


Journal of Craniofacial Surgery
Is There A Relationship Between Subjective Pulsatile Tinnitus and Petrous BonePneumatization?--Manuscript Draft--
Manuscript Number: SCS-12-723
Full Title: Is There A Relationship Between Subjective Pulsatile Tinnitus and Petrous BonePneumatization?
Short Title: Subjective Pulsatile Tinnitus and Petrous Bone Pneumatization
Article Type: Original Article
Keywords: subjective pulsatile tinnitus; petrous bone; pneumatization
Corresponding Author: Esra SÖZEN, M.D.Sisli Etfal Training and Research HospitalİSTANBUL, TURKEY
Corresponding Author SecondaryInformation:
Corresponding Author's Institution: Sisli Etfal Training and Research Hospital
Corresponding Author's SecondaryInstitution:
First Author: Esra SÖZEN, M.D.
First Author Secondary Information:
Order of Authors: Esra SÖZEN, M.D.
İrfan ÇELEBİ, M.D.
Yusuf Orhan UÇAL, M.D.
Berna USLU COŞKUN, Ass.Prof
Order of Authors Secondary Information:
Manuscript Region of Origin: TURKEY
Abstract: Our objective was to evaluate the relationship between subjective pulsatile tinnitus andpetrous bone pneumatization. Twenty-five patients admitted between January 2012and March 2012 were assessed. The control group data were obtained by assessmentof petrous bones images of 25 cases in which paranasal sinus computed tomography(CT) was performed because of chronic sinusitis and in which no ear pathology waspresent. Temporal bone CT images of patients with subjective pulsatile tinnitus werecompared with those of patients with no ear complaints. The presence of petrous bonepneumatization was evaluated by CT. Subjective pulsatile tinnitus complaints werepresent for 32 of 50 ears. Pneumatization was detected in the petrous bone of 22(68.8%) of 32 ears with subjective pulsatile tinnitus. In the control group, 25 patients(50 ears) with no ear complaints were assessed. Petrous bone pneumatization wasdetected in 12 (24%) of 50 ears comprising the control group. There was a statisticallysignificant difference between the two groups (p = 0.000 < 0.001). Petrous bonepneumatization might be the cause of the subjective pulsatile tinnitus.
Powered by Editorial Manager® and Preprint Manager® from Aries Systems Corporation

Copyright Transfer and Disclosure Form SÖZENClick here to download Copyright Transfer and Disclosure Form: renamed_b723a.pdf

Copyright Transfer and Disclosure Form ÇELEBİClick here to download Copyright Transfer and Disclosure Form: renamed_6926f.pdf

Copyright Transfer and Disclosure Form UÇALClick here to download Copyright Transfer and Disclosure Form: renamed_5d550.pdf

Copyright Transfer and Disclosure Form COŞKUNClick here to download Copyright Transfer and Disclosure Form: renamed_62630.pdf
Dear Editor
We transfer all copyright ownership of the manuscript ’ Is There A Relationship Between
Subjective Pulsatile Tinnitus and Petrous Bone Pneumatization?’ to The Journal of
Craniofacial Surgery. We warrant that the article is original, does not infringe upon any
copyright or other proprietary right of any third party, is not under consideration by another
journal, and has not been published previously. The authors declare that they have no
potential or actual competing interest. We sign for and accept responsibility for releasing
this material on behalf of any and all authors.
Esra Sozen; wrote the manuscript, design of study
İrfan Çelebi; evaluations of radiological data
Yusuf Orhan Uçal; wrote the manuscript, Collection data
Berna Uslu Coskun; design of study
Dr Esra Sozen takes responsibility for the integrity of the content of the manuscript.
*Cover Letter
1
Is There A Relationship Between Subjective Pulsatile Tinnitus
and Petrous Bone Pneumatization?
Esra Sözen1, İrfan Çelebi2, Yusuf Orhan Uçal1, Berna Uslu Coşkun1
1 Department of Otolaryngology – Head and Neck Surgery; Şişli Etfal Training and
Research Hospital, İstanbul, Türkiye
2 Department of Radiology; Şişli Etfal Training and Research Hospital, İstanbul, Türkiye
Corresponding Author: Esra SÖZEN,
Department of Otolaryngology – Head and Neck Surgery;
Şişli Etfal Training and Research Hospital,34377 Şişli/ İstanbul, Türkiye
Phone: +902123735186, Fax: +902122962264, e-mail: [email protected]
*Manuscript (All Manuscript Text Pages in MS Word format, including Title Page, References and Figure Legends)

2
ABSTRACT
Our objective was to evaluate the relationship between subjective pulsatile tinnitus and petrous
bone pneumatization. Twenty-five patients admitted between January 2012 and March 2012 were
assessed. The control group data were obtained by assessment of petrous bones images of 25 cases
in which paranasal sinus computed tomography (CT) was performed because of chronic sinusitis and
in which no ear pathology was present. Temporal bone CT images of patients with subjective
pulsatile tinnitus were compared with those of patients with no ear complaints. The presence of
petrous bone pneumatization was evaluated by CT. Subjective pulsatile tinnitus complaints were
present for 32 of 50 ears. Pneumatization was detected in the petrous bone of 22 (68.8%) of 32 ears
with subjective pulsatile tinnitus. In the control group, 25 patients (50 ears) with no ear complaints
were assessed. Petrous bone pneumatization was detected in 12 (24%) of 50 ears comprising the
control group. There was a statistically significant difference between the two groups (p = 0.000 <
0.001). Petrous bone pneumatization might be the cause of the subjective pulsatile tinnitus.
3
INTRODUCTION
Tinnitus is the perception of sound in the absence of an acoustic stimulus [1]. The sound can
be in the form of buzzing, ringing, or whistling [2]. Usually, it appears between the ages of 40 and 70
years with an equal frequency in both males and females [3]. It is classified as subjective or objective
and pulsatile or non-pulsatile (continuous) [4]. While subjective tinnitus is heard only by the patient
himself or herself, objective tinnitus describes tinnitus that can also be heard by others apart from
the patient. While pulsatile tinnitus (PT) is a sound heard synchronously with the pulse of the patient,
non-pulsatile tinnitus is an invariable, continuous sound. Subjective PT (SPT) can accompany vascular
pathologies such as traumatic or spontaneous caroticocavernous fistula, arteriovenous
malformation, intracranial aneurysms, vascular tumors of the temporal bone, fibromuscular
dysplasia, and higher jugular bulbus [5-7]. Nonvascular pathologies include myoclonus of the palatal,
stapedius, or tensor tympani muscles [4]. Many tumors and anomalies can also be seen on CT.
Carotid dissection, aneurysms, atherosclerosis, and fibromuscular dysplasia can be recognized on CT,
magnetic resonance imaging (MRI), or magnetic resonance angiographic studies [2]. Some
researchers classify tinnitus with respect to its etiology within the auditory system (cochlear) or
outside the auditory system (extracochlear) [8-10]. Patients can perceive tinnitus as unilateral or
bilateral [9,10].
Cases of temporal pneumatization associated with PT have been described. The aim of this
study was to investigate patients with SPT and evaluate the relationship between temporal
pneumatization and PT.
PATIENTS AND METHODS
Twenty-five patients with PT admitted to our hospital between January 2012 and March
2012 were assessed. A preliminary case history was obtained from all patients. The character and
location of the tinnitus were investigated. Patients with SPT and who had no disease were included.
No pathology was detected in any patient in the otolaryngological examination or the ear, head-
4
neck, or chest auscultation. There were no additional otologic complaints such as otalgia, otorrhea,
vertigo, aural fullness, or lack of hearing. Patients in whom hearing loss was not detected and who
had no history of continuous drug use; head and neck surgery; trauma; chronic systemic disease such
as anemia, hyperthyroidism, or infection; or smoking were included. There was no history of
continuous drug use in any patient with the exception of antihypertensive drugs. The temporal bones
of 25 patients with SPT were assessed radiologically with multi-detector CT (Somatom Sensation 16;
Siemens AG, Erlangen, Germany). The control group data were obtained by retrospective assessment
of the axial and coronal reconstructive images of the petrous bones of 25 patients in whom paranasal
sinus CT was performed because of chronic sinusitis and who had no ear pathology and tinnitus. The
CT acquisition parameters were as follows: tube current, 150 mAs; voltage, 120 kV; detector
collimation, 16 0.75; rotation time, 0.4 s; table speed, 1 mm/rotation (pitch, 0.92); slice thickness, 1
mm; scan time, 1.26 s; FOV, 250; and matrix, 512 512.
To standardize the petrous pneumatization in the assessment of temporal CT, it was
determined whether the area remaining at the anterior aspect of the parallel line drawn on the
anterior acoustic wall of the internal acoustic channel was pneumotized (Fig.1)
Mean, standard deviation, proportion, and frequency were used as descriptive statistics. The
distribution of the data was evaluated with the Kolmogorov-Smirnov test. The independent samples
t-test was used for comparison of the means between two groups. For analysis of proportional data,
the chi-square test was used. SPSS 20.0 was used for the analyses.
RESULTS
Thirteen (52%) of the 25 patients included in the study group were male, and 12 (48%) were
female. The mean age was 47.1 ± 13.5 years. In the control group, 12 (48%) of the 25 patients were
male, and 13 (52%) were female. The mean age was 46.8 ± 12.8 years. There was no statistically
significant difference between the study and control groups in terms of age or gender (p > 0.05).
There was unilateral tinnitus in 18 (72%) of 25 patients with SPT and bilateral tinnitus in 7 (28%).
5
Thirty-two ears of patients with these complaints were assessed. In 11 of 18 patients with unilateral
tinnitus, pneumatization was detected on the same side. There was no increase in pneumatization in
seven of them. There were increases in pneumatization in both ears of five of seven patients with
bilateral tinnitus and one-sided pneumatization in one patient with bilateral tinnitus. No increase in
pneumatization was detected in one patient. Hence, a complaint of SPT was detected in 32 of 50 ears
that were totally assessed. Pneumatization was detected in the petrous bone in 22 (68.8%) of 32 ears
with SPT (Fig.2) In the control group, 25 patients (50 ears) with no ear complaints were assessed.
There was unilateral pneumatization in four patients and bilateral pneumatization in four patients.
Therefore, petrous bone pneumatization was detected in 12 (24%) of 50 ears comprising the control
group. When the study and control groups were compared, there was a statistically significant
difference between them (p = 0.000 < 0.001) (Table 1).
DISCUSSION
SPT is not frequently seen, and it is usually associated with vascular abnormalities [4]. The
essential arterial and venous structures of the head and neck are in the vicinity of the
hypotympanum [11]. The internal carotid artery (ICA) penetrates the temporal bone from the medial
aspect, and it is in the vicinity of the cochlea and middle ear along its destination. The vertical portion
of the carotid channel is localized at the inferior aspect of the cochlea, at the anterior aspect of the
jugular fossa and medial aspect of the tympanic cavity [4]. The large air cells between the ICA and
cochlea act like an amplifier. Increased transmission in the blood flow reaching the cochlea may lead
to PT [12] (Fig.3) Furthermore, the carotid channel is separated from the middle ear by a thin plate.
This channel is usually thinner than 0.5 mm and is completely absent with 1%-ratio [13].
The diagnostic approach for PT starts with symptom investigation and physical examination.
[7]. The accompanying symptoms are very important for an accurate diagnosis. A complete head and
neck examination should be performed. A palpable thrill can be a sign of cervical arteriovenous
malformation [8]. Auscultation of the external ear channel, periauricular region, orbita, neck, and
6
chest have an important role in detecting existing murmurs in patients with objective PT [14].
Audiologic assessment is also valuable to ensure the differential diagnosis.
The first diagnostic examination in SPT is high-resolution temporal bone CT [7,15]. It is
appropriate to perform neck CT with contrast including the superior mediastinum in patients with
normal temporal bone CT results to eliminate the effects of venous compression and atherosclerotic
disease [16]. Angiography is suggested in patients with objective tinnitus and a normal tympanic
membrane. The role of MRI is restricted and secondary [7]. In this study, temporal bone
pneumatization was examined by CT in patients with SPT.
In temporal bone CT examinations in the general population, there are no differences in the
incidence of petrous apex pneumatization. Glick et al. [17] detected pneumatization in 12 (29%) of 42
temporal bones in 1993. When Lindsay et al. [18] studied 100 temporal bone, they detected
pneumotized petrous apex with 21%-ratio in series of sections. Jen et al. [19] reported a 33%
incidence of petrous apex pneumatization. Virapongse et al. [20] found this ratio to be 35% in their
normal temporal bone CT examinations of 141 patients. One study by Jen et al. [19] established a
grading system that assessed the prevalence of petrous pyramidal pneumatization. They stated that
the intrapetrous carotid artery is an appropriate anatomical landmark. In this study, pneumatization
at the medial aspect of a line drawn parallel to the anterior wall of the internal acoustic channel was
assessed. Hence, a standardized line was constituted to determine the aerated area within the
petrous bone.
Tüz et al. [4] detected diffuse pneumatization around the ICA in the temporal bone in the SPT
case that they reported. They related the cause of late initiation of the tinnitus to the decreased
insulation characteristic of the compact bone around the ICA as secondary to the osteoporosis in
older age. Topal et al. [12] also demonstrated diffuse temporal bone aeration in two patients. Yao et
al. [21] detected erosion in the bone between the ICA and the basal turn of the cochlea in the cases
that they reported. In these patients, unilateral SPT was a symptom. They state that because the
7
aberrant position of the ICA can directly conduct regular vibrations from the arterial wall to the
perilymph or endolymph, SPT can occur. In this study, pneumatization was detected in 68.8% of ears
of patients with tinnitus.
Xue et al. [22] suggested that focal field defects at the transverse and sigmoid junctions in
the mastoid bone may be a new cause of PT. They indicated that PT completely regressed following
mastoid reconstruction. Lund et al. [23] showed that carotid artery-cochlear dehiscence can lead to
PT by virtue of CT.
The observation of the diffuse pneumatization around the carotid channel in the case series
in question in this study can explain the presence of the SPT. Particularly, the air cells around the
carotid channel can cause tinnitus by acting as an amplifier. Conduction of the vibrations occurring in
the wall of ICA to the perilymph and endolymph can lead to SPT.
CONCLUSION
PT is a rarely encountered otological symptom. In the assessment of SPT, it is suggested that
diffuse pneumatization of the petrous bone is one etiological factor.
8
REFERENCES
1. Branstetter BF IV, Weissman JL (2006) The radiologic evaluation of tinnitus. Eur Radiol
16(12):2792-802.
2. Weissman JL, Hirsch BE (2000) Imaging of tinnitus: a review.Radiology 216(2):342-9.
3. Vattoth S, Shah R, Curé JK (2010). A compartment-based approach for the imaging evaluation
of tinnitus. Am J Neuroradiol 31(2):211-8.
4. Tüz M, Doğru H, Yeşildağ A (2003) Subjective pulsatile tinnitus associated with extensive
pneumatization of temporal bone. Auris Nasus Larynx 30(2):183-5.
5. Levine SB, Snow JB (1987) Pulsatile tinnitus. Laryngoscope 97:401–406.
6. Sila CA, Furlan AJ, Little JR (1987) Pulsatile tinnitus. Stroke 18:252–256.
7. Remley KB, Coit WE, Harnsberger HR, Smoker WRK, Jacobs JM, McIff EB (1990) Pulsatile
tinnitus and vascular tympanic membrane: CT, MR and angiographic findings. Radiology
174:383–389.
8. Tyler RS, Babin RW (1993) Tinnitus. In: Cummings CW, Frederickson JM, Harker LA, Krause CJ,
Schuller DE, eds. Otolaryngology-head and neck surgery. 2nd ed. St Louis, Mo: Mosby–Year
Book, pp 3031-3053.
9. Nodar RH (1996) Tinnitus reclassified: new oil in an old lamp. Otolaryngol Head Neck Surg
114:582-585.
10. Moller AR (1994) Tinnitus . In: Jackler RK, Brackmann DE, eds. Neurotology. St Louis, Mo:
Mosby–Year Book pp 153-165.
11. Liyanage SH, Singh A, Savundra P, Kalan A (2006) Pulsatile tinnitus. J Laryngol Otol 120(2):93-
97.
12. Topal O, Erbek SS, Erbek S, Ozluoglu LN (2008) Subjective pulsatile tinnitus associated with
extensive pneumatization of temporal bone. Eur Arch Otorhinolaryngol 265(1):123-5.
9
13. Henriksen SD, Kindt MW, Pedersen CB, Nepper-Rasmussen HJ (2000) Pseudoaneurysm of
lateral internal carotid artery in the middle ear. Int. J. Pediatr. Otorhinolaryngol 52 (2):163-
167.
14. Sismanis A (2003) Pulsatile tinnitus. Otolaryngol Clin North Am 36(2):389-402.
15. Hasso AN (1994) Imaging of pulsatile tinnitus: basic examination versus comprehensive
examination package. Am J Neuroradiol 15:879-889.
16. Kang M, Escott E (2008) Imaging of tinnitus. Otolaryngol Clin North Am 41(1):179-93.
17. Glick HN (1933) Microscopic observation of the petrous apex. Ann Otol Rhinol Laryngol
42:175-191.
18. Lindsay JR (1940) Petrous pyramid of temporal bone-pneumatization and roentgenologic
appearance. Arch Otolaryngol 31:231-255.
19. Jen A, Sanelli PC, Banthia V, Victor JD, Selesnick SH (2004) Relationship of petrous temporal
bone pneumatization to the eustachian tube lumen. Laryngoscope 114(4):656-60.
20. Virapongse C, Sarwar M, Bhimani S, Sasaki C, Shapiro R (1985) Computed tomography of
temporal bone pneumatization: 1. Normal pattern and morphology. Am J Roentgenol
145(3):473-81.
21. Yao W, Benjamin LC III, Korzec K (1998) Aberrant internal carotid artery causing erosion of
the otic capsule: an unusual cause of pulsatile tinnitus. Otolaryngol. Head Neck Surg 118:
678–679.
22. Xue J, Li T, Sun X, Liu Y (2012) Focal defect of mastoid bone shell in the region of the
transverse-sigmoid junction: a new cause of pulsatile tinnitus. J Laryngol Otol 7:1-5. [Epub
ahead of print].
23. Lund AD, Palacios SD (2011) Carotid artery-cochlear dehiscence: a review. Laryngoscope
121(12):2658-60.
10
LEGENDS
Figure 1 Legend: Axial high-resolution temporal bone computed tomography passing through the
internal auditory canal. Bilateral symmetric and almost equal pneumatization of the petrous bone.
The black lines represent the posterior border of the petrous bone. CC: Petrous portion of the carotid
canal.
Figure 2 Legend: Axial high-resolution computed tomography scan at the level of the internal
auditory canal. Unilateral petrous bone pneumatization around the carotid canal (CC) is seen on the
left side (arrows). This patient has tinnitus on the left side.
Figure 3 Legend: Coronal high-resolution computed tomography scan. Bilateral asymmetric petrous
bone pneumatization is dominant on the right side. This patient has tinnitus on the right side.

11
Conflicts of Interest and Source of Funding: There is no conflict of interest.
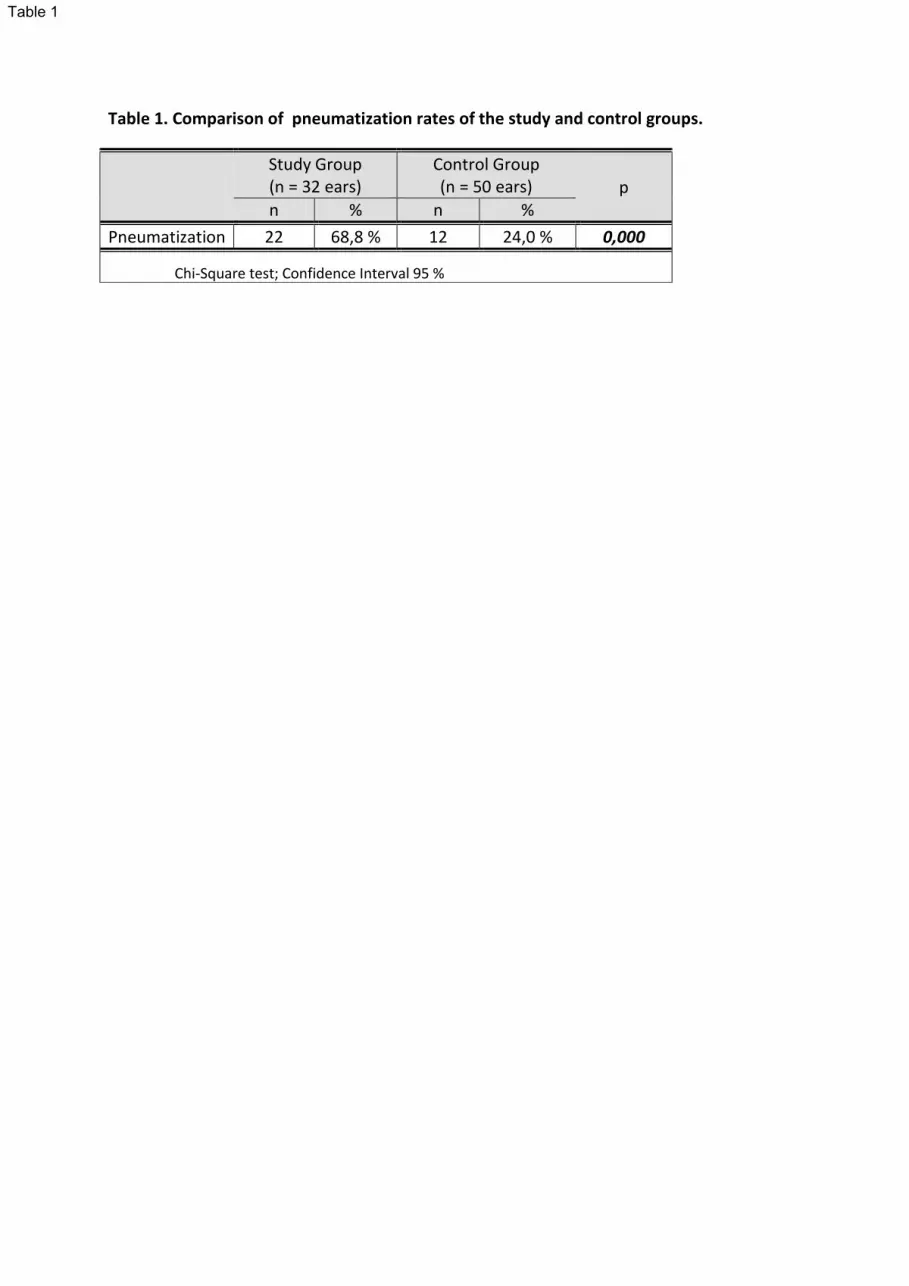
Table 1. Comparison of pneumatization rates of the study and control groups.
Study Group (n = 32 ears)
Control Group (n = 50 ears) p
n % n %
Pneumatization 22 68,8 % 12 24,0 % 0,000
Chi-Square test; Confidence Interval 95 %
Table 1

Figure 1Click here to download high resolution image

Figure 2Click here to download high resolution image
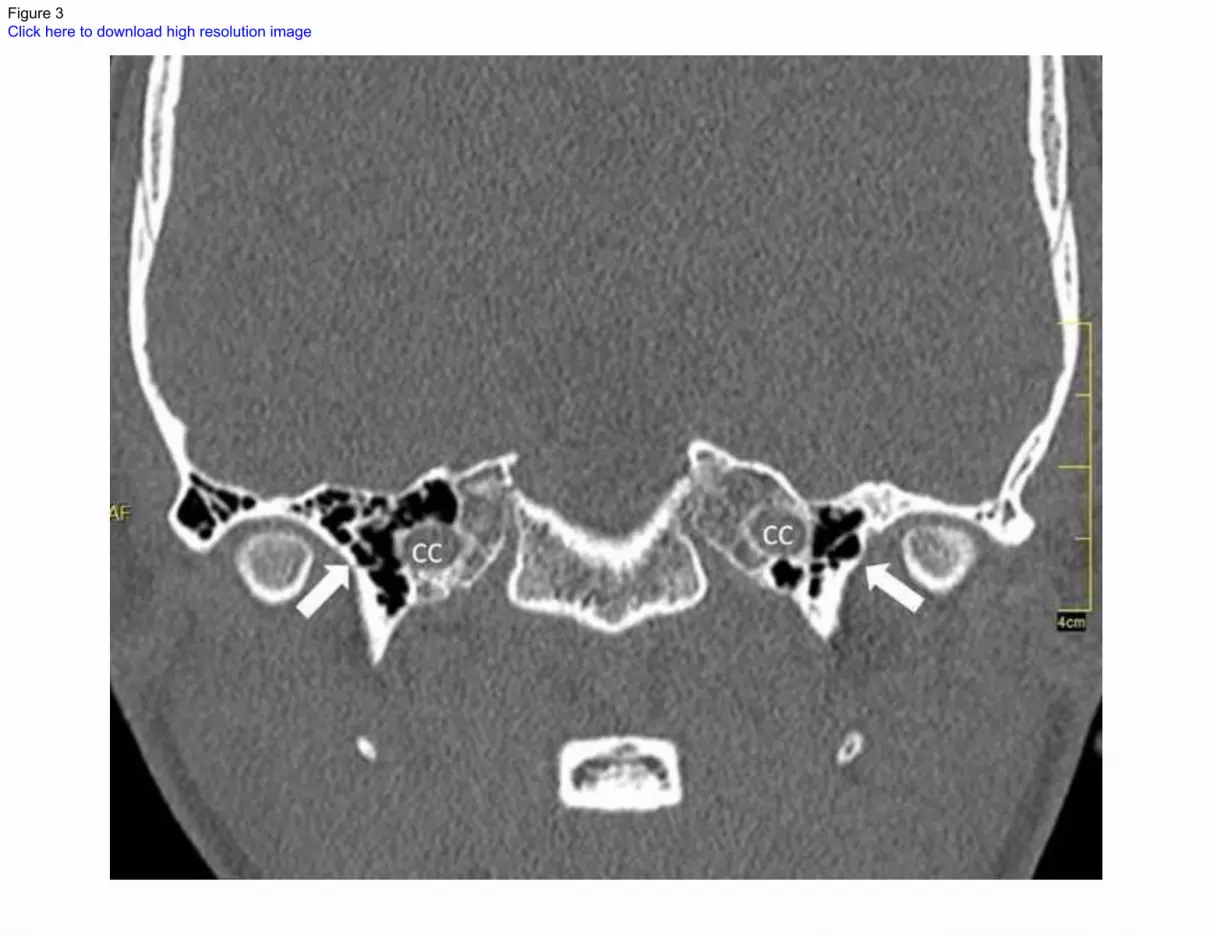
Figure 3Click here to download high resolution image
















![Pulsatile drug delivery system [ppt]](https://static.cupdf.com/doc/110x72/5563b49bd8b42a38198b4cc0/pulsatile-drug-delivery-system-ppt.jpg)













