



Presented by:Lorraine D. Ellis, MS, MBA
President/CEOResearch Dynamics Consulting Group, Ltd.
andWilliam Gluck, Ph.D.
VP, DATATRAK Clinical and Consulting ServicesDATATRAK International, Inc.
Integrating Clinical Operations and Clinical Data Management Through EDC
Speakers
Lorraine D. Ellis, MS, MBA, Research Dynamics Consulting Group, Ltd. @resdyn
Lorraine D. Ellis, is the founder/CEO of Research Dynamics, a full service CRO. Most of her 35 years’ experience in the industry has been in clinical research. Her expertise includes integrating technology with clinical research processes over the past 20 years and developing state-of-the-art training programs for clinical research professionals.
William Gluck, Ph.D, DATATRAK International, Inc. @DATATRAKinc
Bill Gluck joined DATATRAK International in October 2010 as VP of DATATRAK’s Clinical and Consulting Services. Dr. Gluck has more than 25 years of experience in the pharmaceutical and biotechnology industries and has diversified experience in clinical trial management systems and electronic data capture.

Agenda
► Historical Perspectives
► Integrating Clinical Operations
► Integrating Clinical Data Management
► Conclusions and Parting Thoughts
Historical Perspectives
► Drug development process• Paper-based processing
► Electronic Data Capture• Interactive processing

Historical Perspectives
► Age of technological advances
• Application of technology
to a process
• Integration of technology
as part of the process


Clinical Operations:The Past!
► On-site monitoring was an isolated event
► On-site was the only way to monitor
► On-site monitoring = rate-limiting factor for data compilation and database lock
► Monitoring focus was on data checking
► Common (but now archaic) activities:
• Tracking each CRF page as it passes from site to clinical to CDM
• “yellow stickies” and tracking queries separately from CDM’s queries
► Monitored CRF “handoff” to CDM
► Few feedback processes to improve data collection during the trial

Data flow & Monitoring: the past
Patient
Data
Database

Data Flow in the past
► Data recording, collection, compilation and reporting was…..
• CRF design was often hampered by limited interaction with key parties
• Sequential process – little feedback to improve data
• Data was not sent to CDM until after each 4-6 week visit
• On-site monitoring visits were a limiting factor for data processing
• Silo’d processes with formal handoffs
• Paper movement from site to CRA to CDM was the rate limiting factor
• CRF Page tracking was inefficient and time consuming
• Query generation and resolution was a tracking-intensive
• Query process was labor-intensive with both CRA and CDM
• No feedback to improve data collection during trial
………………………………Very paper and process intensive and slow.

Early EDC daysFew process changes
► Monitors still reviewed CRFs on site but using a computer instead of paper.
► EDC = RDE (remote (site) data entry)
► Off-site CRF review was rare
► Limited EDC functionality
► No large process changes to capitalize on advantages of technology
► Some clinical operations/monitors would modify dept. procedures but no integration among all groups that interact with the data.
► Clin ops and CDM was still silo’d and CRFs were still “handed-off”

EDC is not just for CDM!It’s for Monitors too!
= real time monitoring
= more efficient monitoring
= CRF page status tracked
= edit checks= fewer queries
= improved protocol compliance
= flagged protocol violations
= errors caught earlier
= no query tracking (EDC does it)
= immediate feedback improves data quality
= less time data checking
EDC = Data
Entry
Time to maximize technologyand change processes
► Need changes in processes of:
• Collection, monitoring, tracking, cleaning
► Real time data processing requires real time interaction between Clin Ops and CDM
► CRF design including protocol deviations and edit checks require both Clin Ops and CDM
► Query process is more real time and interactive between Clin Ops and CDM for real time changes.
Integration between Clin Ops and CDM enhances efficiency of EDC
► CRF design to address monitoring issues
► Constant data flow to CDM with real time feedback to Clin Ops
► Clin Ops can modify monitoring with EDC and CDM feedback
► Query generation, tracking and resolution simultaneous but integrated into one list

New Monitoring processes
► Real time monitoring
► Off-site and On-site monitoring
► Build edit checks into CRFS to decrease queries
► CRF design requires monitoring considerations (eg,
mandatory fields, protocol compliance, proper procedures, etc)
► NO tracking of pages or queries!
► Less data checking and focus on site performance continuously
► EDC metrics provide “window” to performance (time to eCRF completion, # queries, # data errors, etc)

FDA Guidance
► Risk Based monitoring!
► 1988 guidance withdrawn!
► Centralized (off-site) monitoring is encouraged!
► Centralized monitoring suggested to replace on-site monitoring when it can complete activities better or as well as on-site
► Centralized monitoring (when appropriate) should improve ability to ensure the quality and integrity of data
• Pubs suggest that data anomalies may be more readily detected
► EDC can implement centralized monitoring methods that can enable decreased reliance on on-site monitoring

Clinical Operations: The Future!Monitoring process has changed.
► Real time monitoring (not just every 4-6 wks)
► Data reviewed off-site
► Continuous data flow to CDM
► CRF design with Clin Ops and CDM
• Includes protocol compliance
• Edit checks to reduce queries
• Database designed early requiring earlier data decisions
► Sequential processes become simultaneous (Clin Ops & CDM)
► Silo monitoring processes become integrated with CDM
► Poor communication is improved with interactive communication tools in real time (from EDC system)

Data flow & Monitoring: the past
Patient
Data
Database
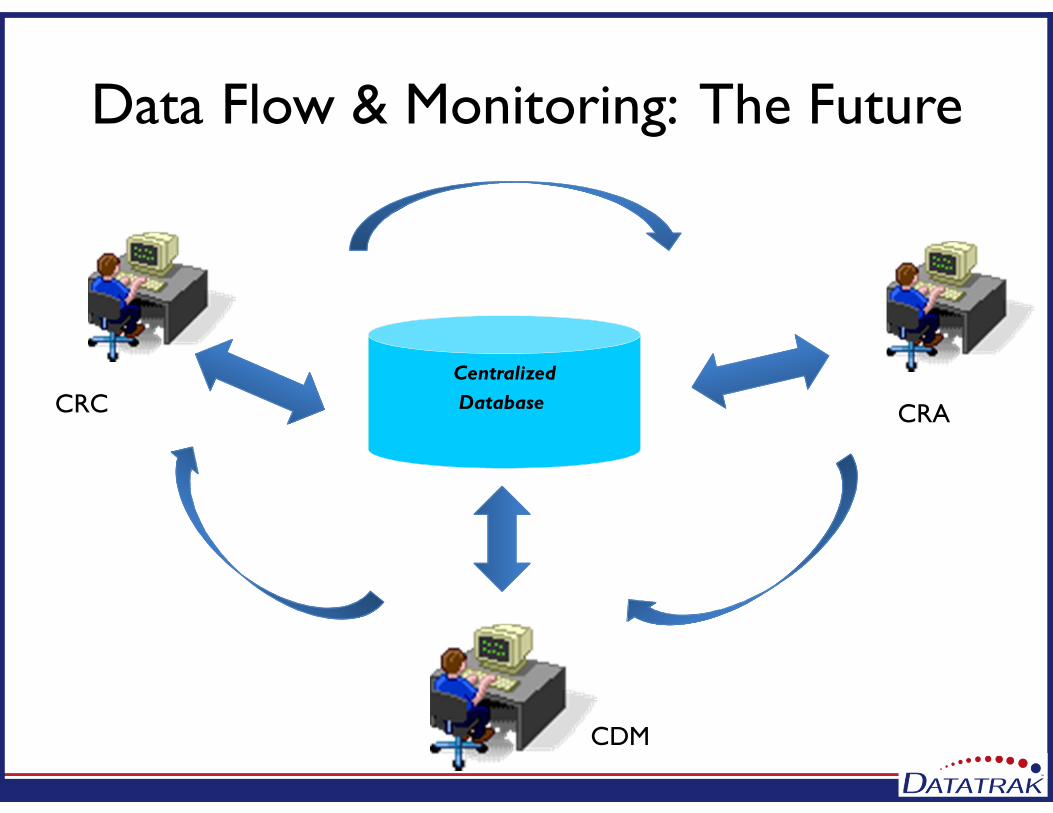
Data Flow & Monitoring: The Future
Centralized
Database CRC CRA
CDM

Monitoring in the 21st Century
► Risk based monitoring► Centralized monitoring (off-site)
► Continual interaction with Site (not just during site visits)
► SDV% will vary► Monitor spends less time on data checking and tracking► Monitor spends more time on overall study mgt.► Continuous data flow to CDM► Immediate query resolution with feedback decreases
monitoring time► Continual interaction with CDM from CRF design
through monitoring to database lock

Clinical Data Management
Process Driven
Technology Driven
Cross-Functionally Driven

CDManagement
► Technology and EDC is not just a CDM tool
► Benefits extend to all functional areas
► Integration and Technology allows for companies to put the MANAGEMENT back in Clinical Data Management

EDC as an Integration Tool
► Technology poses no functional constraints
► Forces process re-evaluation
► Workflow bring Clinical Operations
and CDM closer together
► Groups compliment and build
upon each other – seamless and
without formal handoffs

A Case Study
► Company A had a small clinical operations group with offices next to the CDM and rest of Biometrics
► Paper-based data collection – time from last patient to database freeze/lock was approximately 4 weeks for a ‘typical’ Phase II study
A Case Study
► EDC decision made at Management-level
► Top-down implementation
► No process re-evaluations or changes
► Study protocol in a state of flux
► Costs for EDC builds over $300K and not in production – EDC deemed a disaster

A Case Study
► Same teams 2 years later – CDM pro-EDC but Clinical Operations showing resistance to EDC
► Internal process evaluation/re-evaluation
► Workflow changes implemented
► EDC application implement across functional areas with cross-functional involvement
► EDC
Conclusions
► Use of technology is a great advance but we need to assimilate it into re-engineered processes
► To gain maximum benefit we must approach implementation of any technology through an integrated approach
► EDC can bring together groups traditional separated by process

Questions??
Contact Information:Lorraine D. EllisBill Gluck585-381-1350 x283 440-443-0082 [email protected]@datatrak.net
@ResDyn @DATATRAKinc






























