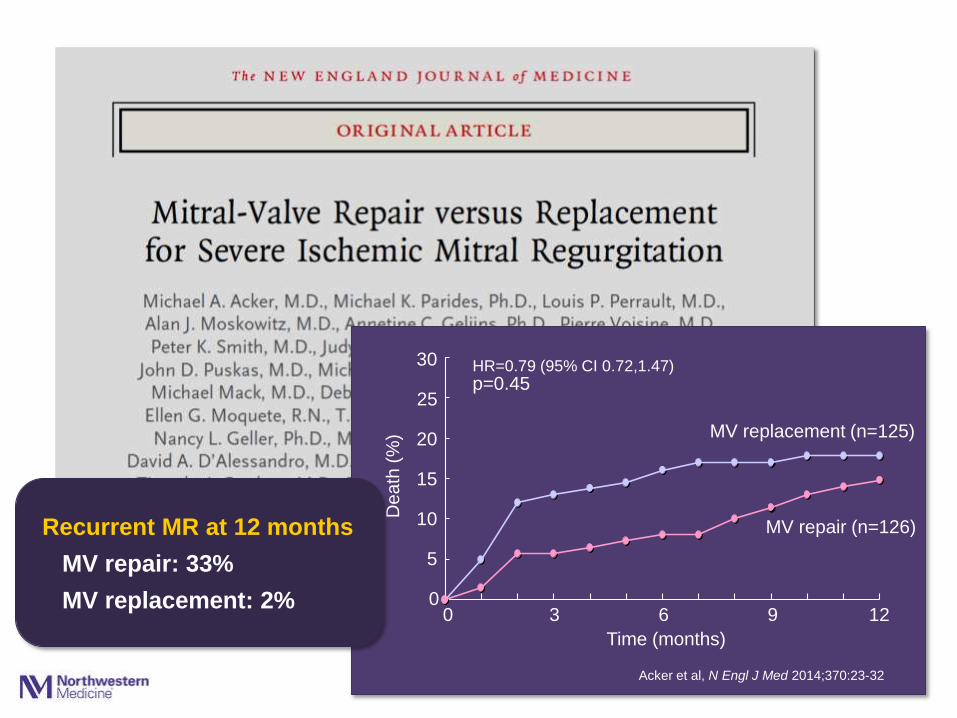
Unlike repair of myxomatous MR,
repair of secondary MR
is often not durable
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8
30
20
15
10
5
0
De
ath
(%
)
Recurrent MR at 12 months
MV repair: 33%
MV replacement: 2% 0 3 6 9 12
Time (months)
Acker et al, N Engl J Med 2014;370:23-32
MV replacement (n=125)
MV repair (n=126)
p=0.45 HR=0.79 (95% CI 0.72,1.47)
25

0
10
20
30
40
50
60
70
80
90
100
0
10
20
30
40
50
60
70
80
90
100100
80
60
40
20
0 LV
En
d-S
ysto
lic V
olu
me In
de
x (
mL
/m2)
LV End-Systolic Volume Index
MV
replacement
MV
repair
MV
repair
MV
replacement
Preop 12 months
Recurrent
MR
No recurrent
MR
p=0.18 p=0.001
Acker et al, N Engl J Med 2014;370:23-32
66 61 61 56 64 47

0
10
20
30
40
1 2 3 4 5 8 Time (months)
Goldstein et al, N Engl J Med 2016;374:344-353
40
30
20
10
0
De
ath
(%
)
0 6 12 18 24
MV replacement (n=125)
MV repair (n=126)
HR=0.79 (95% CI 0.46,1.35) p=0.39

0
100
200
300
400
500
600
700
86 87
0
100
200
300
400
500
600
700
86 87
0
100
200
300
400
500
600
700
86 87
0
100
200
300
400
500
600
700
86 87
70
60
50
40
30
20
10
0
Pe
rce
nt o
f P
atie
nts
Recurrent
MR
Death
No MR
Repair Repair Repair Repair Replace Replace Replace Replace
30 days 6 months 12 months 24 months
30% 38% 45% 46%
5%
9% 12%
Death after
MR


Indications for mitral valve surgery:
• Severe MR, persistent symptoms despite optimal medical therapy, including CRT
class IIb
• Patients with severe MR undergoing CABG or AVR
class IIa
Secondary mitral regurgitation
class I
• Patients with moderate MR undergoing CABG or AVR
class IIb
Guideline-directed medical
therapy for heart failure,
including CRT

Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Data from national Medicare database 1994-1999
684 hospitals
142,488 AVRs
Medicare data
0
2
4
6
8
10
12
14
16
86 87 88 90Age Group (years)
16
0
Pre
vale
nce (
perc
ent)
20-34
10
8
45-54 55-64 65-79 35-44 ≥80
4
Men
Women
6
2
14
12
Prevalence of Heart Failure
United States
Source: NHANES, CDC, and American Heart Association

Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Data from national Medicare database 1994-1999
684 hospitals
142,488 AVRs
Medicare data
0
2
4
6
8
10
12
86 87 88 90Age Group (years)
12
0 50-59
Atrial Fibrillation: Prevalence with Aging
The ATRIA Study
10
8
Go et al, JAMA 2001;285:2370-2375
65-69 75-79 80-84 60-64 70-74 ≥85
4
Men
Women
6
2
n=17,974
Pre
vale
nce (
perc
ent)

0
10
20
30
40
50
60
70
80
90
100
86 87
0
10
20
30
40
50
60
70
80
90
100
86 87
100
80
60
40
20
0
Pe
rce
nt o
f P
atie
nts
Recurrent
AF
Recurrent
AF
Sinus
rhythm
Sinus
rhythm
Baseline Follow-up p=0.005 p=0.72
Severe 36% 29%
71% 64%
Moderate
Mild
18%
18%
64%
19%
19%
57%
5%
Trace/none

Lancet 2006;368:1005-1011
0
1
2
3
4
5
6
7
8
9
10
1 2 3
Perc
ent
Nkomo et al, Lancet 2006;368:1005-1011
7.3
9.6
2
4
8
10
0
Olmstead County (n=16,501)
<45 45-54 55-64 65-74 ≥75
Age
ARIC, CHS, CARDIA (n=11,911)
28,412 subjects
6
Moderate-Severe Mitral Valve Disease

Lancet 2006;368:1005-1011
0
1
2
3
4
5
6
1 2 3
Nkomo et al, Lancet 2006;368:1005-1011
6.0
4.4
4
6
0
Olmstead County (n=16,501)
<45 45-54 55-64 65-74 ≥75
Age
ARIC, CHS, CARDIA (n=11,911)
28,412 subjects
Perc
ent
5
3
1
2
Moderate-Severe Aortic Valve Disease

Aortic Stenosis
Age >60
All patients
Men
Roberts and Ko, Circulation
2005;111:920-925
47% 51%
from Otto and Bonow, Valvular Heart Disease
Braunwald’s Heart Disease, 10th ed, 2014

Stages of Aortic Stenosis
Stage Definition
A Risk of valve disease
B Mild - moderate asymptomatic disease
C Severe valve disease but asymptomatic
C1: Normal LV function
C2: Depressed LV function
D Severe, symptomatic valve disease
D1: High gradient AS
D2: Low gradient, LV dysfunction
D3: Low gradient, normal LV function
BAV, RHD, CVD risk


… the grave prognosis that appears to
accompany the onset of certain symptoms
Ross and Braunwald, Am J Circulation 1968;38:V-61

Ross and Braunwald, Am J Circulation 1968;38:V-61

Circ Cardiovasc Qual Outcomes 2009;2:533-539
0
20
40
60
80
100
0 1 2 3 4
Surv
ival (p
erc
ent)
40
20
0
Bach et al, Circ Cardiovasc Qual Outcomes 2009;2:533-539
0 6 12 18 24 30 36
47%
Time (months)
Aortic Stenosis Survival of Symptomatic Patients
60
80
100

Indications for AVR
• Symptomatic patients with severe AS
Aortic Stenosis
class I

Management challenges:
• The asymptomatic patient with severe AS
• Low-flow, low gradient severe AS
• Indications for TAVR
Aortic Stenosis

Management challenges:
• The asymptomatic patient with severe AS
• Low-flow, low gradient severe AS
• Indications for TAVR
Aortic Stenosis

Aortic stenosis
Indications for valve replacement
Exercise test results:
• Symptoms
• Hypotension
class I
class IIa
Should asymptomatic patients
with severe AS undergo AVR?
…when they are really asymptomatic?

Aortic Stenosis
84 year old man with severe AS
• Watchful waiting?
• More data (more testing)?
• Aortic valve replacement?

Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5
Event-
Fre
e S
urv
ival (%
) 100
80
60
40
20
0 0 1 2 3 4 5
Natural History of Severe Asymptomatic AS
Time (years)
Otto et al. Circulation 1997;95:2262-2270
Rosenhek et al. N Engl J Med 2000;343:611-617
Pellikka et al. Circulation 2005;111:3290-2395
Stewart et al. Eur Heart J 2010;31:2216-2222
Pellikka
Otto
Stewart Rosenhek
Vmax > 4.0 m/s

Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5
Event-
Fre
e S
urv
ival (%
) 100
80
60
40
20
0 0 1 2 3 4 5
Natural History of Severe Asymptomatic AS
Time (years)
Rosenhek et al. N Engl J Med 2000;343:611-617
Moderate or severe calcification
No or mild calcification
n=128
p<0.001

Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5
Event-
Fre
e S
urv
ival (%
) 100
80
60
40
20
0 0 1 2 3 4 5
Natural History of Severe Asymptomatic AS
Time (years)
Vmax 5.0 – 5.5 m/s
Vmax >5.5 m/s
Vmax 4.0 – 5.0 m/s
Rosenhek et al. Circulation 2010;121:151-156
n=198
p<0.001

Management challenges:
• The asymptomatic patient with severe AS
• Low-flow, low gradient severe AS
• Indications for TAVR
What is the risk of death while
waiting for symptoms to trigger AVR?
Aortic Stenosis

Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5
Surv
ival (%
) 100
80
60
40
20
0 0 1 2 3 4 5
Natural History of Severe Asymptomatic AS
Time (years)
Pai et al. Ann Thorac Surg 2006;82:116-122
Kang et al. Circulation 2010;121:1502-1509
Nistri et al. Am J Cardiol 2012;109;718-723
Taniguchi et al. J Am Coll Cardiol 2105;66:2827-2838
Pai
Kang
Nistri
Taniguchi

Average hospital mortality: 8.8%
• Low volume centers: 13.0%
• High volume centers: 6.0%
Medicare data
0
20
40
60
80
100
0 1 2 3 4 5
Surv
ival (%
) 100
80
60
40
20
0 0 1 2 3 4 5
Time (years)
Conservative (n=291)
AVR (n=291)
Taniguchi et al. J Am Coll Cardiol 2105;66:2827-2838
85%
74% Taniguchi
31% of patients who developed
symptoms did not have AVR
17 deaths
Natural History of Severe Asymptomatic AS

class IIb
class IIa
Aortic stenosis
Indications for valve replacement
in asymptomatic patients:
• Very severe AS:
Vmax ≥5 m/s
• Rapid progression and low
surgical risk

Aortic stenosis
The ACC/AHA guidelines have
lowered the threshold for surgery
in asymptomatic patients with AS
• Severity of AS
• Severity of calcification
• Left ventricular function
• Exercise response
• BNP?

Aortic stenosis
…but there needs to be
renewed emphasis on the
class I indications for
surgery in symptomatic
patients with severe AS
The ACC/AHA guidelines have
lowered the threshold for surgery
in asymptomatic patients with AS

Aortic stenosis
Management challenges:
• The asymptomatic patient with severe AS
• Low-flow, low gradient severe AS
• Indications for TAVR

from Pibarot and Dumesnill, J Am Coll Cardiol 2012:60:1845-1853
Diastole
Systole
Normal Flow
High Gradient
Normal LV Function
Low Flow
Low Gradient
LV Dysfunction
Low Flow
Low Gradient
Normal LV Function
Dobutamine
echocardiography
• Valve calcification
• Myocardial strain
• Myocardial fibrosis
• Clinical skillset


Clavel et al, J Am Coll Cardiol
2013;62:2239-2238
Ozkan et al, Nat Review Cardiol
2011;8:494-501
Herrmann et al, J Am Coll Cardiol
2011;58:402-412

class IIa
Low Flow, Low Gradient Aortic Stenosis
Indications for valve replacement:
• Normal EF, if clinical,
hemodynamic and anatomic
data support severe AS

Aortic stenosis
Management challenges:
• The asymptomatic patient with severe AS
• Low-flow, low gradient severe AS
• Indications for TAVR

Indications for TAVR vs surgical AVR:
class I
class IIa
Intervention for Severe AS
• Evaluation by a Heart Team
• Surgical AVR for patients at
low or intermediate risk
• TAVR for patients with
prohibitive surgical risk and
life expectancy >12 months
class I
class I
• TAVR alternative for patients
at high surgical risk

Indications for TAVR vs surgical AVR:
class I
class IIa
Intervention for Severe AS
• Evaluation by a Heart Team
• Surgical AVR for patients at
low or intermediate risk
• TAVR for patients with
prohibitive surgical risk and
life expectancy >12 months
class I
class I
• TAVR alternative for patients
at high surgical risk
?
? class I?
TAVR as alternative?
0
20
40
60
80
100
120
140
160
0
20
40
60
80
100
120
140
160
0
20
40
60
80
100
120
140
160
16
14
12
10
8
6
4
2
0
30-D
ay M
ort
alit
y (
pe
rce
nt)
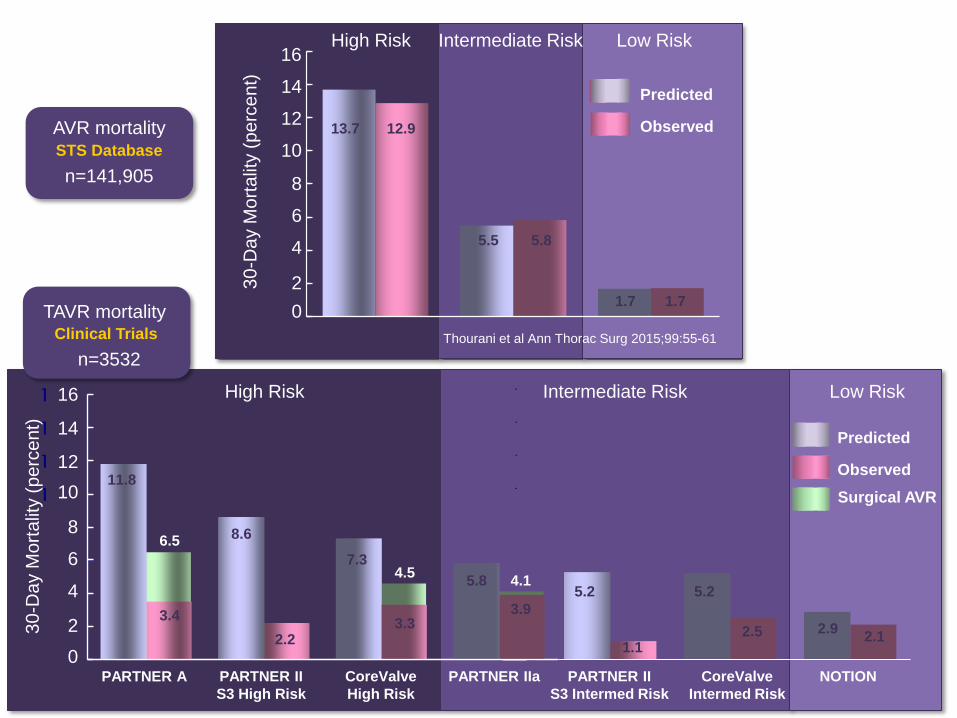
High Risk Intermediate Risk Low Risk
Thourani et al Ann Thorac Surg 2015;99:55-61
1.7
Observed
Predicted
AVR mortality STS Database
n=141,905
Low Risk
TAVR mortality Clinical Trials
Predicted
Observed
5.3
2.5
NOTION
n=3532
Surgical AVR
1.7
12.9
0
20
40
60
80
100
120
140
160
11.8
3.4
8.6
2.2
7.3
3.3
5.2
2.9 2.1
6.5
4.5
30-D
ay M
ort
alit
y (
pe
rce
nt)
16
10
12
8
6
4
0
13.7
5.5 5.8
14
2
PARTNER A PARTNER II
S3 High Risk
CoreValve
High Risk
PARTNER II
S3 Intermed Risk
CoreValve
Intermed Risk
High Risk Intermediate Risk
PARTNER IIa
5.2
1.1
5.8
3.9
4.1

Barreto-Filho et al, JAMA 2013;210:2078-2085
Aortic Valve Replacement Hospital Mortality
Medicare 1999-2011
0
1
2
3
4
5
6
7
8
9
10
0 1 2 3 4 5
30
Da
y A
VR
Mort
alit
y (
perc
en
t)
8
10
6
4
2
0 1999 2001 2003 2005 2007 2009 2011
7.6%
4.2%
Year
Medicare 1999-2011
N=24,900 N=33,441

Barreto-Filho et al, JAMA 2013;210:2078-2085
Aortic Valve Replacement Hospital Mortality
Medicare 1999-2011
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
0 1 2 3 4 5
30
Da
y A
VR
Mort
alit
y (
perc
en
t)
8
14
6
4
2
0 1999 2001 2003 2005 2007 2009 2011
5.9%
12.3%
Year
5.8%
3.3%
12
10
Age 65-74
Age 75-84
Age ≥85
Medicare 1999-2011

TAVR Now
• TAVR has been truly transformative
• Surgical AVR remains the standard with proven
durability and safety for most patients
• TAVR provides treatment options for patients
who previously had no options other than a
predictably very poor short term outcome
• TAVR is an alternative to SAVR in patients at
high surgical risk
• The threshold for TAVR is declining in clinical
trials, registries and clinical practice
• All patients want this

TAVR in the Future
• Judgment of the Heart Team remains essential
in patient selection for TAVR
• Appropriate use criteria and performance
measures are needed to define quality
• Guidelines will need to adapt to the rapidly
evolving TAVR evidence base
TAVR in intermediate and low risk surgical patients
• Availability of TAVR is likely to inform new
indications for valve replacement
Moderate AS in primary cardiomyopathy
Asymptomatic severe AS?
• •

Aortic stenosis is a simple mechanical fault
which, if severe enough, imposes a heavy
burden on the left ventricle and sooner or
later overcomes it.
Wood P, Am J Cardiol 1958;1:553-571





























