FY 2011:The MACs, RACs, Rules, and Tools
DisclaimerAudits from federal and states are changing
daily.Consult your RAC Issues site for more
information. This is changing daily.Every practice needs to be responsible for
internal compliance.
2

AgendaThis presentation will focus on a variety of
audits planned (and anticipated) for FY 2011 and beyond.
How We Got HereOIG FY 2011 Work PlanThe RAC The MICOthersMinimizing Your Risk
3

Disclaimer 2 If this presentation does not make you totally
paranoid, you either are doing something very wrong or very right!!!
4

Fraud Waste & Abuse Defined
Fraud: an intentional act of deception, misrepresentation, or concealment in
order to gain something of value. Waste: over-utilization of services (not caused by criminally negligent actions) and the misuse of resources.Abuse: excessive or improper use of services or actions that are inconsistent with acceptable business or medical practice. Refers to incidents that, although not fraudulent, may directly or indirectly cause financial loss. Examples include:
Charging in excess for services or supplies. Providing medically unnecessary services. Billing for items or services that should not be paid for by
Medicare. Billing for services that were never rendered. Billing for services at a higher rate than is actually justified. Misrepresenting services resulting in unnecessary cost to the
Medicare program, improper payments to providers, or overpayments.
5
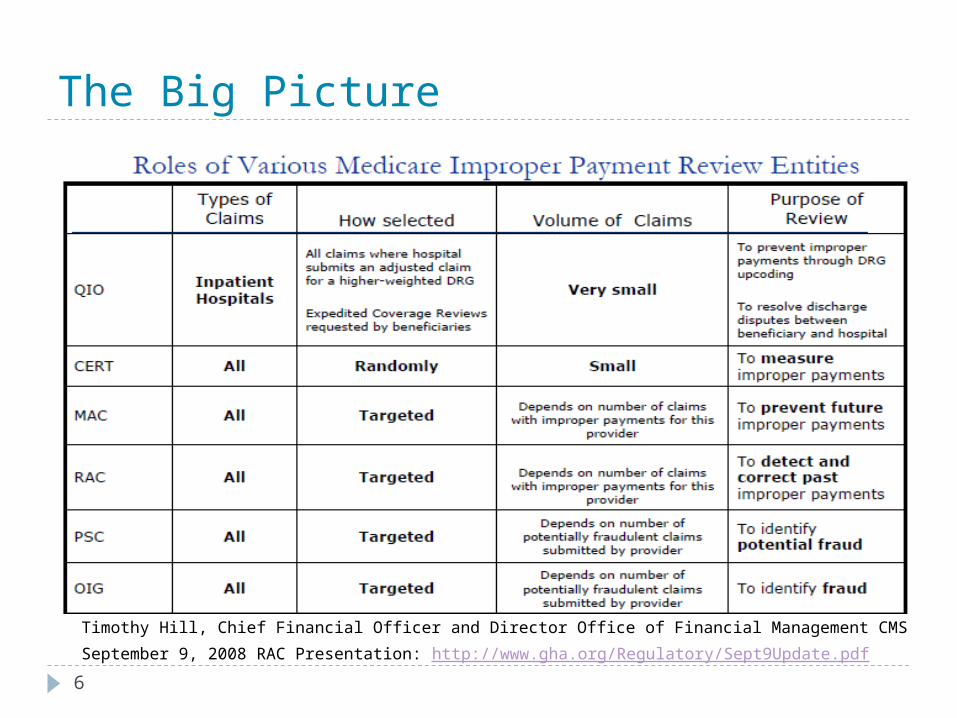
The Big Picture
Timothy Hill, Chief Financial Officer and Director Office of Financial Management CMS
September 9, 2008 RAC Presentation: http://www.gha.org/Regulatory/Sept9Update.pdf6

The OIG FY 2011 Work PlanReleased October 1, the Plan describes the
OIG’s new and ongoing projects. It is often used by providers to develop compliance activities.
The Plan includes new priorities relating to the American Recovery and Reinvestment Act of 2009.
The Obama administration has previously indicated that funding for health care reform will come, in part, from recoveries of alleged Medicare and Medicaid overpayments. So, enforcement is going to be more vigorous!
http://oig.hhs.gov/publications/docs/workplan/2011/Work_Plan_FY_2011.pdf
7
OIG Mission
Protect US Department of Health and Human Services (HHS) program integrity and beneficiary wellbeing by:- detecting and preventing waste, fraud and abuse- identifying to Congress, HHS and the public opportunities to improve program economy, efficiency and effectiveness- holding accountable those who violate Medicare requirements
8
Work ActivitiesOIG mission accomplished by:
- conducting audits, investigations and inspections- providing industry guidance- imposing civil monetary penalties, assessments and sanctions- work with DOJ
9
OIG Components
OIG components:Office of Audit Services (OAS)
- performs independent assessments of HHS programs and operations
Office of Investigations (OI)- conducts investigations of fraud and misconduct
Office of Evaluation & Inspections (OEI)- conducts national evaluations to provide HHS and Congress w/information and recommendations to improve program
Office of Counsel to the Inspector General (OCIG) - provides general legal services to OIG, represents OIG in fraud and abuse cases, negotiates and monitors corporate integrity agreements, renders advisory opinions, publishes fraud alerts
10
OIG WorkplanWorkplan identifies and prioritizes OIG’s
projects for future implementation- identifies risk areas OIG will study, audit and/or investigate
2011: Looks at many of the projects in the Patient Protection and Accountable Care Act (PPACA)
11

Physicians: Place Of Service ErrorsBackground: Medicare pays physicians a
higher amount when a service is performed in a non-facility setting, than when it is performed in a hospital or ASC
Review: whether physicians properly coded the places of service on claims for services provided in ASCs and hospital outpatient departments
(OAS work in progress, FY 2011)
12
Physicians: Evaluation And Management Services (E/M)
Review:Do E/M codes represent the type, setting
and complexity of services provided, and patient status (new or established)
Trends in coding for E/M services (MACs have noted increased frequency of medical records w/identical documentation across services)> “Boilerplate”
Multiple E/M services for same providers and/or patients to identify EHR documentation practices
13
Physicians: Medicare Payments For Imaging Services
Background: Medicare fee schedule covers physician cost component, malpractice costs and practice expense (includes equipment utilization rate)
Review: whether Medicare payments reflect expenses incurred (focus on practice expense component and equipment utilization rate)
(OAS, new start, FY 2011)
14

All Providers: Excluded ProvidersBackground: no payment made be
made for items or services furnished, ordered or prescribed by an excluded individual or entity
Review: were Medicare payments made for services ordered or referred by excluded providers
OEI, new start, FY 2012
15
All: “Error Prone” Providers
Background: CMS’ Comprehensive Error Rate Testing (CERT) program identified providers that consistently submit claims w/errors
Review: select top error-prone providers based on dollar error amounts and match against National Claims History file to determine dollar amounts paid, then conduct a medical review on a sample of claims, project results to population and request refunds
OAS new start FY 2011
16
Medicare Incentive Payments For Electronic Health Records
Background: ARRA authorizes Medicare incentive payments over 5 years to providers that demonstrate meaningful use of certified EHR technology (scheduled to begin 2011-2016, w/reductions in 2015 for providers who fail to become meaningful users)
Review: of Medicare incentive payments from 2011 to identify payments to providers who should not have received payment
17
Information Data PrivacyReview:Have Medicare and Medicaid providers
implemented privacy standards of HIPAA as strengthened by HITECH
Adequacy of OCR’s oversight of HIPAA privacy rule
OEI work in progress FY 2012
18
Medicare Billings With Modifier GYBackground: Modifier GY is to be used to
code services not covered under Medicare, and patients are responsible- but providers are not required to provide patients with advance notice of charges for services excluded from Medicare by statute
Review: whether providers have appropriately used modifier GY on claims for services not covered by Medicare
(OEI work in progress)
19

Medicare Part D Prescription Drug ProgramReview: Duplicate drug claims to hospice patients Duplicate payment when patients change
plans Part A and B claims included with Part D
claims Out of pocket costs Administrative costs included in bid
submissions Audits of pharmacies Internal controls for fraud, waste and abuse P&T Committee Conflicts of Interest
20
RACs
What Are They Up To?
21
22
What is a RAC?RAC Program Mission
The RACs will detect and correct past improper payments so that CMS and the Carriers/FIs/MACs can implement actions that will prevent future improper paymentsProviders can avoid submitting claims that
don’t comply with Medicare rules CMS can lower its error rateTaxpayers and future Medicare beneficiaries
are protected
222

23
RAC Legislation
Tax Relief and Healthcare Act of 2006, Section 302: requires a permanent and nationwide RAC program
by no later than 2010gave CMS the authority to pay RACs on a
contingency fee basis
23

SOURCE: RAC Data Warehouse
Overpayments Collected by Provider Type Overpayments Collected by Error Type
Inpatient Hospital
Outpatient Hosp/IRF/SNF
DMEPhysician/Ambulanc
e/ Lab/Other
14% 1%1.5%
84%
RACs collected $980 million dollars, March 2005 – March 2008
Medically Unnecessary
40%
Incorrectly Coded
35%
Other17%
No/Insufficient Documentation
8%
CMS has not updated the figure of $980 million to reflect successful appeals through 6/30/08
Demonstration Results
24
Source of Majority of Overpayments in the Project
Inpatient Hospitals—84% of overpayments collected
Why? Certain claims such as physician visits
excluded from demonstration project RACs target high dollar improper payments to
maximize contingency fees
25
26
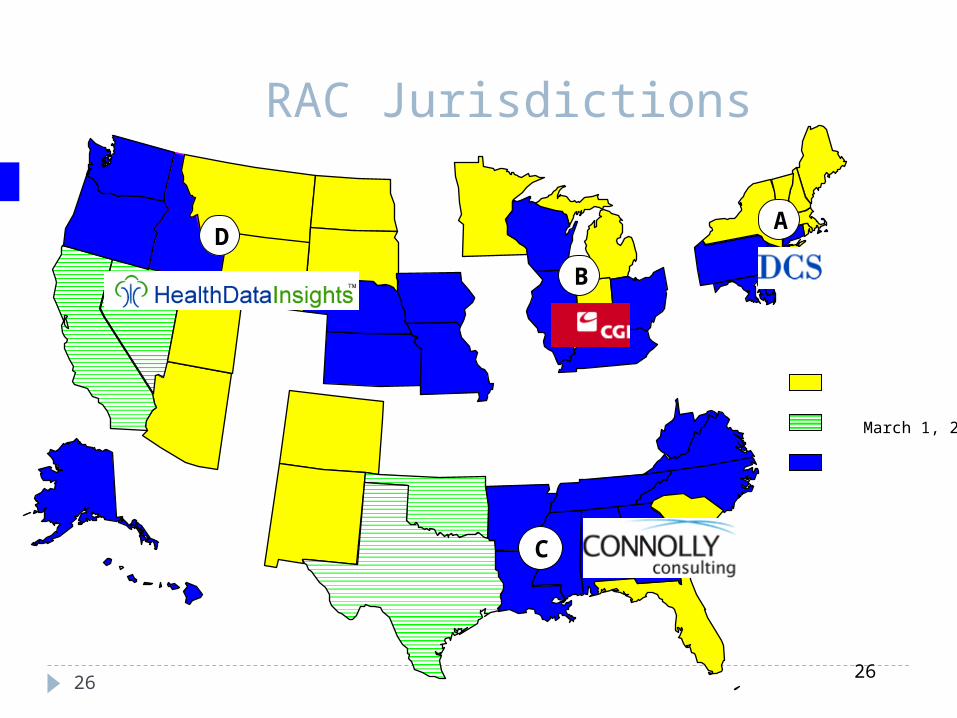
D
C
B
A
RAC Jurisdictions
March 1, 2009
326

Differences Between Demonstration and Permanent RACs
Strategy Demonstration RACs Permanent RACs
RAC Medical Director Not Required Mandatory
Coding Experts Optional Mandatory
Validation Process Optional Mandatory
RAC must payback the contingency fee if the claim overturned at any level of
Appeal
RAC must pay back contingency fee if the claim is overturned on
the first level of appeal
RAC must pay back if the claim is overturned on any level of
appeal
Claims Reviewed Records from three prior fiscal years
Claims with initial determination on or after October 1, 2007
Number of Records Requested No limit per SOW To be set by CMS
27
Know your enemy(oops, I meant RAC)From Connolly’s website:
“Connolly is now the healthcare industry's largest data mining recovery audit firm, reviewing over $120 billion in paid medical claims annually.”
All RACs are paid on a contingency basisIn FY 2007, payments for contingency fees
and other administrative expenses totaled $77.7 million
Good news: Connolly’s contingency only 9% (lowest of all national RACs)—others are 12%
28

29
RAC Review Process
RACs review claims on a post payment basis RACs use the same Medicare policies as FIs, Carriers and
MACs NCDs, LCDs & CMS manuals
Two types of review: Automated (no medical record needed) Complex (medical record required)
RACs will NOT be able to review claims paid prior to October 1, 2007 RACs will be able to look back three years from the date
the claim was paid RACs are required to employ a staff consisting of nurses,
therapists, certified coders & a physician CMD
529
30
RAC Program’s Three Keys to Success
1. Minimize Provider Burden 2. Ensure Accuracy 3. Maximize Transparency
630
31
Minimize Provider Burden
Limit the RAC “look-back period” to three years Maximum look back date is October 7, 2007
RACs will accept imaged medical records on CD/DVD
Limit the number of medical record requests (based on previous year Medicare volume)—We’ll talk about this in a minute…
731

32
Ensure Accuracy
Each RAC employs: A physician medical director Certified coders
CMS’ New Issue Review Board provides greater oversight
RAC Validation Contractor provides annual accuracy scores for each RAC
If a RAC loses at any level of appeal, the RAC must return the contingency fee
832
33
Maximize Transparency
New issues are posted to the web
Major Findings are posted to the web
RAC claim status web interface Detailed Review Results Letter following all Complex Reviews
933

Automated Reviews (Part B 2010)
RAC makes a claim determination at the system level without human review of the medical record Coverage / coding determination made through automated
review when the following applies: Certainty the service is not covered or is incorrectly coded, AND
Written Medicare policy Medicare article or Medicare sanctioned coding guidelines exist
CPT Statements CPT Assistant Statements Coding Clinic Statements
Other determinations made through automated reviews Duplicate Claims Pricing mistakes Units Discharge Disposition / Transfer DRG
35
Complex Reviews
• Reviews requiring human review of the medical record
• Where there is a high probability that the service is not covered
• Copies of medical records will be needed to support overpayment
• Use of proprietary data scrubber identifying cases with highest probability of DRG changes
Medical Necessity1 Day StaysOBSIncorrect coding3 day qualifying stay36
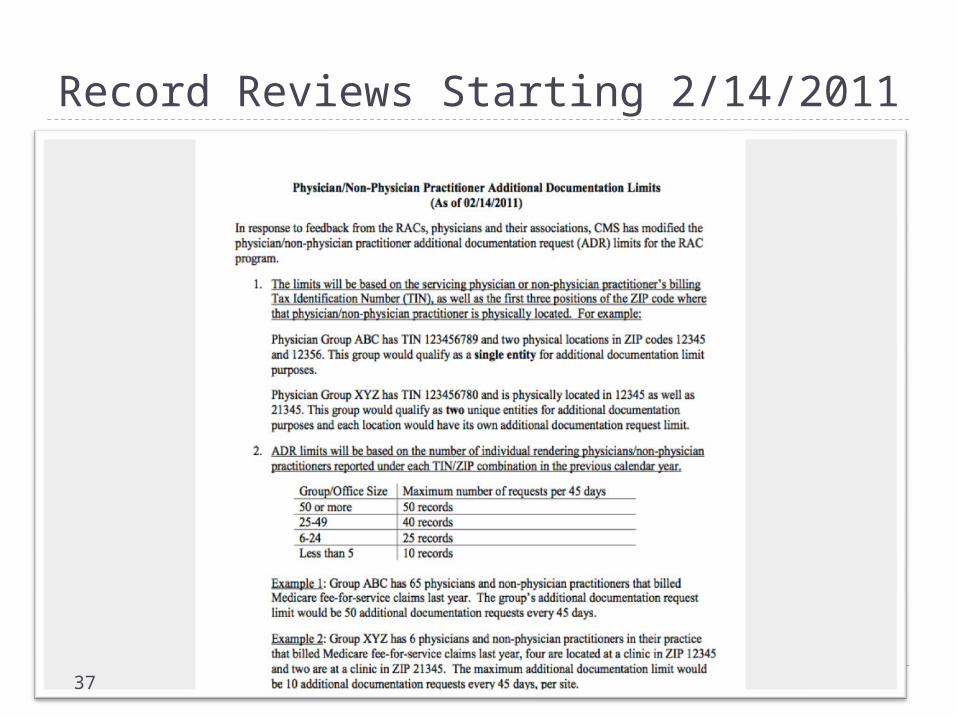
Record Reviews Starting 2/14/2011
37

RAC Updates Through COA
Go to CAN web site http://communityoncology.info
Select your RAC Region Then, you can click on your RAC Issues by STATE
38

Oncology Specific: Region A (Check Individual States)DCS
Multiple DME Rentals CSW Services During
Inpatient Pharmacy Supply
dispensing Fee: Orals Date of Death vs. DME -TC During Inpatient IV Hydration Units TC/PC Issues Claims overpaid for add-on
codes when the required primary procedure is not billed on any claim (same or different) for the same date of service.
DCS Transfusions Neulasta Once In A Lifetime New vs Established
patients Duplicate Claims CCI Edits Add-on Codes With No
Qualifying Place of service codes Identification of overpayments associated
with providers billing 'initial' intravenous infusion (90765 and 96365), and subcutaneous infusion (90769 and 96369) with more than 1 unit per day
39

Oncology Specific Region BBlood TransfusionsHydrationNeulastaOnce In A LifetimeAdd-on codes without the primary procedure
40
RAC Issues—Region CPart B Offices
Dose versus billedFulvestrantPalonosetronFilgrastim 480 mcgDolasetronRituximabLeuprolidePaclitaxelCetuximabAbraxane
41

RAC Issues—Region CHospital Outpatient
Units Billed versus DoseTenecteplasePamidronate sodiumAdenosineZoledronic Acid IrinotecanDocetaxelCarboplatinBevacizumabDarbepoetin
42
RAC Issues-Region C Both Settings
CSW During Hospital Stay Admit Order for Admission Blood Transfusions IV Hydration Pegfilgrastim Units of Service Billing the pharmacy supplier fee in error Duplicate claims
43

Region D Oncology Specific IssuesPlace of ServiceOnce In A LifetimeTransfusionPegfilgrastimTC vs. PCCSW During InpatientHydrationSNF vs Part BA4221 units of
serviceHospice vs. Part B
Date of DeathInfusion Pump vs.
SuppliesMUEsDME Duplicate ClaimsNew vs. Established
PatientNCCI EditsDME In HospicePart B Duplicate
Claims
44
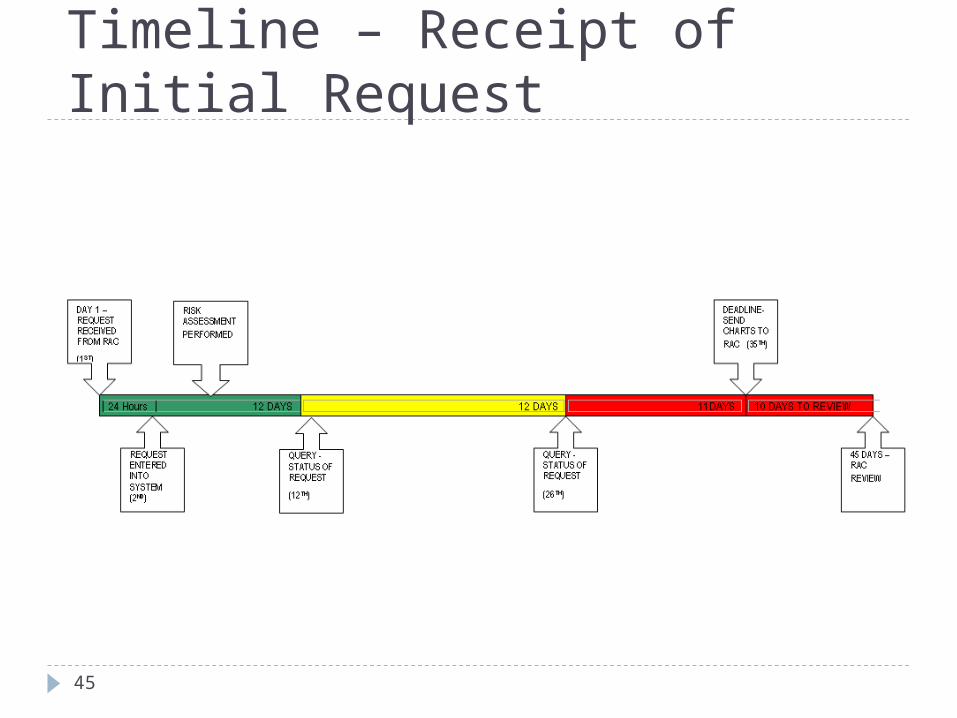
Timeline – Receipt of Initial Request
45
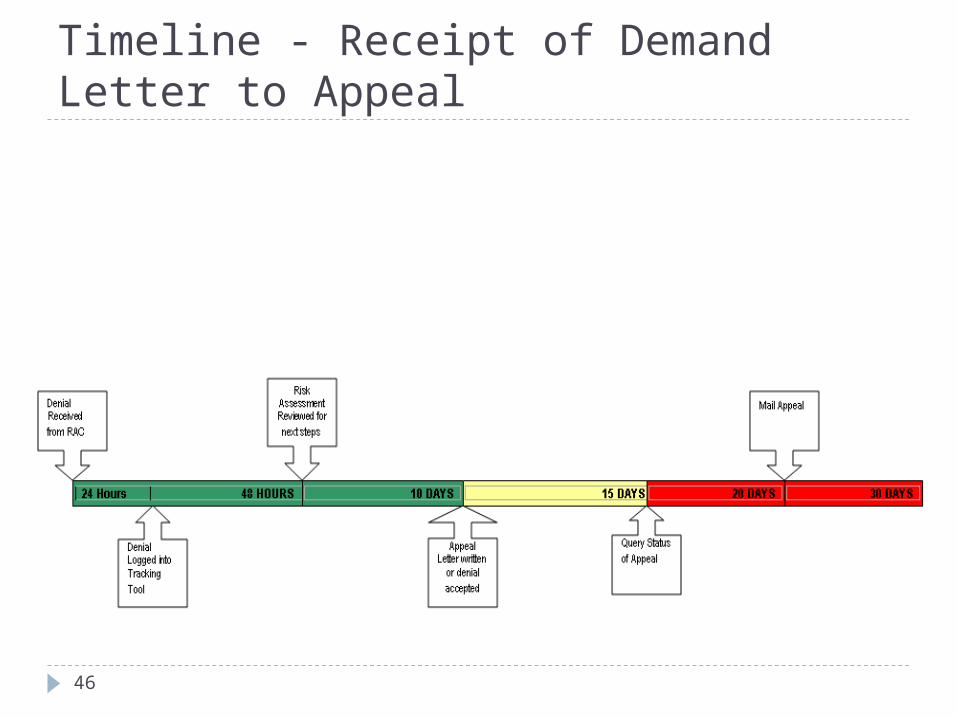
Timeline - Receipt of Demand Letter to Appeal
46
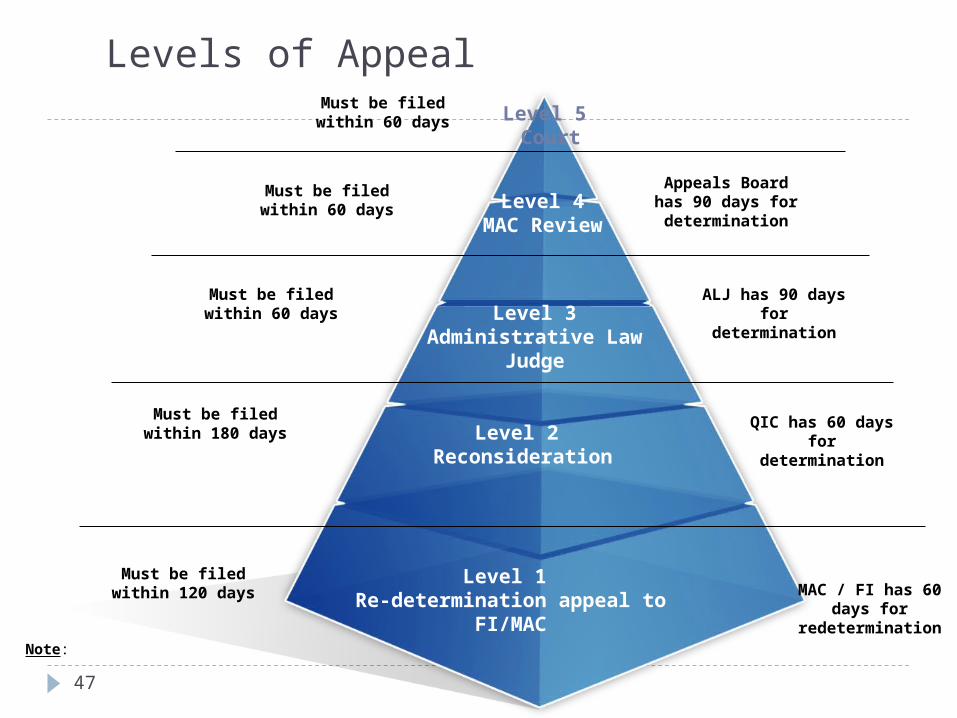
Levels of Appeal
Level 1 Re-determination appeal to
FI/MAC
Level 2 Reconsideration
Level 3Administrative Law
Judge
Level 4MAC Review
Level 5 Court
Must be filed within 120 days MAC / FI has 60
days for redetermination
Must be filed within 180 days
QIC has 60 days for
determination
ALJ has 90 days for
determination
Must be filed within 60 days
Must be filed within 60 days
Must be filed within 60 days
Appeals Board has 90 days for determination
Note:
47

Medicaid Integrity ContractorsReview Medicaid claims for inappropriate
payments or fraud. Similar to the RACs, the MICs will use a data-driven approach to focus efforts on aberrant billing practices.
Three Types:Review MICAudit MICEducation MIC
Contracting Right Now!
http://www.cms.hhs.gov/medicaidintegrityprogram/ http://www.tha.org/HealthCareProviders/Advocacy/
FederalIssues/MedicaidRACAudits/hms%20-%20Medicaid%20Integrity%20Audit%20Overview.ppt#931,11,Audit MIC Contractors
48

Medicaid Integrity Contractors
MICs are paid a fee for their services; plus a bonus tied to quality of work, not quantity of recoupment
http://www.ipro.org/index
http://www.ipro.org/index/news-app/story.27/title.ipro-awarded-medicaid-integrity-program-task-order-by-cms
49
Medicaid Integrity ContractorsPossible Targets Include:Services Provided After the Death of a
BeneficiaryDuplicate ClaimsUnbundling of ServicesOP Claims That Overlap With IP StayUnlikely ServicesExcluded Individuals
Possible Medical record reviews:Documentation and Medical NecessityDiagnosis and Procedure CodingCovered ServicesAppropriate Billing and Reimbursement
50
Medicaid Integrity ContractorsThe MIC Program is Based on State Guidelines,
Not the Same as RAC: Look-back PeriodAfter the audit providers deal with their stateMedical Record Request LimitsMedical Record TAT (MA is 30 Days)MICs will not review every claim; instead, they
will select a sample and then extrapolate the results over the universe of claims
51
Medicaid Integrity Contractors
Nearly 750 medical record audits are under way in 25 states, with the help of an additional 3,800 state program integrity officials.
Audits Targets Involve: Hospitals, SNF/NH, Home Health, Hospice, ESRD, Labs, Radiology, DME, Pharmacies, Ambulance and Physicians/Practitioners.
$24M in overpayments identified.
Robb Miller, Director, Division of Field Ops, CMS Medicaid Integrity Group November 3, 2009, Audio Conference (HCCA)
52
Others: ZPICsZone Program Integrity Contractors - formerly
known as Program Safeguard Contractors (PSCs), serve the same jurisdictions as the Medicare Administrative Contractors.
The ZPICs are authorized to conduct investigations, provide support to law enforcement and conduct audits of Medicare advantage plans.
Some ZPICs will concentrate on various Medicare billing "hot" targets.
53
Others: ZPICsProvide data analysis program are to identify
provider billing practices and services that pose the greatest financial risk to the Medicare program. Specifically:
Coverage and Coding Errors
Establish baseline data to enable the contractor to recognize unusual trends, changes in utilization over time or schemes
Identify where there is a need for LCD
Identify claim review strategies that efficiently prevent or address potential errors (e.g. prepayment edit specifications or parameters)
54

Others: ZPICs
Produce innovative views of utilization or billing patterns that illuminate potential errors
Identify high volume or high cost services that are being widely over-utilized. Otherwise these services do not appear as an outlier and may be overlooked when, in fact, they pose the greatest financial risk
Identify and target program areas and/or specific providers for possible fraud investigations
55
Others: MACs Medicare Administrative Contractors process
claims for both Part A and Part B services. They are charged with overseeing claim completion and accuracy in addition to determining correct payments for services.
Since MACs review both facility Part A claims and the professional provider Part B claims related to the same beneficiaries and services, CMS feels that the MACs will be able to review discrepancies between the two sets of claims, revise payments and/or increase denials.
MACs have revived the Comprehensive Error Rate Testing (CERT) program.
56
Particularly Nasty WPS:
99211 with warfarin/anti-coagulant reviews “High dollar” claims CERT by specialty
Highmark 99204, 99205 review
57

Highmark 99204, 99205 A recent widespread post payment audit performed by Highmark Medicare Services’ Medical Review
Department revealed that 73% of new patient office or outpatient visits, procedure codes 99204 and 99205, were billed incorrectly. While the number one error was incorrectly coding the level of service, other issues were identified. The issues included the lack of an accepted form of provider signature, the documentation did not support incident to guidelines as there was no evidence of the physician initiating the plan of care, and no documentation was received to support the services billed. In order to bill a new patient office or outpatient visit, the patient must not have received any professional service from any physician in the group of the same specialty within the last three years.
As a result of these review findings, a prepayment edit will be implemented on procedure codes 99204 and 99205 for physicians and non-physician practitioners (NPP) of all specialties.
Medicare requires that medical record entries for services provided/ordered be authenticated by the author. The method used shall be a hand written or an electronic signature. Stamp signatures are not acceptable. Patient identification, date of service, and provider of the service should be clearly identified on the submitted documentation.
If you question the legibility of your signature, you may submit an attestation statement with the documentation. A suggested format for attestation statements can be found on our website. The signature attestation statement must be signed by the provider. If the signature requirements are not met, the reviewer will conduct the review without considering the documentation with the missing or illegible signature. This could lead the reviewer to determine that the medical necessity for the service billed has not been substantiated.
In order to bill the services of an NPP such as a physician assistant or a nurse practitioner incident to a physician, there must have been a direct, personal, professional service furnished by the physician to initiate the course of treatment of which the service being performed by the NPP is an incidental part, and there must be subsequent services by the physician of a frequency that reflects the physician’s continuing active participation in and management of the course of treatment. In addition, the physician must be physically present in the same office suite and be immediately available to render assistance if that becomes necessary. If services are rendered to a new patient, there is no course of treatment already initiated by the physician, therefore, the service provided by the NPP may not be billed under the physician’s rendering provider number. 58
Others: HEATThe Healthcare Fraud Prevention and Enforcement
Action Team (HEAT) combats Medicare fraud. An interagency effort and the expansion of Strike Force team operations to Detroit and Houston including the expansion of joint DOJ-HHS Medicare Fraud Strike Force teams that have been fighting fraud in south Florida and Los Angeles.
Established in 2007, the teams have used a “data-driven” approach to identify unexplainable billing patterns and investigating these providers for possible fraudulent activity.
59

PPCA Revised Compliance Requirements Mandatory Compliance Program for All Providers
HHS Secretary authorized to require as a condition of enrollment in the Medicare program that classes of providers and suppliers implement compliance programs
Secretary has discretion to dictate the timelines for implementation of compliance programs, as well as the types of providers and suppliers who will be required to adopt compliance programs
Law directs the Secretary to develop core elements of compliance programs for each class of provider or supplier required by the Secretary to adopt them
RAC Program Expansion to Medicaid Effective December 31, 2010, States must establish contracts
with one or more RAC contractors Will identify underpayments and overpayments and recoup
overpayments
60

Physician Practice Compliance ProgramFoundation for an Effective Compliance
& Ethics Program (OIG’s 7 Elements)1. Standard Policies & Procedures2. Oversight & Documentation
Responsibility3. Education & Training4. Lines of Communication5. Audit & Monitoring6. Enforcement & Discipline7. Response & PreventionTo see the whole thing: oig.hhs.gov/authorities/docs/physician.pdf
61

Mandatory Reporting & Repayment Of Overpayments
PPACA 6402(d): “If a person has received an overpayment, the person shall –
(A) report and return the overpayment to the Secretary, the State, an intermediary, a carrier, or a contractor, as appropriate, at the correct address;
(B) Notify the Secretary, State, intermediary or carrier to whom the overpayment was returned in writing of the reason for the overpayment.”
62

When Must The Overpayment Be Reported/Returned?
An overpayment must be reported and returned the later of –(A) the date which is 60 days after the date on which the overpayment was identified; or(B) the date any corresponding cost report is due, if applicable
63
Failure To Return Money Is A False Claim“Any overpayment retained by a person after
the deadline for reporting and returning the overpayment is an obligation as defined in Section 3729(b)(3) of title 31 USC (False Claims Act).
64
What Is An Overpayment?“The term ‘overpayment’ means any funds that
a person receives or retains under title XVIII or XIX to which the person, after appropriate reconciliation, is not entitled.”
65
Kickback As An OverpaymentPPACA 6402(g): “ . . . A claim that includes
items or services resulting from a violation of this section (a kickback) constitutes a false or fraudulent claim for purposes of” the False Claims Act”
66

To Do’sHave a compliance plan and make it a priority.From your RAC issues, identify areas of risk in your
region.Audit these areas that I have identified as high risk
for almost everybody: Consults and New Patients “Incident to” Drug units New versus established patients Nursing drug administration documentation
If you are at risk for whistle blower(s), hire and attorney to implement your compliance program.
GIVE THE $$ BACK!Educate! Educate! Educate!
67

68