HORMONES OF THE
ADRENAL GLANDS
LEC. 4

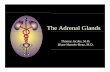
The adrenal glands, as their name implies (ad = near; renal = kidneys), lie atop the kidneys. Each consists of an outer portion, called the cortex, and an inner portion, called the medulla. These portions, like the anterior pituitary and the posterior pituitary, have no functional connection with one another.

Adrenal MedullaThe adrenal medulla secretes norepinephrine and epinephrine under conditions of stress. They bring about all those responses we associate with the "fight or flight" reaction: increasing blood pressure, opening airways in the lungs, narrowing blood vessels in the skin and intestine to increase blood flow to major muscle groups,. This increased circulation to the muscles causes them to have more stamina than usual. In times of emergency, the sympathetic nervous system initiates these responses, but they are maintained by secretions from the adrenal medulla.
HO
OH
NH
HO
epinephrine
HO
OH
H2N
HO
norepinephrine

The adrenal medulla releases epinephrine and norepinephrine into the bloodstream (normally in a ratio approximately 17:3). These hormones help us and other animals to cope with situations that threaten survival.
The adrenal medulla is not essential for life, and no diseases of deficiency are known.
Therapeutic use of these hormones is based on the pharmacology of sympathomimetic amines and not on the principle of replacement.

• Epinephrine elicits vasoconstrictor and vasopressor responses, acting in general as a sympathomimetic agent of rapid onset but brief duration of action.
• Epinephrine is administered by intravenous or intramyocardial injection in cardiac arrest.
• The labile catechol function precludes oral administration of epinephrine, which must be administered by subcutaneous or intramuscular injection.

Epinephrine
Biosynthesis. From the biosynthetic viewpoint, epinephrine may be considered an alkaloidal amine of the phenylpropanoid type. Its derivation from tyrosine has been demonstrated experimentally.
Tyrosine
OHO
NH2
OH
Epinephrine
NH
OH
OH
HO
H
CH3


–Epinephrine may be isolated as a hormone from adrenal medulla or may be prepared synthetically.
–Dextrorotatory epinephrine is almost completely inactive, and optically inactive mixtures have approximately half the activity of natural epinephrine.
–PRESCRIPTION PRODUCTS. Adrenalin®, Epifrin®, Epinal®, Eppy/N®, Epitrate®, Glaucon®, and Sus-Phrine®.

Levarterenol or norepinephrine
Levarterenol is a sympathetic stimulant closely related in chemical structure and pharmacologic action to epinephrine.
Its chief difference in clinical utility lies in its predominantly alpha-receptor adrenergic activity. It is a strong peripheral vasoconstrictor and is especially useful in restoration of blood pressure in acute hypotensive situations.
PRESCRIPTION PRODUCT. Levophed®.

Adrenal CortexAlthough the adrenal medulla can be removed with no ill effects, the adrenal cortex is absolutely necessary to life. The two major classes of hormones made by the adrenal cortex are the glucocorticoids and the mineralocorticoids. The cortex also secretes a small amount of male sex hormone and an even smaller amount of female sex hormone. All of these hormones are steroids.

Glucocorticoids•Of the various glucocorticoids, the hormone responsible for the greatest amount of activity is Cortisol.
•Cortisol promotes the hydrolysis of muscle protein to amino acids that enter the blood. This leads to an increased level of glucose when the liver converts these amino acids to glucose.
•In opposition to insulin, therefore, cortisol raises the blood glucose level.

Cortisol and cortisone counteract
the inflammatory response, which
leads to the pain and the swelling
of joints in arthritis and bursitis.
The administration of cortisol or
cortisone aid these conditions
because they reduces
inflammation.
O
O OH
OHHO
H
H
H
Cortisol
O
O
HO
HO
O
H
H
H
Cortisone

• The secretion of cortisol or cortisone by the adrenal cortex is under the control of the anterior pituitary hormone ACTH.
• The hypothalamus produces a releasing hormone (CRH) that stimulates the anterior pituitary to release ACTH. ACTH in turn stimulates the adrenal cortex to secrete cortisol and cortisone, which regulate their own synthesis by negative feedback of both CRH and ACTH synthesis.

MineralocorticoidsThe secretion of mineralocorticoids, aldosterone and desoxycorticosterone, are not under the control of the anterior pituitary.• Aldosterone is not available for
therapeutic use.• Aldosterone regulates the level of
sodium and potassium in blood, its primary target organ being the kidney, where it promotes renal absorption of sodium and renal excretion of potassium.
O
OH
O
HO
H
H
H
Aldosterone
O
CH3
CH3OH
O
H
H H
Desoxycorticosterone

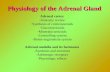
If the blood level of sodium is low, the kidneys secrete renin.
The increased renin acts via the increased production of angiotensin I and II to stimulate aldosterone secretion.
Aldosterone promotes reabsorption of sodium by the kidneys; when the sodium level in the blood rises, the kidneys stop secreting renin.
Renin-angiotensin-aldosterone system.


• The level of sodium is particularly important to the maintenance of blood pressure because its concentration indirectly regulates the secretion of aldosterone.
• When the blood level of sodium is low, the kidneys secrete renin. Renin is an enzyme that converts the plasma protein angiotensinogen to angiotensin I, which becomes angiotensin II in the lungs. Angiotensin II stimulates the adrenal cortex to release aldosterone. This is called the renin-angiotensin-aldosterone system.

The effect of this system is to raise the blood pressure in two ways.
First, angiotensin II constricts the arteries directly.
secondly, aldosterone causes the kidneys to reabsorb sodium. When the blood level of sodium is high, water is reabsorbed, and blood volume and pressure are maintained.
Cortisol, which raises the blood glucose level, and aldosterone, which raises the blood sodium level, are two hormones secreted by the adrenal cortex.

Synthetic glucocorticoids
•The potential therapeutic utility of the glucocorticoids has promoted intensive efforts to discover modifications of the naturally occurring hormones that will be more potent and more specific in their activity.
•The best success has been achieved with desired increases in potency. Prednisone (Deltasone®, Meticorten®) and prednisolone (Delta-Cortef®, Sterane®) represent early achievements in these efforts.

Elimination of any mineralocorticoid activity has been a major objective; a degree of success has been attained with such compounds as:₋ betamethasone (Celestrone®)₋ dexamethasone (Decadron®,
Dexone®, Hexadrol®) ₋ methylprednisolone (Medrol®)₋ paramethasone (Haldrone®)₋ triamcinolone (Aristocort®,
Kenacort®).
Cortisone Cortisol
O
CH3
CH3OH
O
F
HO
H
CH3OH
H
Betamethasone
O
CH3
CH3OH
O
F
HOOH
CH3
H
H
Dexamethasone
O
CH3
CH3OH
O
CH3
HOOH
H
H H
Methylprednisolone
O
F
CH3
HOCH3
CH3
O
OHOH
H
H H
Paramethasone
CH3
CH3
OOH
OHOHHO
O
H
F H
Triamcinolone
O
CH3
OCH3 OH
OHO
H
H H
CH3
CH3
OOH
O
HOOH
H
H H

It is interesting to note that successful modifications in the basic steroid molecule fall into 4 categories:
1. 1-dehydrogenation
2. 16-hydroxylation
3. 6- or 9-fluorination
4. 6-, 16-, or 16-methylation.

Sex Hormones
The adrenal cortex produces a small amount of both male and female sex hormones.
In males, the cortex is a source of female sex hormones, and in females, it is a source of male hormones.
A tumor in the adrenal cortex can cause the production of a large amount of sex hormones, which can lead to feminization in males and masculinization in females.

DISORDERS
•When the level of adrenal cortex hormones is low, a person begins to suffer from Addison disease.
•When the level of adrenal cortex hormones in the body is high, a person suffers from Cushing syndrome.

•Addison Disease • Because of the lack of cortisol, the Addison disease patient is unable to maintain the glucose level of the blood, tissue repair is suppressed, and there is a high susceptibility to any kind of stress. Even a mild infection can cause death.
•Due to the lack of aldosterone, the blood sodium level is low, and the person experiences low blood pressure along with acidosis and low pH. In addition, the patient has a peculiar bronzing of the skin.

• Cushing Syndrome In Cushing syndrome, a high level of cortisol causes a tendency toward diabetes mellitus, a decrease in muscular protein, and an increase in subcutaneous fat. Because of these effects, the person usually develops thin arms and legs and an enlarged trunk. Due to the high level of sodium in the blood, the blood is basic and the patient has hypertension and edema of the face, which gives the face a moon shape.