



HIV associated renal disease
Dr David Makanjuola
Dr Stephen Sampson

HISTOPATHOLOGICAL ASPECTS
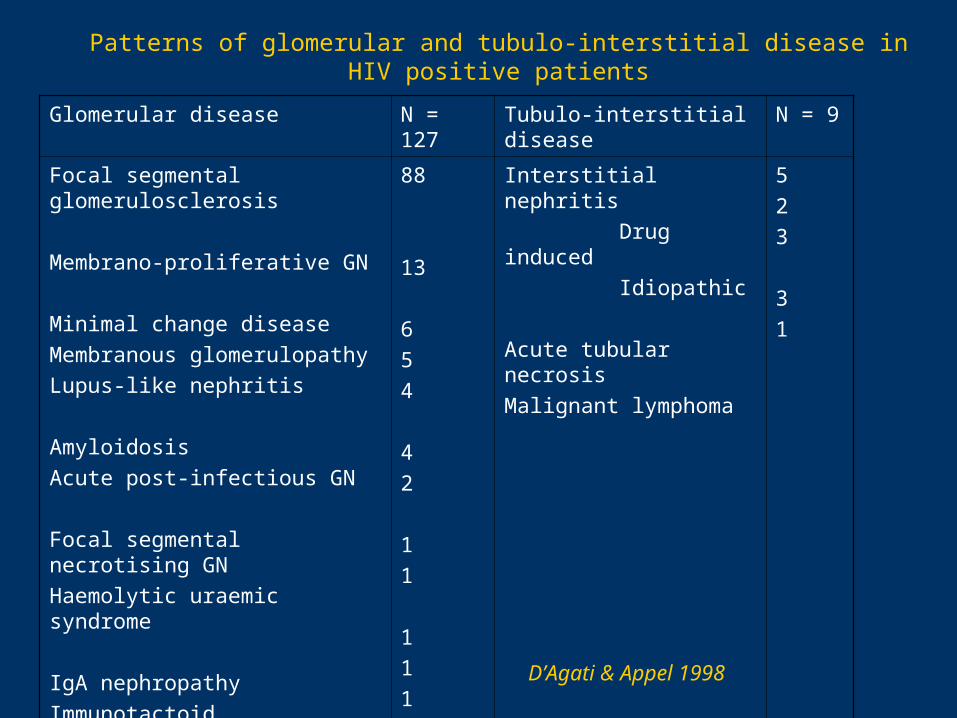
Patterns of glomerular and tubulo-interstitial disease in HIV positive patients
Glomerular disease N = 127 Tubulo-interstitial disease N = 9
Focal segmental glomerulosclerosis
Membrano-proliferative GN
Minimal change disease
Membranous glomerulopathy
Lupus-like nephritis
Amyloidosis
Acute post-infectious GN
Focal segmental necrotising GN
Haemolytic uraemic syndrome
IgA nephropathy
Immunotactoid glomerulopathy
End-stage kidney
88
13
6
5
4
4
2
1
1
1
1
1
Interstitial nephritis
Drug induced
Idiopathic
Acute tubular necrosis
Malignant lymphoma
5
2
3
3
1
D’Agati & Appel 1998

Normal renal biopsy (PAS stain)

Mesangial proliferation and focal sclerosis

Florid interstitial nephritis in a patient with HIV
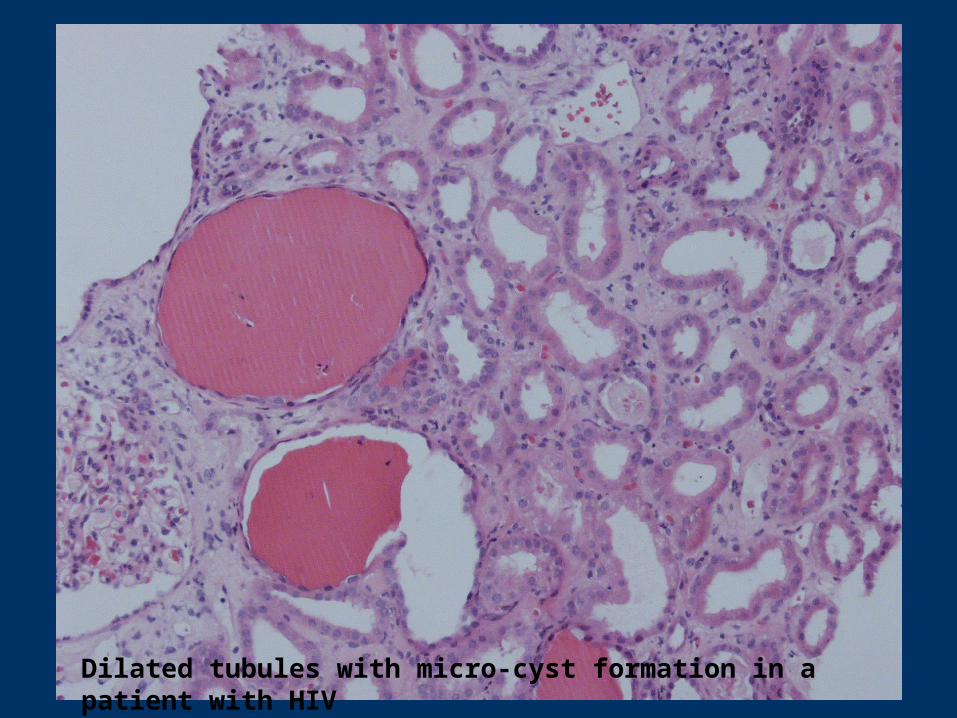
Dilated tubules with micro-cyst formation in a patient with HIV
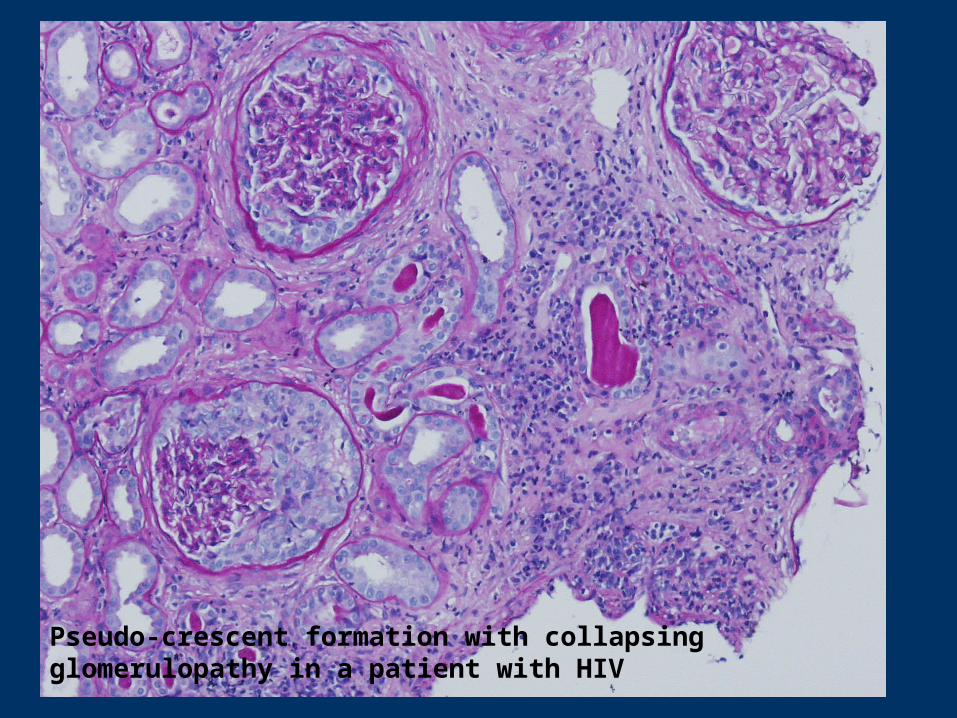
Pseudo-crescent formation with collapsing glomerulopathy in a patient with HIV
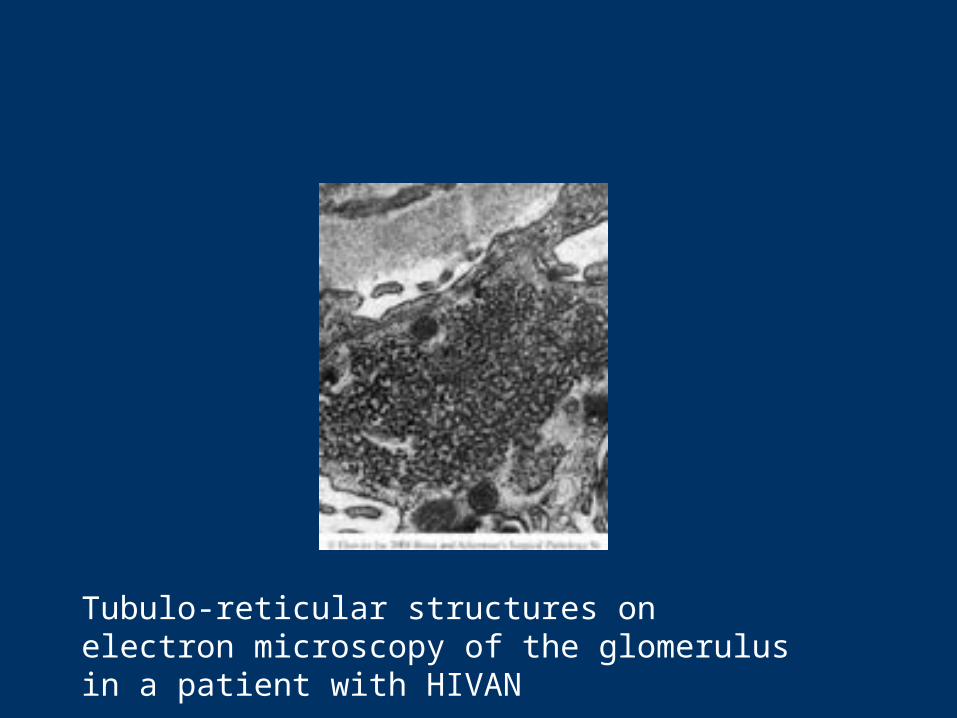
Tubulo-reticular structures on electron microscopy of the glomerulus in a patient with HIVAN

CLINICAL ASPECTS
Overview of HIV-associated renal disease:
• Acute renal failure (ARF) – common, with causes broadly similar to those of the non-HIV population, together with some specific to pts with HIV
• Chronic renal failure (CRF) - largely due to focal glomerulosclerosis (classical HIVAN)/other chronic glomerulopathies
Aetiology of ARF in HIV:
• Pre-renal• Acute Tubular Necrosis• Allergic interstitial nephritis• Rapidly progressive immune-complex-GN• Thrombotic Tthrombocytopaenic Purpura
(TTP) & Haemolytic Uraemic Syndrome (HUS)• Obstructive nephropathy from crystal-induced
renal failure• Rhabdomyolysis & myoglobinuric renal failure
Aetiology of ARF in HIV:• Pre-renal
– hypovolaemia due to diarrhoea/vomiting/infections– hypotension from sepsis/bleeding/fluid loss
Acute Tubular Necrosis
due to hypovolaemia, nephrotoxins, sepsis etc is the
commonest cause of intrinsic ARF in HIV pts
Some of the nephrotoxins implicated:– Pentamidine, – amphotericin B, – foscarnet, – aminoglycosides, – ritonavir, – radio-contrast material
ARF in HIV, continued:
• Acute tubulointerstitial nephritis is usually a complication of drugs such as:– Trimethoprim-sulfamethoxazole– Rifampicin– Foscarnet– Sulfadiazine– ciprofloxacin
• TTP & HUS more common in HIV-sero+ve & AIDS– Rx with plasmapheresis using FFP– Can occur at any stage of HIV infection & prognosis is
poor
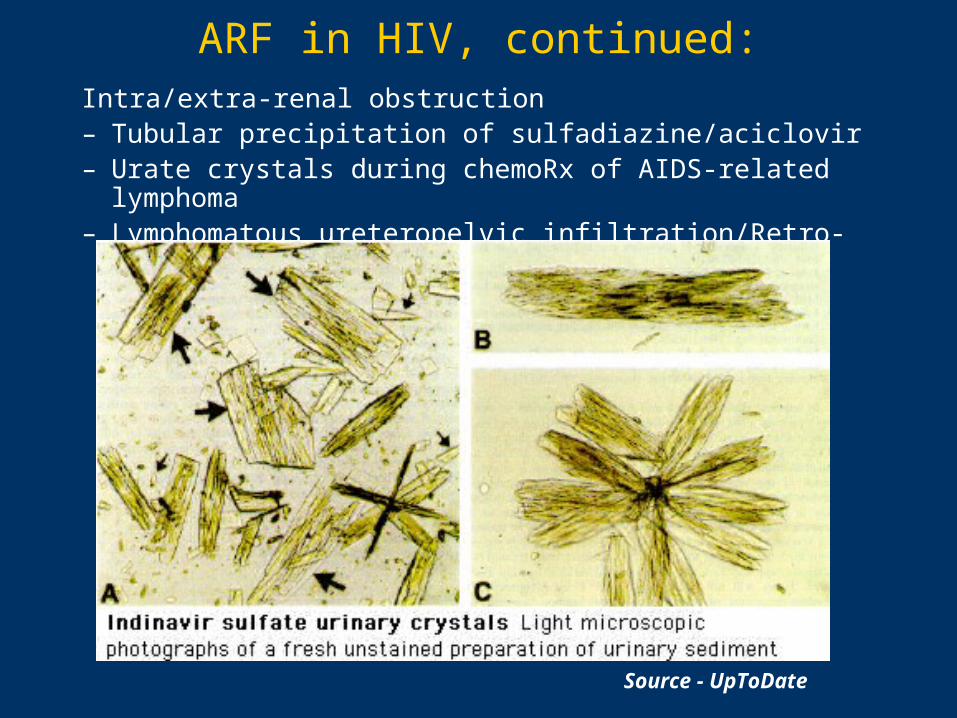
ARF in HIV, continued:Intra/extra-renal obstruction– Tubular precipitation of sulfadiazine/aciclovir– Urate crystals during chemoRx of AIDS-related lymphoma– Lymphomatous ureteropelvic infiltration/Retro-peritoneal fibrosis
Source - UpToDate
HIVAN • HIVAN is a disease of progressive renal failure with both
glomerular & tubulointerstitial components in sero positive patients
• A description of a new renal syndrome in patients with AIDS 1st reported in 1984
• Rao et al described focal & segmental glomerulosclerosis in 9 pts with AIDS & the nephrotic syndrome in New York city
• A histological pattern similar to heroin-associated nephropathy was recognised, but a much more rapid deterioration in renal f(x) was noted
• This HIV-associated focal glomerulosclerosis or “HIVAN” is the commonest HIV nephropathy found in biopsy series
HIVAN: Epidemiology• Accounts for 60-70% of chronic glomerular lesions in
adults with HIV but only 33% of such lesions in children
• Strong predilection for blacks 12:1
• HIVAN usually occurs in pts with low CD4 counts– But can occur in otherwise asymptomatic sero-positive individuals– Has been seen in all groups at risk for AIDS, including perinatally
acquired transmission
• Strongly associated with IV drug use– up to 50% of patients in some case series have a history of intra-
venous drug use
HIVAN: Clinical features
• 1. Usually presents with proteinuria, renal failure or the nephrotic syndrome
• 2. The onset of nephropathy is often abrupt with massive proteinuria and uraemia – these lesions may present as acute renal failure
• 3. The blood pressure is often normal, even in advanced stages of renal failure
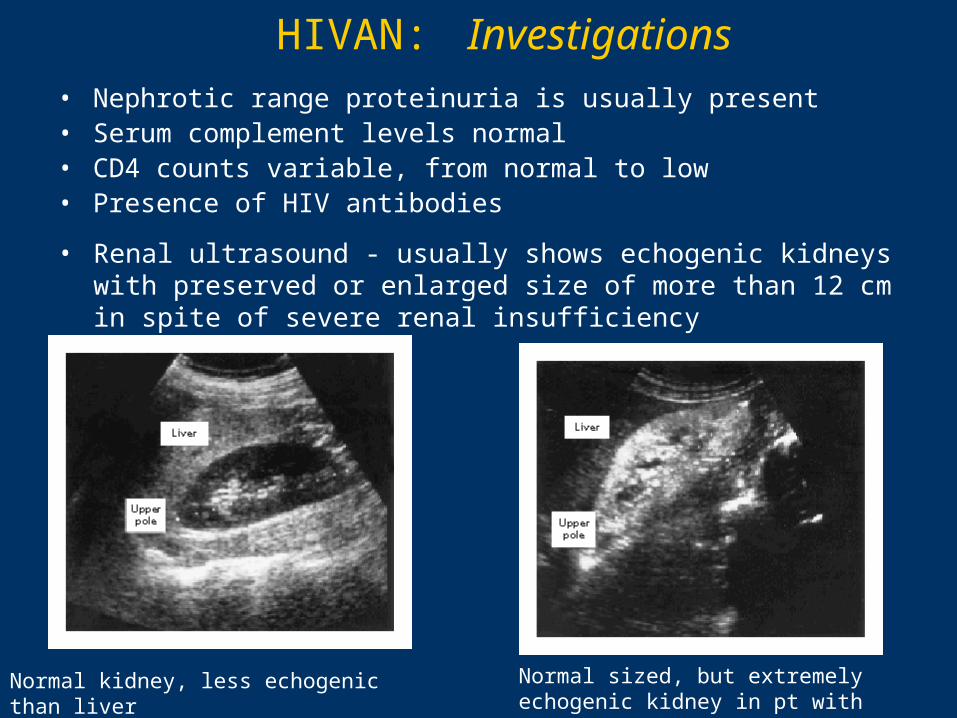
HIVAN: Investigations• Nephrotic range proteinuria is usually present• Serum complement levels normal• CD4 counts variable, from normal to low• Presence of HIV antibodies
Normal kidney, less echogenic than liver Normal sized, but extremely echogenic kidney in pt with HIVAN
• Renal ultrasound - usually shows echogenic kidneys with preserved or enlarged size of more than 12 cm in spite of severe renal insufficiency
HIVAN: Clinical course
• The progression of renal insufficiency is rapid, especially in nephrotic patients and in blacks, with a median time from presentation to dialysis of 11 weeks
• Children with HIV-associated glomerulosclerosis have a more protracted clinical course, with a median time from presentation to end-stage renal failure of about 12 months
• Survival is dictated by the clinical progression of AIDS and is independent of the renal disease

HIVAN: Management strategies
• There are no prospective randomised controlled trials of treatment in HIVAN
• Some evidence exists for the following however:
1) Zidovudine • isolated case reports noting temporary remission of proteinuria or delay in occurrence of renal failure
2) Immunosuppressive agents (steroids/cyclosporin A)• Concerns about the use of these agents in an infected population• Significant improvements in proteinuria and renal function have been reported with
use of high dose steroids in pre-HAART era• It is likely that those with significant interstitial inflammation are the most likely to
respond to steroid therapy• Long-term results of these studies suggest high morbidity from opportunistic
infection• Cyclosporin used in paediatric patients with biopsy proven HIVAN has achieved
remissions; with relapses on discontinuation due to intercurrent infection
3) Highly Active Anti-Retroviral Therapy (HAART)
4) Angiotensin Converting Enzyme Inhibitors (ACEIs)
HIVAN: Evidence for HAART
• Wali et al (1998)• 37yr old with Cr 203 -> 770 in 5/52 and biopsy proven HIVAN
• Initiation of HAART for 13/52 (12/52 dialysis), allowed cessation of haemodialysis
• Proteinuria dropped from 9.9g/day to 0.7g/day, with Creatinine 132, fourteen weeks after stopping dialysis
• Viral load fell from 906,000 copies/mL to <500 copies/mL
• Repeat renal biopsy at time of discontinuation of dialysis revealed substantial improvement in histology
HIVAN: Possible mechanisms of benefit of HAART
– Suppression of viral replication felt to be a key factor
– ?viral proteins/cytokines released during active viral replication directly cytopathic to kidneys
– Recent evidence (Foster, 2004) suggests ‘non-viral’ actions of HAART may be equally important
– Protease inhibitors shown to inhibit reactive O2 species (ROS) generation and ROS-linked apoptosis of murine mesangial cells independent of HIV gene expression
– This anti-apoptotic non-virologic effect of protease inhibitors may be important in humans

HIVAN: ACEIs
• Wei et al (2003) • single centre prospective cohort study of the long-term effects of ACEIs
on renal survival in HIVAN
• 44 patients with biopsy proven HIVAN enrolled prior to severe renal insufficiency (Creatinine < 180) during period 5 yrs
• 28 patients received Fosinopril 10mg/d, 16 followed as controls
• Median renal survival of treatment group was 479.5 days, with only 1 patient developing ESRF
• All untreated patients progressed to ESRF, median renal survival was 146.5 days (P < 0.0001)
HIVAN: ACEIs
• RR of renal failure reduced with ACEI (RR = 0.003, P<0.0001)
• No significant differences between Rx and control groups in age, antiretroviral therapy, CD4 count, initial median Cr, or proteinuria
• Results suggest ACE inhibition initiated early in natural history of HIVAN may offer long-term benefits on renal survival
• ?Mechanism – altered glomerular haemodynamics, altered growth factor expression/mesangial matrix production

SUMMARY:
• The spectrum of kidney disease in patients with HIV is broad.
• 7000 young people contract HIV-1 every day worldwide (UNAIDS); 5-10% of pts develop nephropathy/ ESRF, HIVAN is assuming increasing importance.
• Typical clinical features of proteinuria, minimal oedema, normal/enlarged echo-bright kidneys in a sero-positive/at risk patient should prompt consideration of dialysis and renal biopsy.
• Early, aggressive use of HAART to obtain undetectable viral load may produce recovery of renal excretory function.
• Despite the advent of HAART, the outlook for patients remains poor.
• Formal randomised controlled trials are needed to evaluate new therapeutic strategies, in particular the role of & timing of introduction of ACEIs, and the efficacy & patient selection criteria for the use of immunosuppressive agents such as steroids and cyclospotin A.






















![Crescentic IgA nephropathy and acute renal failur ien an HIV … · 2013-03-12 · heroin-associated nephropathy and idiopathic focal segmental glomerulosclerosis [21]. TRI are by](https://static.cupdf.com/doc/110x72/5f8efdc3bf398034506ee9f4/crescentic-iga-nephropathy-and-acute-renal-failur-ien-an-hiv-2013-03-12-heroin-associated.jpg)







