


Interleukin-17 Induces Expression of Chemokines and Cytokinesin Prostatic Epithelial Cells but Does Not Stimulate Cell GrowthIn Vitro
Zongbing You1,*, Dongxia Ge1, Sen Liu1, Qiuyang Zhang1, Alexander D. Borowsky2, andJonathan Melamed3
1Department of Structural & Cellular Biology, Department of Orthopaedic Surgery, Tulane CancerCenter, Louisiana Cancer Research Consortium, Tulane Center for Stem Cell Research andRegenerative Medicine, Tulane Center for Aging, Tulane University School of Medicine, NewOrleans, Louisiana 70112
2Department of Pathology & Laboratory Medicine and Center for Comparative Medicine,University of California Davis, Davis, California 95616
3Department of Pathology, New York University School of Medicine, New York, New York 10016
Abstract
BACKGROUND—Interleukin-17 (IL-17A) expression is increased in prostate cancer. This study
investigated the expression of IL-17A receptor C (IL-17RC) in prostatic intraepithelial neoplasia
(PIN) lesions and the effects of IL-17A on prostatic epithelial cells in in-vitro studies.
METHODS—IL-17RC expression in human and rodent prostate tissues was detected by
immunohistochemistry. Quantitative real-time reverse-transcription polymerase chain reaction
(qRT-PCR) and Western blot analyses were used to determine mRNA and protein expression in
human and mouse prostatic epithelial cell lines.
RESULTS—IL-17RC protein was increased in human and rodent PIN lesions, compared to the
normal human and rodent prostatic epithelium. IL-17A treatment activated the Nuclear Factor-κB
(NF-κB) and/or Extracellular signal-Regulated Kinase (ERK) pathways in human PIN and LNCaP
cell lines as well as mouse prostate cancer cell line TRAMP-C1. IL-17A treatment did not affect
cell growth of the cell lines studied. However, IL-17A induced expression of CXCL1, CXCL2,
CCL2, CCL5, and IL-6 in human and mouse prostatic epithelial cell lines. When the full-length
IL-17RC was over-expressed in human PIN and LNCaP cell lines, activation of NF-κB and/or
ERK pathways and expression of CXCL1, CXCL2, and CCL5 chemokines were significantly
enhanced upon IL-17A treatment.
CONCLUSION—These findings suggest that the prostatic epithelial cells in PIN lesions may
respond to IL-17A stimuli with augmented synthesis of chemokines, due to increased IL-17RC
expression.
*Correspondence to: Zongbing You, MD, PhD, Department of Structural & Cellular Biology, Tulane University School of Medicine,1430 Tulane Ave SL 49, New Orleans, LA 70112. Fax: 504-988-1687; Tel: 504-988-0467; [email protected].
Conflicts of InterestThe authors have no conflicts of interest in publication of this chapter.
NIH Public AccessAuthor ManuscriptInt J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
Published in final edited form as:Int J Med Biol Front. 2012 ; 18(8): 629–644.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

Keywords
IL-17; PIN; prostate cancer
INTRODUCTION
Almost all surgical prostate specimens contain evidence of inflammation [1–3]. Chronic
inflammation invokes proliferative inflammatory atrophy (PIA) of prostate – a potential
precursor lesion to prostatic intraepithelial neoplasia (PIN) and/or carcinoma [4,5]. The
cause of prostate inflammation includes infection, urine reflux, diet, estrogen, and physical
trauma [6,7]. Normal prostate may contain a small number of T cells, B cells, macrophages,
and mast cells that increase in number with aging [8].
In animal models of prostate cancer, chronic inflammation with T cells was noted in a
significant proportion of the mice with high-grade PIN [9]. When TRAMP mice were fed
with the COX-2 inhibitor celecoxib, only 25% mice developed prostate cancer, compared to
a rate of 100% in control mice without celecoxib treatment. None of the celecoxib-treated
mice had any metastatic tumor, whereas the control mice showed metastasis to the lymph
nodes (65%), lungs (35%) and liver (20%) [10]. This study highlights the role of
inflammation in cancer initiation and progression in this model. Inflammatory cells were
also noted in the PB-Cre4 × Ptenloxp/loxp model at 26–29 weeks of age [11]. At this stage,
more than 80% of the prostate tissue was composed of microinvasive cancer cells and PIN,
with less than 20% of stroma and inflammatory cells. The cancer-dominant mouse prostate
tissues had 3- to 8-fold increase of some cytokines and chemokines such as CXC ligand 1
(CXCL1), C-C ligand 2 (CCL2) and CCL20, compared to the age-matched normal mouse
prostate tissues [11]. In a 2-amino-1-methyl-6-phenylimidazo (4,5-b) pyridine (PhIP)-treated
rat model [12], significantly more inflammation occurred in the PhIP-treated rat prostate
glands than in the controls and inflammation preceded proliferative atrophy and PIN.
In human PIA lesions, over 80% of inflammatory cells are CD3+ T cells, of which most are
CD4+ [4,13,14]. The CD4+ T helper cells are classified into TH1, TH2, and TH17 subtypes.
TH1 cells produce interferon (IFN)-γ and interleukin (IL)-2, while TH2 cells produce IL-4,
IL-5, and IL-13. TH17 is a new subtype that produces IL-17A and IL-17F [15,16]. The
inflammatory cells and the inflammation-stimulated prostatic epithelial and stromal cells
produce a variety of cytokines, chemokines, and growth factors [13,14,17]. It is known that
sequence variants of IL-1β, IL-8, IL-10, tumor necrosis factor (TNF) α and vascular
epithelial growth factor are associated with human prostate cancer risk [18].
IL-17A is a pivotal cytokine that stimulates expression of other cytokines and chemokines
such as TNFα, IL-6, and IL-8 [19–22]. The percentage of TH17 cells in prostate-infiltrating
lymphocytes was higher than that in the peripheral blood, though this TH17 skewing was
inversely correlated with Gleason grade [23]. IL-17A expression is increased in 79% of
benign prostate hyperplasia (BPH) and 58% of prostate cancer specimens [14]. IL-17RA and
IL-17RC are the receptors for IL-17A and IL-17F [24–27]. Both receptors have been found
in prostate cancer [14,28,29]. The full-length IL-17RC protein inhibited TNFα-induced
apoptosis in a human prostate cancer cell line LNCaP [30]. IL-17RC protein expression as
You et al. Page 2
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
detected by the anti-IL-17RC intracellular domain (anti-ICD) antibodies was significantly
increased in castration-resistant prostate cancer, compared to hormone sensitive prostate
cancer [30,31].
In this study, we found that IL-17RC expression was increased in PIN lesions from human,
rat, and mouse prostate tissues. In addition, we found that recombinant human IL-17A acted
through Nuclear Factor-κB (NF-κB) and/or Extracellular signal-Regulated Kinase (ERK)
pathways to stimulate expression of a variety of chemokines and cytokines in prostatic
epithelial cell lines.
MATERIALS AND METHODS
Antibodies and Reagents
Rabbit anti-IL-17RC intracellular domain (anti-ICD) antibodies that recognize an
intracellular domain of IL-17RC protein were affinity-purified [28,30–32]. pERK1/2
antibodies were obtained from Santa Cruz Biotechnology, Santa Cruz, CA. ERK1/2, pIκBα,
IκBα, pAKT (serine 473), and pSTAT3 (Tyr705) antibodies were obtained from Cell
Signaling Technology, Beverly, MA. Mouse anti-glyceraldehyde-3-phosphate
dehydrogenase (GAPDH) antibodies were obtained from Chemicon, Temecula, CA. The
VECTSTAIN elite ABC Reagent and DAB Substrate Kit were obtained from Vector
Laboratories, Burlingame, CA.
Cell Culture
The RWPE-1 [33] and pRNS-1-1 [34] cells (immortalized human prostatic epithelial cell
lines) were cultured in a serum-free keratinocyte medium. The PIN cell line, derived from a
human high-grade PIN lesion [35,36], was cultured in a keratinocyte medium supplemented
with 10% fetal bovine serum (FBS). Human prostate cancer cell line LNCaP and mouse
prostate cancer cell line TRAMP-C1 were obtained from the American Type Culture
Collection (Manassas, VA). The LNCaP cells were cultured in the T-medium (custom
formula # 02-0056) supplemented with 5% FBS. The TRAMP-C1 cells were cultured in
Dulbecco's modified Eagle's medium (DMEM) supplemented with 4.5 g/L glucose, 5 ng/ml
recombinant human insulin, 10 nM R1881 (synthetic androgen), and 10% FBS. The cell
lines over-expressing human full-length IL-17RC (PIN-RC and LNCaP-RC) and the control
cell lines (PIN-C and LNCaP-C, transfected with empty vector) were established as
described previously [30]. Medium and supplements were obtained from Invitrogen,
Carlsbad, CA, unless noted otherwise. The cells were cultured in a 37°C, 5% CO2
humidified incubator.
Immunohistochemical Staining
Sixty of human prostate tissue samples were provided by the New York University Prostate
Cancer Tissue Resource, Department of Pathology, New York University School of
Medicine. The prostate tissues were collected from either radical prostatectomy specimens
or transurethral resection specimens. The tissue sections contained high-grade PIN lesions
that were confirmed by a pathologist (J.M.). The use of these archival tissues was approved
by the Tulane University Institution Review Board.
You et al. Page 3
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

The rat prostate tissues were obtained from a prior study [12]. The age-matched control and
PhIP-treated rat prostate tissues were collected from 45- and 65-week-old rats. The mouse
prostate tissues were collected from 9-week-old TRAMP mice [37] [C57BL/6 background,
strain name C57BL/6-Tg(TRAMP)8247Ng/J, the Jackson Laboratory, Bar Harbor, ME].
Ptenloxp/loxp (PtenL/L) mice [11] (129S4/SvJae*BALB/c background, strain name C;129S4-
Ptentm1Hwu/J) were obtained from the Jackson Laboratory, Bar Harbor, ME. PB-Cre4 mice
[38] (B6.Cg background, strain name B6.Cg-Tg(Pbsn-cre)4Prb) were obtained from Mouse
Models of Human Cancers Consortium (MMHCC) of the National Cancer Institute. Cross-
breeding of PB-Cre4 mice and PtenL/L mice generated Pten conditional knockout male mice
with PIN lesions in the prostate at 6 weeks of age according to the published protocol [11].
The use of the animals was approved by the Institutional Animal Use and Care Committees
at the University of California Davis and Tulane University.
The human and rodent prostate tissue slides were stained with 7.5 µg/ml anti-ICD
antibodies, using the VECTSTAIN elite ABC Reagent and DAB Substrate Kit with
hematoxylin counterstaining according to the manufacturer’s protocol [30–32]. The stained
slides were assessed by two pathologists (A.D.B. for rodent tissues and J.M. for human
tissues). Representative photomicrographs of the prostate tissues were captured under a
microscope with digital camera.
Western Blot Analysis
The cells were cultured in serum-free medium for 16 hours and treated with or without 20
ng/ml of recombinant human IL-17A (R&D Systems Inc., Minneapolis, MN) for 10 to 120
minutes. Proteins were extracted from the cultured cells in RIPA lysis buffer [50 mM
sodium fluoride, 0.5% Igepal CA-630 (NP-40), 10 mM sodium phosphate, 150 mM sodium
chloride, 25 mM Tris pH 8.0, 1mM phenylmethylsulfonyl fluoride, 2 mM
ethylenediaminetetraacetic acid (EDTA), 1.2 mM sodium vanadate] supplemented with
protease inhibitor cocktail (Sigma-Aldrich, St. Louis, MO). Equal amount of proteins was
subjected to 10% SDS-polyacrylamide gel electrophoresis and transferred to polyvinylidene
difluoride membrane. The membranes were blocked with 5% nonfat dry milk in TBST (25
mM Tris-HCl, 125 mM NaCl, 0.1% Tween 20) for 2 hours and probed with the indicated
primary antibodies overnight and then IRDye®800CW- or IRDye®680-conjugated
secondary antibodies (LI-COR Biosciences, Lincoln, NE) for 1 hour. The results were
visualized by using an Odyssey Infrared Imager (LI-COR Biosciences, Lincoln, NE). For
loading control, the membranes were stripped and probed for non-phosphorylated proteins
and/or GAPDH.
Cell Growth Assay
About 2 × 104 cells per well were cultured in the complete culture medium in 12-well plates.
Triplicate wells per group were treated with or without 20 ng/ml of IL-17A for 4 days. The
medium was replaced by serum-free DMEM containing 5 mg/ml of 3-[4,5-
dimethylthiazol-2-yl]-2,-5-diphenyl-tetrazolium bromide (MTT, Sigma-Aldrich, St. Louis,
MO). After 4 hours of incubation, medium was carefully removed, the formazan dye was
dissolved by dimethylsulfoxide, and absorbance at 595 nm was read on a Plate Reader.
You et al. Page 4
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

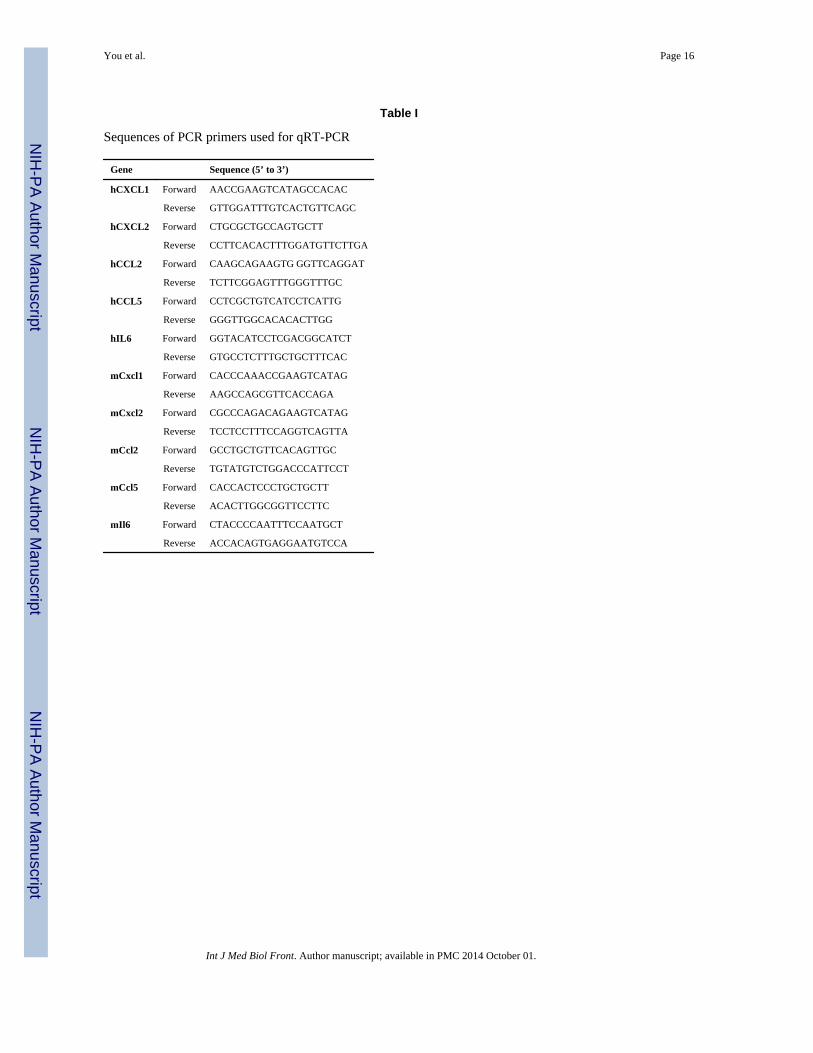
Analysis of mRNA Expression by Quantitative Real-time RT-PCR
The cells were cultured in serum-free medium for 16 hours and treated with or without 20
ng/ml of IL-17A for 2 hours. Total RNA was extracted from the cells using RNeasy Mini
Kit (QIAGEN, Valencia, CA) with on-membrane DNase I digestion to avoid genomic DNA
contamination. cDNA was made from total RNA using Superscript™ First-Strand Synthesis
System with oligo dT primers (Invitrogen, Carlsbad, CA). Human and mouse GAPDH
primers were obtained from Applied Biosystems (Foster City, CA). The PCR primers
specific for each chemokine and cytokine have been published previously [39–43], except
that the mouse Il-6 primers were obtained from Real Time Primers, LLC., Elkins Park, PA
(see Table I for primer sequences). Real-time quantitative PCR was performed in triplicates
with an iQ5®iCycler (Bio-Rad Laboratories, Hercules, CA) following the recommended
protocols. Results were normalized to GAPDH levels using the formula ΔCt (Cycle
threshold) = Ct of target gene – Ct of GAPDH. The mRNA level of the untreated control
cells was used as the baseline; therefore, ΔΔCt was calculated using the formula ΔΔCt = ΔCt
of target gene - ΔCt of the baseline. The fold change of mRNA level was calculated as fold
= 2ΔΔCt.
Statistical Analysis
The difference of IL-17RC staining (negative versus positive) between the normal human
prostatic epithelium and human PIN lesions was analyzed by χ2 test. The Student’s t test was
used to analyze the other quantitative data. P < 0.05 was considered statistically significant.
RESULTS
IL-17RC Protein Expression Was Increased in Human and Rodent PIN Lesions
In human prostate tissues with high-grade PIN, we found that 38 of the 60 cases (63%) of
high-grade PIN lesions showed positive staining for IL-17RC (Fig.1A and 1B). The typical
high-grade PIN lesions showed micropapillary growth pattern of stratified cells with
enlarged nuclei and prominent nucleoli. The normal epithelium in all of the 60 cases stained
negatively for IL-17RC expression (Fig.1A and 1B). Thus, IL-17RC expression is
significantly increased in human PIN lesions compared to the normal prostatic epithelium (P
< 0.001). The endothelium of adjacent blood vessels also stained positively for IL-17RC
(Fig. 1B).
The normal prostatic epithelium from the untreated rats stained negatively for IL-17RC
expression, though the adjacent endothelium of blood vessels stained positively (Fig. 1C),
suggesting that the normal rat prostatic epithelium is truly negative for IL-17RC staining. In
contrast, the prostatic epithelium of the PhIP-treated rats showed focal lesions of crowded
cells with enlarged and hyperchromatic nuclei. The focal lesions were diagnosed as
epithelial hyperplasia according to the Bar Harbor Classification [44]. These focal lesions
stained moderately positive for IL-17RC (Fig. 1D). Strong staining for IL-17RC was found
in typical rat PIN lesions (Fig. 1E). The PIN lesions were characterized by a cribriform
architecture with neoplastic epithelial cells forming solid bridges within the glandular
lumen. The lesions filled the glandular lumen but did not show signs of stromal invasion
(Fig. 1E). In TRAMP mouse prostate tissues, PIN lesions were characterized by crowded
You et al. Page 5
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

and/or stratified cells with enlarged and atypical nuclei. The mouse PIN lesions stained
moderately positive for IL-17RC (Fig. 1F). Of note, the adjacent normal prostatic epithelium
stained negatively for IL-17RC (Fig. 1F). In Pten wild-type mouse prostates, the prostatic
epithelium stained negatively for IL-17RC (Fig. 1G). In contrast, the neoplastic epithelium
stained strongly positive for IL-17RC in the PIN lesions of Pten conditional knockout mice
(Fig. 1H).
IL-17A Induced Activation of ERK and/or NF-κB Signaling Pathways
When PIN-C cells were treated with 20 ng/ml of IL-17A, phosphorylated ERK1/2 was not
obviously increased (Fig. 2A). When IL-17RC was over-expressed in PIN-RC cells,
phosphorylated ERK1/2 was slightly increased upon IL-17A treatment (Fig. 2A).
Phosphorylated ERK1/2 was transiently increased in TRAMP-C1 cells after 10 to 15 min of
IL-17A treatment (Fig. 2B). Phosphorylated IκBα was transiently increased in LNCaP-C
cells after 10 min of IL-17A treatment (Fig. 2C), but not in PIN-C or TRAMP-C1 cells (data
not shown). Phosphorylated ERK1/2 was also transiently increased in LNCaP-C cells after
10 min of IL-17A treatment (Fig. 2C). When IL-17RC was over-expressed in LNCaP-RC
cells, phosphorylated IκBα and phosphorylated ERK1/2 were increased to higher levels and
sustained up to 60 min after IL-17A treatment, compared to LNCaP-C cells (Fig. 2C).
Phosphorylated AKT or STAT3 (Signal Transducer and Activator of Transcription 3) was
not increased in any of the cells studied (Fig. 2C and data not shown).
IL-17A Did Not Affect Cell Growth but Stimulated Expression of Chemokines andCytokines
We did not observe any difference in cell growth when IL-17RC was over-expressed in
LNCaP or PIN cells or when the cells were treated with IL-17A (Fig. 2D). However, we
found that IL-17A induced expression of CXCL1 and CXCL2 chemokines by approximately
2-fold in RWPE-1, pRNS-1-1, PIN-C, and LNCaP-C cells (see Table II for a summary of
the results). IL-17A also induced expression of CCL2 chemokine and IL-6 cytokine by
approximately 2-fold in LNCaP-C cells. Expression of CCL2, CCL5 and IL-6 was not
noticeably induced by IL-17A in RWPE-1, pRNS-1-1, and PIN-C cells. IL-17A induced
expression of CXCL1 and CXCL2 by 3-fold in PIN-RC cells (P < 0.05, compared to PIN-C
cells). Expression of CXCL1 and CCL5 was induced by 15- and 9-fold in LNCaP-RC cells
(P < 0.05, compared to LNCaP-C cells). In TRAMP-C1 cells, IL-17A induced expression of
CXCL1, CXCL2, CCL2, CCL5, and IL-6 by approximately 3- to 33-fold (Table II).
DISCUSSION
IL-17RC gene was originally identified from prostate cancer [28]. We have previously
reported that protein expression of the IL-17RC isoform recognized by the anti-ICD
antibodies was significantly increased in castration-resistant prostate cancer, compared to
androgen-dependent prostate cancer [30,31]. We recently reported that the normal human
prostatic epithelium stained negatively using the anti-ICD antibodies [32]. The rationale to
investigate IL-17RC expression in PIN lesions is to complete our study of IL-17RC
expression in a spectrum of normal prostatic epithelium, PIN, androgen-dependent prostate
cancer, and castration-resistant prostate cancer. In this study, we found that normal human
You et al. Page 6
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
prostatic epithelium stains negatively for IL-17RC expression, whereas 38 of the 60 cases
(63%) of high-grade PIN lesions stain positively. The IL-17RC-positive rate in PIN lesions
is significantly higher than in normal prostatic epithelium (P < 0.001). In order to determine
whether or not the increased IL-17RC expression is unique in human PIN lesions, both rat
and mouse PIN lesions were stained for IL-17RC expression. We found that in both rat and
mouse PIN lesions, IL-17RC expression is increased compared to the adjacent normal
prostatic epithelium. In addition, we found that IL-17RC expression is also increased in the
alveolar hyperplasia lesions in a K-rasLA1 transgenic mouse model of lung adenocarcinoma
[45] (You, et al., unpublished observation). Taken together, these findings suggest that
increase of IL-17RC expression is possibly a common phenomenon in epithelial hyperplasia
and PIN lesions.
IL-17A and IL-17F cytokines act through IL-17RA and IL-17RC to activate intracellular
signalling pathways [24–27,46]. We found that ERK1/2 and/or NF-κB pathways in human
and mouse prostate epithelial cells are activated by IL-17A treatment. This is consistent with
the reports in the literature that ERK1/2 and NF-κB pathways are the two major IL-17-
induced signalling pathways [47]. It is worth noting that activation of ERK1/2 and/or NF-κB
pathways is enhanced in PIN-RC and LNCaP-RC cells that over-express IL-17RC,
compared to the control cell lines PIN-C and LNCaP-C. This finding implies that increased
IL-17RC expression in prostatic epithelium may enhance cellular responses to IL-17 stimuli.
TH17 cell number and IL-17A expression have been found to be increased in prostate cancer
[14,23]. IL-17-expressing macrophages and neutrophils also accumulate in the PIA lesion -
a potential precursor to PIN and carcinoma [4,48]. However, the effects of IL-17A on
prostatic epithelium have not been well studied. In this study, we found that IL-17A does not
affect cell growth rate of the cultured prostatic epithelial cells. This is consistent with
previous in-vitro studies showing that IL-17 does not stimulate cellular proliferation in other
cell types [49–52]. However, it has been reported that IL-17A induced expression of a
variety of chemokines and cytokines in some mesenchymal cell lines [43]. We have recently
reported that IL-17A induces expression of chemokines and cytokines in human gynecologic
cancer cell lines [53]. It is not known whether IL-17A has similar effects on prostatic
epithelial cells. Therefore, we examined the expression of chemokines and cytokines in
human and mouse prostatic epithelial cells treated with IL-17A. We found that expression of
CXCL1, CXCL2, CCL2, CCL5, and IL-6 is induced by IL-17A. Moreover, when IL-17RC
is over-expressed in PIN-RC and LNCaP-RC cells, expression of CXCL1, CXCL2, and
CCL5 is significantly enhanced, compared to the control cell lines PIN-C and LNCaP-C.
Therefore, it is possible that an increased IL-17RC expression in the prostatic epithelial cells
may confer an enhanced response upon IL-17 stimulation. It has been shown that CXCL1
plays important roles in inflammation, angiogenesis, tumorigenesis, and tumor invasion in
several cancer types [39,54,55]. CXCL2 promotes colorectal tumor cell proliferation [56].
CCL2 enhances prostate cancer cell migration and metastasis [57,58]. CCL5 is correlated
with cancer formation and progression in breast and prostate cancers [59–61]. The function
of these chemokines in the prostatic epithelial-stromal interaction is yet to be determined.
You et al. Page 7
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

CONCLUSION
This study demonstrates that IL-17RC expression is increased in human and rodent PIN
lesions. Over-expression of IL-17RC enhances IL-17A-induced signalling activity and
expression of chemokines.
Acknowledgments
The authors thank Dr. Prescott L. Deininger (Director of Tulane Cancer Center) and Tulane Cancer Center CoreFacilities for research support; Dr. Johng S. Rhim who was the original source of RWPE-1 and pRNS-1-1 cell lines;Dr. Mark Stearns who was the original source of the PIN cell line and Dr. Alice C. Levine who provided the PINcell line. Grant sponsors: National Institutes of Health’s Centers of Biomedical Research Excellence (COBRE)grant (2P20RR020152-06), Department of Defense grants (W81XWH-05-1-0567 and W81XWH-10-1-0937), thedevelopmental funds of the Tulane Cancer Center, Louisiana Cancer Research Consortium, and Tulane Frameworkfor Global Health Seed Grant.
Abbreviations
Anti-ICD anti-IL-17RC intracellular domain antibodies
CCL C-C ligand
CXCL CXC ligand
ERK Extracellular signal-Regulated Kinase
GAPDH glyceraldehyde-3-phosphate dehydrogenase
IL interleukin
IL-17RC interleukin-17 receptor C
NF-κB Nuclear Factor-κB
PhIP 2-amino-1-methyl-6-phenylimidazo (4,5-b) pyridine
PIN prostatic intraepithelial neoplasia
TH17 T helper cells subtype 17
TNF tumor necrosis factor.
REFERENCES
1. Nickel JC, Downey J, Young I, Boag S. Asymptomatic inflammation and/or infection in benignprostatic hyperplasia. BJU Int. 1999; 84(9):976–981. [PubMed: 10571623]
2. Gerstenbluth RE, Seftel AD, MacLennan GT, Rao RN, Corty EW, Ferguson K, Resnick MI.Distribution of chronic prostatitis in radical prostatectomy specimens with up-regulation of bcl-2 inareas of inflammation. J Urol. 2002; 167(5):2267–2270. [PubMed: 11956490]
3. Schatteman PH, Hoekx L, Wyndaele JJ, Jeuris W, Van Marck E. Inflammation in prostate biopsiesof men without prostatic malignancy or clinical prostatitis: correlation with total serum PSA andPSA density. Eur Urol. 2000; 37(4):404–412. [PubMed: 10765070]
4. De Marzo AM, Marchi VL, Epstein JI, Nelson WG. Proliferative inflammatory atrophy of theprostate: implications for prostatic carcinogenesis. Am J Pathol. 1999; 155(6):1985–1992.[PubMed: 10595928]
5. Wang W, Bergh A, Damber JE. Morphological transition of proliferative inflammatory atrophy tohigh-grade intraepithelial neoplasia and cancer in human prostate. Prostate. 2009; 69(13):1378–1386. [PubMed: 19507201]
You et al. Page 8
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
6. De Marzo AM, Platz EA, Sutcliffe S, Xu J, Gronberg H, Drake CG, Nakai Y, Isaacs WB, NelsonWG. Inflammation in prostate carcinogenesis. Nat Rev Cancer. 2007; 7(4):256–269. [PubMed:17384581]
7. Sutcliffe S, Platz EA. Inflammation in the etiology of prostate cancer: an epidemiologic perspective.Urol Oncol. 2007; 25(3):242–249. [PubMed: 17483023]
8. Bierhoff E, Walljasper U, Hofmann D, Vogel J, Wernert N, Pfeifer U. Morphological analogies offetal prostate stroma and stromal nodules in BPH. Prostate. 1997; 31(4):234–240. [PubMed:9180933]
9. Song Z, Wu X, Powell WC, Cardiff RD, Cohen MB, Tin RT, Matusik RJ, Miller GJ, Roy- BurmanP. Fibroblast growth factor 8 isoform B overexpression in prostate epithelium: a new mouse modelfor prostatic intraepithelial neoplasia. Cancer Res. 2002; 62(17):5096–5105. [PubMed: 12208767]
10. Gupta S, Adhami VM, Subbarayan M, MacLennan GT, Lewin JS, Hafeli UO, Fu P, Mukhtar H.Suppression of prostate carcinogenesis by dietary supplementation of celecoxib in transgenicadenocarcinoma of the mouse prostate model. Cancer Res. 2004; 64(9):3334–3343. [PubMed:15126378]
11. Wang S, Gao J, Lei Q, Rozengurt N, Pritchard C, Jiao J, Thomas GV, Li G, Roy-Burman P,Nelson PS, Liu X, Wu H. Prostate-specific deletion of the murine Pten tumor suppressor geneleads to metastatic prostate cancer. Cancer Cell. 2003; 4(3):209–221. [PubMed: 14522255]
12. Borowsky AD, Dingley KH, Ubick E, Turteltaub KW, Cardiff RD, Devere-White R. Inflammationand atrophy precede prostatic neoplasia in a PhIP-induced rat model. Neoplasia. 2006; 8(9):708–715. [PubMed: 16984728]
13. Steiner GE, Djavan B, Kramer G, Handisurya A, Newman M, Lee C, Marberger M. The picture ofthe prostatic lymphokine network is becoming increasingly complex. Rev Urol. 2002; 4(4):171–177. [PubMed: 16985676]
14. Steiner GE, Newman ME, Paikl D, Stix U, Memaran-Dagda N, Lee C, Marberger MJ. Expressionand function of pro-inflammatory interleukin IL-17 and IL-17 receptor in normal, benignhyperplastic, and malignant prostate. Prostate. 2003; 56(3):171–182. [PubMed: 12772186]
15. Harrington LE, Hatton RD, Mangan PR, Turner H, Murphy TL, Murphy KM, Weaver CT.Interleukin 17-producing CD4+ effector T cells develop via a lineage distinct from the T helpertype 1 and 2 lineages. Nat Immunol. 2005; 6(11):1123–1132. [PubMed: 16200070]
16. Park H, Li Z, Yang XO, Chang SH, Nurieva R, Wang YH, Wang Y, Hood L, Zhu Z, Tian Q, DongC. A distinct lineage of CD4 T cells regulates tissue inflammation by producing interleukin 17.Nat Immunol. 2005; 6(11):1133–1141. [PubMed: 16200068]
17. Steiner GE, Stix U, Handisurya A, Willheim M, Haitel A, Reithmayr F, Paikl D, Ecker RC,Hrachowitz K, Kramer G, Lee C, Marberger M. Cytokine expression pattern in benign prostatichyperplasia infiltrating T cells and impact of lymphocytic infiltration on cytokine mRNA profile inprostatic tissue. Lab Invest. 2003; 83(8):1131–1146. [PubMed: 12920242]
18. Sun J, Turner A, Xu J, Gronberg H, Isaacs W. Genetic variability in inflammation pathways andprostate cancer risk. Urol Oncol. 2007; 25(3):250–259. [PubMed: 17483024]
19. Kolls JK, Linden A. Interleukin-17 family members and inflammation. Immunity. 2004; 21(4):467–476. [PubMed: 15485625]
20. Moseley TA, Haudenschild DR, Rose L, Reddi AH. Interleukin-17 family and IL-17 receptors.Cytokine Growth Factor Rev. 2003; 14(2):155–174. [PubMed: 12651226]
21. Qian Y, Liu C, Hartupee J, Altuntas CZ, Gulen MF, Jane-Wit D, Xiao J, Lu Y, Giltiay N, Liu J,Kordula T, Zhang QW, Vallance B, Swaidani S, Aronica M, Tuohy VK, Hamilton T, Li X. Theadaptor Act1 is required for interleukin 17-dependent signaling associated with autoimmune andinflammatory disease. Nature immunology. 2007; 8(3):247–256. [PubMed: 17277779]
22. Li X. Act1 modulates autoimmunity through its dual functions in CD40L/BAFF and IL-17signaling. Cytokine. 2008; 41(2):105–113. [PubMed: 18061473]
23. Sfanos KS, Bruno TC, Maris CH, Xu L, Thoburn CJ, DeMarzo AM, Meeker AK, Isaacs WB,Drake CG. Phenotypic analysis of prostate-infiltrating lymphocytes reveals TH17 and Tregskewing. Clin Cancer Res. 2008; 14(11):3254–3261. [PubMed: 18519750]
You et al. Page 9
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

24. Yao Z, Fanslow WC, Seldin MF, Rousseau AM, Painter SL, Comeau MR, Cohen JI, Spriggs MK.Herpesvirus Saimiri encodes a new cytokine, IL-17, which binds to a novel cytokine receptor.Immunity. 1995; 3(6):811–821. [PubMed: 8777726]
25. Yao Z, Painter SL, Fanslow WC, Ulrich D, Macduff BM, Spriggs MK, Armitage RJ. HumanIL-17: a novel cytokine derived from T cells. J Immunol. 1995; 155(12):5483–5486. [PubMed:7499828]
26. Kuestner RE, Taft DW, Haran A, Brandt CS, Brender T, Lum K, Harder B, Okada S, OstranderCD, Kreindler JL, Aujla SJ, Reardon B, Moore M, Shea P, Schreckhise R, Bukowski TR, PresnellS, Guerra-Lewis P, Parrish-Novak J, Ellsworth JL, Jaspers S, Lewis KE, Appleby M, Kolls JK,Rixon M, West JW, Gao Z, Levin SD. Identification of the IL-17 receptor related moleculeIL-17RC as the receptor for IL-17F. J Immunol. 2007; 179(8):5462–5473. [PubMed: 17911633]
27. Wright JF, Bennett F, Li B, Brooks J, Luxenberg DP, Whitters MJ, Tomkinson KN, Fitz LJ,Wolfman NM, Collins M, Dunussi-Joannopoulos K, Chatterjee-Kishore M, Carreno BM. Thehuman IL-17F/IL-17A heterodimeric cytokine signals through the IL-17RA/IL-17RC receptorcomplex. J Immunol. 2008; 181(4):2799–2805. [PubMed: 18684971]
28. Haudenschild D, Moseley T, Rose L, Reddi AH. Soluble and transmembrane isoforms of novelinterleukin-17 receptor-like protein by RNA splicing and expression in prostate cancer. J BiolChem. 2002; 277(6):4309–4316. [PubMed: 11706037]
29. Haudenschild DR, Curtiss SB, Moseley TA, Reddi AH. Generation of interleukin-17 receptor-likeprotein (IL-17RL) in prostate by alternative splicing of RNA. Prostate. 2006; 66(12):1268–1274.[PubMed: 16688746]
30. You Z, Shi XB, DuRaine G, Haudenschild D, Tepper CG, Lo SH, Gandour-Edwards R, de VereWhite RW, Reddi AH. Interleukin-17 receptor-like gene is a novel antiapoptotic gene highlyexpressed in androgen-independent prostate cancer. Cancer Res. 2006; 66(1):175–183. [PubMed:16397230]
31. You Z, Dong Y, Kong X, Zhang Y, Vessella RL, Melamed J. Differential expression of IL-17RCisoforms in androgen-dependent and androgen-independent prostate cancers. Neoplasia. 2007;9(6):464–470. [PubMed: 17603628]
32. Ge D, You Z. Expression of interleukin-17RC protein in normal human tissues. Int Arch Med.2008; 1(1):19. [PubMed: 18928529]
33. Bello D, Webber MM, Kleinman HK, Wartinger DD, Rhim JS. Androgen responsive adult humanprostatic epithelial cell lines immortalized by human papillomavirus 18. Carcinogenesis. 1997;18(6):1215–1223. [PubMed: 9214605]
34. Lee MS, Garkovenko E, Yun JS, Weijerman PC, Peehl DM, Chen LS, Rhim JS. Characterizationof adult human prostatic epithelial cells immortalized by polybrene-induced DNA transfectionwith a plasmid containing an origin-defective SV40 genome. Int J Oncol. 1994; 4:821–830. 4.[PubMed: 21566988]
35. Wang M, Liu A, Garcia FU, Rhim JS, Stearns ME. Growth of HPV-18 immortalized humanprostatic intraepithelial neoplasia cell lines. Influence of IL-10, follistatin, activin-A, and DHT. IntJ Oncol. 1999; 14(6):1185–1195. [PubMed: 10339677]
36. Liu XH, Kirschenbaum A, Lu M, Yao S, Klausner A, Preston C, Holland JF, Levine AC.Prostaglandin E(2) stimulates prostatic intraepithelial neoplasia cell growth through activation ofthe interleukin-6/GP130/STAT-3 signaling pathway. Biochem Biophys Res Commun. 2002;290(1):249–255. [PubMed: 11779161]
37. Greenberg NM, DeMayo F, Finegold MJ, Medina D, Tilley WD, Aspinall JO, Cunha GR,Donjacour AA, Matusik RJ, Rosen JM. Prostate cancer in a transgenic mouse. Proc Natl Acad SciU S A. 1995; 92(8):3439–3443. [PubMed: 7724580]
38. Wu X, Wu J, Huang J, Powell WC, Zhang J, Matusik RJ, Sangiorgi FO, Maxson RE, Sucov HM,Roy-Burman P. Generation of a prostate epithelial cell-specific Cre transgenic mouse model fortissue-specific gene ablation. Mech Dev. 2001; 101(1–2):61–69. [PubMed: 11231059]
39. Wang D, Wang H, Brown J, Daikoku T, Ning W, Shi Q, Richmond A, Strieter R, Dey SK, DuBoisRN. CXCL1 induced by prostaglandin E2 promotes angiogenesis in colorectal cancer. J Exp Med.2006; 203(4):941–951. [PubMed: 16567391]
You et al. Page 10
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
40. Knight BC, Kissane S, Falciani F, Salmon M, Stanford MR, Wallace GR. Expression analysis ofimmune response genes of Muller cells infected with Toxoplasma gondii. J Neuroimmunol. 2006;179(1–2):126–131. [PubMed: 16934877]
41. Sawa Y, Tsuruga E. The expression of E-selectin and chemokines in the cultured human lymphaticendothelium with lipopolysaccharides. J Anat. 2008; 212(5):654–663. [PubMed: 18410313]
42. Keller C, Keller P, Marshal S, Pedersen BK. IL-6 gene expression in human adipose tissue inresponse to exercise--effect of carbohydrate ingestion. J Physiol. 2003; 550(Pt 3):927–931.[PubMed: 12794182]
43. Shen F, Ruddy MJ, Plamondon P, Gaffen SL. Cytokines link osteoblasts and inflammation:microarray analysis of interleukin-17- and TNF-alpha-induced genes in bone cells. J Leukoc Biol.2005; 77(3):388–399. [PubMed: 15591425]
44. Shappell SB, Thomas GV, Roberts RL, Herbert R, Ittmann MM, Rubin MA, Humphrey PA,Sundberg JP, Rozengurt N, Barrios R, Ward JM, Cardiff RD. Prostate pathology of geneticallyengineered mice: definitions and classification. The consensus report from the Bar Harbor meetingof the Mouse Models of Human Cancer Consortium Prostate Pathology Committee. Cancer Res.2004; 64(6):2270–2305. [PubMed: 15026373]
45. Johnson L, Mercer K, Greenbaum D, Bronson RT, Crowley D, Tuveson DA, Jacks T. Somaticactivation of the K-ras oncogene causes early onset lung cancer in mice. Nature. 2001; 410(6832):1111–1116. [PubMed: 11323676]
46. Ely LK, Fischer S, Garcia KC. Structural basis of receptor sharing by interleukin 17 cytokines. NatImmunol. 2009; 10(12):1245–1251. [PubMed: 19838198]
47. Gaffen SL. Structure and signalling in the IL-17 receptor family. Nat Rev Immunol. 2009; 9(8):556–567. [PubMed: 19575028]
48. Vykhovanets EV, Maclennan GT, Vykhovanets OV, Gupta S. IL-17 Expression by macrophages isassociated with proliferative inflammatory atrophy lesions in prostate cancer patients. Int J ClinExp Pathol. 2011; 4(6):552–565. [PubMed: 21904631]
49. Tartour E, Fossiez F, Joyeux I, Galinha A, Gey A, Claret E, Sastre-Garau X, Couturier J, MosseriV, Vives V, Banchereau J, Fridman WH, Wijdenes J, Lebecque S, Sautees-Fridman C. Interleukin17, a T-cell-derived Cytokine, Promotes Tumorigenicity of Human Cervical Tumors in NudeMice. Cancer Res. 1999; 59(15):3698–3704. [PubMed: 10446984]
50. Numasaki M, Fukushi J-i, Ono M, Narula SK, Zavodny PJ, Kudo T, Robbins PD, Tahara H, LotzeMT. Interleukin-17 promotes angiogenesis and tumor growth. Blood. 2003; 101(7):2620–2627.[PubMed: 12411307]
51. Benchetrit F, Ciree A, Vives V, Warnier G, Gey A, Sautes-Fridman C, Fossiez F, Haicheur N,Fridman WH, Tartour E. Interleukin-17 inhibits tumor cell growth by means of a T-celldependentmechanism. Blood. 2002; 99(6):2114–2121. [PubMed: 11877287]
52. Hirahara N, Nio Y, Sasaki S, Minari Y, Takamura M, Iguchi C, Dong M, Yamasawa K, Tamura K.Inoculation of human interleukin-17 gene-transfected Meth-A fibrosarcoma cells induces T cell-dependent tumor-specific immunity in mice. Oncology. 2001; 61(1):79–89. [PubMed: 11474253]
53. Lai T, Wang K, Hou Q, Zhang J, Yuan J, Yuan L, You Z, Xi M. Interleukin 17 Induces Up-Regulation of Chemokine and Cytokine Expression Via Activation of the Nuclear Factor kappaBand Extracellular Signal-Regulated Kinase 1/2 Pathways in Gynecologic Cancer Cell Lines. Int JGynecol Cancer. 2011
54. Dhawan P, Richmond A. Role of CXCL1 in tumorigenesis of melanoma. J Leukoc Biol. 2002;72(1):9–18. [PubMed: 12101257]
55. Kawanishi H, Matsui Y, Ito M, Watanabe J, Takahashi T, Nishizawa K, Nishiyama H, Kamoto T,Mikami Y, Tanaka Y, Jung G, Akiyama H, Nobumasa H, Guilford P, Reeve A, Okuno Y,Tsujimoto G, Nakamura E, Ogawa O. Secreted CXCL1 is a potential mediator and marker of thetumor invasion of bladder cancer. Clin Cancer Res. 2008; 14(9):2579–2587. [PubMed: 18451219]
56. Kollmar O, Junker B, Rupertus K, Menger MD, Schilling MK. Studies on MIP-2 and CXCR2expression in a mouse model of extrahepatic colorectal metastasis. Eur J Surg Oncol. 2007; 33(6):803–811. [PubMed: 17314027]
You et al. Page 11
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
57. Li X, Loberg R, Liao J, Ying C, Snyder LA, Pienta KJ, McCauley LK. A destructive cascademediated by CCL2 facilitates prostate cancer growth in bone. Cancer Res. 2009; 69(4):1685–1692.[PubMed: 19176388]
58. Loberg RD, Day LL, Harwood J, Ying C, St John LN, Giles R, Neeley CK, Pienta KJ. CCL2 is apotent regulator of prostate cancer cell migration and proliferation. Neoplasia. 2006; 8(7):578–586. [PubMed: 16867220]
59. Colombatti M, Grasso S, Porzia A, Fracasso G, Scupoli MT, Cingarlini S, Poffe O, Naim HY,Heine M, Tridente G, Mainiero F, Ramarli D. The prostate specific membrane antigen regulatesthe expression of IL-6 and CCL5 in prostate tumour cells by activating the MAPK pathways.PLoS ONE. 2009; 4(2):e4608. [PubMed: 19242540]
60. Soria G, Ben-Baruch A. The inflammatory chemokines CCL2 and CCL5 in breast cancer. CancerLett. 2008; 267(2):271–285. [PubMed: 18439751]
61. Vaday GG, Peehl DM, Kadam PA, Lawrence DM. Expression of CCL5 (RANTES) and CCR5 inprostate cancer. Prostate. 2006; 66(2):124–134. [PubMed: 16161154]
You et al. Page 12
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

Fig. 1. IL-17RC expression was increased in human and rodent PIN lesions as shown byimmunohistochemical stainingA. Human high-grade PIN lesions (in the three circles); original magnification, ×100. B.
High magnification (×400) of a representative PIN lesion; ar rows indicate PIN; open arrow
indicates normal epithelium; and arrowhead indicates a blood vessel. C. Rat normal prostatic
epithelium (open arrow) and a blood vessel (arrowhead). D. Rat normal atrophic prostatic
epithelium (open arrow) and epithelial hyperplasia (arrow). E. Rat normal prostatic
epithelium (open arrow) and PIN (arrow). F. TRAMP mouse PIN lesions (arrows) and
You et al. Page 13
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

adjacent normal epithelium (open arrows). G. Pten wild-type mouse normal prostatic
epithelium (open arrow). H. Pten conditional knockout mouse PIN (arrows). Original
magnification, × 400.
You et al. Page 14
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript

Fig. 2. Effects of IL-17A on signaling pathways and cell growth in the prostati c epithelial celllinesA. Western blot analysis of phosphorylated ERK1/2 (pERK1/2) and regular ERK1/2 in
human PIN -C and PINRC cells. B. Western blot analysis of pERK1/2 and ERK1/2 in
mouse TRAMP -C1 cells. C. Western blot analysis of pIκBα, IκBα, pERK1/2, ERK1/2,
pAKT, and pSTAT3 in human LNCaP-C and LNCaP-RC cells. For loading control, the
membranes were stripped and probed for GAPDH. D. Cell growth assay. The cells were
cultured in the complete culture medium in 12-well plates. Triplicate wells per group were
treated with or without 20 ng/ml of IL-17A for 4 days. The medium was replaced by serum-
free DMEM containing 5 mg/ml of MTT. After 4 hours of incubation, medium was removed
and the formazan dye was dissolved by dimethylsulfoxide. Absorbance at 595 nm was read.
The difference between the groups in comparison was not statistically significant (P > 0.05).
You et al. Page 15
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
You et al. Page 16
Table I
Sequences of PCR primers used for qRT-PCR
Gene Sequence (5’ to 3’)
hCXCL1 Forward AACCGAAGTCATAGCCACAC
Reverse GTTGGATTTGTCACTGTTCAGC
hCXCL2 Forward CTGCGCTGCCAGTGCTT
Reverse CCTTCACACTTTGGATGTTCTTGA
hCCL2 Forward CAAGCAGAAGTG GGTTCAGGAT
Reverse TCTTCGGAGTTTGGGTTTGC
hCCL5 Forward CCTCGCTGTCATCCTCATTG
Reverse GGGTTGGCACACACTTGG
hIL6 Forward GGTACATCCTCGACGGCATCT
Reverse GTGCCTCTTTGCTGCTTTCAC
mCxcl1 Forward CACCCAAACCGAAGTCATAG
Reverse AAGCCAGCGTTCACCAGA
mCxcl2 Forward CGCCCAGACAGAAGTCATAG
Reverse TCCTCCTTTCCAGGTCAGTTA
mCcl2 Forward GCCTGCTGTTCACAGTTGC
Reverse TGTATGTCTGGACCCATTCCT
mCcl5 Forward CACCACTCCCTGCTGCTT
Reverse ACACTTGGCGGTTCCTTC
mIl6 Forward CTACCCCAATTTCCAATGCT
Reverse ACCACAGTGAGGAATGTCCA
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.

NIH
-PA
Author M
anuscriptN
IH-P
A A
uthor Manuscript
NIH
-PA
Author M
anuscript
You et al. Page 17
Tab
le II
Che
mok
ines
and
cyt
okin
es in
duce
d by
IL
-17A
in h
uman
and
mou
se p
rost
atic
epi
thel
ial c
ell l
ines
Gen
eH
uman
nor
mal
cel
lsH
uman
PIN
cel
lsH
uman
can
cer
cells
Mou
se c
ance
r ce
lls
RW
PE
-1pR
NS-
1-1
PIN
-CP
IN-R
CL
NC
aP-C
LN
CaP
-RC
TR
AM
P-C
1
CX
CL
12.
7±1.
82.
0±1.
71.
9±0.
63.
1±0.
5*2.
8±1.
615
.0±
3.3*
32.7
±1.
1
CX
CL
22.
3±1.
11.
9±1.
32.
0±0.
43.
0±0.
7*2.
0±1.
12.
4±1.
59.
3±1.
5
CC
L2
1.0±
0.5
1.2±
0.3
1.2±
0.4
1.8±
1.1
2.4±
1.9
2.8±
1.3
4.5±
1.0
CC
L5
0.4±
0.5
1.3±
0.3
1.3±
1.2
1.0±
0.5
1.5±
1.2
9.2±
2.8*
2.8±
1.1
IL-6
1.3±
0.3
1.5±
0.4
1.7±
0.3
1.3±
0.3
2.3±
1.4
1.8±
0.6
5.6±
1.0
The
cel
l lin
es w
ere
trea
ted
with
or
with
out 2
0 ng
/ml o
f IL
-17A
for
2 h
. The
mR
NA
exp
ress
ion
was
ana
lyze
d by
qR
T-P
CR
, whi
ch w
as n
orm
aliz
ed b
y G
APD
H a
nd p
rese
nted
as
mea
n ±
sta
ndar
d de
viat
ion
offo
ld in
crea
se o
f th
ree
expe
rim
ents
usi
ng th
e un
trea
ted
cont
rol c
ells
as
base
line.
Ast
eris
k in
dica
tes
that
the
fold
incr
ease
was
of
stat
istic
al s
igni
fica
nce
(P <
0.0
5), c
ompa
red
to th
e PI
N-C
or
LN
CaP
-C c
ells
,re
spec
tivel
y.
Int J Med Biol Front. Author manuscript; available in PMC 2014 October 01.






























