


Hysterectomy: GKS: Recommendations for pre-and postoperative treatment
GKS 27.9.2007
Anna-Mari Heikkinen
KYS naistenklinikka

Hysterectomy: Preoperative recommendationsThrombosis prophylaxis
Antibiotic prophylaxis
Other
Hysterectomy: Postoperative recommendationsThrombosis prophylaxisSick leaveOther
Käypä Hoito
”Laskimotukos ja keuhkoembolia” 2004, new version coming Preoperative prevention of venous
thromboembolism ”Leikkausta edeltävä arviointi ja hoito” will be
published 2007-2008 Special preoperative guidelines (cardiac stents,
varfarin treatment etc.)

Hysterectomy and prevention of venous thromboembolism: References Käypä Hoito: Laskimotukos ja keuhkoembolia
2004 Prevention and Treatment of Venous
Thromboembolism: International Consensus Statement 2006
ACOG Practice Bulletin: Clinical Management Guidelines for Ob/Gyn Number 84, August 2007
Hysterectomy and the risk of venous thromboembolism Gynecologic surgery without prophylaxis: 15-
40%
FINHYST 1996: Thromboembolism AH 0,2% VH 0,2% LH 0,3%
FINHYST 2006: Only 2 cases of pulmonary embolism reported! Not a single venous thromboses of the lower limb were reported.
Hysterectomy and prevention of venous thromboembolism : Methods of choice Early mobilization! Graduated compression stockings (GCS) Intermittent pneumatic compression (IPC) LMWH
Enoxaparin (Klexane®) 40 mgx1 Dalteparin (Fragmin®) 5000 IUx1
Thrombin inhibitors Ximelagatran (Exanta®) Melagatraani (Melagatran®) Bivalirudin (Angiox®)
FX infibitor: Fondaparinux (Arixtra®)

Hysterectomy and prevention of venous thromboembolism: LMWH treatment 12 h preop, continuing >12 h after postop. OR: 6-12 h postoperatively Duration: Immobilization (hospitalization or 7-10 days?) Prolonged: 1 month Tiny / obese patients
Hysterectomy and prevention of venous thromboembolism: Estimation of risk LOW RISK: Risk of TE 2-3%
No prophylaxis (early mobilization) Duration of operation less than 45 min < 40 years No risk factors
MODERATE RISK: Risk of TE 10-20%
HIGH RISK: Risk of TE 40-80%GCS (IPC) + LMWH 1 month Cancer Previous TE (idiopatic/recurent) Coagulopathy Severe medical illness/complication 6 w postpartum

Hysterectomy and prevention of venous thromboembolism: Moderate risk A. LMWH during hospitalization
B. LMWH during hospitalization, 7-10 days if risk factors
C. LMWH 7-10 if risk factors,
GCS if no risk factors
IMMOBILIZATION ----- HOSPITALIZATION

Risk factors 7-10 d prophylaxis: 1-2 p4 w prophylaxis: > 3 p
5p History of TE, coagulopathy, cancer, severe trauma3p Immobilization, paresis, pregnancy, puerperium1p Infection/complication
Age > 60yBMI > 30SmokingOC, HT, SERMInflammatory bowel diseaseHeart failure, MCIVenous disorder (varicosis, thromboflebitis)Central venous catheterizationAc/chr medical illness increasing risk of TE
When no LMWH prophylaxis? Uncomplicated operation and cure < 40-60y patient, no risk factors Early mobilization, short hospitalization
Intermittent pneumatic compression (IPC) Level 2 evidence Possible indications during hysterectomy
High risk patient: LMWH + IPC Moderate risk patient, prolonged immobilization:
LMWH + IPC Moderate risk patient, contraindication for LMWH
Other medications affecting coagulation
ASA (50-100mg): Stop 1 week preop Plavix®: Stop 1 week preop Marevan®: Stop 4-5 d preop. Bridge therapy! KÄYPÄ HOITO: Leikkausta edeltävä arvio ja
hoito (2007 -2008)
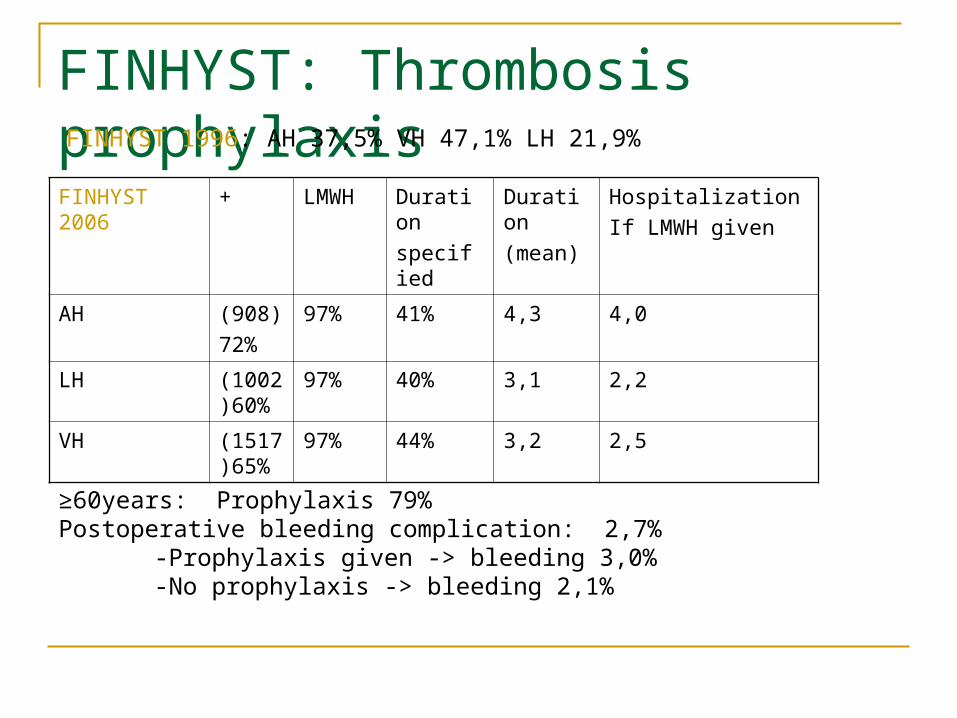
FINHYST: Thrombosis prophylaxisFINHYST 2006
+ LMWH Duration
specified
Duration
(mean)
Hospitalization
If LMWH given
AH (908)
72%
97% 41% 4,3 4,0
LH (1002)60%
97% 40% 3,1 2,2
VH (1517)65%
97% 44% 3,2 2,5
FINHYST 1996: AH 37,5% VH 47,1% LH 21,9%
≥60years: Prophylaxis 79%Postoperative bleeding complication: 2,7%
-Prophylaxis given -> bleeding 3,0%-No prophylaxis -> bleeding 2,1%

Hysterectomy and prevention of venous thromboembolism :GKS recommendation LOW RISK: No prophylaxis (early mobilization)
Duration of operation less than 45 min , <40 years patient, no risk factors
MODERATE RISK : ”Normal hysterectomy” GCS alone if no risk factors LMWH always > 60 yr, or < 60yr and at least 1 risk factor 7-10 days prophylaxis according pre- and postop. risk factors
HIGH RISKI: GCS (IPC) +LMWH 1 month Cancer Previous TE (idiopatic/recurent) Coagulopathy Severe medical illness/complication 6 w postpartum
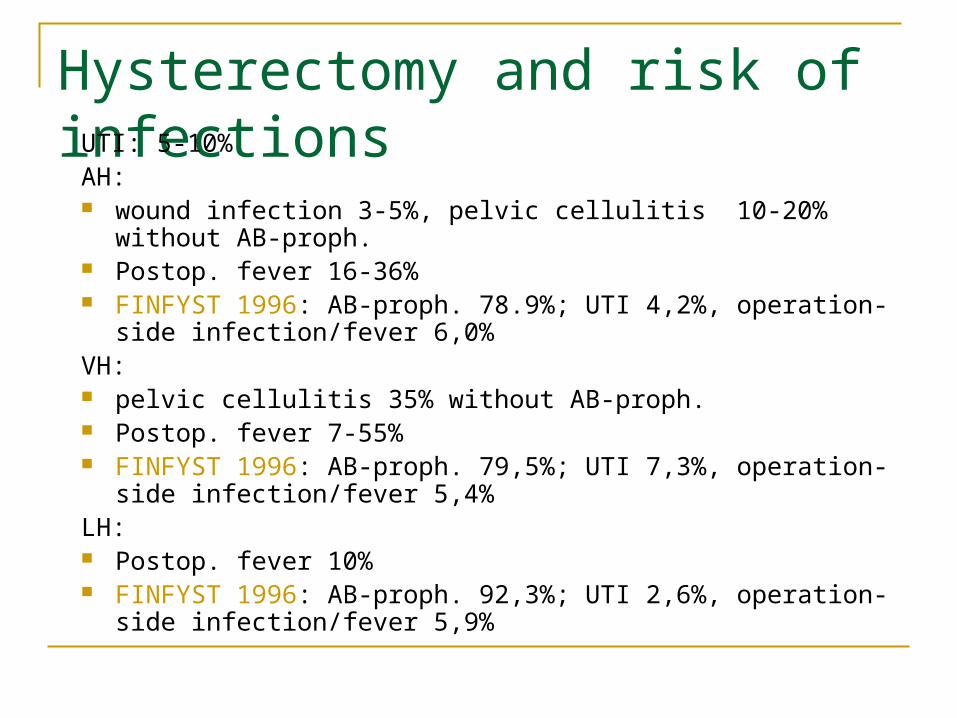
Hysterectomy and risk of infectionsUTI: 5-10%
AH: wound infection 3-5%, pelvic cellulitis 10-20% without AB-proph. Postop. fever 16-36% FINFYST 1996: AB-proph. 78.9%; UTI 4,2%, operation-side
infection/fever 6,0% VH: pelvic cellulitis 35% without AB-proph. Postop. fever 7-55% FINFYST 1996: AB-proph. 79,5%; UTI 7,3%, operation-side
infection/fever 5,4%LH: Postop. fever 10% FINFYST 1996: AB-proph. 92,3%; UTI 2,6%, operation-side
infection/fever 5,9%

Antibiotic prophylaxis
ACOG Practice Bulletin (Ob Gyn July/2006):
Always antibiotic prophylaxis before hysterectomy
> 30 prospective clinical trials 2 meta-analysis
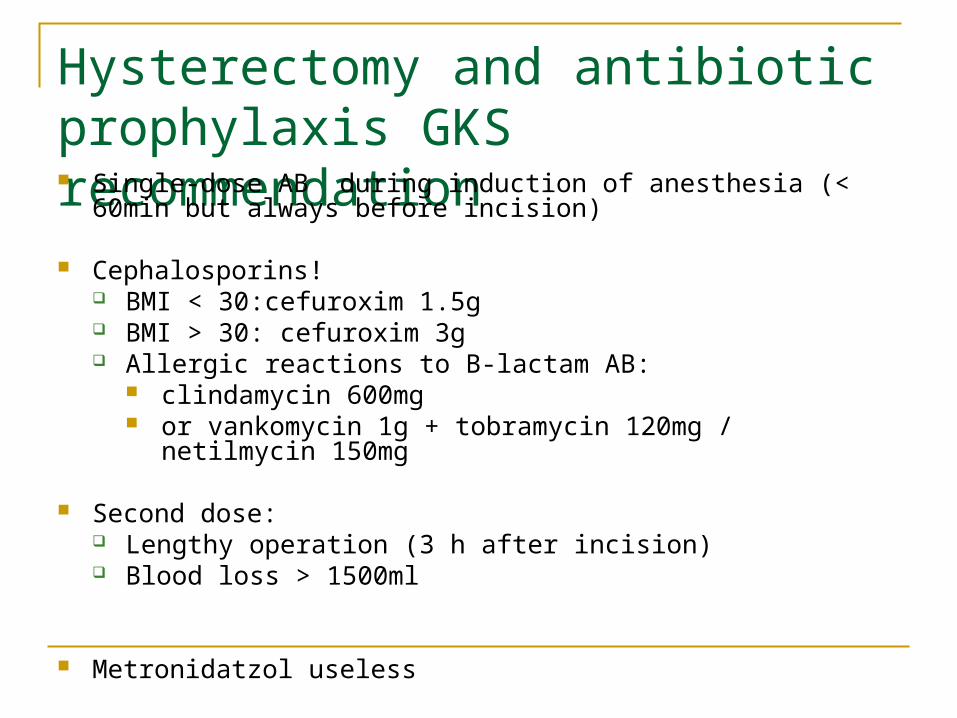
Hysterectomy and antibiotic prophylaxis GKS recommendation Single-dose AB during induction of anesthesia (< 60min but always
before incision)
Cephalosporins! BMI < 30:cefuroxim 1.5g BMI > 30: cefuroxim 3g Allergic reactions to B-lactam AB:
clindamycin 600mg or vankomycin 1g + tobramycin 120mg / netilmycin 150mg
Second dose: Lengthy operation (3 h after incision) Blood loss > 1500ml
Metronidatzol useless
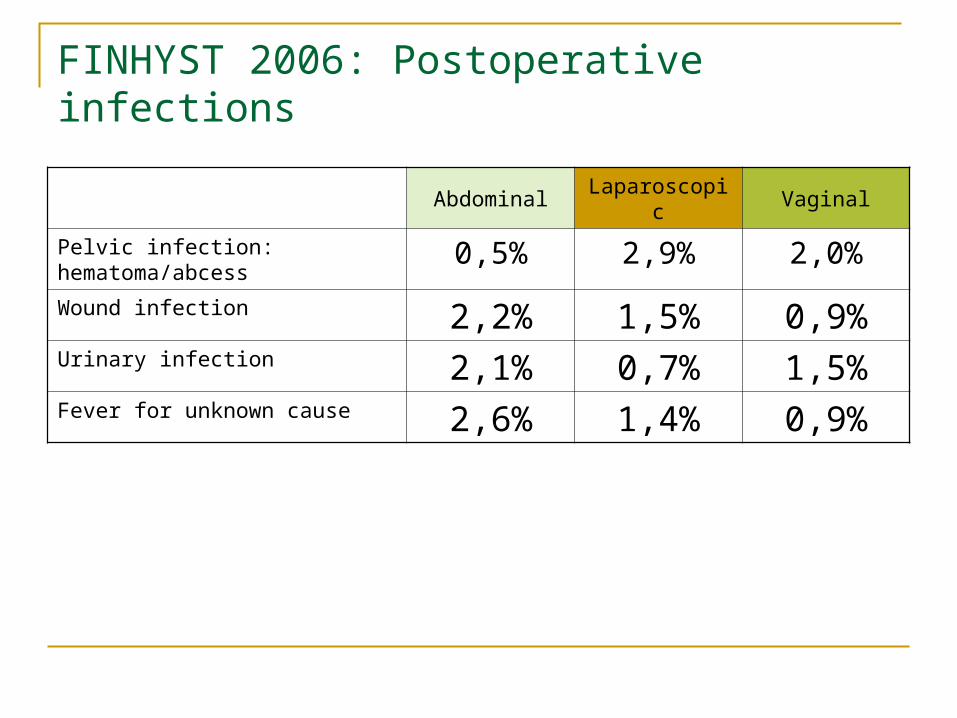
FINHYST 2006: Postoperative infections
Abdominal Laparoscopic Vaginal
Pelvic infection: hematoma/abcess 0,5% 2,9% 2,0%Wound infection 2,2% 1,5% 0,9%Urinary infection 2,1% 0,7% 1,5%Fever for unknown cause 2,6% 1,4% 0,9%
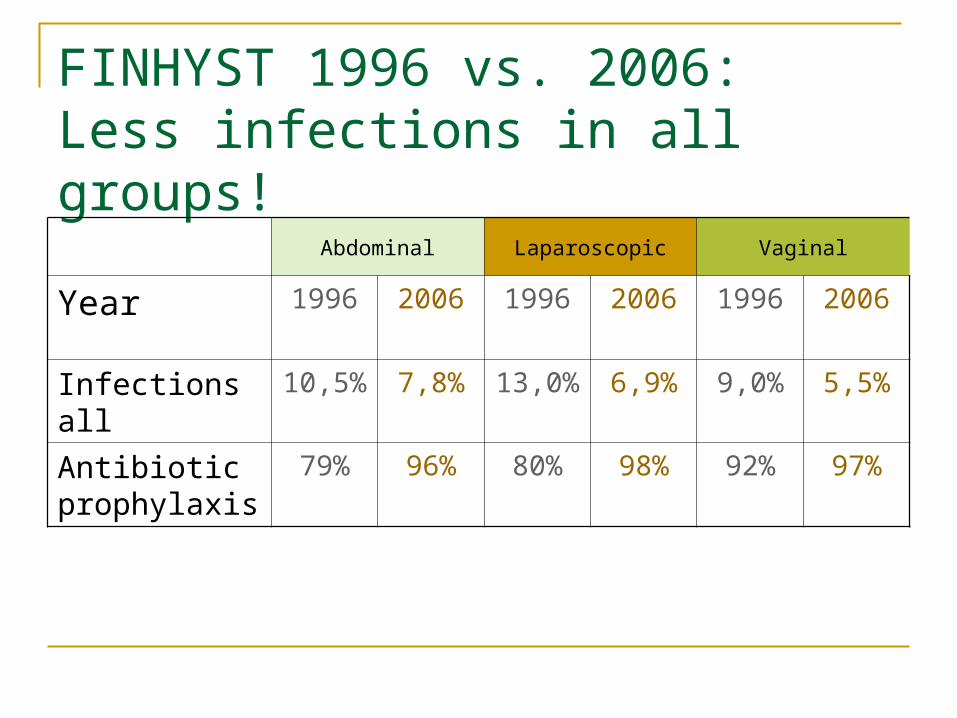
FINHYST 1996 vs. 2006:Less infections in all groups!
Abdominal Laparoscopic Vaginal
Year 1996 2006 1996 2006 1996 2006
Infections all 10,5% 7,8% 13,0% 6,9% 9,0% 5,5%
Antibiotic prophylaxis
79% 96% 80% 98% 92% 97%
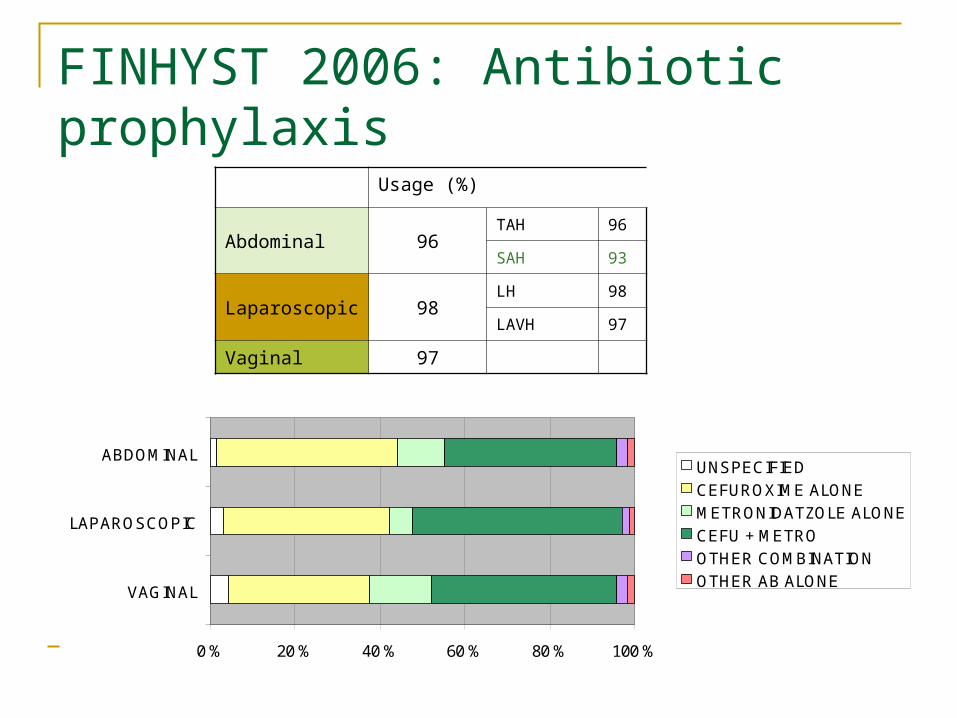
FINHYST 2006: Antibiotic prophylaxis
0 % 20 % 40 % 60 % 80 % 100 %
VAGINAL
LAPAROSCOPIC
ABDOMINALUNSPECIFIED
CEFUROXIME ALONE
METRONIDATZOLE ALONE
CEFU + METRO
OTHER COMBINATION
OTHER AB ALONE
Usage (%)
Abdominal 96TAH 96
SAH 93
Laparoscopic 98LH 98
LAVH 97
Vaginal 97
Reasons to NOT give routine prophylactic metronidatzol Interactions: Varfarin!! Bacterial resistance Costs
-> indicated only if bowel injury

Costs of prophylaxis (examples of hospital prices /dose) Klexane 40 mg 3.80€ Fragmin 5000 IU 3.60€ Kefuroksiimi 1.5: 1.80€ Metronidatsoli 500 mg 3.10€ Klindamysiini 600 mg 5.50€ Siprofloksasilliini 200 mg 14.00€ Vankomysiini 1 g 5.60€ Tobramysiini 120 mg6.40€ Netilmysiini 10 mg 7.00€
Postoperative treatment
Moller C et al 2001: Variation in recommendations for hysterectomy and vaginal surgery patients in Denmark
Sick leave: 4 w (1-8 w) work without heavy lifting, 6 w (2-12 w) work with heavy lifting
Lifting restrictions : 2-15 kg, 2-12 weeks No sex intercourse: 4 w (0-12 w)
SICK leave after hysterectomy
No evidence based medicine
Persson et al. 2006. Rand. multicenter trial
AH (n=56) vs. LH (n=63)
Sick leave 14 days
Final sick leave:
AH: 33.5vrk LH: 26vrk
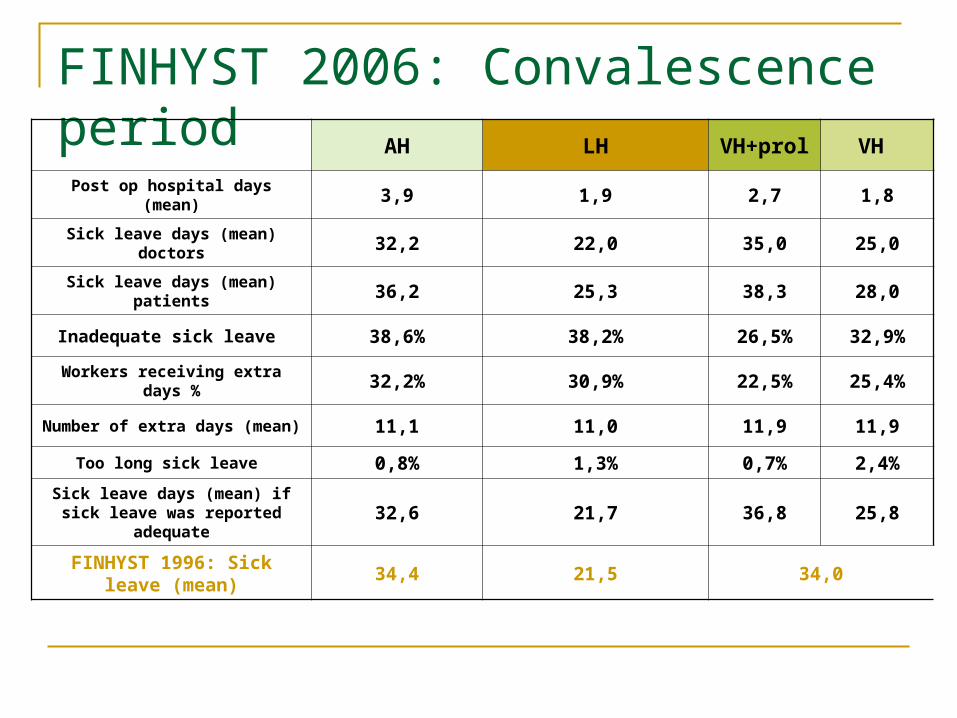
FINHYST 2006: Convalescence period AH LH VH+prol VH
Post op hospital days (mean) 3,9 1,9 2,7 1,8
Sick leave days (mean) doctors 32,2 22,0 35,0 25,0
Sick leave days (mean) patients 36,2 25,3 38,3 28,0
Inadequate sick leave 38,6% 38,2% 26,5% 32,9%
Workers receiving extra days % 32,2% 30,9% 22,5% 25,4%
Number of extra days (mean) 11,1 11,0 11,9 11,9
Too long sick leave 0,8% 1,3% 0,7% 2,4%
Sick leave days (mean) if sick leave was reported adequate 32,6 21,7 36,8 25,8
FINHYST 1996: Sick leave (mean)
34,4 21,5 34,0
Postoperative recommendations (HUS, TAYS, TYKS, OYS, PKKS, KYS):
Sick leave: AH: 4 w LH: 2-3 w VH: 2-3 w VH+prolapse: 3-6 w
No sex intercourse: Postop. control or 4 w Postop. control: 4/6 Other very specific restrictions: Preop peräruiske
kaikille, istumakielto laskeumissa 2vi, ei saunaan 1vi, ei ammekylpyjä/uintia, ei kovia löylyjä, alapesu vähintään 2x/vrk, ei tampoonia, ei raskaita töitä 1-2 viikkoon, PAPA 5v välein, gyn tutkimus vuosittain, ei pyöräilyä ennen jt, ei autolla ajoa 2 viikkoon jne…

Sick leave after hysterectomy:GKS recommendations LH: 2-3 weeks AH: 4 weeks VH, no prolaps surgery: 2-3 weeks VH + prolaps surgery : 4 weeks
Hysterectomy: Other GKS recommendations No pubic hair shaving, shortening if
necessary No bowel preparation No routine abd. cavity drainage No lifting restrictions (no heavy work during
sick leave) No sexual intercourse during sick leave No other specific restrictions to patient
guidelines No routine postoperative control
KIITOS!

![Dnevni avaz [broj 4315, 27.9.2007]](https://static.cupdf.com/doc/110x72/577d2f701a28ab4e1eb1b6e0/dnevni-avaz-broj-4315-2792007.jpg)




























