KEGAWAT KEGAWAT DARURATAN DARURATAN
KULITKULIT
ERYTHEMA ERYTHEMA MULTIFORMEMULTIFORME
a group of acute self limited
exanthematic intolerance
reaction.
• Von Hebra descriptions EM
associated HSV.
• Steven & Johnson as EM
linked SJS because the same
pathologic, differ only in
severity & term EM minor &
major.
• EM major synonym SJS.
Two main subset
1. EM - a fairly common, usually
mild & relapsing eruption that
is most often triggered by
recurrent HSV infection.
2. SJS - TEN complex an
infrequent severe muco-
cutaneus intolerance
reaction most often elicited
by drugs.
E t i o l o g y
• Triggered by HSV-1 & HSV-2.
• Drugs as rare cause of EM.
P a t h o g e n e s i s
• A cell mediated immune
reaction aimed at the
destruction of keratocytes
expressing HSV antigens.
• EM associated SJS-TEN is
characterized by a dense
dermal inflammatory infiltrate
that is composed chiefly of
CD4+ T lymphocyte &
monocyte the wheal-like
clinical appearance of the
typical target lesion.
Clinical Manifestation
• Lesion appear within 3
days.
• Up to hundred of lesion
may form.

• Symmetric, extensor surfaces
of the extremities & face
(centripetal).
• Less often on palms & soles,
thigh, bottocks & trunk.
• Usually symptomless,
sometimes burning & itching.
• Typically, the lesion is a highly
regular circular, wheal-like
erythematous papule or plaque
that is stable with classic target
as iris lesion.
• Target lesion consist : a
dusky central disk (blister),
more peripherally a ring of
place edema & erythematous
halo.
• Not all lesion are typical.
P a t h o l o g y
• Early :
Lymphocyte accumulation at
the dermal - epidermal
interface with exocytosis into
the epidermis.
Scattered keratinocyte necrosis
with lymph attached to the
necrotic keratinocye (satellite-
cell necrosis).
Spongiosis, vacuolar
degeneration of the basal
layer.
Focal junctional & sub-
epidermal cleft formation.
• Advanced : subepidermal
blister formation & frank
epidermal necrosis.
Differential Diagnosis
• Acute annular urticaria.
• Urticaria vasculitis.
• Disseminated lesion of contact dermatitis.
• Bullous pemphigoid.
• Linear IgA dermatosis.
• Herpes gestationes.
T r e a t m e n t
• Symptomatic : shake lotion,
topical steroid, analgetic &
anti histamin.
• Systemic glucocorticoids :
Unnecessary & possibly
worsened.
• Because recurrent EM most
often by triggered HSV
infection the ideal
approach : prevention of HS
episodes with oral acyclovir
or derivates.

Alternatives Treatment
• Dapsone.
• Anti malaria.
• Azathioprine.
• Thalidomide.
P r o g n o s i s
• Self limited, recovery is
complete & there are no
sequelae.
• Does not occur progression
to SJS-TEN.
• Recurrences are common.

STEVENS-JOHNSON STEVENS-JOHNSON SYNDROMESYNDROME
STEVENS-JOHNSON STEVENS-JOHNSON SYNDROMESYNDROME
Episodic acute mucocutaneous
intolerance reactions most
often elicited by drugs & less
so by infections..
> 50% drug
Minority infections,
vaccination or graft-versus-
host (GVHD)
Etiology
Pathogenesis
Hypersensitivity reaction
III & IV type..
Trias sign :
1. Skin.
2. Mucous-membrane.
3. Eye.
Clinical Feature
It begins nonspecific prodrome :
• Fever • Malaise
• Headache • Rhinitis
• Cough • Sore throat
• Chest pain • Vomiting
• Diarrhea • Myalgia
• Arthralgia.
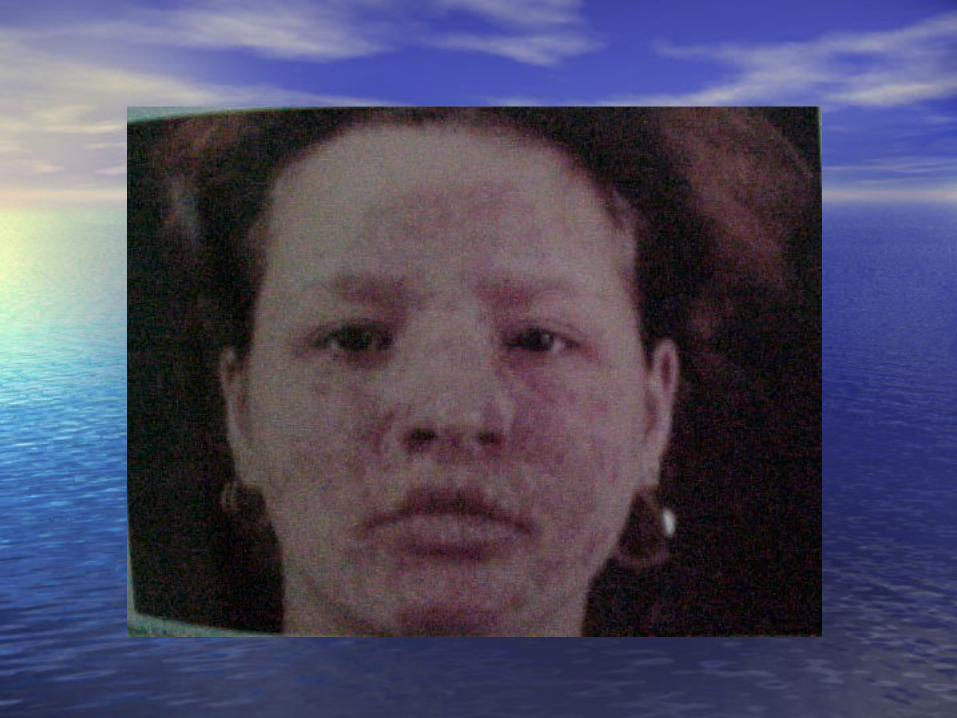
Skin :
• Erythematous (sometimes
morbiliform rash).
• Vesicle.
• Bullous, pustuler rarely..
Mucous membrane :
Two mucous surface minimize
• Lips.
• Oral cavity (palate,
buccal).
• Anogenital..
Sign :
• Erythema.
• Edema followed blister that rupture & transform into extensive.
• Hemorrhagic dull red erosions coated by grayish-white pseudomembrane or shallow aphthous-like ulcers.
Oral lesions painful, cause
eating difficult & hyper-
salivation.
Genital painful hemorrhagic
bullous-erosive or purulent
lesions.
Anal erosi.
Eye : Conjunctiva
• Inflammation & chemosis.
• Vesiculation & painful
erosions.
• Bilateral lacrimation.
• Purulent conjunctivitis with
photophobia &
pseudomembran.
• Corneal ulceration, anterior
uveitis & panophthalmitis.
• Satellite-cell necrosis (early
stages) epidermal
eosinophilic necrosis of the
basal & suprabasal layers
subepidermal separation.
Histopathology
• Mononuclear cell infiltrate
papillary dermis.
• Exocytosis epidermis..
Laboratory
• Blood sedimentation rate .
• Leucocytosis.
• Fluid-electrolyte imbalance.
• Microalbuminuria, hypo-
proteinemia
• Liver transaminase ,
anemia..
Diagnosis
Trias sign :
• Skin, mucous-membrane, eye.
• < 10% or 10 – 30% body
surface area involvement.
Differential Diagnosis
• Erythema multiforme.
• SSSS staphylococcal
epidermolisyn toxynemia
subcorneal acantholysis.
• Macular drug eruption.
• Fixed drug eruption.
• Acute GVHS.
• Viral exanthems.
Complication
Toxicity, dehydration, water &
electrolyte imbalance
hemodynamic shock.
Pulmonary edema, mental
obtusion, confusion, coma &
seizure..
• Skin of heal : hyper and/ or
hypopigmentation.
• Mucosa : scarring.
• Eye :
Symblepharon, synechiae
corneal opacities or
scarring blindness..
Late Complication
• According cause, type, stage & complications.
• Corticosteroid : Not be used routinely. Early stage of drug induced
SJS. Prednisone 1 – 2 mg/kgBB/d
or dexamethasone 4 x 10 mg/d/i.v..
Treatment
• Antibiotic : Prophylactic prevention
infection. According result culture
skin, mucous erosion.e.g. gentamycine 2 x 60 mg < 40 kg body weight, 2 x 80 mg > 40 kg body weight monitoring renal function / week..
• KCl 3 x 500 mg/d K level .
• Monitoring Hm, blood gases
& fluid, electrolytes & protein
balance..
• Supportive care :
Pulmonary care (suctioning,
postural drainage, etc).
Ophthalmologic care.
High-calorie & high protein
diet.
• Topical treatment :
Sofratulle / sulfadiazine
cream.
Kenalog in orabase oral
lesion..
Mortality rate severity
disease & medical care.
Prognosis

TOXIC EPIDERMAL TOXIC EPIDERMAL NECROLYSIS NECROLYSIS
(TEN)(TEN)
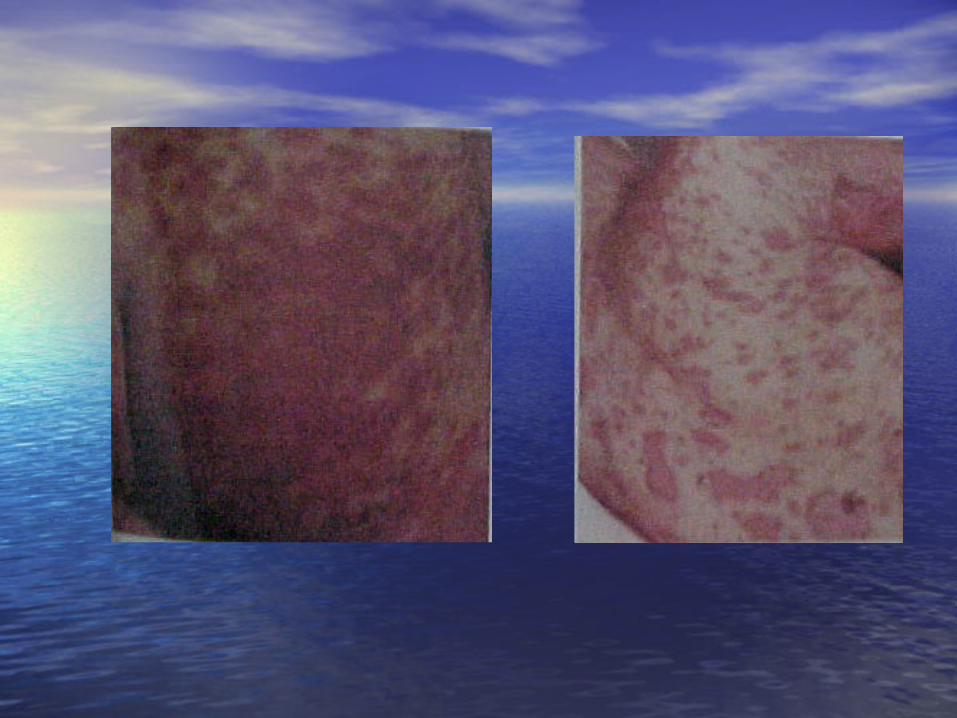
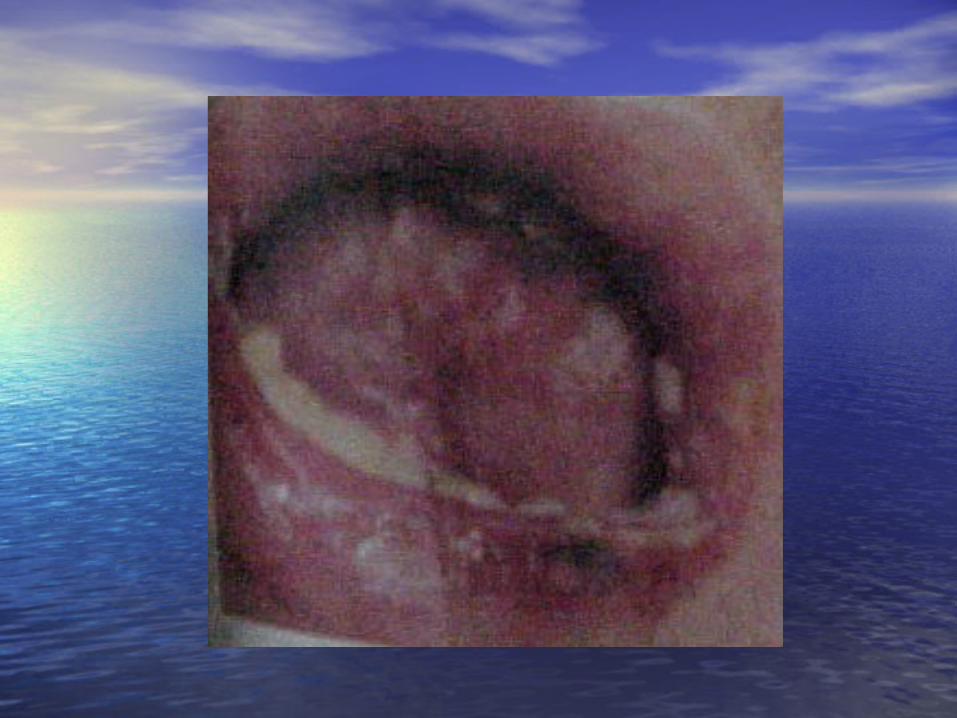
The disease that characterized by:
Rapidly expanding macular rashes of more than one mucosal site.
The rash coalesces to widespread erythema, necrosis, & bullous detachment of the epidermis resembling scalding.
DEFINITION
Drugs (the leading causative
factors).
Infection.
Vaccination.
Graft versus host disease
(GVHD).
ETIOLOGY
It is a polyetiologic reason pattern :
PATHOGENESIS
Cytotoxic immune reaction Cell T (CD4
& % CD8)
TNF α
Inducing apoptosis
destruction of epidermis & keratinocyte
TEN begins with a
nonspecific prodrome of 1
to 14 days in at least half of
patients.
CLINICAL FEATURES
A macular at times morbiliform
rash appears first on the face,
neck, chin, & central trunk
areas & may then spread to the
extremities & the rest of the
body.
The lesions rapidly increase in
numbers & size : maximal
disease expression is usually
reached within 4 to 5 days.
The rash is paralleled or even
preceded by mucous membrane
lesions.
Extra cutaneous symptoms :
Constitutional sign.
Internal organ involvement.
Toxicity, dehydration, &
water & electrolyte
imbalance may proceed to
hemodynamic shock,
pulmonary edema, coma,
etc.

Late complications :
Skin lesions heal with
transitory hyper- and / or
hypopigmentation
Scarring of mucosal lesions,
which is most serious in the
eyes.
A Sjogren like syndrome.
Erythema multiforme with
extensive eosinophilic necrosis
of the epidermis & cleavage
plane above the basement
membrane.
HISTOPATHOLOGY
An elevated blood
sedimentation rate.
Moderate leukocytosis,
anemia.
LABORATORY INVESTIGATIONS
Fluid-electrolyte imbalances,
microalbuminuria, hypo-
proteinemia.
A transient decrease of
peripheral CD4+ T lymphocyte
counts.
Tzank preparations showing
cuboidal cells & skin biopsy can
be used to confirm the
diagnosis.
DIAGNOSIS
Staphylococcal scalded skin
syndrome.
Generalized fixed drug
eruption.
Burns, cauterizations, etc.
Toxic erythroderma.
DIFFERENTIAL DIAGNOSIS
Systemic glucocorticoids 80
to 120 mg of
methylprednisolone per day by
mouth until disease
progression has ceased.
TREATMENT
Prophylactic antibiotic
treatment should be started
right from the beginning.
Sulfonamides & antibiotics with
known sensitizing potential must
be avoided (aminopenicilline,
cephalosporins).
Topical treatment may be
carried out with hydrocolloid or
more conservatively, with
gauze dressing.
Obviously, sulfonamide-
containing topical agents
should be avoided.
Severe morbidity & high
mortality (20-30%).
Death is usually due to :
Sepsis.
Gastrointestinal hemorrhage.
Renal, hepatic or pulmonary
complications.
PROGNOSIS