




Integrating Family Planning and VCT Services
Clients Seeking HIV-related Services
Why Integrate HIV and RH Services
Share common needs and concerns:• are often both sexually active and fertile• are at risk of HIV infection or might be infected • need access to contraceptives• need to know how HIV affects contraceptive options and Vice Versa
Clients Seeking RH Services
AND
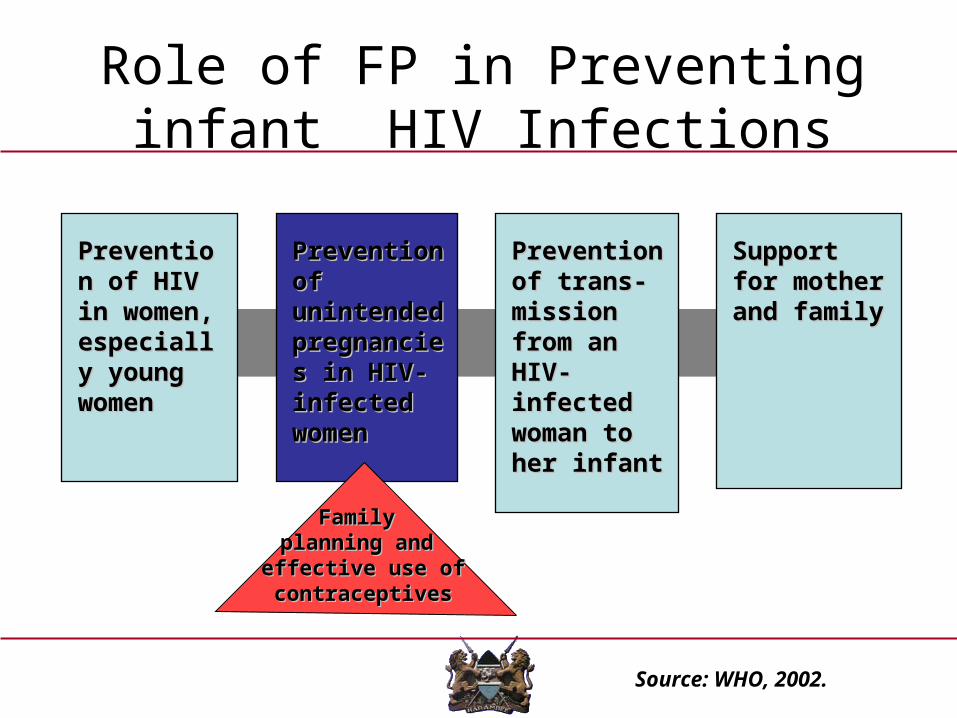
Role of FP in Preventing infant HIV Infections
Support for Support for mother and mother and familyfamily
Prevention Prevention of trans-of trans-mission mission from an HIV-from an HIV-infected infected woman to woman to her infanther infant
Prevention Prevention of of unintended unintended pregnancies pregnancies in HIV-in HIV-infected infected women women
Prevention Prevention of HIV in of HIV in women, women, especially especially young young womenwomen
Source: WHO, 2002.
Family Family planning and planning and
effective use of effective use of contraceptivescontraceptives
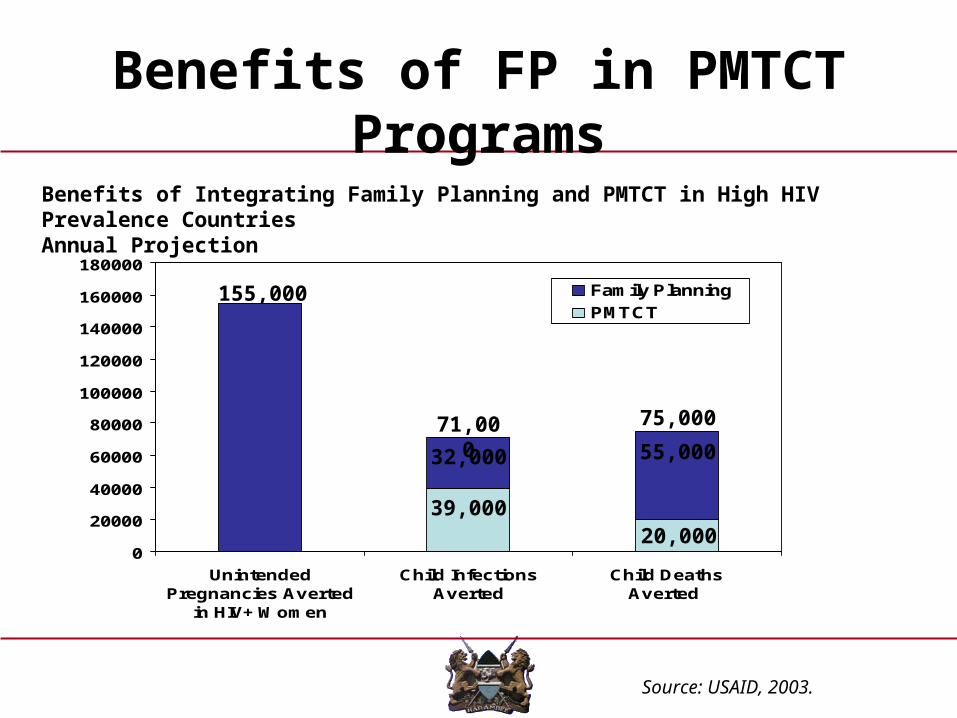
Benefits of FP in PMTCT Programs
Source: USAID, 2003.
Benefits of Integrating Family Planning and PMTCT in High HIV Prevalence CountriesAnnual Projection
0
20000
40000
60000
80000
100000
120000
140000
160000
180000
UnintendedPregnancies Averted
in HIV+ Women
Child InfectionsAverted
Child Deaths Averted
Family Planning
PMTCT155,000
32,000
39,000
55,000
20,000
75,00071,000
Dual protection
Means using a method/methods that protects both against HIV/STIs and Pregnancy
This can be achieved in three ways• Abstinence• Mutual monogamy with uninfected partner and
using of a contraceptive method • Use of Female or Male Condoms• Use of a condom and another more effective
contraceptive method-Dual Method Use

BENEFITS FP IN VCT
• 1) VCT services reach more clients than any other HIV service, thus Family planning in VCT is a way of increasing access to family planning services.
• Family planning in VCT services can reach clients who do not typically go to family planning services such as men and youth.
• FP-VCT also prevents unintended pregnancies in HIV+ women and therefore reduces MTCT and number of infants born HIV infected

Enabling Factors
• Well structured and stable VCT programme• Supportive MOH structure [DRH/Nascop• Existence of VCT and FP guidelines and a
supportive NHSSP11• Existence of and oversight by a technical
committee• Commitment and team work from the VCT/FP
sub-committee
• Mobilisation of funds for a common goal
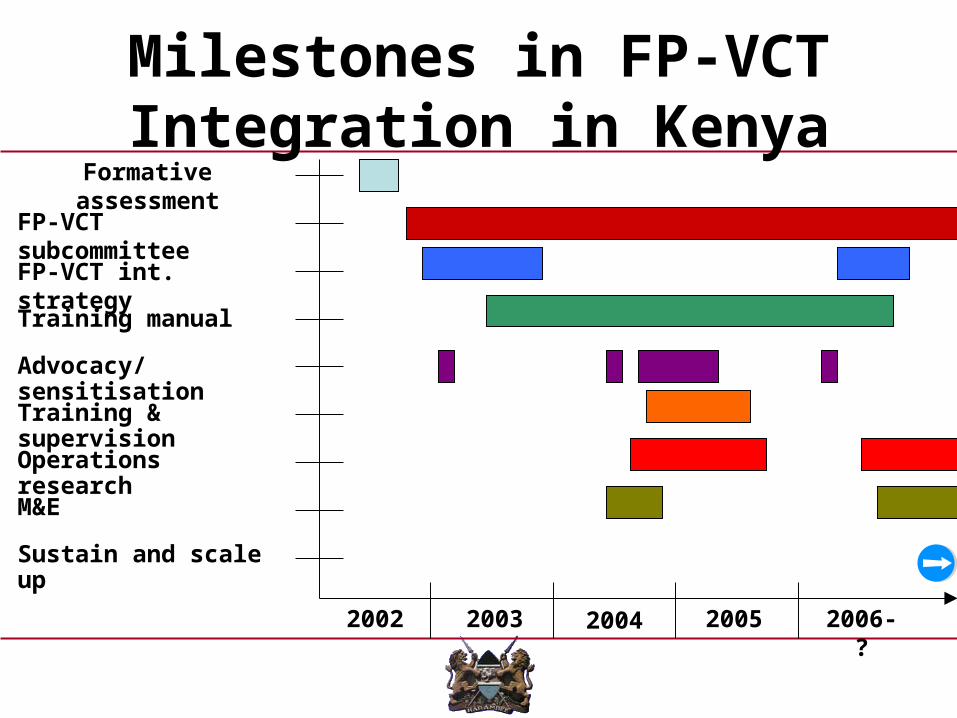
Milestones in FP-VCT Integration in Kenya
FP-VCT subcommittee
FP-VCT int. strategy
Training manual
Advocacy/ sensitisation
Training & supervision
M&E
Operations research
Sustain and scale up
Formative assessment
2002 2003 2004 2005 2006-?
FP-VCT integration in Kenya
• Results of formative assessment in 2003: – Integration is acceptable
• 89% of clients• 100% of service providers and in-charges
– Potential FP demand exists» 40% of clients not on FP
– Wide variation in VCT provider background• 61% had clinical background• 37% were FP-trained
– Level of FP in VCT should be decided facility-by-facility
Source: FHI report, 2003
Conclusions based on findings
• Assessment in Kenya found that integrating FP into VCT services:– Is feasible– Is acceptable – Does not appear to affect HIV service
quality– Family planning demand exists

Development Of FP/VCT Integration Strategy
1. Sharing of formative assessment results
2. Formation of FP-VCT Sub-committee
3. Final product
DRAFTMINISTRY OF HEALTH
NATIONAL AIDS & STD CONTROL PROGRAM (NASCOP)AND
DIVISION OF REPRODUCTIVE HEALTH
STRATEGY FOR THE INTEGRATION OF HIV VOLUNTARY CONSELLING AND
TESTING (VCT) SERVICESAND FAMILY PLANNING SERVICES
Task Force MembersMOH-NASCOP, MOH-DRH, FHI, CDC, JHPIEGO, KNH,
KICOSHEP, AMKENIFHI facilitated the functioning of the
Task Force

Levels of Integration
• Definition: Incorporation of some or all of family planning services in VCT
• Four levels depending on resources and level of provider training: – Level I: Condoms and pills – Level II: Condoms, pills, and injectables– Level III: Condoms, pills, injectables, and IUCD– Level IV: A full range of contraceptive methods
• All levels should be able to:– Assess for pregnancy and STI/HIV infection risks– Provide information and counseling on FP methods– Refer clients for services not available

Training Manual Development• Tools approved by NASCOP’s VCT main committee in June 2004
• Harmonization of the TRAINING Manuals which resulted in a Trainers and Participant manual
Ministry of Health – Kenya
Family Planning Training for Voluntary Counselling and Testing Providers: An Integrated Approach to Counselling and Service Provision
Trainer’s Manual
Kenya National Training Manual for Integrating FP into VCT, December 2006
Ingredients for FP/VCT Integration
• Advocacy and sensitisation at all levels of the health care system
• Pre-training site selection to diagnose whether the site will benefit from integrated services
• Training of TOTs and service providers• Provider tools• Regular Support supervision• Client education materials for demand creation• M&E / Operations research-monitor VCT
quality and FP method provision

FP-VCT integration in Kenya (con’t)
• Results of operations research in 2006: – Trained VCT providers nearly twice as likely to
discuss a client’s desire for more children (11% to 20%)
– Providers only slightly more likely to discuss clients’ current FP use (23% to 28%)
– Providers more likely to discuss FP methods with clients (46% to 63%)
– Small effect on clients’ reports of contraceptive uptake (17% to 29%)
• Condoms only method provided
Source: FHI report, 2006

Results of operations research in 2006 [contd]
– 27% - 29% of VCT clients at risk of unintended pregnancy
– No change in VCT session time or counseling content– Provider, in-charges, and clients said FP in VCT
improved VCT quality
Source: FHI report, 2006
Recommendations
• Improve provider skills in pregnancy risk screening• Train more VCT providers per centre to increase
access• Continue monitoring of VCT quality and FP method
choice provision
Sustaining and Scaling up FP in VCT
• Continuous advocacy • Training of service providers
• Diversification of funding sources
• Mobilization of available resources
• Institutionalization supervision
• Utilization of already developed Human resource, tools and materials
• Adoption of the OJT model of training





























