



FLU-FOBT and FLU-FIT Programs: The FLU-FOBT program: pairing colorectal cancer screening with another essential preventative service.
California Colorectal Cancer Roundtable, April 2012Mike Potter, UCSF/San Francisco Bay Area Collaborative Research Network
• Describe FLU-FOBT and FLU-FIT Programs and their potential role to increase access to colorectal cancer screening.
• Consider other opportunities to pair colorectal cancer screening with other essential health services.
Objectives
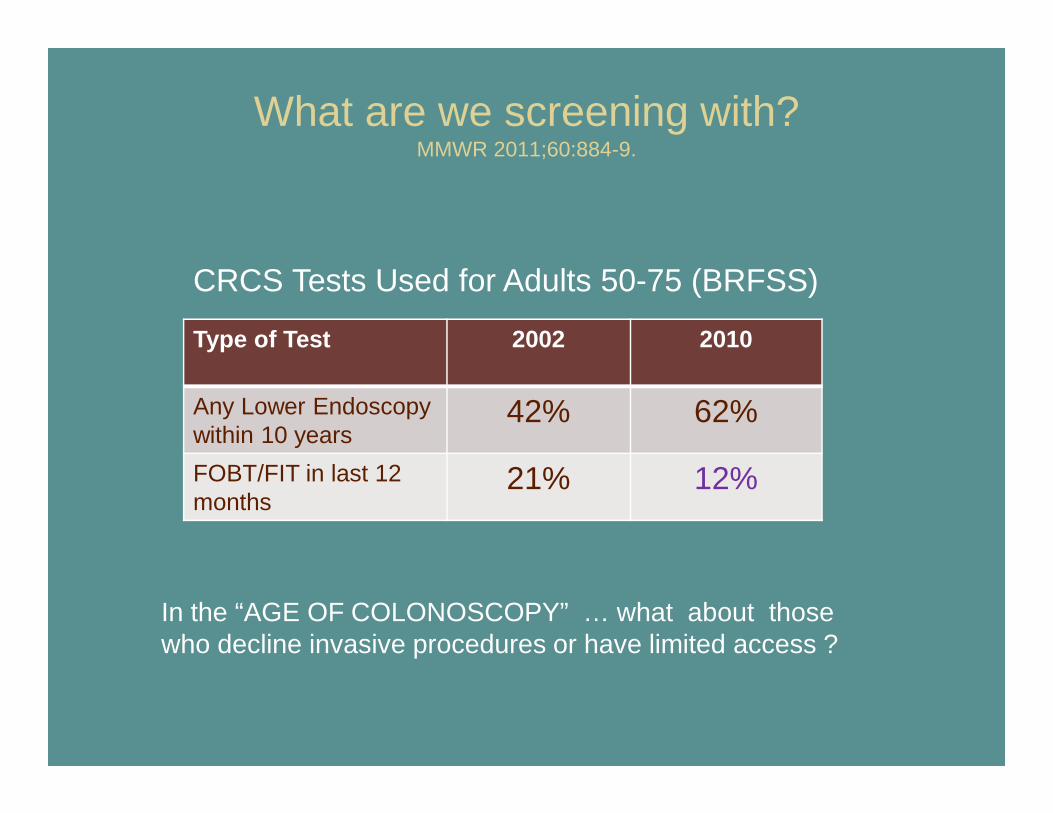
What are we screening with?MMWR 2011;60:884-9.
Type of Test 2002 2010
Any Lower Endoscopywithin 10 years
42% 62%
FOBT/FIT in last 12 months
21% 12%
In the “AGE OF COLONOSCOPY” … what about those who decline invasive procedures or have limited access ?
CRCS Tests Used for Adults 50-75 (BRFSS)
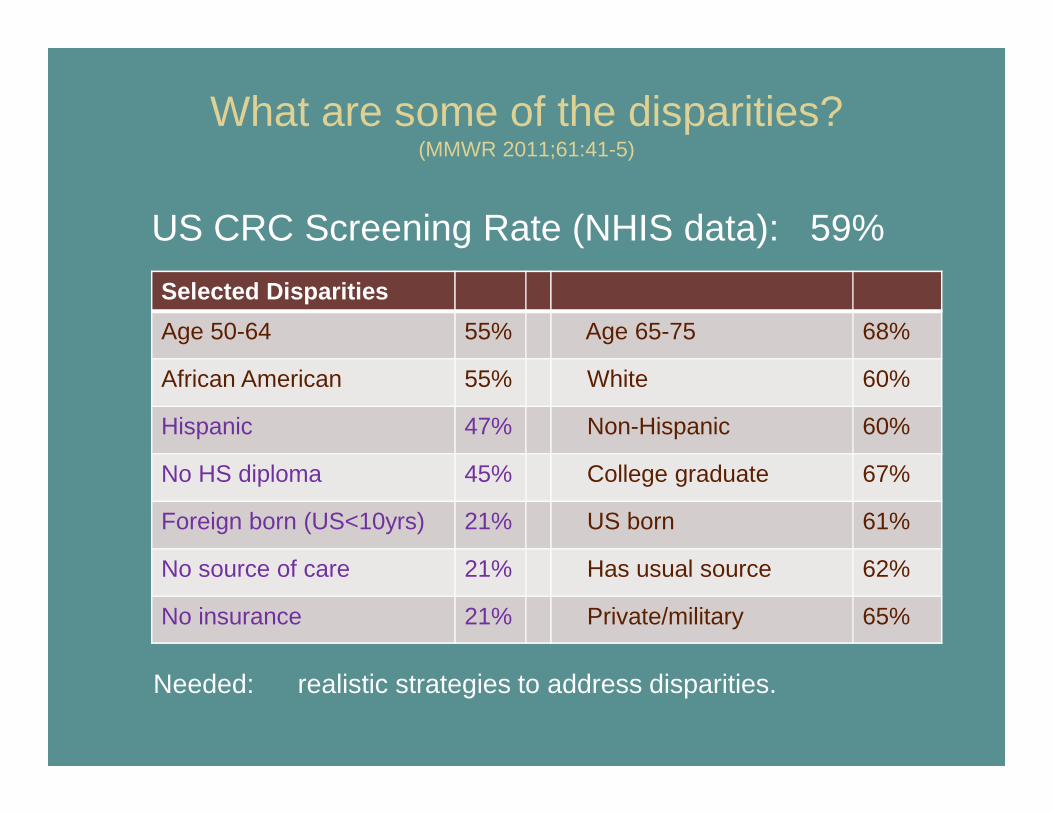
What are some of the disparities? (MMWR 2011;61:41-5)
US CRC Screening Rate (NHIS data): 59%
Selected Disparities
Age 50-64 55% Age 65-75 68%
African American 55% White 60%
Hispanic 47% Non-Hispanic 60%
No HS diploma 45% College graduate 67%
Foreign born (US<10yrs) 21% US born 61%
No source of care 21% Has usual source 62%
No insurance 21% Private/military 65%
Needed: realistic strategies to address disparities.
Rationale for FOBT & FIT and FOBT & FIT Outreach Programs
• FOBT/ FIT remains an effective, inexpensive, and essential component of national efforts to increase CRCS rates across all populations.
• FOBT/FIT can be provided with algorithm-driven care by individuals with limited clinical training.
• Organized outreach programs can complement the work of primary care clinicians.
Rationale for Pairing FOBT/FIT with Influenza Vaccination Activities
• Screening opportunity for individuals not reached or responding to other methods.
• Efficient bundling of preventive services.
• Engages non-clinician staff in a yearly cancer screening campaign.
• Provides a message to clinic staff, patients and the community that “Just like flu shots, FOBT/FIT should be done every year”
San Francisco General HospitalFamily Health Center
Грипп можно предотвратить! Рак толстой кишки можно предотвратить!·• Проводить ежегодно анализ кала очень просто.
•Проведение анализа кала ежегодно может спасти вам жизнь.
• Обследование с целью предотвращения рака толстой кишки рекомедуется докторами всем женщинам и мужчинам в возрасте от 50 до 79лет.
•Когда нужно сделать тест? Мы скажем Вам об этом сегодня.
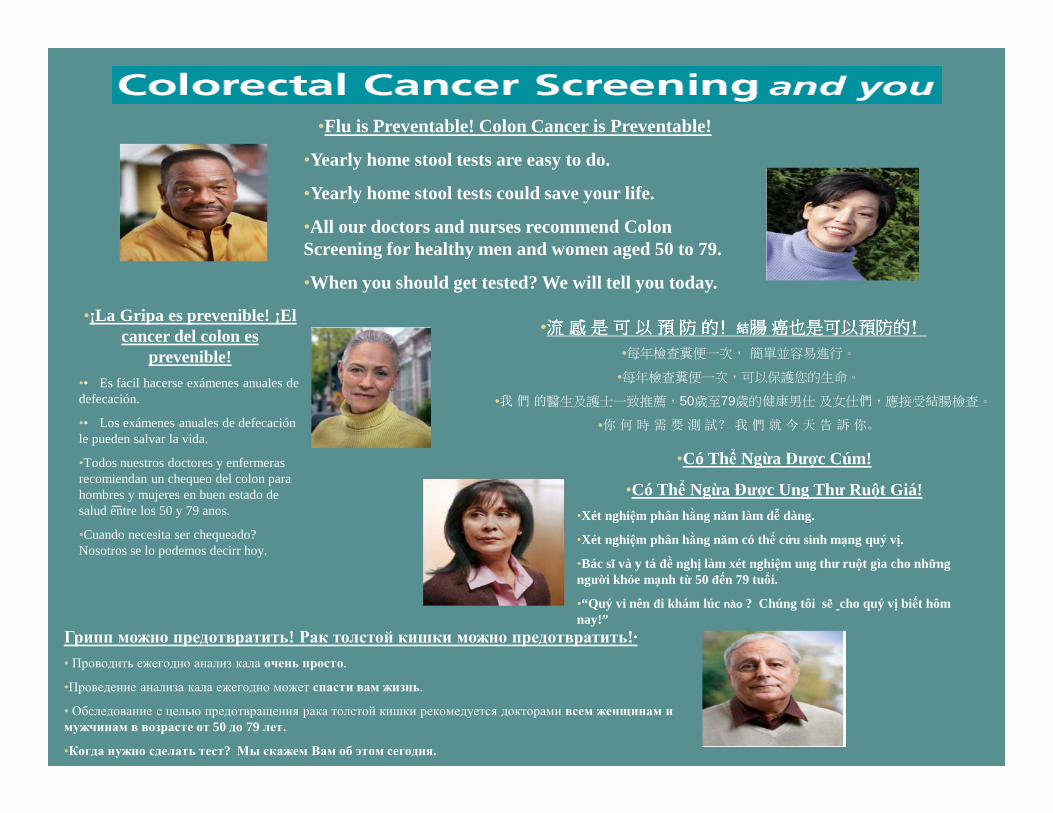
•Flu is Preventable! Colon Cancer is Preventable!
•Yearly home stool tests are easy to do.
•Yearly home stool tests could save your life.
•All our doctors and nurses recommend Colon Screening for healthy men and women aged 50 to 79.
•When you should get tested? We will tell you today.
•Có Thể Ngừa Được Cúm!
•Có Thể Ngừa Được Ung Thư Ruột Giá!•Xét nghiệm phân hằng năm làm dễ dàng.
•Xét nghiệm phân hằng năm có thể cứu sinh mạng quý vị.
•Bác sĩ và y tá đề nghị làm xét nghiệm ung thư ruột gìa cho nhữngngười khỏe mạnh từ 50 đến 79 tuổi.
•“Quý vi nên đi khám lúc nào ? Chúng tôi sẽ cho quý vị biết hômnay!”
•¡La Gripa es prevenible! ¡El cancer del colon es
prevenible!•• Es fácil hacerse exámenes anuales de defecación.
•• Los exámenes anuales de defecaciónle pueden salvar la vida.
•Todos nuestros doctores y enfermerasrecomiendan un chequeo del colon parahombres y mujeres en buen estado de salud entre los 50 y 79 anos.
•Cuando necesita ser chequeado? Nosotros se lo podemos decirr hoy.
•流流流流 感感感感是是是是 可可可可以以以以 預預預預防防防防 的的的的﹗﹗﹗﹗結結結結腸腸腸腸癌也是可以預防的癌也是可以預防的癌也是可以預防的癌也是可以預防的﹗﹗﹗﹗
•每年檢查糞便一次, 簡單並容易進行。
•每年檢查糞便一次,可以保護您的生命。
•我們的醫生及護士一致推薦,50歲至79歲的健康男仕及女仕們,應接受結腸檢查。
•你何時需要測試?我們就今天告訴你。
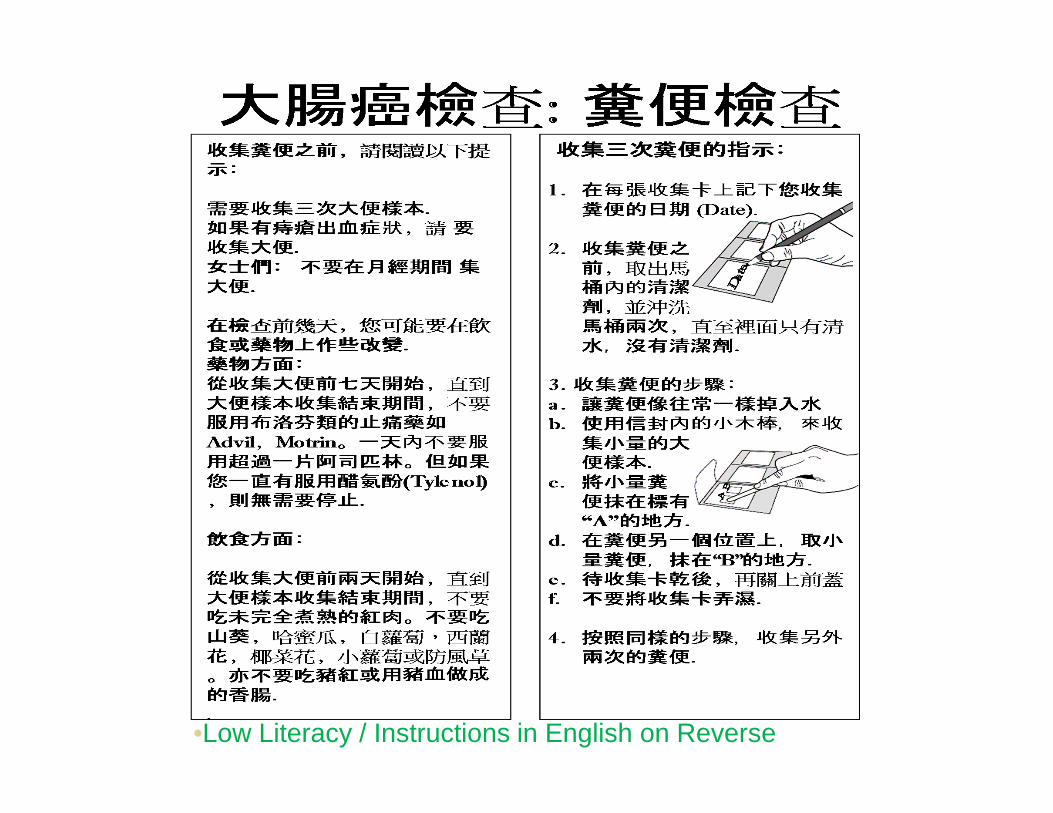
•Low Literacy / Instructions in English on Reverse
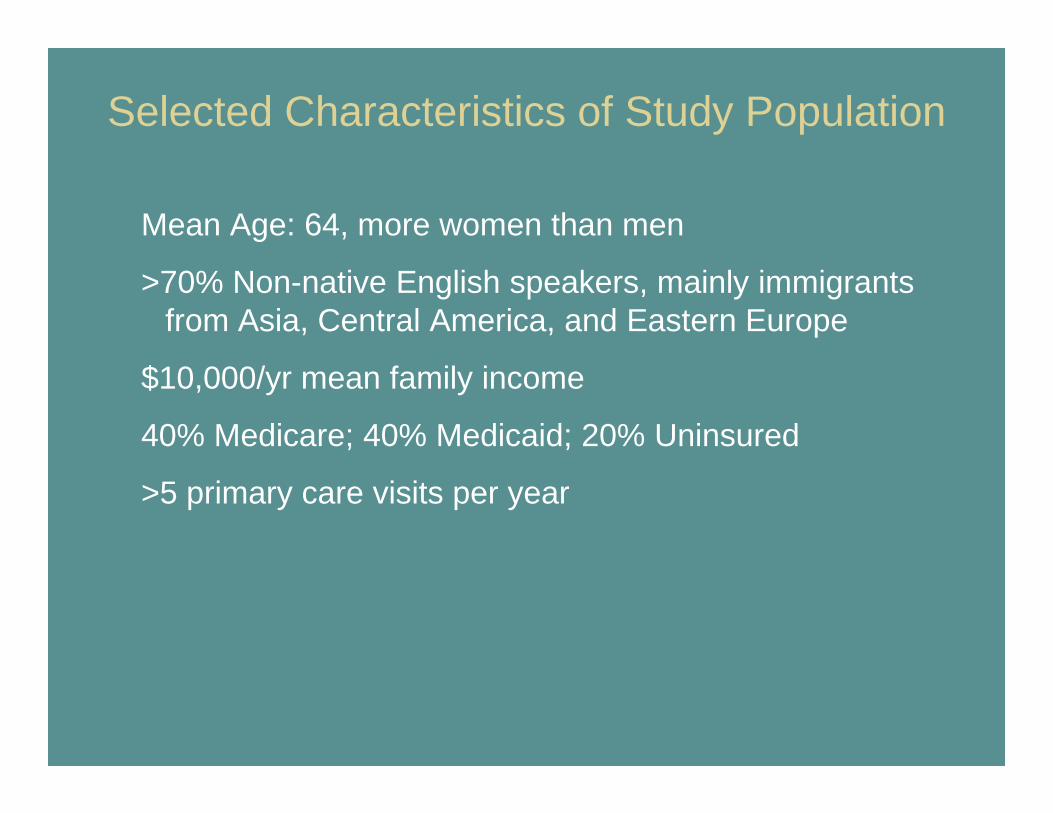
Selected Characteristics of Study Population
Mean Age: 64, more women than men
>70% Non-native English speakers, mainly immigrants from Asia, Central America, and Eastern Europe
$10,000/yr mean family income
40% Medicare; 40% Medicaid; 20% Uninsured
>5 primary care visits per year
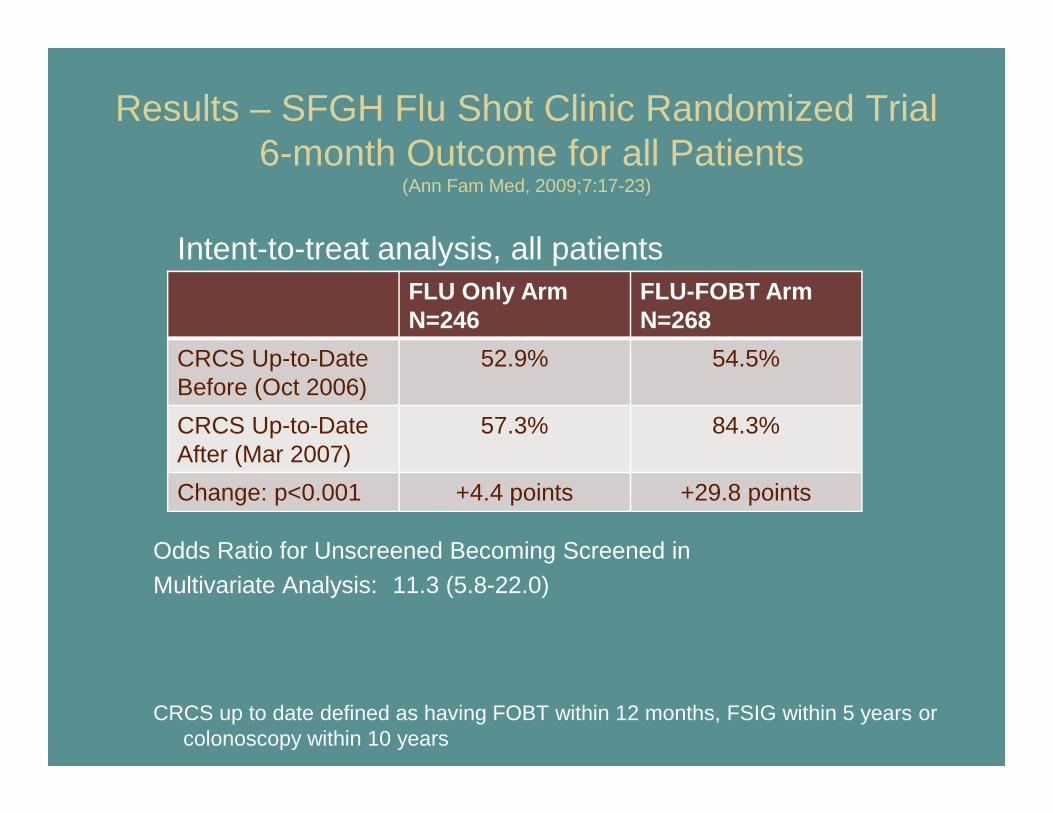
Results – SFGH Flu Shot Clinic Randomized Trial6-month Outcome for all Patients
(Ann Fam Med, 2009;7:17-23)
Odds Ratio for Unscreened Becoming Screened inMultivariate Analysis: 11.3 (5.8-22.0)
CRCS up to date defined as having FOBT within 12 months, FSIG within 5 years or colonoscopy within 10 years
FLU Only ArmN=246
FLU-FOBT ArmN=268
CRCS Up-to-DateBefore (Oct 2006)
52.9% 54.5%
CRCS Up-to-Date After (Mar 2007)
57.3% 84.3%
Change: p<0.001 +4.4 points +29.8 points
Intent-to-treat analysis, all patients
Translating findings into practice
• Move from efficacy to effectiveness– Adapting for “real world” settings with lower
baseline screening rates, less external support, no phone reminders, etc.
• Reproduce results in diverse settings and populations
• Develop tools for dissemination
FLU-FOBT and FLU-FIT Projects
• San Francisco Dept of Public Health (with Judith Walsh and Steve McPhee)
– CDC R18 (2008-2011) “Translation of an Evidence-Based Colorectal Cancer Screening Intervention to Primary Care Settings Where Disparities Persist ”
• Kaiser Permanente Northern California (with Carol Somkin)– HMO Cancer Research Network (2008-2009) “Preparation for the FLU-FIT
Program at Kaiser Permanente Santa Clara”– ACS Research Scholars Grant (2009-2012) “Colorectal Cancer Screening
with During Annual Flu Shot Clinics at Kaiser Perma nente”
• Walgreens Pharmacies (with Lisa Kroon)– Alexander and Margaret Stewart Trust (2008-2009) “A Pharmacy-Based
Intervention to Increase Colorectal Cancer Screenin g”
Integrating the FLU-FOBT Program with Routine Primary Care Visits

Visual Aids and Video Instructions for non-English speaking and/or for low literacy patients (for guaiac FOBT)
Randomized Trial: 6 SFDPH Health Centers(Focusing on effectiveness with limited resources: clinics given uniform training and resources, but flexibility in implementation, without phone reminders for patients)
Selected Characteristics of Study Population
Mean Age: 60, more men than women
35% African American, 25% Non-Hispanic white
>80% English as primary language
35% Medicare, 30% Medicaid, 35% Uninsured
Large number of marginally housed patients
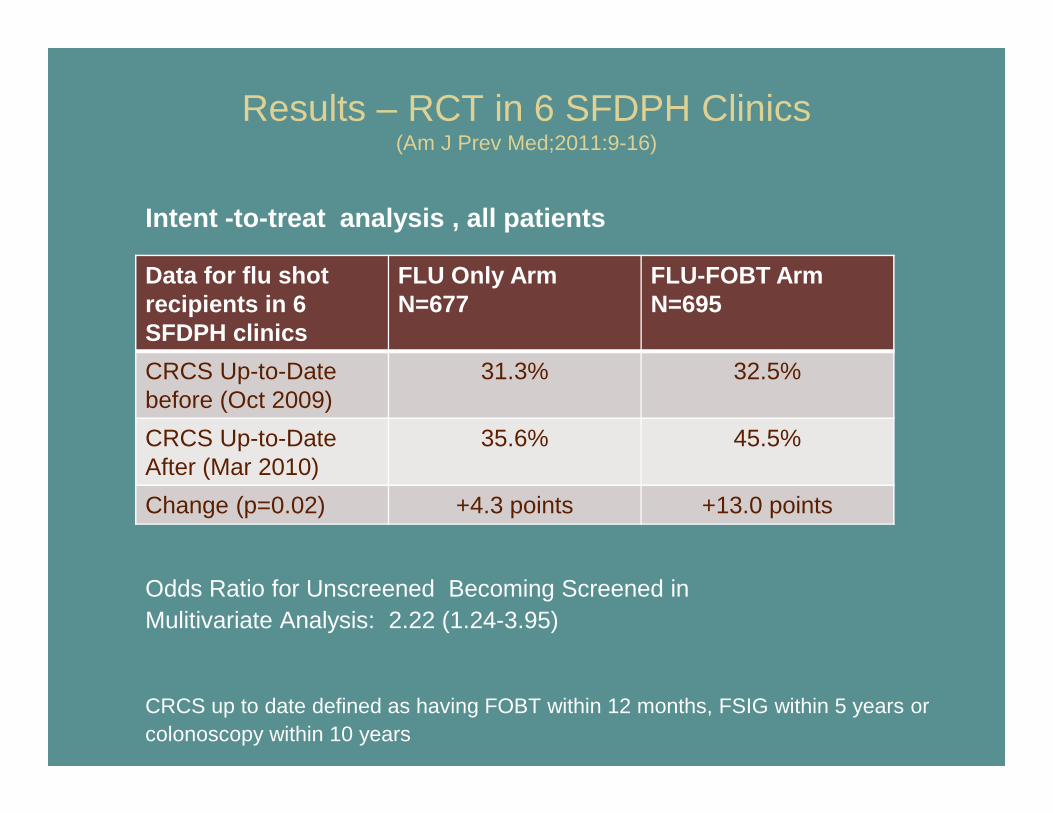
Results – RCT in 6 SFDPH Clinics(Am J Prev Med;2011:9-16)
Intent -to-treat analysis , all patients
Odds Ratio for Unscreened Becoming Screened in Mulitivariate Analysis: 2.22 (1.24-3.95)
CRCS up to date defined as having FOBT within 12 months, FSIG within 5 years or colonoscopy within 10 years
Data for flu shot recipients in 6 SFDPH clinics
FLU Only ArmN=677
FLU-FOBT ArmN=695
CRCS Up-to-Datebefore (Oct 2009)
31.3% 32.5%
CRCS Up-to-Date After (Mar 2010)
35.6% 45.5%
Change (p=0.02) +4.3 points +13.0 points
Results – Lasting Changes in the Clinics(Health Educ Res, in press)
• One Year Later…
– 4 of 6 clinics continued FLU-FOBT Program
– Practice changes at all RCT sites:• Increased clinic staff responsibility for FOBT• FOBT patient education materials retained• Systems for patients to mail completed FOBT kits to lab
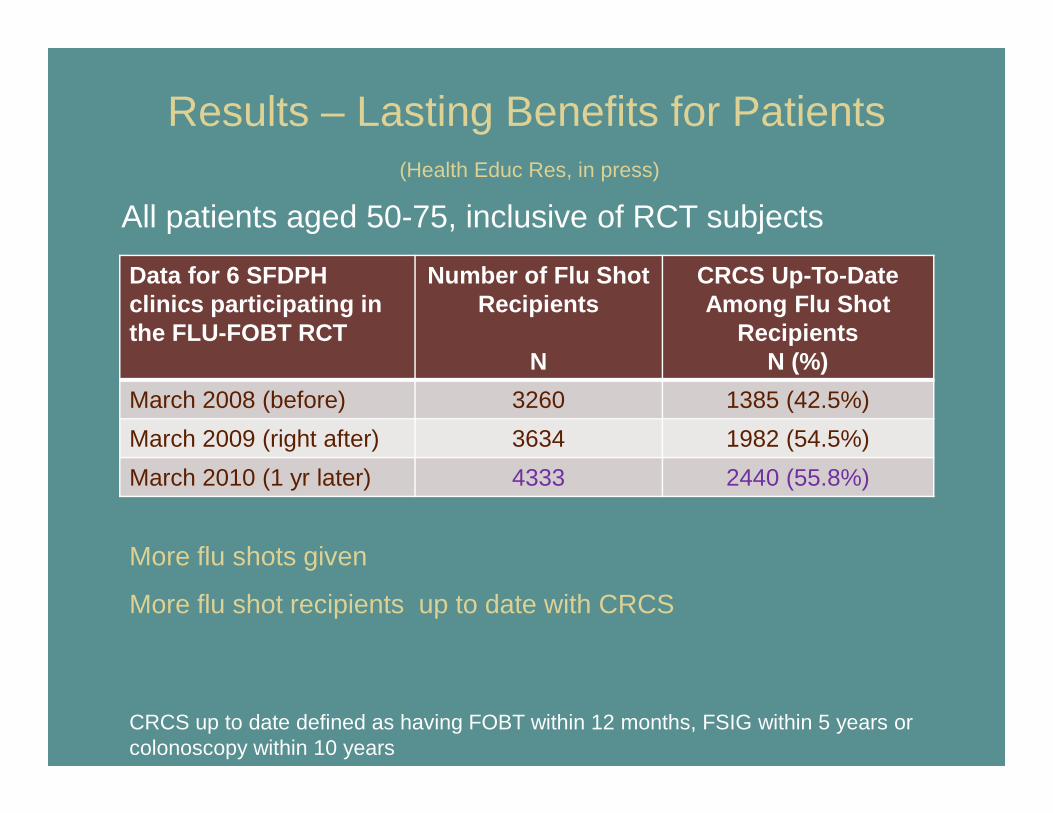
Results – Lasting Benefits for Patients(Health Educ Res, in press)
Data for 6 SFDPHclinics participating inthe FLU-FOBT RCT
Number of Flu Shot Recipients
N
CRCS Up-To-Date Among Flu Shot
RecipientsN (%)
March 2008 (before) 3260 1385 (42.5%)
March 2009 (right after) 3634 1982 (54.5%)
March 2010 (1 yr later) 4333 2440 (55.8%)
More flu shots given
More flu shot recipients up to date with CRCS
CRCS up to date defined as having FOBT within 12 months, FSIG within 5 years or colonoscopy within 10 years
All patients aged 50-75, inclusive of RCT subjects
FLU-FIT Program at Kaiser Permanente(with co-PI - Carol Somkin, PhD)
The FLU-FIT “Assembly Line” with use of EHR developed in 2007 and used in 2008 pilot study
KP Santa Clara FLU-FIT Pilot Program 2008
Kaiser RCT: Fresno, Richmond, Redwood City, South San Francisco and Union City
Selected characteristics of flu shot clinic attendees due for screening
• mean Age: 62 -- 57% female
• 45% w/no primary care visit in last year, 20% w/only 1 primary care visit in last year
• ethnically diverse communities
• all with Kaiser insurance
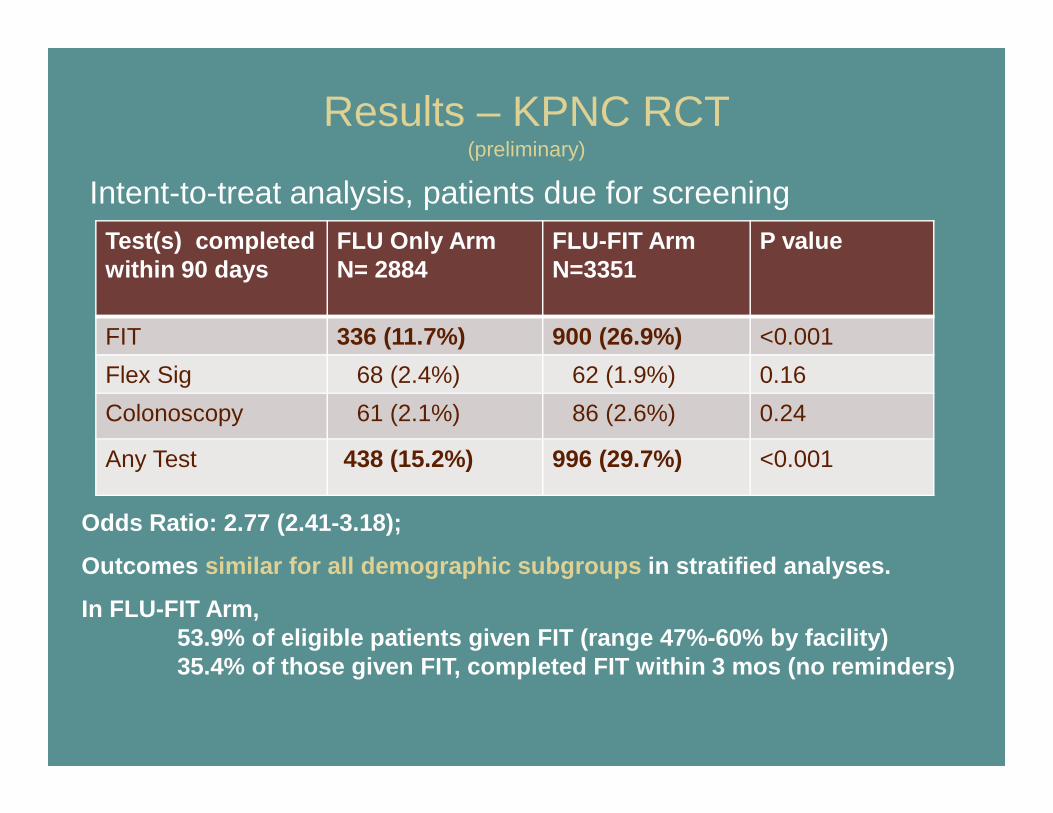
Results – KPNC RCT (preliminary)
Test(s) completed within 90 days
FLU Only ArmN= 2884
FLU-FIT ArmN=3351
P value
FIT 336 (11.7%) 900 (26.9%) <0.001
Flex Sig 68 (2.4%) 62 (1.9%) 0.16
Colonoscopy 61 (2.1%) 86 (2.6%) 0.24
Any Test 438 (15.2%) 996 (29.7%) <0.001
Odds Ratio: 2.77 (2.41-3.18);
Outcomes similar for all demographic subgroups in stratified analyses.
In FLU-FIT Arm, 53.9% of eligible patients given FIT (range 47%-60% by facility)35.4% of those given FIT, completed FIT within 3 mo s (no reminders)
Intent-to-treat analysis, patients due for screening
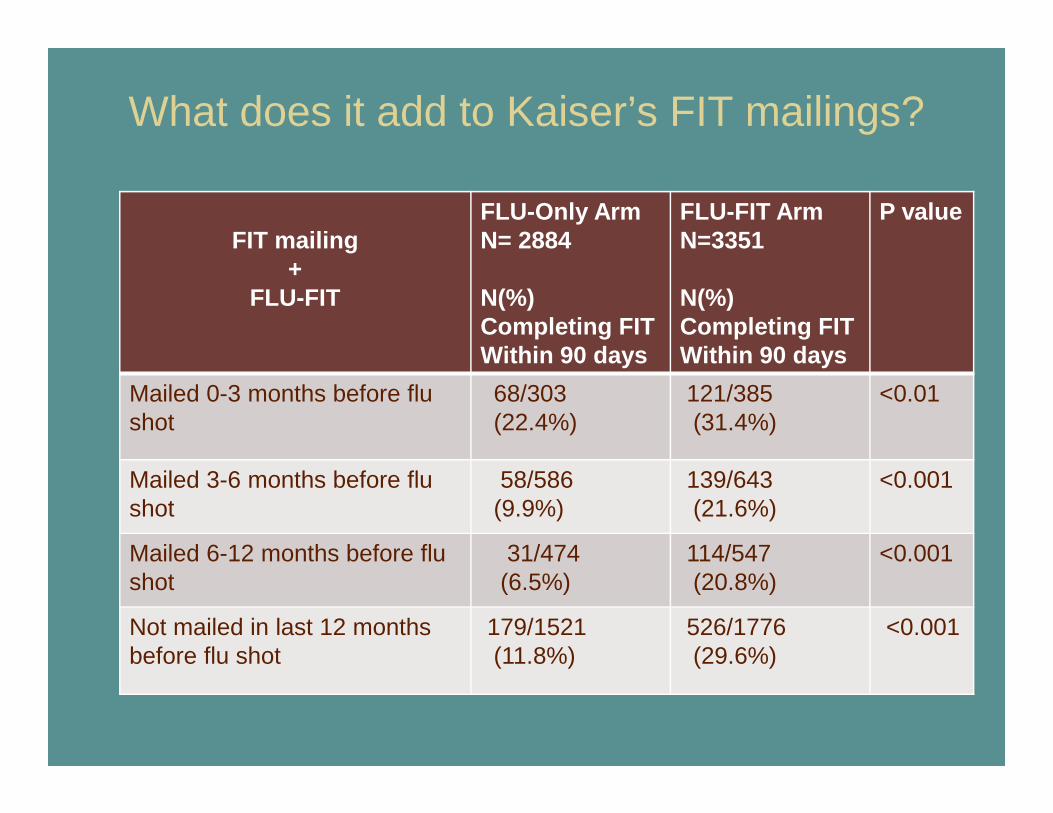
What does it add to Kaiser’s FIT mailings?
FIT mailing +
FLU-FIT
FLU-Only Arm N= 2884
N(%) Completing FITWithin 90 days
FLU-FIT ArmN=3351
N(%)Completing FITWithin 90 days
P value
Mailed 0-3 months before flu shot
68/303(22.4%)
121/385(31.4%)
<0.01
Mailed 3-6 months before flu shot
58/586(9.9%)
139/643 (21.6%)
<0.001
Mailed 6-12 months before flu shot
31/474(6.5%)
114/547 (20.8%)
<0.001
Not mailed in last 12 months before flu shot
179/1521(11.8%)
526/1776(29.6%)
<0.001
2011 Dissemination and Implementation Study Targeting All KPNC Facility Flu Shot Clinic Sites
•Endorsed but not required by KPNC Regional Leadership
•Disseminated through Regional Flu Shot Clinic Coordinators
•Hands-on training offered at KPNC’s Center for Innovation in San Leandro, CA.
•Webinar offered to new and experienced flu shot clinic sites
•Internal KPNC website with KPNC-specific procedures and downloadable materials created
Public version available at FluFIT.org
What happened in 2011?(preliminary data)
• 26 of 46 KPNC flu shot clinic sites tried offering FIT with flu shots in various ways.
• Established sites did very well; New sites had challenges without hands-on training.
• Other preventive services offered at many flu shot clinics (Pap referrals, mammograms, pneumococcal vaccines, etc).
• Survey of flu shot clinic leaders is underway.
25,000+ FIT kits dispensed since 2007
Walgreens Pilot Studymoving FLU-FIT into the community
Small Sample Pilot Study (n=114)Characteristics of Participants
Mean Age: 60, 70% White
>80% insured, >80% college educated
<30% with any CRC screening test in the past
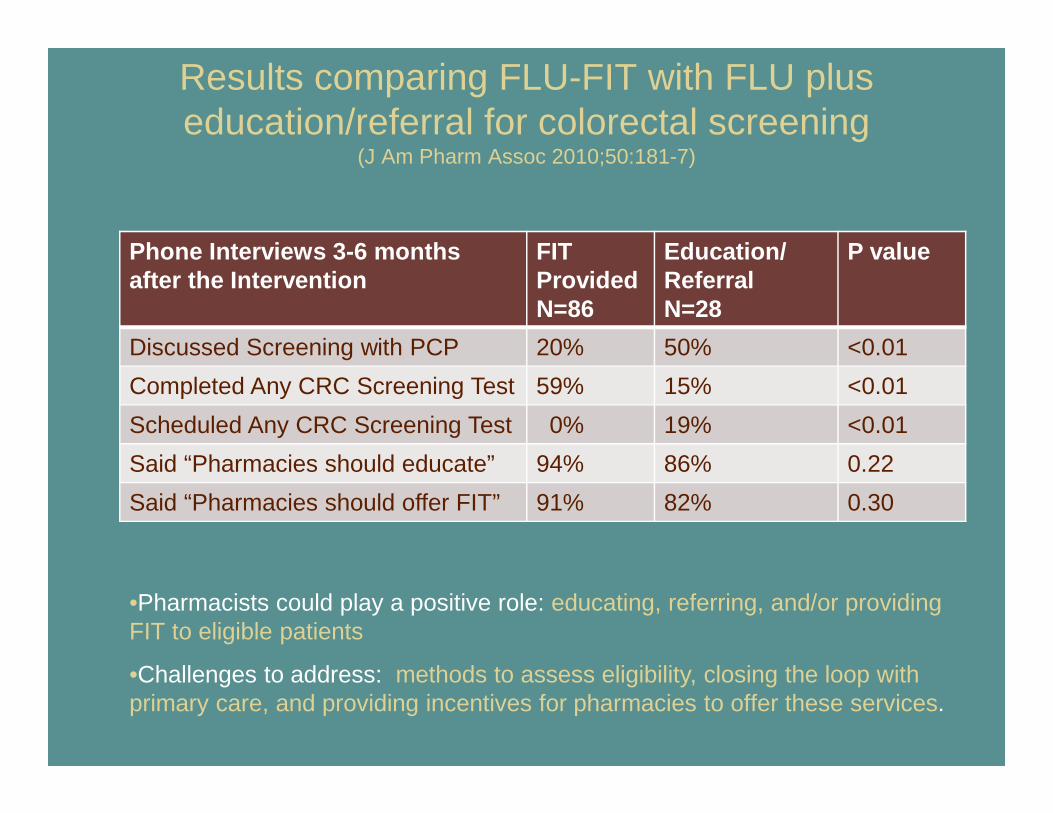
Results comparing FLU-FIT with FLU plus education/referral for colorectal screening
(J Am Pharm Assoc 2010;50:181-7)
Phone Interviews 3-6 months after the Intervention
FIT ProvidedN=86
Education/ReferralN=28
P value
Discussed Screening with PCP 20% 50% <0.01
Completed Any CRC Screening Test 59% 15% <0.01
Scheduled Any CRC Screening Test 0% 19% <0.01
Said “Pharmacies should educate” 94% 86% 0.22
Said “Pharmacies should offer FIT” 91% 82% 0.30
•Pharmacists could play a positive role: educating, referring, and/or providing FIT to eligible patients
•Challenges to address: methods to assess eligibility, closing the loop with primary care, and providing incentives for pharmacies to offer these services.
Other Examples of “Pairing” and “Community-Based” Strategies
• Mammo/FIT (Grace Hillyer, New York City mammography suites)
• Mammo/Colo (Ruth Carlos, Ann Arbor VAMC mammography suites)
• Flu/Mammo (Doug Shenson, SPARC/community-based flu shot clinics)
• Vote & Vax Programs (Doug Shenson, SPARC, polling places)
• Pharmacies and FIT (Australian National Program)
Conclusions
• FLU-FOBT and FLU-FIT Programs
– Complement other efforts to increase CRCS in diverse settings and populations
– Can be implemented successfully in many different forms
– Work best when introduced with effective leadership and training, coupled with follow-up reminders and navigation of abnormal results
Acknowledgments
• Mentors, Co-Investigators, Consultants, Collaborators and Project Coordinators (partial list)
– Judith Walsh, Stephen McPhee, Estie Hudes, Tina Yu, Albert Yu, Ginny Gildengorin, Carol Somkin, Vicky Gomez, Teresa Dao, TR Levin, Lynn Ackerson, Lisa Kroon, Sean Haughtaling, Jim Allison, Larry Green, Russ Glasgow
• Funders– ACS, CDC, HMO-CRN (NCI), AANCART (NCI and CDC),
the Alexander and Margaret Stewart Trust, and the San Francisco Bay Area Collaborative Research Network (UCSF CTSI)
• Community-Based Participants– Leaders, Clinicians, and Clinic Staff at SFDPH Community
Health Network, Kaiser Permanente Northern California, and Walgreens Pharmacies
Thank You!
http://flufit.org – includes videos, downloadable implementation materials, and our research papers





![[PPT]PENYAKIT FLU BURUNG - Keluarga IKMA FKMUA … · Web viewPENYAKIT FLU BURUNG * * * * * * * * * * * * * * * * * * * EPIDEMIOLOGI Penyebab FLU BURUNG FLU burung atau flu unggas](https://static.cupdf.com/doc/110x72/5ae835287f8b9a8b2b8facf5/pptpenyakit-flu-burung-keluarga-ikma-fkmua-viewpenyakit-flu-burung-.jpg)























