Gentle Ventilation in Infants with
Pulmonary Hypertension
Jen Wung, MD
Professor of Pediatrics
Columbia University College of Physicians and Surgeons
Morgan-Stanley Children’s Hospital Of New York
New York, NY

Disclosures
Off-Label Usage: None
Interests: None

7th Bubble CPAP and Non-Invasive
Respiratory Management of the Neonate
Conference & Workshop
The George Washington University School of
Medicine and Health Sciences
Washington, DC.
December 9 & 10, 2017

Gentle Ventilation in Infants
with Pulmonary Hypertension
Jen-Tien Wung, M.D., FCCM
Neonatal Intensivist
Professor of Pediatrics
Columbia University Medical Center
New York (CHONY)

I have no conflict of interest to disclose.



Persistence of fetal circulation

PPHN - Causes
•Perinatal asphyxia, MAS
•Congenital heart diseases
•Pulmonary hypoplasia, CDH, Oligohydramion
•RDS
•GBS or other sepsis
•Premature ductal closure secondary to maternal drug therapy (NSAIDs)
•Maternal use of selective serotonin-reuptake inhibitor (SSRI, fluoxetine) in late pregnancy
•Alveolar capillary dysplasia (Misaligment of PVs)
•Idiopathic
•Iatrogenic

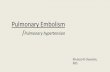
Normal Lung(left) vs PPHN Lung (right)
There is smooth muscle hypertrophy of the pulmonary
arteriole (PA) and narrowing of the arteriolar lumen in PPHN

Misaligment of pulmonary Vessels

Diagnosis of PPHN
•Case history
•Oxygen requirment out of proportion to the severity of lung
disease (chest X-xay)
•Pre- / Post- Oxygen Saturation discrepancy
•EKG (RV hypertrophy)
•Echocardiography
•Cardiac Catheterization - Gold standard
•Biochemical Marker: B-type natriuretic peptide (BNP),and
N-terminal proBNP(NT-proBNP)

Echocardiographic Estimation of PA presssure
➢TR jet flow
Modified Bernouli equation: Systolic PAP = 4 × (TR peak jet
velocity)2
+ RA pressure
➢Septal flattenning, Interventricular septum at end-systole
RV pressure/Systemic pressure: round <50%,
Flat = 50-100%, Bowing to LV ≥100%
➢RA enlargement, RV hypertrophy / dilation, thick RV wall,
dilated PA, ↑ velocity PV regurgitation,
↓ acceleration time of RV ejection to PA

PPHNManagement in 1980’s
“Full Artillery” Approach
1. FiO2 100%
2. IMV 50 – 100/min.
PIP 25 – 45 cm H2O to achieve PaCO2 < 25 mmHg
3. Muscle relaxant
4. Tolazoline
5. To achieve mean BP 45 – 50 mmHg: Dopamine 2-20 g/kg/min
and/or Dobutamine 5-30 g/kg/min
6. NaHCO3 1 meg/kg/hr to keep pH > 7.55


Hyperventilation
• Overventilation impedes venous return, decreases pulmonary blood flow, oxygenation, cardiac output and blood pressure
• Increases pulmonary vascular resistance. The capillaries are stretched and their caliber are reduced
• Increases lung injury (barotrauma, volutrauma, and biotrauma).
• Shifts O2-hemoglobin dissociation curve to the left due to alkalosis
• Decreases cerebral blood flow.
• Causes hearing loss.

Management of PPHNColumbia Approach
• Treating the underlying disease
• Continuous monitoring of pre- & post-ductal O2 saturation
• Mechanical Ventilation: 1. Conventional ventilation 2. PTV (SIMV +/- PS, A/C) 3. HFPPV 4. HFV (HFO)
• No hyperventilation, induction of alkalosis or neuromuscular blockade
• Pulmonary vasodilator-- INO (for pre-ductal oxygen saturation < 90%). If no response, milrinone, inhaled iloprost or I.V. sidenafil may be added.
• ECMO as last resort

MAP: MAP at referral hospital, MAP1: baseline MAP
following admission and before INO therapy, MAP2:
MAP within 24 hours of INO therapy
Journal of Perinatology 2002; 22: 435
10
15
20
MAP MAPI MAP2
MEAN AIRWAY PRESSURE
CM
H2O
*
*
*p<0.01

0
20
40
60
O I - A O I - B
oxyg
en
ati
on
in
de
x
*
Oxygenation index before (OI-A),
and after starting INO therapy (OI-B)Journal of Perinatology 2002; 22: 435
*p<0.001

CHONY Kinsella NINOS Davidson Clark
N 112 107 114 114 126
Gestation (wks) 40 (med) >34 >34 >37 >34
Baseline O.I. 50.7 2.6 49.3 3.4 43.0 17.6 24 9 37+24
PaO2 (mm Hg) 32.7 1.3 40.3 1.7 46.8 15.5 59 16 72+64
PH 7.26 0.2 7.41 0.02 NA 7.50 0.11 7.45+0.1
PaCO2 (mm Hg) 51.9 2.2 35.5 1.3 NA 30 9 35+13
INO (hours) 45 (med) 75.5 1.1 40 (med) 58 <96
Ventilator days 6.69 0.3 9 1 11.6 7 9.2 7.4 11+7
Nonresponders (ECMO+deaths)
25% 30-60% 46% 29.8% 40%
ECMO 17.9% 39% 38%
Mortality 8% 15% 14% 8% 8%

➢ IMV (CMV) or
➢HFPPV (rate 100, P 20/1, Ti 0.3 seconds
➢PTV (SIMV +/- PS, A/C, NAVA )
➢Inhaled nitric oxide
➢ HFV (HFO)
➢ ECMO

Mechanical Ventilation
Conventional
• Pressure-Limit
❖For small child or
❖large air leak with small endotracheal tube
❖Watch chest excursion
• Volume-limit
❖ Tidal volume 4-7 ml/kg
❖ Compressed volume 1 ml/H2O/L
(>> tidal volume 6 ml/kg)

Infant Ventilators
Conventional
• Flo-Disc MVP-10
• Healthdyne(PremieCare, Infant Star-200)
• Infant Star-500, Star Sync, Infant Star-950
• V.I.P.Bird Gold, V.I.P. Bird Sterling
• Bear Cub 750PSV
• Servo 300
• Draeger Babylog 8000, Servo i
• Servo n, Servo u, Babylog VN500, Avea, Puritan Bennett 840

MVP-10 Babylog 8000
Servo i

Servo n

Infant VentilatorBasic Simplified Schematic
1. O2 blender. 2. flowmeter. 3. heated humidifier.
4. manometer. 5. exhalation valve. 6. PEEP/CPAP control.
7. PIP control. 8. solenoid valve/ timer.

Infant VentilatorParameters
• FiO2
• Flow rate
• IMV rate
• Inspiration Time (Ti)
• Peak Inspiratory
Pressure (PIP)
• Positive end expiratory
Pressure (PEEP)

Mechanical Ventilation Complications associated with endotracheal intubaton
1.Hypoxia, bradycardia
2.Esophageal perforation
3.Increased airway resistance
4.Obstruction of endotracheal tube (ETT)
5.Malposition or dislodged ETT
6.Nasal septum damage (nasotracheal tube)
7.Aquired palatal groove (orotracheal tube)
8.Vocal cord injury. Unilateral → dysphonia, Bilateral → aphonia
9.Subglottic edema
10.Subglottic stenosis
11.Tracheomalacia, Tracheal stenosis
12.Release of plasticizer (DEHP)

Mechanical VentilationComplications associated with Positive Pressure
Ventilation :
A. Cardiovascular Effects
1. The abolition of the "thoracic pump" mechanism, decrease of venous return and cardiac output
2. "Tamponade" of the heart
3. Interference with pulmonary blood flow
B. Acute lung injuries ( barotrauma, volotrauma, biotrauma, atelectasis)
C. Airleaks
D. Uneven Ventilations, V/Q mismatch
E. Acid-base Imbalance
F. Neurologic; PV-IVH, PVL, Sensorineural hearing loss
G. Pulmonary Hypertension
H. Chronic Lung Disease (BPD)
I. Cor Pulmonary
J. VAP (ventilator associated pneumonia)

Effect of lung volume on pulmonary vascular resistance
when transmural pressure of the capillaries is held
constant. At low lung volumes, resistance is high
because extra alveolar vessels become narrow.
At high volumes, the capillaries become stretched as
the caliber is reduced.

Froese, et al., Anesthesiology, 1974
Paralyzing the diaphragm
is asking for trouble!

Gattinoni, et al., Critical Care Medicine, 1991
It is not good to spend all day
laying on your back!

The Best Mode of Ventilation is
Spontaneous Breathing

Spontaneous breathing improves lung
aeration in oleic acid-induced lung injury
Anesthesiology 2003;99:376-384
Wrigge H, Zinserling J, Neumann P, et al

Spontaneous breathing affects the spatial ventilation and
perfusion distribution during mechanical ventilatory
support
Crit Care Med 2005; 33:1090-1095
Newmann P. et al
Spontaneous breathing during APRV
(airway pressure release ventilation) is
associated with better ventilation and more
pulmonary blood flow to dependent lung
regions located close to the diaphragm

IMV Ti PIP PEEP FiO2 pH PaCO
2
PaO2
Before
transfer
80 0.4 35 5 1.0 7.41 44 33
After
transfer
40 0.6 30 5 1.0 7.30 55 31
After
reversal*
25 0.6 30 5 1.0 7.34 53 68
*TcPO2 rises (arrow) with spontaneous breathing after
pavulon reversal



➢A large body of evidence indicates that physiologic rhythms
are characterized by spontaneous variability. Heart rate,
respiratory rate, and blood pressure amplitude are all variable
and clearly affect each other.
➢In fact, therapeutic interventions with life-support systems
diminish or eliminate spontaneous physiologic rhythms.
Elimination of these inherent spontaneous rhythms may be
detrimental and contribute to the morbidity and mortality
associated with such life-support systems.
➢Specifically, mechanical ventilation may be improved if
normal physiologic variation is reproduced.
➢Using a computer-controller, the onset, duration, rate and
volume of the ventilator inspiratory cycle could be varied and
influence alveolar recruitment and thereby produce better
oxygenation
.
.

A large body of evidence
indicates that physiologic
rhythms are characterized by
spontaneous variability. Heart
rate, respiratory rate, and blood
pressure amplitude are all
variable and clearly affect each
other.

➢In fact, therapeutic interventions
with life-support systems diminish or
eliminate spontaneous physiologic
rhythms.
➢Elimination of these inherent
spontaneous rhythms may be
detrimental and contribute to the
morbidity and mortality associated
with such life-support systems.

➢Specifically, mechanical ventilation
may be improved if normal
physiologic variation is reproduced.
➢Using a computer-controller, the
onset, duration, rate and volume of
the ventilator inspiratory cycle could
be varied and influence alveolar
recruitment and thereby produce
better oxygenation

Biologically Variable or Naturally Noise
Mechanical Ventilation Recruits
Atelectatic Lung
W.Alan, C. Mutch,et. al
Am J Respir Crit Care Med 2000; 162: 319-23
Stochastic resonance -The addition of noise
to input signal (variable PIP) to amplify
output (PaO2) in a nonlinear system

PaO2 PaCO2 Shunt% Crs MAP Vt
ml/kg
Vbv 502 35 9.7 1.15 15.7 14.7
Vc 381 48 14.6 0.79 18.8 13.2
Vs 309 50 22.9 0.77 18.9
Vbv: biologically variable MV,
Vc: monotonously control MV,
Vs: Vc plus sigh

Biologically Variable Ventilation
➢Improves lung mechanics, gas exchange,
inflammatory mediators, and histological
evidence of lung injury in ARDS.
➢Recruits atelectatic and poorly areated
lung regions.
Graham M.R. et al, Crit Care Med 2011;39:1721-1730

Stochastic Resonance
is most simply described as
the addition of noise to an input signal
to enhance output in a nonlinear system

Stachastic Resonance

Overdistention may be regionalEven a “normal” VT can create regional overdistention

Mechanical Ventilation Using Conventional Infant
Ventilators
Four Techniques
1. Conventional technique (IMV < 41/min.)
2. High Frequency Positive Pressure Ventilation (HFPPV)
3. Prolonged inspiratory time with inspiratory pressure plateau (reverse I/E ratio)
4. Synchronization (IMV rate between 40 and 100/min to synchronize with patient's spontaneous respiration)

Parameter• FiO2 (1)
• Flow rate (2)
• IMV rate (8)
• Ti (8)
• PIP (7)
• PEEP (6)

Conventional VentilationFiO2
To keep PaO2 50 – 70 mmHg
Acceptable O2 Saturation around 90%
(Alarm limit 85 – 95%)

Conventional VentilationFlow
• Usually 5 – 8 lpm
• Enough to reach PIP within Ti
• Minimum flowrate to prevent rebreathing CO2 :
minute ventilation (200ml/kg) × 2.5 plus air leak

Conventional Ventilation(<40/min)
IMV Rate
• Usually start at 20 – 40/min
• To keep PaCO2 40 – 70 mmHg
• To avoid excessive labored spontaneous
breathings

Conventional Ventilation(<40/min)
Ti
• Usually 0.5 seconds
(about 2 time constant,
T.C. = C x R)

Tc=C× R
Tc = c× R
Tc =C x R

Conventional Ventilation(<40/min)
PIP
• Usually start at 20 cmH2O (15 cmH2O for
preemie)
• To have adequate chest and/or abdominal
excursion

Conventional Ventilation(<40/min)
PEEP
• Usually 5 cmH2O
• To increase for deep inspiratory retraction
due to low FRC
• To decrease for lung hyperinflation

Conventional Technique
Settings1. Flow rate 5 - 8 LPM
2. FiO2 to keep PaO2 50-70 mmHg
3. IMV rate
• Usually started at 20-40/min.
• Avoid excessive labored breathing
• Maintain PaCO2 40-70 mmHg
4. Inspiration time (Ti) 0.5 seconds
5. Peak inspiratory pressure (PIP)
• Adequate chest excursions
• Usually started at 20 cmH2O for term infant and 15 cm H2O for preemie
6. PEEP 5 cmH2O

Conventional Technique
Improvement
• Decrease IMV rate by 2-5/min for PaCO2 <50 mmHg
• Decrease PIP by 2-5cmH2O for excessive chest excursion
• Decrease FiO2 by 1/10 for PaO2>60mmHg
• Usually no change for flow rate, Ti or PEEP

Conventional Technique
Deterioration
• R/O ET tube obstruction, pneumothorax, underventilation, overventilation, etc.
• For PaCO2>70mmHg or excessive labored breathings, increase IMV rate (up to 40/min)
• For hypoxemia,
➢ Increase PIP if chest excursion is inadequate
➢ Increase PEEP for severe inspiratory retractions
➢ Increase FiO2





Indications for a Trial of HFPPVOn Conventional Technique:
1. PaO2 < 50 mm Hg with an FiO2 100%
2. PaO2 is very labile
3. PIP > 30 cm H2O to achieve visible chest excursions
4. PaCO2 > 70 mm Hg or excessive labored
spontaneous breathing with IMV rate up to 40/min.
5. Pulmonary interstital emphysema (P.I.E.)

High Frequency Positive Pressure Ventilation
(HFPPV)
Setting
1. IMV 100/min.
2. Ti 0.3 sec. (Te 0.3 sec)
3. Flow rate (>6 LPM)
4. PIP is usually the same as conventional
settings
5. PEEP 1 (to prevent intrinsic high PEEP)

Mechanical Ventilation Using Conventional Infant
Ventilators
Four Techniques
3. Prolonged inspiratory time with inspiratory pressure plateau (called reverse I/E ratio in the past)
• Inspiration time (Ti): 0.5 -1.0 seconds
• For infants with severe parenchymal lung disease, e.g. severe RDS, congenital pneumonia, etc.
• Replaced by HFO

Mechanical Ventilation Using Conventional Infant
Ventilators
Four Techniques
4. Synchronization
• IMV rate between 40 and 100/min to synchronize with patient's spontaneous respiration
• Ti: 0.5 seconds or I:E ratio = 1, whichever is shorter
• Replaced by patient triggered ventilation (SIMV, A/C, PS or NAVA)

“Agitation”
“Fighting with respirator”
Patient is telling us something is wrong

“Agitation”
“Fighting with respirator”
• Looking for the cause
• Suctioning of the endotracheal tube
• Nasotracheal intubation
• Mild sedation if necessary
• Best sedation is a clear airway and
television set

Ramsay Sedation Scale
1. Agitated, anxious, restless
2. Cooperative, oriented, tranquil
3. Drowsy, respond to commend
4. Sleepy, easy arousal
5. Sleepy, difficult arousal
6. Sleepy, not arousal
Ramsay et al Br Med J 1974;2:656-9

Sedation Analgesia
----------------------------------------- --------------
Amnesia Hypnosis Anxiolysis
----------------------------------------------------------
Selective α2 adrenoreceptor agonist
Dexmedetomidine (precedex)
Loading :1 ug/kg over 10-20 minutes
Maintenance: 0.2 – 0.7 ug/kg/hr (max. 24 hours)

Tolerance,withdrawal, and physical
dependence of children in PICU after
long-term sedation and analgesia
Joseph P. Tobias
Crit Care Med 2000; 28: 2122-32

Neuromuscular blocking agents
Undesirable side effects1. Loss of spontaneous respiration and increase of respirator
settings which cause barotrauma and volotrauma
2. V/Q mismatch
3. suppression of cough reflex resulting in secretion retention and atelectasis
4. Immobility leading to peripheral edema, peripheral nerve injuring, muscle atrophy, contractures, skin breakdown/stasis ulcer, deep vein thrombosis and pulmonary embolism
5.Inability or limitation of doing a thorough neurological examination
6. Autonomic and cardiovascular changes
7. Inappropriate use of sedatives and analgesics
8. Prolonged paralysis or weakness
9. Myopathy, particularly if corticosteroids are concurrently used.

The act of breathing depends on rhythmic discharge from the respiratory center of the brain. This discharge travels along the phrenic nerve, excites the diaphragm muscle cells, leading to muscle contraction and decent of the diaphragm dome. As a result, the pressure in the airway drops, causing an inflow of air into the lungs

Central nervous system
↓
Phrenic nerve
↓
Diaphragm excitation
↓
Diaphragm contraction
↓
Chest wall and lung expansion
↓
Airway pressure drop, flow reversal --→ PTV

Patient Triggered Ventilation
Beware of
• :Sensor: It may not working properly and need calibration.Watch sensitivity level. Avoid autocycling due to water condensation or heart beat in VLBW.
• Tidal volume: Part from spontaneous breathing and part from respirator. Pay attention to airleakage and hypoplastic lung.
• A/C mode: May need to adjust Ti. May not synchronized with high respiration rate.
• Narcotic and sedative suppress respiratory effort

IMV SIMV A/C PS
Flowrate Flowrate Flowrate Flowrate
FiO2 FiO2 FiO2 FiO2
IMV rate SIMV rate Patient,
Backup rate
Patient,
Backup rate
Ti Ti Ti Insp. cycle off
PIP PIP PIP Support P.
PEEP PEEP PEEP PEEP
Sensitivity Sensitivity Sensitivity
Sync. Synchronization Sync.
Readjust Ti and PEEP Readjust PEEP







SIMV + PS



88
Patient Ventilator Interaction
Nature 1999


Central nervous system
↓
Phrenic nerve
↓
Diaphragm excitation --→ NAVA
↓
Diaphragm contraction
↓
Chest wall and lung expansion
↓
Airway pressure drop, flow reversal --→ PTV
NAVA (Neurally Adjusted Ventilatory Assist)

91
Edi Catheter positioning procedure
Position and Edi signal

92
Asynchrony
Even with current technology the most sensitive
triggers will exhibit lag time = Asynchrony.


Formula for estimating peak pressures during
NAVA:
Ppeak est.=NAVA level X (Edipeak – Edimin) + PEEP
* NAVA level is the factor by which the Edi signal
is multiplied to adjust the amount of assist
delivered to the patient


Implement NAVA Mode

High Frequency Ventilation
⚫ Defined by FDA as a ventilator that delivers
more than 150 breaths/min.
⚫ Delivers a small tidal volume, usually less than
or equal to anatomical dead space volume.
⚫ While HFV’s are frequently described by their
delivery method, they are usually classified by
their exhalation mechanism (active or
passive).

HIGH FREQUENCY VENTILATION
Types of Ventilators
• HFPPV (High Frequency Positive Pressure Ventilation, infant respirator, rate 60 - 150)
• HFFI (High Frequency Flow Interrupter, Infant Star, rate ~ 22 Hz)
• HFJV (High Frequency Jet Ventilator, Bunnell Life Pulse, 7 Hz)
• HFO (High Frequency Oscillatory Ventilator, SensorMedics 3100A, rate ~ 15 Hz )
• HFCWO (High Frequency Chest Wall Oscillator)


AIRWAY PRESSURE WAVEFORMS
HFJV
HFOV

HFJV
HFOV
CV
MAP
seconds0.80.60.40.2
10
15
20
5
Tra
ch
ea
l P
res
su
re
cm
H
2O
Time
0
0
PRESSURE WAVEFORM COMPARISON

LifePulse HFJV-Model 204


➢Rate: 4-11Hz, usually 7Hz
➢Inspiration: active
➢Expiration: passive
➢A jet is produced by
opening and closing of a
control valve
➢Tidal volume > anatomical
deadspace
➢Microprocessor –controlled
➢Feedback control (peak pressure and gas temperature)
➢Patient box contains pressure transducer and pinch valve
➢Lifeport ET tube adaptor

LifePort ET tube adapter
ET Tube Connector
Jet Port Cap
Jet Injection Port
15-mm Connector
Pressure Monitoring Line

LifePort Adapter
Jet
Port
Inspired gas is
injected down
the ETT in high
velocity spurts.
PIP is measured
here and filteredto estimate PIP
at the tip of ETT.
Pressure
Monitoring
Port


HFJV in Tandem with CV
Jet CV
LifePort adapter
Ventilation Oxygenation
PEE
P
Valve
Jet Flow 1 Lpm
CV Flow 5 Lpm
PIP Rate PIP Rate

HFJV
Bunnell Life Pulse- (3)
Operator-selected parameter:
➢Conventional ventilator required for FiO2, IMV
rate (0-10,) PIP and PEEP
➢Jet: PIP
rate 420/min (4 – 11 Hz)
Ti 0.02 seconds
➢Oxygenation: PIP, PEEP, FiO2
➢Ventilation: Jet PIP

HFJV vs. HFOVWhen is the Jet the HFV of choice?
• Air Leak Syndromes
• Excessive Secretions
• Hemodynamic Compromise
• When HFOV Fails(e.g., non-homogenous lung diseases)
(e.g., Ptx, PIE)
(e.g., pneumonias)

Operator-selected parameter:
▪FREQUENCY(10 – 15 HZ)
▪INSPIRATION TIME (33%)
▪MEAN AIRWAY
PRESSURE (MAP)
▪AMPLITUDE
▪BIAS FLOW RATE
▪PISTON CENTERING
▪FIO2 (ATTACHED OXYGEN
BLENDER)


How to begin!
for infant
• Start with mean airway pressure 0-4 cmH20 above
CMV mean airway pressure(disease dependent)
✓ Monitor SaO2 to maintain SaO2 to 88 -93%
✓ If SaO2 does not increase within the first 5 – 10
minutes, increase mean airway pressure by 1-2
cmH20.
• Start with the power setting at 2.5 and monitor
chest wiggle to umbilicus.
• Inspiration time 33%

Respiratory Distress of NeonatesFour Categories
➢Diffuse homogeneous lung diseases e.g. RDS,
pneumonia, ARDS
➢Nonhomogeneous lung diseases e.g. MAS,
focal pneumonia, BPD
➢Lung hypoplastic syndromes e.g.
hypoplastic lung, CHD, Potter’s Syndrome
➢Airleak syndromes e.g. P.I.E.,
pneumothorax, bronchopleural fistula

SensorMedics 3100Astrategies for diffuse homogeneous lung disease
➢ Initial settings: Bias flow: > 6 LPM MAP: 1 – 2 cm H2O above conventional MAP F: 10 – 15 Hz Ti: 33% Amplitude: chest vibration
➢ Adjustment: MAP: 1 cm H2O increment till no PaO2 improvement
Chest X-ray: Rt. diaphragm at T 9 Amplitude for PaCO2
Avoid lung overexpansion & cardiovascular decompensation
➢ Weaning: decrease FIO2 till 60% then decrease MAP, decrease MAP if lung hyperinflation or cardiovascular decompensation

SensorMedics 3100AStrategy for Airleak Syndrome
➢MAP = conventional MAP reduce MAP if
possible
➢Increase FIO2 for low PaO2
➢F: 10 Hz
➢Amplitude to keep PaCO2 at 50’S
➢Continue for 48 hrs after airleaks resolved and then resume
RDS strategy

SensorMedics 3100AStrategies for:
Nonhomogeneous Lung Diseases and Lung Hypoplastic Syndrome
➢To improve PaO2 at lowest possible MAP
➢MAP = conventional MAP to decrease MAP if possible
➢F: 10 – 15 Hz
➢Ti: 33%
➢Amplitude: chest vibration

OXYGENATION:
➢Conventional ventilator: FiO2, PIP, PEEP, Ti
➢HFO: MAP, FiO2
VENTILATION:
➢Conventional ventilator: MV = Vt F
where F is IMV rate, Vt is PIP – PEEP
➢HFO : MV = Fa Vtb
where a is estimated as 0.75 to 1.24 and b is between
1.5 and 2.2 (About MV = F x Vt2)
Vt is related to amplitude




Patient on HFOV. O2 sat. increase with
spontaneous breathings

Shunt Oscillation

HFO
• Very sensitive to increase of airway resistance
• Less sensitive to Nonhomogeneous compliance

Left lung collapsed
(lower compliance)Left lung opened
on HFO


HFV versus CMV -1
Reference Device N BW(kg) CLD Rate
Carlo ’87 HFJV 41 1.48 No difference
HIFI ’89 HFOV 673 1.10 No difference
Carlo ’90 HFJV 42 1.42 No difference
Clark ’92 HFOV 83 1.10 30% vs 65% 30d
10% vs 38% 36w
Ogawa’92 HFOV 92 1.20 No difference
Pardou’93 HFFI 24 1.30 No difference

HFV versus CMV -2
Reference Device N BW(kg) CLD Rate
Gerstman’96 HFOV 125 1.50 24% vs 44% 30d
Wiswell
’96
HFJV 73 0.90 No difference
Keszler
’97
HFJV 130 1.00 67% vs 71% 30d
20% vs 40% 36w
Rettwitz-Volk
’98
HFOV 96 1.10 No difference
Thome’99 HFFI 284 0.88 No difference

HIGH FREQUENCY VENTILATION Concern of the
trials
✓The results are contradictory
✓Masking of investigators is not possible
✓ Most of these trials have been performed by investigators who have extensive experience in HFV
✓A standardized approach for HFV versus a non-standardized approach for CMV
✓Only studies in which there is a relatively high rate of BPD in CMV group have demonstrated a lower incidence of BPD in HFV group

HIGH FREQUENCY VENTILATION Indication -
Prophylactic
✓In animal experiments, HFV cause less lung trauma
than conventional ventilation
✓Whether this is also true in human preterm infants is
still uncertain
✓The findings of clinical trials are contradictory
✓There remain concerns that HFV may be associated
with a high rate of brain injury
HFV as a primary mode of ventilation is not recommended

HIGH FREQUENCY VENTILATION Indication - Rescue
✓Most of the evidence of benefit is short term
and in term babies
✓No clear evidence to support a rescue role in
preterm babies
✓Indications should be considered on a case by
case basis

P P H NVasodilator Therapy
• tolazoline (priscoline)
• epinephrine (0.1 ug/kg/min)
• prostaglandin E1 (0.1 ug/kg/min)
• magnesium sulfate
• inhaled nitric oxide (after 5/1994)
• milrinone I.V.
• sidenafil P.O., or I.V
• inhaled iloprost
.

P P H Ntolazoline (priscoline)
• Infuse into upper extremity or scalp
vein
• Test dose: 1 mg/kg
• Maintenance: 1mg/kg/hr





Vasodilator TherapyInhaled Nitric Oxide
Phosphodiesterase type 5 inhibitor (PDE5):
sildenafil
Prostacycline:
inhaled iloprost
inhaled treprostinil ( lasting >3 hrs )
flolan
Phosphodiesterase type 3 inhibitor (PDE3):
milrinone
Endothelin receptor antagonist:
bosentan
Ambrisentan

Nitric Oxide Pathway
GTP cGMP Relaxation
guanylyl cyclase
NO or NO donor
X Sildenafil(Type 5 phosphodiesterase inhibitor)
Ca++

Schematic of NO uptake and
mechanism for pulmonary vasodilatation

PPHN PPHN + INO

PPHN + Nipride PPHN + INO

Inhaled Nitric Oxide
•Selective pulmonary vasodilator
•The gold standard therapy for PPHN

INOmaxTM
Dosage
• The recommended initial dose is
20 ppm.
• Dose reduced as tolerated to 5 ppm
after a sustained improvement in
oxygenation (24 to 48 hours).
• Duration is usually 2 to 6 days

Methemoglobin Concentration-Time ProfilesNeonates Inhaling 0, 5, 20 or 80 ppm INOmaxTM

Methemoglobin Concentration - Time Profile
Davidson et al. Pediatrics 1998;101:325-334

Inspired NO2 level - Time Profile
Davidson et al. Pediatrics 1998;101:325-334

INOmaxTM
Weaning
20ppm →15ppm →10 ppm →
5 ppm →( 4 --->3 -->2 -->1 ) → 0

INOmaxTM
Discontinuation
• INOmaxTM discontinued when the infant is
stable on 5 ppm, and FiO2 <60%
• About half of patients require an increase of
FiO2 (20 - 40%) for a few hours after weaning off
INOmaxTM

Discontinuation
of INO (1)
Note the stability of mean
blood pressure, heart
rate, and SPO2 with the
same FiO2 as INO is
withdrawn.
Aly H, Sahni R, Wung JT
Arch Dis Child 1997;76:

Discontinuation
of INO (2)
Acute deterioration of mean
blood pressure, heart rate,
and SPO2 with the same
FiO2 followed the initial
attempt at weaning. FiO2
was increased and the
weaning was successful.
Note how quickly FiO2 was
reduced following
successful weaning.
Aly H, Sahni R, Wung JT
Arch Dis Child 1997;76:

Changes in PaO2 30 minutes after
discontinuing INO treatment gases

PPHN Case #8 (1)• 4250g B/M 40 wk. gestation
• 35y.o. G5 P4 gestational D.M. on Insulin Variable deceleration, vaginal delivery, cord around neck x 2
• In nursery - tachypnea & acrocyanosis
• 2hrs - oxyhood FiO2 90% VBG 7.31/54/55
• Endotracheal intubation
• 28.5 hrs - arrived CHONY
• 29.1hrs - INO 25 PPM started
• 56hrs - INO discontinued
• 3d - extubated, 7d - off CPAP

PPHN Case #8 (2)Hrs IMV P Ti FiO2 pH PCO2 PO2
8 40 25/5 0.35 100 7.44 31 150
9 7.50 27 127
12 7.48 21 150
17 7.32 39 57
19 60 35/5 0.48 100 7.45 25 81
19.1 7.44 28 58
21 86 22/3 0.25 7.49 26 81
24 80 24/4 0.35 7.37 37 52
28.5 Arrived at CHONY
29 100 25/0 0.3 100 7.21 56 16
29.1 INO 25 ppm started
30 100 22/0 0.3 65 7.45 33 99

PPHN 4250g IMV 100 P25/0 Ti 0.3
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80
Time
FiO2
Pre-SO2
INO 25 INO 20

PPHN 4250g IMV 100 P25/0 Ti 0.3
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80
Time
FiO2
Pre-SO2
Post-SO2
INO 25 INO 20

PPHN 4250g IMV 100 P25/0 Ti 0.3
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80
Time
FiO2
Pre-SO2
Post-SO2
SBP
INO 25 INO 20

PPHN 4250g IMV 100 P25/0 Ti 0.3
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80
Time
FiO2
Pre-SO2
Post-SO2
SBP
DBP
INO 25 INO 20

Fig. 8. BP and O2 saturation change after INO for a PPHN infant 4250g IMV 100 P25/0 Ti 0.3.
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80
Time
FiO2
Pre-SO2
Post-SO2
SBP
DBP
HR
INO 25 INO 20
Case #8 –(3), on IMV 100, P 25/0, Ti 0.3
O2 saturation and BP response to INO,

•Understand the nature of the disease
•Watch for trending
•Be patience

• 735 gm, 26 wks,PROM x7 days, oligohydramions
• Stat c-section for preterm labor, variable deceleration,
breech presentation, cord prolapse,
• Apgar score 7/1’, 8/5’
• CPAP FiO240%, Deteriorated during transport from
TN to NICU, FiO260%,→ NTT → FiO2100%,IMV
rate 40, P 20/5, O2 sat. 50’s→Curosurf → O2 sat.
transiently ↑to 90’s for 5 min. and then ↓to <20’s
• ECHO revealed PPHN
• INO 20ppm started with slowly ↑ O2 sat.
• INO x 3days, IMV x 4days, CPAP x 85 days,
Discharged at DOL#100

30% of PPHN fail to respond to iNO
It is not the single magic bullet for the
complex pathophysiology of PPHN

Nitic Oxide Pathway
GTP cGMP Relaxation
guanylyl cyclase
NO or NO donor
X Sildenafil(Type 5 phosphodiesterase inhibitor)
Ca++

Sildenafil (PDE 5 Inhibitor) inhibits cGMP-specific
phosphodiesterase type 5 (PDE 5, an enzyme that promotes
degradation of cGMP.)
• Oral sildenafil (dose range 1-2 mg/kg every 6 h) improves
oxygenation and reduces mortality
• Intravenous sildenafil is administered as a load of 0.42 mg/kg
over 3 hours (0.14 mg/kg/h) followed by 1.6 mg/kg/day as a
continuous maintenance infusion (0.07mg/kg/h). Steinhorn et
al, J Pediatr, 2009
• It should be restricted to refractory cases at a center with ECMO
back-up, due the potential risk of systemic hypotension and
pulmonary hemorrhage, presumably due to sudden reversal of
ductal shunt
• Systemic hypotension is a major side effect and can increase
morbidity in PPHN by worsening right-to-left shunt.
• Long-term therapy with sildenafil in children (1-17 years) has
been associated with increased mortality.

Prostacycline Pathway
cAMP Relaxation
PGI2
X milrinone(Type 3 phosphodiesterase inhibitor, PDE)
Adenylyl cyclase

Inhaled Nitric Oxide
Phosphodiesterase type 5 inhibitor (PDE5):
sildenafil
Prostacycline:
ventavis ( iloprost) inhalation
treprostinil (remodulin) I.V. or S.C.
(tyvaso) oral inhalation (>18 yr. old)
epoprostenol (flolan) I.V.2ng/kg/min, ↑2 ng q8h
Phosphodiesterase type 3 inhibitor (PDE3):
milrinone
Endothelin receptor antagonist:
bosentan, Ambrisentan

Inhaled prostacyclin for term infants
with PPHN refractory to iNO
Four infants with severe PPHN unresponsive to iNO show improvement with inhaled PGI2. The intravenous form of PGI2 was aerosolized in an alkaline solution through the respiratory circuit. Age at initiation of PGI2 ranged from 1 day to 16 days old and was preceded with iNO for at least 3 hours (range 3hr to 14 days). Within 1 hour of initiation of PGI2, mean PaO2 increased from 57 to 100 (p = 0.06) and within 2 hours, mean OI decreased from 29 to 19 (p<0.05). 3 MAS survived, 1 ACD with transient response and died 6 days later.
The journal of Pediatrics 2002;141:830-2, Kelly LK et. al.

Prostaglandin E1 (PGE1)
Dose: PGE1 solution for aerosolization is prepared
from Alprostadil® (Prostin VR 500, Pfizer, New
York NY) and administered as a continuous
nebulization through a MiniHeart low flow jet
nebulizer (WestMed Inc, Tuczon, AZ) at 150-300
ng/kg/min diluted in saline to provide 4 ml/hr67.
Intravenous PGE1 has also been used in patients
with CDH in combination with iNO to promote
pulmonary vasodilation and to maintain ductal
patency and reduce right ventricular afterload69

Inhaled Prostacyclin (PGI2)
Dose: Inhaled PGI2 has been used in PPHN resistant to
iNO at a dose of 50 ng/kg/min68. The intravenous
formulation Flolan° (Glaxo-Wellcome, Middlesex,
UK) is dissolved in 20 ml of manufacturer’s diluent (a
glycine buffer, pH -10). Fresh solution is added to the
nebulization chamber every 4 hours.
Iloprost is an analog of prostacyclin and has
anecdotally shown to be effective in neonates and
children with pulmonary hypertension.

iloprost (Ventavis) inhaled
•2.5 - 5mcg (10 mcg/ml) diluted with Glycine
solution or normal saline to make total volume 2 ml
to be inhaled over 15 min.
•Nebulization using Aeroneb (electronic
micropump) q3hr. 6 - 9 times/day
•(Half-life 20 – 30 min.)
•For severe acute PPHN, q 45 - 60 min
•Continuously nebulization: 10 mcg diluted in 9 ml
N/S to run 2-3 ml/hr, after 2.5 - 5 mcg in 2 ml N/S to
show improvement.
•Monitor vital signs and O2 saturations






Ilopost inhaled continuously


SIMV HFO

flolan I.V. infusion
→inhaled ilopost continuously

1
32 44
1.HFO
2.A/C
3. Iloprost 5 ug
(in 2 ml saline)
nebulization
followed
by continous
nebulization 1.67ug
(in 2 ml saline)/hr
4. Et tube suction

Ilopost 5ug
then 1.67ug/hr
Et tube suctionEt tube suction

Ilopost 2.5ug
in 2 ml N/S
bolus
Ilopost 2.5ug in 2 ml N/S bolus
then Ilopost 10ug in 11 ml N/S
to run 2ml/hr

Increased deadspace

Prosacycline Pathway
cAMP Relaxation
PGI2
X milrinone(Type 3 phosphodiesterase inhibitor, PDE)
Adenylyl cyclase

Inhaled Nitric Oxide
Phosphodiesterase type 5 inhibitor (PDE5):
sildenafil
Prostacycline:
ventavis ( iloprost) inhalation
treprostinil (Remodulin) I.V. or S.C.
epoprostenol (flolan) I.V.2ng/kg/min, ↑2 ng q8h
Phosphodiesterase type 3 inhibitor (PDE3):
milrinone (0.3 ug/kg/min → 0.5ug/kg/min)
Endothelin receptor antagonist:
bosentan ,Ambrisentan

Milrinone (PDE 3 Inhibitor)
Milrinone inhibits PDE3 and increases concentration of cAMP
in pulmonary and systemic arterial smooth muscle and in cardiac
muscle.
IV milrinone: loading dose (50 mcg/kg over 30-60 min) followed
by a maintenance dose (0.33 mcg/kg/min and escalated to 0.66
and then to 1 mcg/kg/min based on response)
Milrinone may be the pulmonary vasodilator of choice in the
presence of PPHN with left ventricular dysfunction
Hypotension is a clinical concern and blood pressure needs to be
closely monitored.
one case series described an increased incidence of intracranial
hemorrhage with the use of milrinone in PPHN

Inhaled Nitric Oxide
Phosphodiesterase type 5 inhibitor (PDE5):
sildenafil
Prostacycline:
ventavis ( iloprost) inhalation
treprostinil (Remodulin) I.V. or S.C.
epoprostenol (flolan) I.V.2ng/kg/min, ↑2 ng q8h
Phosphodiesterase type 3 inhibitor (PDE3):
milrinone
Endothelin receptor antagonist:
bosentan (ETA & ETB antagonist, 1.5mg/kg/d
q12h → 3mg/kg/d q12h, P.O. )
ambrisentan (selective ETA antagonist)

Bosentan (Endothelin-1 receptor blocker):Endothelin receptor antagonists are beneficial and well
tolerated in adult patients with pulmonary arterial
hypertension
The results of a multi-center, randomized, double-blind,
placebo-controlled exploratory trial of bosentan in PPHN
was recently reported. Bosentan (2mg/kg/dose BID) did
not show any additive effect on the top of iNO in term
neonates with PPHN.
However, endothelin receptor antagonists may have a
role in the management of chronic pulmonary
hypertension associated with BPD or CDH.

Endothelin receptor antagonists
• bosentan and sitaxsentan
have been reported to be effective in
treating pulmonary hypertension. It
remains to be seen if they are safer,
more effective or even complementary
to sildenafil.

Which is the gold standard in diagnosis of PPHN?
1. Pre- / Post- Oxygen Saturation discrepancy
2. Echocardiography
3. Cardiac Catheterization
4. Biochemical Marker: BNP and NT-proBNP