Enhancing Patient Identification for Point of Care Glucose Testing in
the Clinic Setting
• Executive Sponsor: David Mountjoy, Associate Director Practice Mgmt
• Advisors: – Laura Burnett, Manager of Outpatient Services – Sue Scott, RN, MSN Patient Safety Coordinator
• Team: – Cindy Roller, MLT Point of Care Testing– Shelly Jackman, RN Nurse Supervisor
• Support: – Jeanne Harmon, RN Nurse Supervisor
Performance Improvement Leadership Development Program
February 19, 2010
AIM STATEMENT
Develop an electronic process for entering patient information into Point of Care (POC) glucose meter (Roche Accu-Chek Inform) to increase
operator accuracy and satisfaction by 50% on or before Jan 31, 2010.
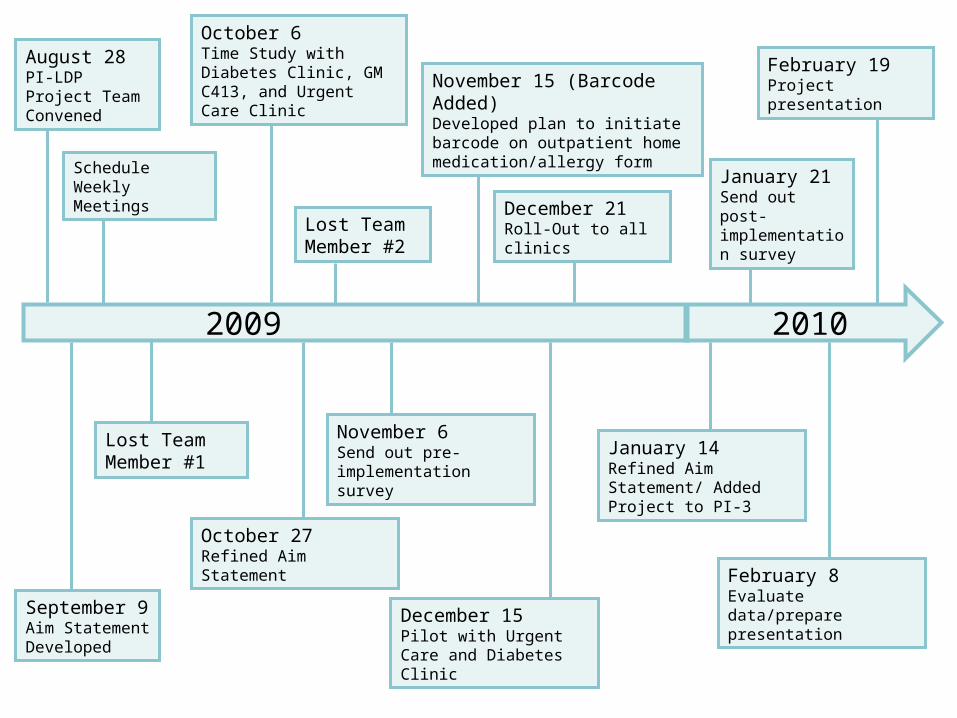
2009 2010
August 28PI-LDP Project Team Convened
September 9Aim Statement Developed
Schedule Weekly Meetings
Lost Team Member #1
October 6Time Study with Diabetes Clinic, GM C413, and Urgent Care Clinic
October 27Refined Aim Statement
Lost Team Member #2
November 6Send out pre-implementation survey
November 15 (Barcode Added)Developed plan to initiate barcode on outpatient home medication/allergy form
December 15Pilot with Urgent Care and Diabetes Clinic
December 21Roll-Out to all clinics
January 14Refined Aim Statement/ Added Project to PI-3
January 21Send out post- implementation survey
February 8Evaluate data/prepare presentation
February 19Project presentation

Goal for University Physicians Clinics
• Improve patient safety in accordance with National Patient Safety Goals
• Increase operator accuracy and satisfaction
• Service = Improve turn around time
• People = Increase patient safety and increase staff satisfaction
• Financial = Streamline workload
• Quality = Deliver accurate and timely patient results
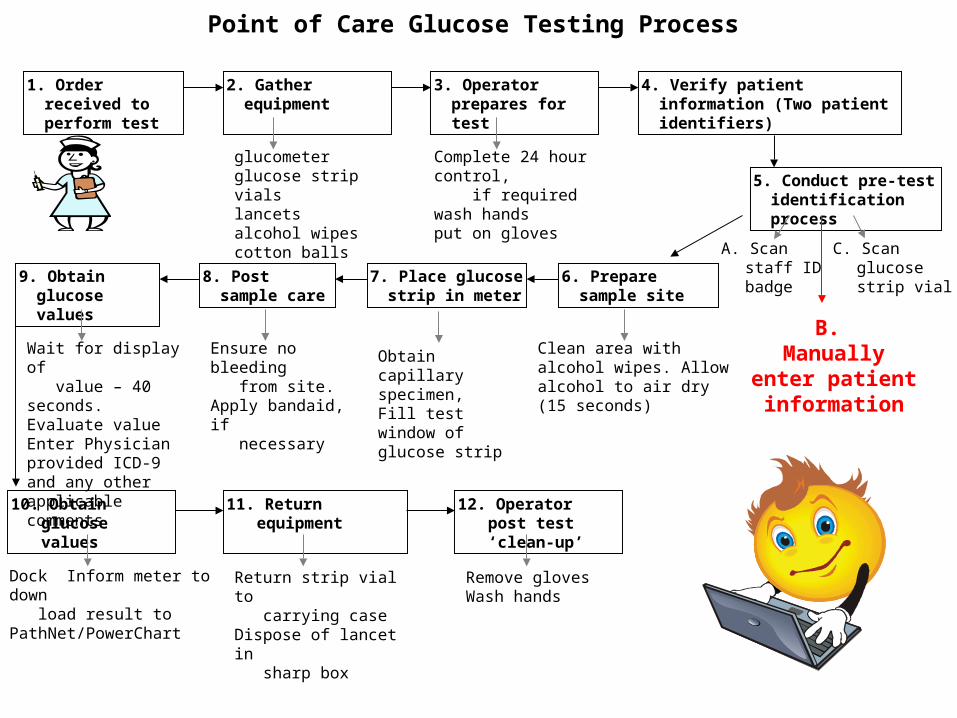
Point of Care Glucose Testing Process
1. Order received to perform test
2. Gather equipment 3. Operator prepares for test
4. Verify patient information (Two patient identifiers)
glucometerglucose strip vialslancetsalcohol wipescotton balls
Complete 24 hour control, if requiredwash handsput on gloves
5. Conduct pre-test identification process
6. Prepare sample site
7. Place glucose strip in meter
8. Post sample care
B. Manually enter
patient information
A. Scan staff ID badge
C. Scan glucose strip vial9. Obtain glucose
values
Clean area with alcohol wipes. Allow alcohol to air dry (15 seconds)
Ensure no bleeding from site. Apply bandaid, if necessary
Wait for display of value – 40 seconds.Evaluate valueEnter Physician provided ICD-9 and any other applicable comments
10. Obtain glucose values
11. Return equipment 12. Operator post test ‘clean-up’
Dock Inform meter to down load result to PathNet/PowerChart
Return strip vial to carrying caseDispose of lancet in sharp box
Remove glovesWash hands
Obtain capillary specimen, Fill test window of glucose strip
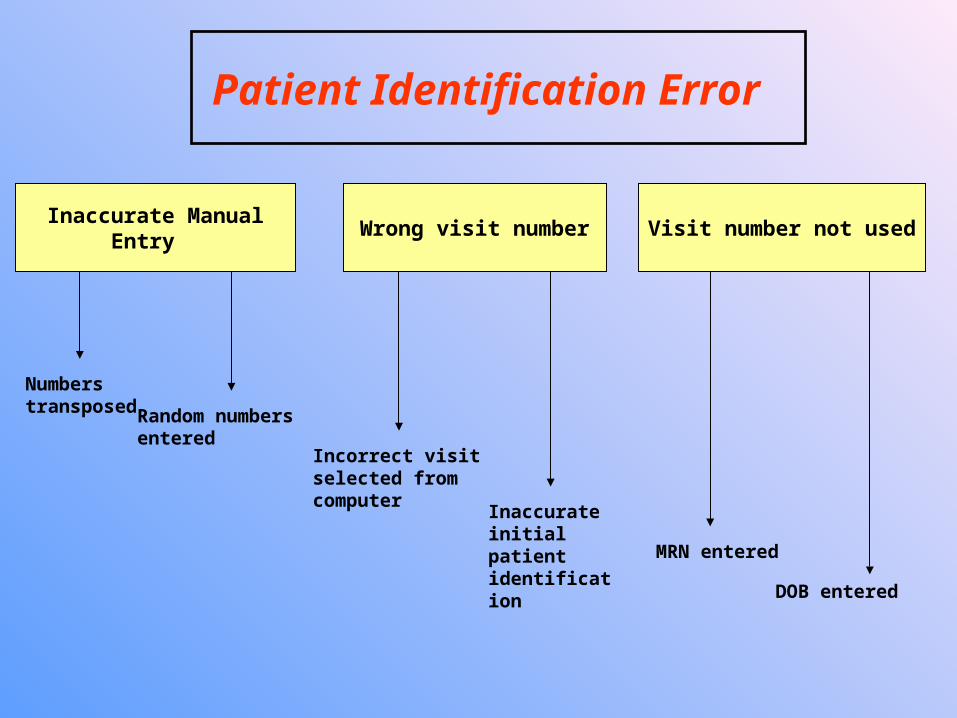
Patient Identification Error
Visit number not usedInaccurate Manual
Entry Wrong visit number
Numbers transposed Random numbers
entered Incorrect visit selected from computer
Inaccurate initial patient identification MRN entered
DOB entered
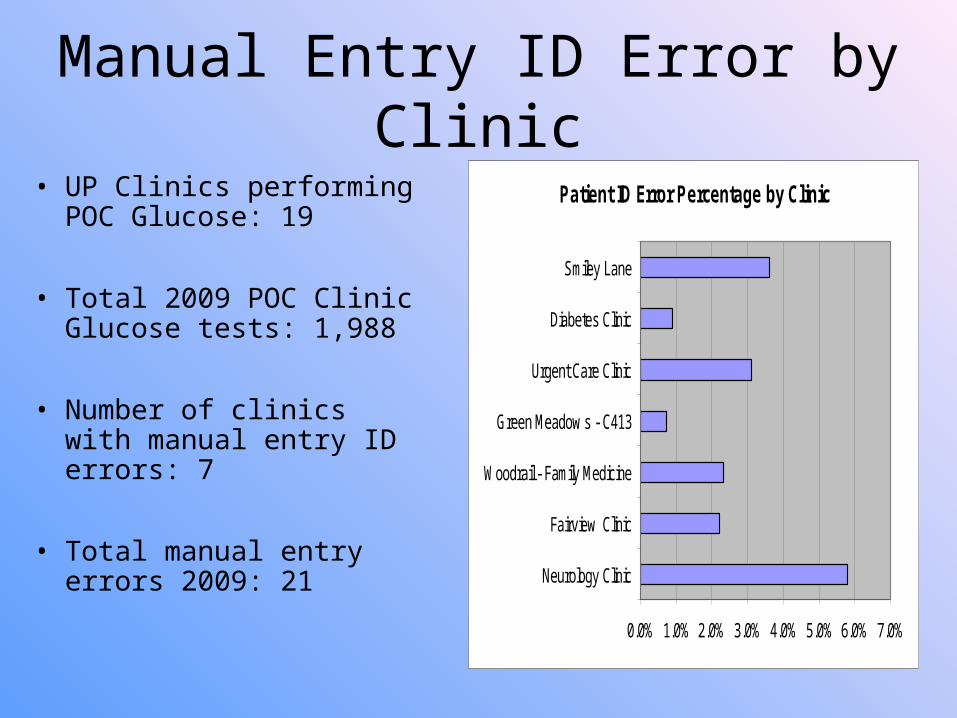
Manual Entry ID Error by Clinic
• UP Clinics performing POC Glucose: 19
• Total 2009 POC Clinic Glucose tests: 1,988
• Number of clinics with manual entry ID errors: 7
• Total manual entry errors 2009: 21
Patient ID Error Percentage by Clinic
0.0% 1.0% 2.0% 3.0% 4.0% 5.0% 6.0% 7.0%
Neurology Clinic
Fairview Clinic
Woodrail - Family Medicine
Green Meadow s - C413
Urgent Care Clinic
Diabetes Clinic
Smiley Lane
Pre-Implementation Staff Survey Results
Results: 56/138 (41% return) 57.2% very satisfied/satisfied with ease of entering patient
identification into Inform glucose meter 42.8% neither satisfied/dissatisfied/very dissatisfied 55.4% perceived time to perform test was 2-3 minutes At the time of the survey, 23.2% reported scanning (work-around
already in place)
Comments: “It would be less time consuming to scan a barcode rather than
entering a visit number, I also think this would cut down errors in entering patient info.”
“Would be nice and quicker to get to the testing if we had a barcode with patient information.”

We know what the problem is, now how do we fix it?
• Meet with clinic staff to determine current procedures and possible alternatives
• Barcode scanning would be great – but what should we scan? Different clinics had different options
• Several clinics had already established “work-arounds”
• Work with IT to create a barcode for the medication/allergy form that all clinics were able to print for each patient – this will enable us to standardize the procedure

We know what the problem is, now how do we fix it?
• Change to policy and procedure
• Education and training must be adapted to meet the new standards
• Managers and trainers were notified of the change and encouraged to update all staff
• Emergency “Unregistered Patient” barcode available to scan
Post-Implementation Staff Survey Results
Results: 57/138 Responses (41%) 78.2% very satisfied/satisfied with ease of entering patient
identification into the meter (up from 52.7%) 21.7% neither satisfied/dissatisfied/very dissatisfied (down from
42.8%) 60.9% reported time <1 minute (up from 28.6%)
Comments: “Awesome Change!” “I hated doing the manual entry of patient information –
transcribing errors were a problem. Love the new way with the bar coding. THANK YOU!!!!!!!”
“Love the bar code on the med sheet, it does save a few seconds and that is important - seems very accurate and it worked well”
“So much more convenient!”

Outcomes Increased patient safety / Decreased error rate
• No patient ID errors post implementation when using barcode scanning• Two manual entry errors post implementation
• Operator manually entered another patient’s visit number• Operator manually entered patient’s medical record number
Decreased “Work-Arounds”• Scanning patient labels/stickers
Standardized process• New CED module• New training/orientation• Policy updates
Increased staff satisfaction• Shortened overall time to perform test• Staff confidence in accuracy• Limit # of PSN reports• Limit lab staff interventions

Lessons Learned/Future Plans• Smiley Clinic does not print the Medication/Allergy form
– how do we accommodate them?
• Turn off manual access – allow barcode scanning only
• Ongoing monitoring for compliance and operator satisfaction
• PI-LDP project could have been more efficient with additional team members

Barriers
• Multiple processes in place
• Staff Education
• Staff Compliance
• Sustaining PI-LDP Team
Questions?