



Improving End-of-Life Care in the Emergency Department
Michael A. Gisondi, MD Associate Professor and Program DirectorMedical Education Fellowship DirectorDirector, Feinberg Academy of Medical EducatorsNorthwestern University Feinberg School of Medicine
Presented to:Palmetto Richland Emergency Medicine ResidencyUniversity of South Carolina School of MedicineAugust 2016

In a 1996 Gallup survey,
over 90% of respondents
expressed a desire to die at home.
Instead, 80% of patients die
in hospitals or institutions.
Over 200,000 Americans die
in emergency departments
each year.

Can we meet patient preferences
at the time of death?

Objectives
Define ‘Primary Palliative Care’
Describe The EPEC-EM™ Project
Identify opportunities and strategies for
palliative care education and research in the
field of emergency medicine
6

Disclosures
(1) NIH Co-Investigator
“Palliative Care for Cancer Patients in
Emergency Wards” – 2007-2011
NCI - 1R25CA116472-01A1 (PI= Emanuel)
$1,298,000
(2) Faculty, The EPEC-EM™ Project
7

What is Palliative Care?
World Health Organization
“…the active total care of patients whose
disease is not responsive to curative
treatment.”
“Control of pain.. and of psychological, social
and spiritual problems is paramount.”
“The goal of palliative care is the achievement
of the best possible quality of life for patients
and their families.”9

What is Palliative Care?
Palliative care actively addresses the physical,
spiritual, psychological, therapeutic, and social
needs of patients and families affected by
terminal illness, from the time of diagnosis of
a terminal illness to death, as well as
bereavement services for survivors.
10

Palliative Care Mandates
Prevent and relieve suffering
Affirm the dignity of the living
Do not hasten or postpone death
Offer a support system
Utilize multi-disciplinary approach
11
Team Goals
Pain and symptom management
Information sharing
Advanced care planning
Psychosocial support
Coordination of access to care
Bereavement counseling
12
Active Comfort Care
Both patient and family centered
Improves the quality of life
Regards dying as a normal process
13
Patient Expectations
Patients and families expect that their
physician is competent in facilitating the dying
process
Until recently, end-of-life care was absent from
medical school and residency curricula
14
Death = Failure?
Many emergency providers see death as a failure
We are often uncomfortable with loss
We were not trained in the expected
pathophysiology of normal dying
15

Care Comes Too Late
We recognize dying very late
The average length of hospice care is 15 days
16
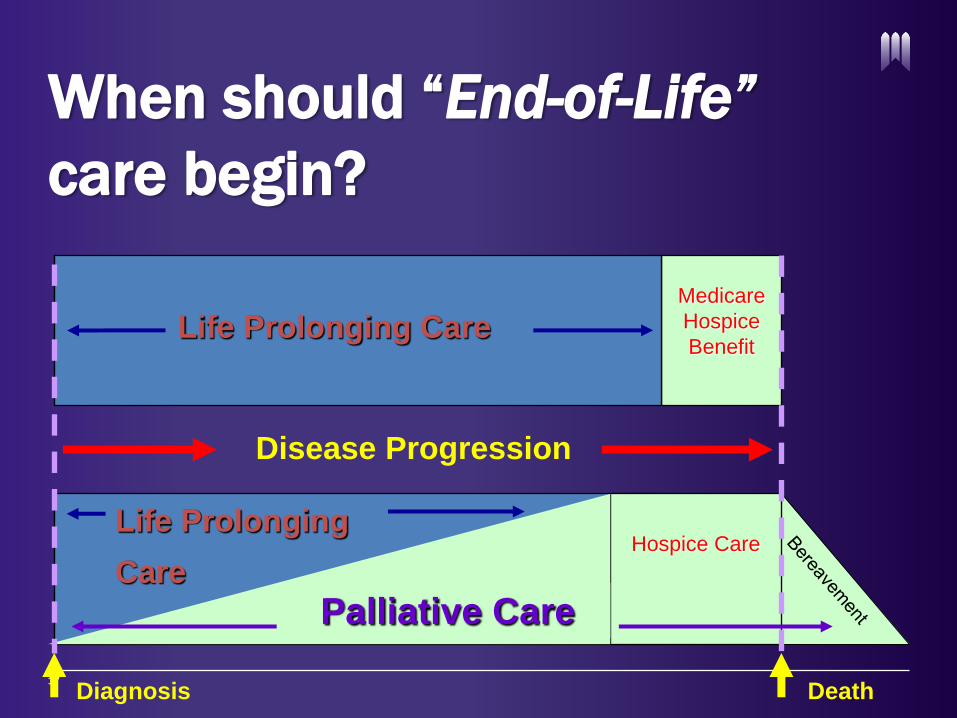
When should “End-of-Life”
care begin?
17
Palliative Care
Medicare
Hospice
Benefit
Disease Progression
Life Prolonging Care
Hospice CareLife Prolonging
Care
Diagnosis Death

The EPEC-EM Project™
The EPEC-EM™ Project
The mission of The EPEC-EM™ Project is to
educate all emergency healthcare
professionals on the essential clinical
competencies of emergency palliative care
Education and research to drive performance
change
19

‘Primary’ Palliative Care
The basic level of knowledge and skills that all
practitioners should have to relieve suffering
- Pain and symptom management
- Communication skills
- Ethical and responsible care
20
‘Tertiary’ Palliative Care
Hospice and Palliative Medicine (HPM)
- Co-sponsored by ABEM
- Training and Practice Pathways
Unique clinical, research and service model of
emergency palliative medicine practice
21

Emergency Palliative Care
Identification of ED patients who will benefit
from pain and symptom management
ED providers committed to relief of suffering
through validated interventions
22
EPEC-EM™ Grant Timeline
Year 1: Define a body of knowledge
Year 2: Disseminate core content
Year 3: Create symptom assessments
Year 4: Test interventions
23

FY 1: Body of Knowledge
Goal: EPEC-EM™ Core Content
Developed by an expert, multi-disciplinary
advisory board
Adaptation of materials from original EPEC,
as well as ABHPM core content
24
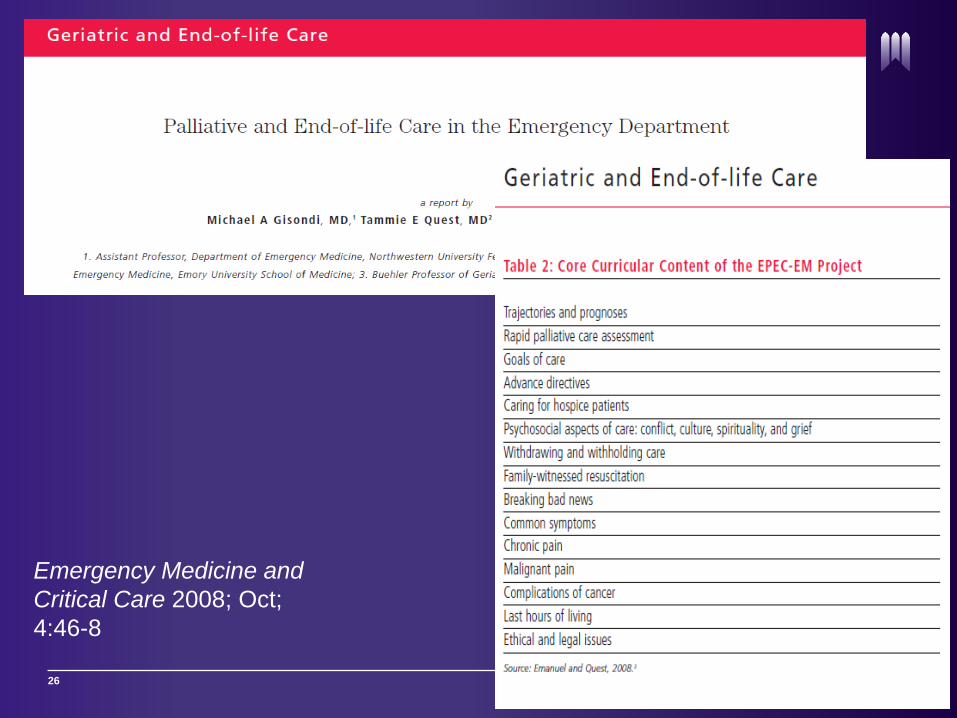
The EPEC-EM Curriculum is produced by the EPECTM Project with major funding provided by NCI.
Education in Palliative and End-of-life Care – Emergency Medicine
The
Project
EPEC-EMTM
26
Emergency Medicine and
Critical Care 2008; Oct;
4:46-8

27
FY 1: EPEC-EM Curriculum
28
1. Death Trajectories
2. Rapid Assessments
3. Goals of Care
4. Advance Directives
5. Hospice
6. Communication Skills
7. Withdrawing Care
8. Witnessed Resuscitation
9. Death Disclosure
10. Symptom Management
11. Chronic Pain
12. Malignant Pain
13. Cancer Complications
14. Last Hours of Life

FY 2: Dissemination
Goal: ‘Become an EPEC-EM Trainer’ Course
2 day, train-the-trainer program
400+ page course manual, teaching videos
www.epec.net
29

Module 1:
Trajectories &
Prognoses
E
P
E
C
E
M
EPEC -EMThe
TM
ProjectEducation in Palliative and End-of-life Care – Emergency Medicine
How do we die?

Global trajectories
• Terminal illness (e.g. cancer)
•Organ failure (e.g. CHF)
• Frailty (e.g. failure to thrive/SNF)
• Sudden death (e.g. trauma, V Fib)
• Lunney, Lynn et al. JAMA 2003.

Cancer
• Complications accelerate prognosis
Untreated Brain Mets
Treated Brain Mets
4-8 weeks
3-6 months
Malignant Hypercalcemia(except breast ca and myeloma)
8 weeks
Malignant Effusion 8 weeks
Carcinomatous Meningitis 8-12 weeks

Prognosis drives goals and
interventions
Prognosis Days Weeks Months Years
Goals Comfort only Prioritize quality
of life over
longevity
Try
Interventions,
but stop if they
are not working
Full efforts to cure
Interventions Pain control
Family presence
by bedside
Refer to hospice
Treat for comfort
Refer to hospice
Attempt
resuscitation;
Stop if signs of
instability
persist after
reasonable
efforts
Full resuscitation
efforts; maximal
efforts to stabilize;
transfer to ICU

Video 1:
Trajectories &
Prognoses
E
P
E
C
E
M
EPEC -EMThe
TM
ProjectEducation in Palliative and End-of-life Care – Emergency Medicine
FY 2: Outcome
12 EPEC EM conferences since 2007
Approximately 500 trainers
Over 25,000 end-users
Met NIH goal: 1 trainer at 50% of EM pgms.36
FY 2: Secondary Outcome
EPEC-EM curriculum can be successfully
adapted to various types of learners and
instructional formats
Mini-EPEC
Asynchronous Learning
37
• EPEC EM adapted materials were effective
• Synchronous and asynchronous instructional
methods were similarly effective
38
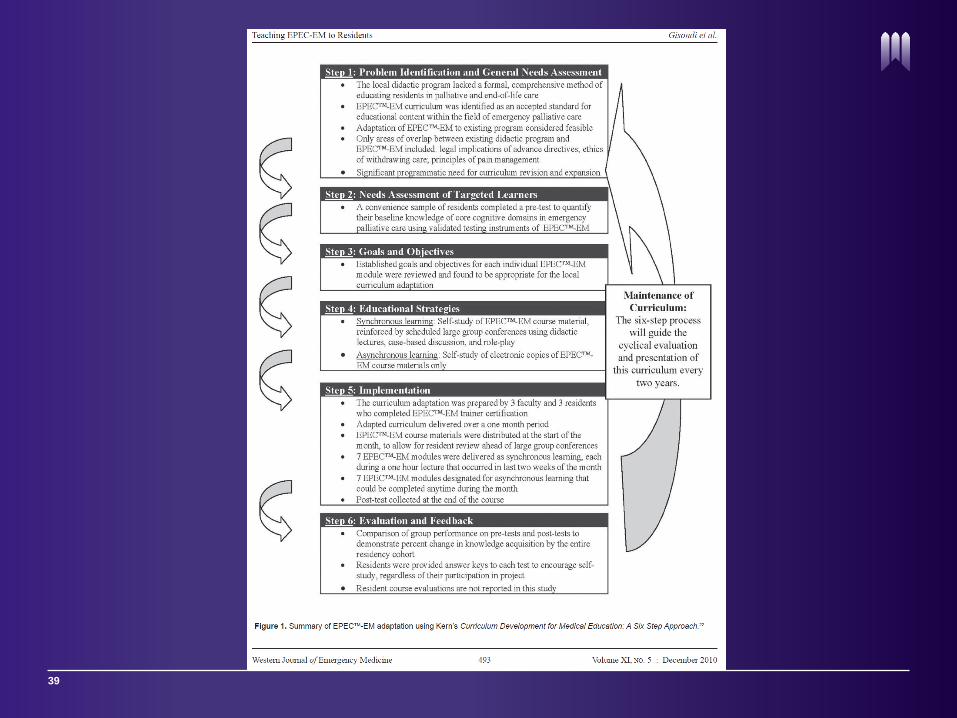
39

40
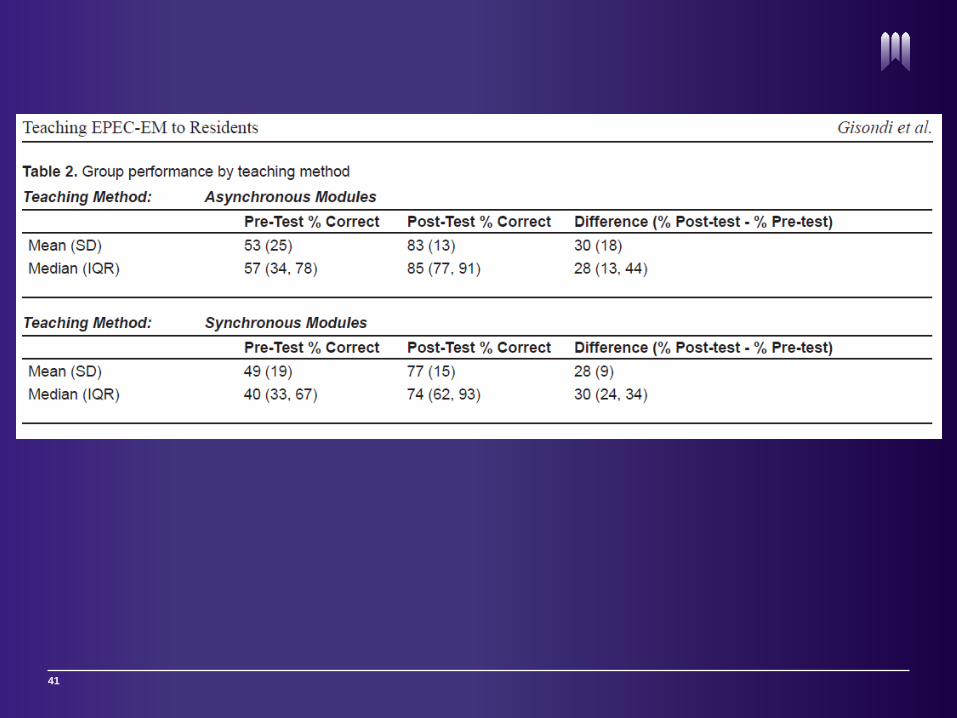
41
FY 3: Assess Symptoms
42
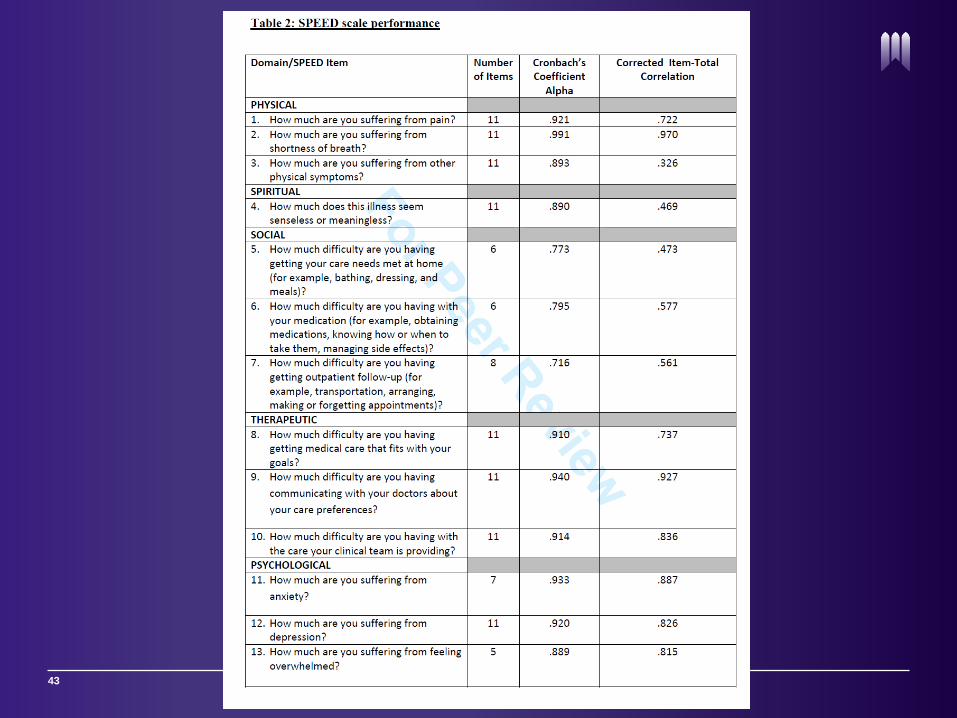
Goal: Develop a validated symptom
assessment tool for use in the ED
43
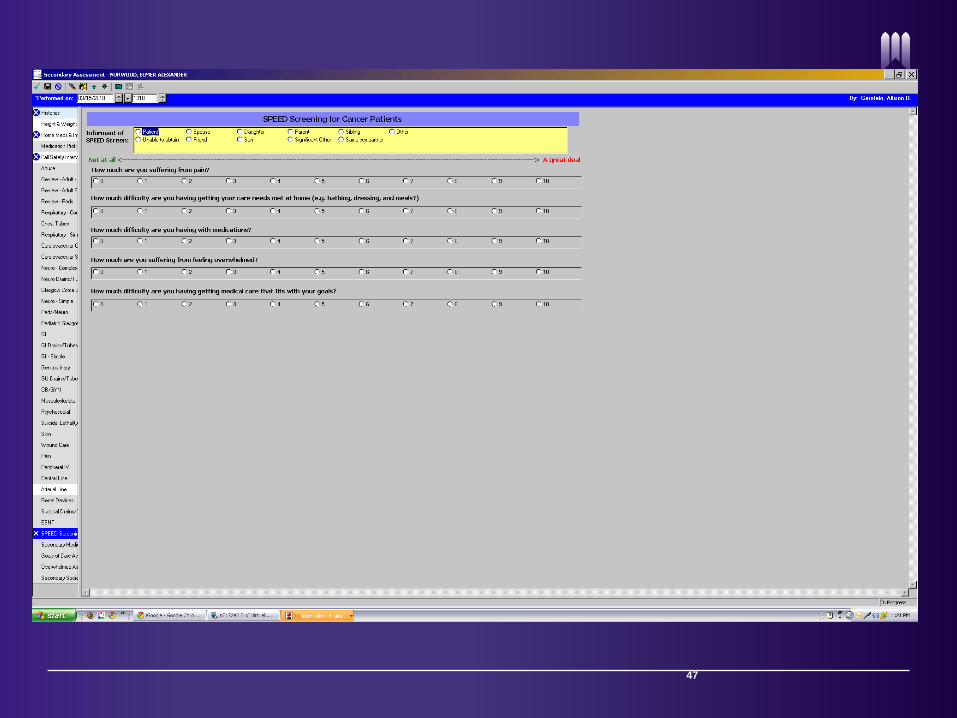
FY 3 Outcome: SPEED tool
Validated, brief
Likert scale 0-10 with threshold values linked
to proposed interventions
SPEED-short (5 item version)
44

SPEED question
How much are you suffering from pain?
(threshold ≥ 4)
How much difficulty are you having getting
your care needs met at home? (threshold ≥ 3)
How much difficulty are you having with your
medications? (threshold ≥ 3)
How much are you suffering from feeling
overwhelmed? (threshold ≥ 5)
How much difficulty are you having getting
medical care that fits with your goals?
(threshold ≥ 3)
46
47
FY 4: Test Interventions
Goal: Develop meaningful interventions
linked to the symptom burden uncovered by
SPEED
Employ multi-disciplinary approach
48

Post ED Visit
Admit / Discharge
3. Clinical Care
Primary Assessment
EPEC-EM Protocol Flow Chart
Triage Patient presents to Emergency Department (ED)
How much are
you suffering
from pain?
Threshold = 4
2. First SPEED questions
0-10 point scale
1. Active cancer screen
How much
difficulty are you
having getting your
care needs met at
home?
Threshold = 3
How much
difficulty are you
having with your
medications?
Threshold = 3
How much are
you suffering from
feeling
overwhelmed?
Threshold = 5
How much
difficulty are you
having getting
medical care
that fits with
your goals?
Threshold = 3
If pt. scores above threshold values,
the Palliative Care Resource Nurse
is notified to interact with the ED
Power Plan. Power plan includes
specific interventions triggered by
SPEED categories above threshold.
(S)
Palliative Care
Consult
(S)
Social Work
Consult
(S)
Pharmacy Consult
(focused
medication
teaching)
(S)
Palliative Care
Consult
(S)
Social Work
Consult
(S)
Chaplaincy
Consult
(S)
Palliative Care
Consult
Patient perspective of care:
A survey of patient centered
outcomes only for questions with
above threshold score at first
SPEED
How much are
you suffering
from pain?
How much
difficulty are
you having
getting your
care needs met
at home?
How much
difficulty are you
having with
communication
with your
medications?
How much are
you suffering
from feeling
overwhelmed?
How much difficulty
are you having
getting medical
care that fits with
your goals?
Second SPEED questions are
administered upon admission or
discharge only for questions above
threshold at first SPEED
(M)
Pain Protocol
(M)
Secondary
Chronic Pain
Assessment
(M)
Secondary
Social Needs
Assessment
(M)
Secondary
Medication
Assessment
(M)
Secondary
Mental Health
Assessment
(M)
Encourage
verbalization
of goals
4. Summary of care provided by ED
What could providers have done better to assess and respond
to...(your pain, your care needs, your difficulty with medications,
your feeling of being overwhelmed, your goals)?
Patient feedback opportunity:
Only for questions with above
threshold score at first SPEED
(S)
Palliative Care
Consult
(S)
Palliative Care
Consult
(M)
Secondary
Goals of Care
Assessment
(M)
Bedside
counseling
(M)
Goals of care
conversation
5. Admit/ Discharge survey
(M) = Mid-level provider
intervention (e.g.,
physician, nurse)
(S) = Sub-specialty
intervention
(e.g., social work,
chaplaincy, pharmacy,
patient liason)
How much did providers do everything they could to help
with...(your pain, your care needs, your difficulty with medications,
your feeling of being overwhelmed, your goals)? NEVER,
SOMETIMES, USUALLY or ALWAYS
6. Follow-up surveyPatient follow-up survey conducted by
research assistant
Palliative Care Resource Nurse (PCRN) notified of patients scoring above threshold values on any SPEED category

SPEED Screening for Cancer Patients
How much are you suffering from pain?
0
1
2
3
4
5
6
7
8
9
10
How much difficulty are you having getting your care needs met at home (e.g. bathing, dressing, and meals?)
0
1
2
3
4
5
6
7
8
9
10
How much difficulty are you having with your medications?
0
1
2
3
4
5
6
7
8
9
10
How much are you suffering from feeling overwhelmed?
0
1
2
3
4
5
6
7
8
9
10
How much difficulty are you having getting medical care that fits with your goals?
0
1
2
3
4
5
6
7
8
9
10
Submit
Not at all A great deal
Ask the patient:
Threshold
values
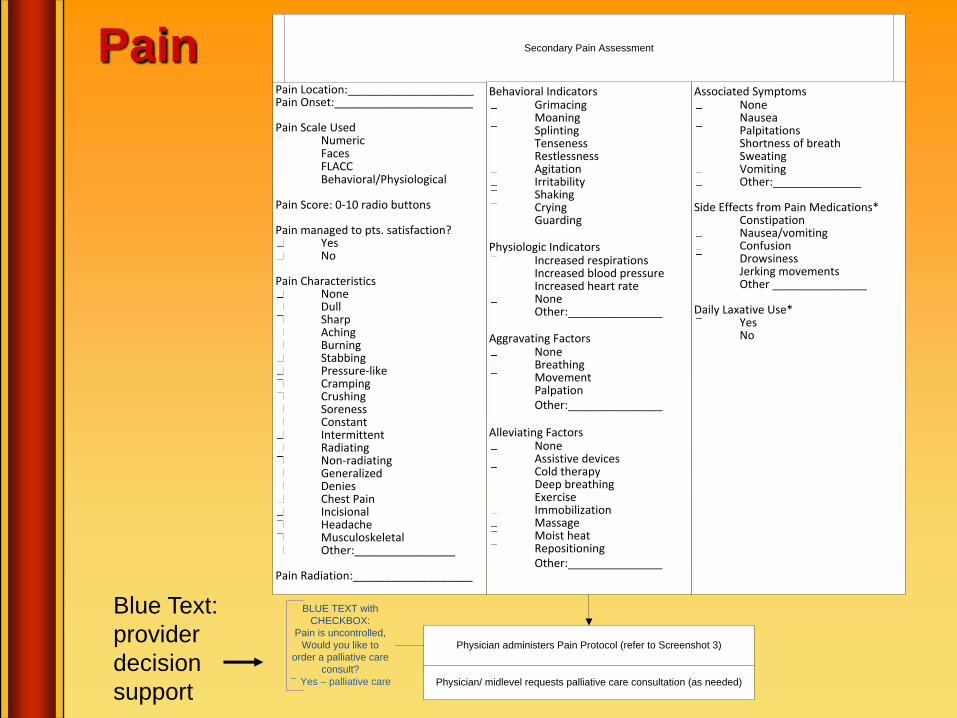
Pain
Blue Text:
provider
decision
support
Pain Location:____________________Pain Onset:______________________
Pain Scale UsedNumericFacesFLACCBehavioral/Physiological
Pain Score: 0-10 radio buttons
Pain managed to pts. satisfaction?YesNo
Pain CharacteristicsNoneDullSharpAchingBurningStabbingPressure-likeCrampingCrushingSorenessConstantIntermittentRadiatingNon-radiatingGeneralizedDeniesChest PainIncisionalHeadacheMusculoskeletalOther:________________
Pain Radiation:___________________
Secondary Pain Assessment
Behavioral IndicatorsGrimacingMoaningSplintingTensenessRestlessnessAgitationIrritabilityShakingCryingGuarding
Physiologic IndicatorsIncreased respirationsIncreased blood pressureIncreased heart rateNoneOther:_______________
Aggravating FactorsNoneBreathingMovementPalpationOther:_______________
Alleviating FactorsNoneAssistive devicesCold therapyDeep breathingExerciseImmobilizationMassageMoist heatRepositioningOther:_______________
Associated SymptomsNoneNauseaPalpitationsShortness of breathSweatingVomitingOther:______________
Side Effects from Pain Medications*ConstipationNausea/vomitingConfusionDrowsinessJerking movementsOther _______________
Daily Laxative Use*Yes No
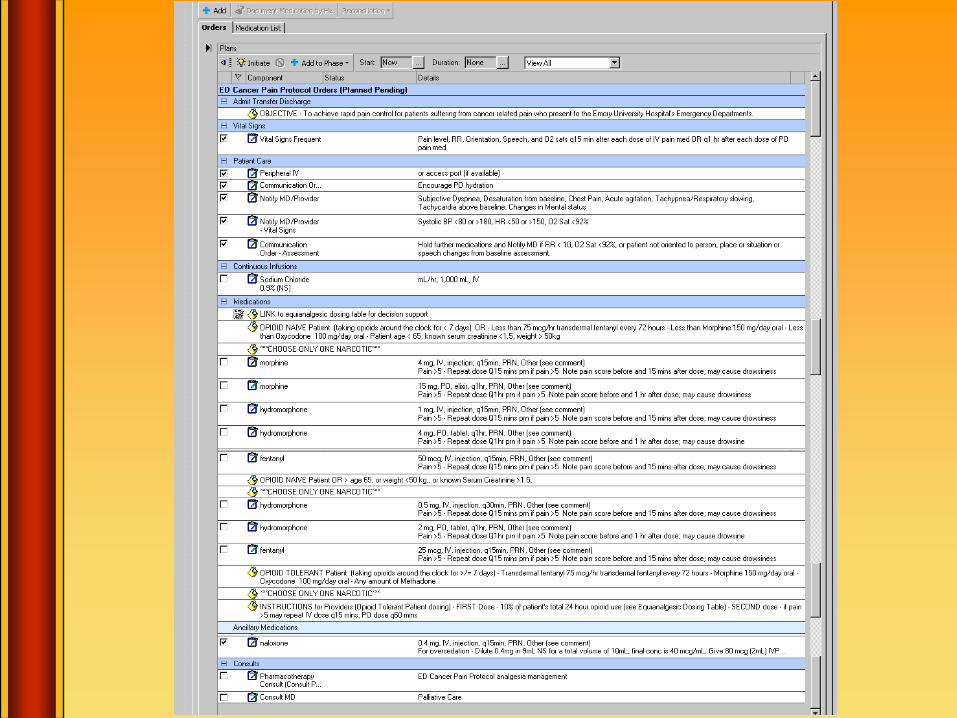
Physician administers Pain Protocol (refer to Screenshot 3)
Physician/ midlevel requests palliative care consultation (as needed)
BLUE TEXT with
CHECKBOX:
Pain is uncontrolled,
Would you like to
order a palliative care
consult?
Yes – palliative care

Care Needs
At home, are you having difficulty…?Using the toiletDressing yourselfTaking care of your hygieneMoving around (mobility problems)Managing medicationsPreparing mealsHome-makingGetting around to places (transportation)
Are you having financial difficulty with…?Utility bills (such as water, lights)Groceries and foodEquipment (such as a wheelchair, harness)Medications
Secondary Social Needs Assessment
Nurse requests social work consultation (as needed)
BLUE TEXT with
CHECKBOX:
Social needs are
unmanaged.
Would you like to
order a social work
and/ or palliative care
consult?
Yes – social work
Yes – palliative care
Physician/ midlevel provider requests palliative care consultation (as
needed)
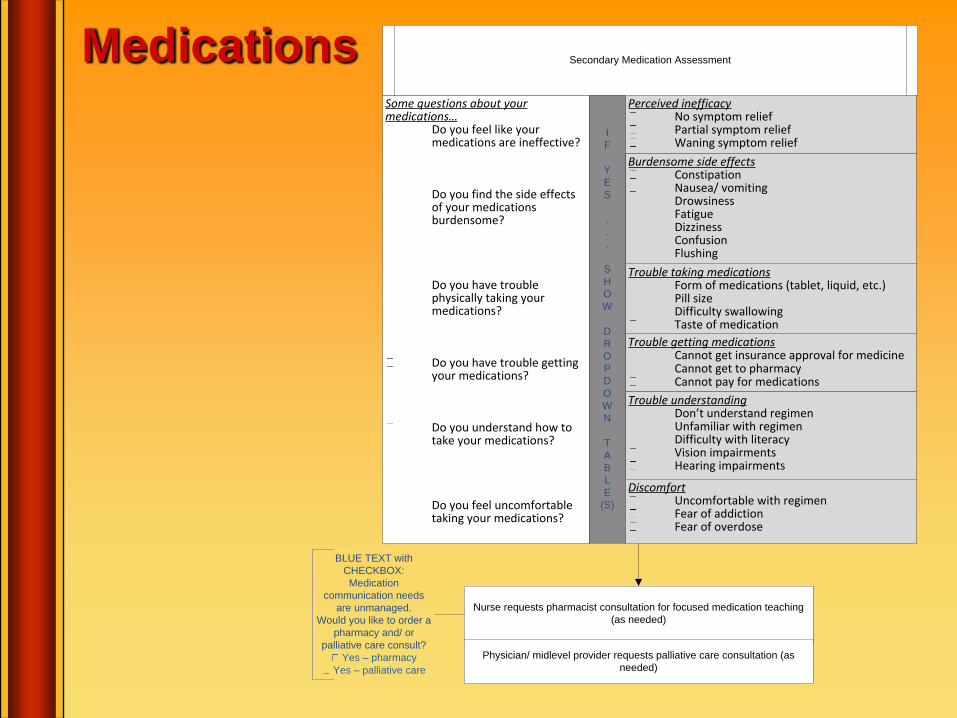
MedicationsSome questions about your medications…
Do you feel like your medications are ineffective?
Do you find the side effects of your medications burdensome?
Do you have trouble physically taking your medications?
Do you have trouble getting your medications?
Do you understand how to take your medications?
Do you feel uncomfortable taking your medications?
Secondary Medication Assessment
Trouble getting medicationsCannot get insurance approval for medicineCannot get to pharmacyCannot pay for medications
Trouble taking medicationsForm of medications (tablet, liquid, etc.)Pill sizeDifficulty swallowingTaste of medication
Burdensome side effectsConstipationNausea/ vomitingDrowsinessFatigueDizzinessConfusionFlushing
Trouble understandingDon’t understand regimenUnfamiliar with regimenDifficulty with literacyVision impairmentsHearing impairments
I
F
Y
E
S
.
.
.
S
H
O
W
D
R
O
P
D
O
W
N
T
A
B
L
E
(S)
Nurse requests pharmacist consultation for focused medication teaching
(as needed)
Physician/ midlevel provider requests palliative care consultation (as
needed)
Perceived inefficacyNo symptom reliefPartial symptom reliefWaning symptom relief
DiscomfortUncomfortable with regimenFear of addictionFear of overdose
BLUE TEXT with
CHECKBOX:
Medication
communication needs
are unmanaged.
Would you like to order a
pharmacy and/ or
palliative care consult?
Yes – pharmacy
Yes – palliative care

Overwhelmed
Depression screenAre you depressed?
YesNo
Anxiety screenAre you suffering from anxiety?
YesNo
Overwhelmed Assessment
Do you have anyone I can call to be with you right now?Yes – contact support directlyNo
I could use support in the following areas:Coping with IllnessSpiritualityCounselingSupport GroupsGetting support for caregiver(s)
Nurse provides bedside support and elicits information to inform potential
consult choice
CHECK BOX:
Provided bedside
counseling
If yes (depressed):
Suicidality Screen
Are you suicidal?YesNo
Normal procedures of hospital
to address suicidality
Nurse requests social work consultation (as needed)
BLUE TEXT with
CHECKBOX:
Patient is
overwhelmed.
Would you like to
order a social work,
chaplaincy, and/ or
palliative care consult?
Yes – social work
Yes – chaplaincy
Yes – palliative care
Physician/ midlevel provider requests palliative care consultation (as
needed)
Nurse requests chaplaincy consultation (as needed)
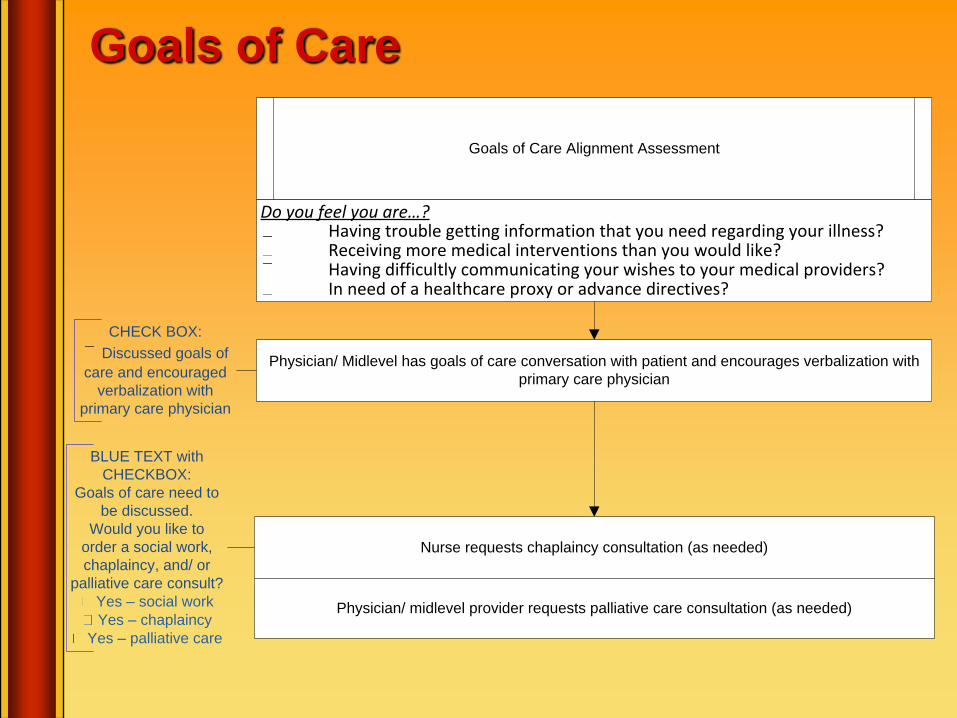
Goals of Care
Goals of Care Alignment Assessment
Physician/ Midlevel has goals of care conversation with patient and encourages verbalization with
primary care physician
Do you feel you are…?Having trouble getting information that you need regarding your illness?Receiving more medical interventions than you would like?Having difficultly communicating your wishes to your medical providers?In need of a healthcare proxy or advance directives?
BLUE TEXT with
CHECKBOX:
Goals of care need to
be discussed.
Would you like to
order a social work,
chaplaincy, and/ or
palliative care consult?
Yes – social work
Yes – chaplaincy
Yes – palliative care
Physician/ midlevel provider requests palliative care consultation (as needed)
Nurse requests chaplaincy consultation (as needed)
CHECK BOX:
Discussed goals of
care and encouraged
verbalization with
primary care physician

Patient reassessed at end of stay
Post ED Visit
Admit / Discharge
Patient perspective of care:
A survey of patient centered
outcomes only for questions with
above threshold score at first
SPEED
How much are
you suffering
from pain?
How much
difficulty are
you having
getting your
care needs met
at home?
How much
difficulty are you
having with
communication
with your
medications?
How much are
you suffering
from feeling
overwhelmed?
How much difficulty
are you having
getting medical
care that fits with
your goals?
Second SPEED questions are
administered upon admission or
discharge only for questions above
threshold at first SPEED
4. Summary of care provided by ED
What could providers have done better to assess and respond
to...(your pain, your care needs, your difficulty with medications,
your feeling of being overwhelmed, your goals)?
Patient feedback opportunity:
Only for questions with above
threshold score at first SPEED
5. Admit/ Discharge survey
How much did providers do everything they could to help
with...(your pain, your care needs, your difficulty with medications,
your feeling of being overwhelmed, your goals)? NEVER,
SOMETIMES, USUALLY or ALWAYS
6. Follow-up surveyPatient follow-up survey conducted by
research assistant
58

Future Considerations
59

Fiscal Imperatives
Emphasis on symptom assessments and
interventions with improved quality of life
outcomes and decreased hospitalization
Early ED palliative care has been shown to
decrease hospital stay and increase quality
60
Education and Research
Addition of core domains of palliative care to
the Model of Clinical Practice in EM
Define quality of life indicators, identify those
that can be addressed in ED
Focus on interventions, consultation
61

Summary
Palliative care is the active treatment of physical symptoms and social needs experienced by patients with terminal illness
EPEC-EM™ has defined core domains of palliative care are pertinent to EM practice
There are numerous opportunities for new knowledge and skills in palliative ED care62

EPEC-EM 2016Omni Chicago HotelSeptember 8 & 9www.epec.net
63






























