




David F. Dinges, Ph.D.Professor and Chief
Division of Sleep & ChronobiologyUniversity of Pennsylvania School of Medicine
Philadelphia, Pennsylvania
Caffeine and cognitive performance with and without sleep deprivation
NIDA-ODS SymposiumCaffeine: Is the Next Problem Already Brewing?
Neuroscience CenterRockville, Maryland
July 7 - 8, 2009
Penn
Founded by Benjamin Franklin America’s 1st secular University (1749) America’s First Medical School (1765)

Modern humans are the only species that light the night
Philadelphia
Coffee (and caffeine in general) is the most widely used stimulant in the world—and use is continuing to increase
• Caffeine binds at adenosine receptors throughout the brain.
• Coffee is 2nd most traded commodity (oil is #1).
• US imports more coffee than any other country.
• 108 million coffee consumers in the US.
• $9 billion spent on coffee per year.
• Average person consumes 3.3 cups/day.
• 54% of adults are regular coffee drinkers.
• 18% drink gourmet coffee beverages daily, which have more caffeine.
• Wall Street Journal found that coffee house chains (e.g., Starbucks) have house blends that contain 29%-56% more caffeine than those at food stores.
Source: Coffee Research Institute, 2001

The continuity, intensity and duration of sleep contain the “recovery” that re-establishes stable waking cognitive functions:
Sleepiness increases when as these aspects are denied.
During sleep—especially the most intense sleep (EEG slow waves)—the brain is
dynamically reorganizing. Forced awakenings at these times reveal an inability of the brain to use its waking cognitive functions such as
working memory
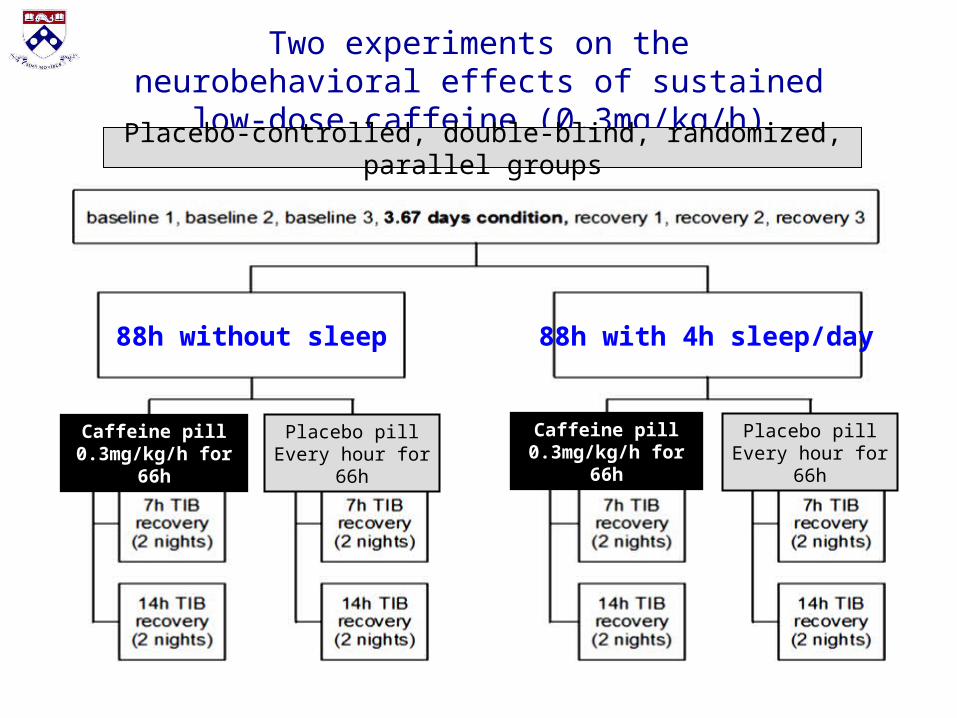
Two experiments on the neurobehavioral effects of sustained low-dose caffeine (0.3mg/kg/h)
Caffeine pill 0.3mg/kg/h for 66h
Placebo pillEvery hour for 66h
Placebo pillEvery hour for 66h
Caffeine pill 0.3mg/kg/h for 66h
88h without sleep 88h with 4h sleep/day
Placebo-controlled, double-blind, randomized, parallel groups
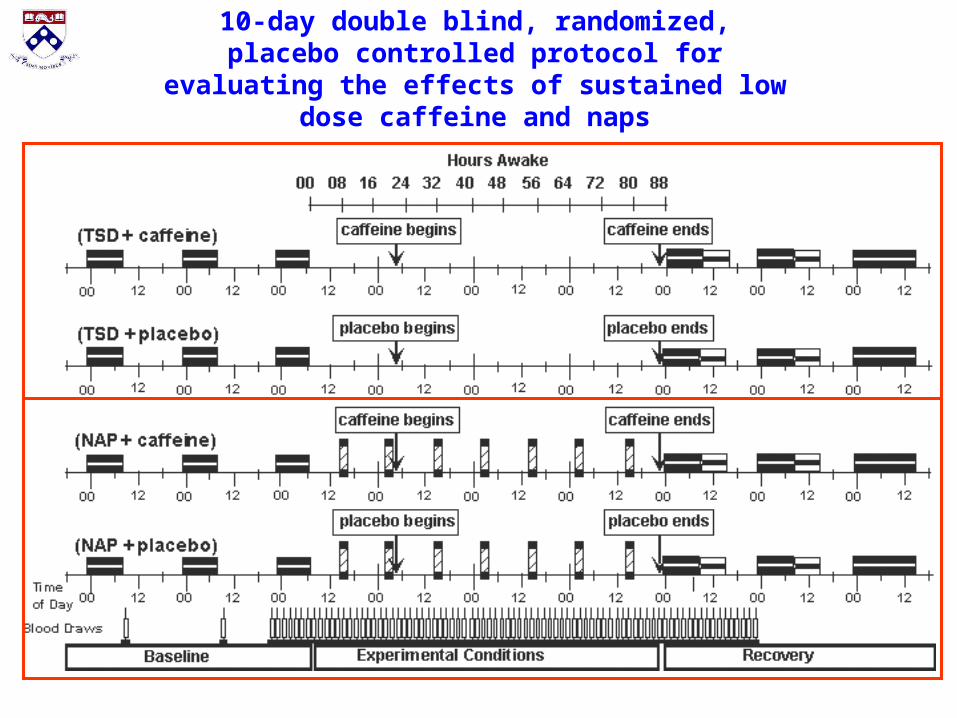
10-day double blind, randomized, placebo controlled protocol for evaluating the effects of
sustained low dose caffeine and naps
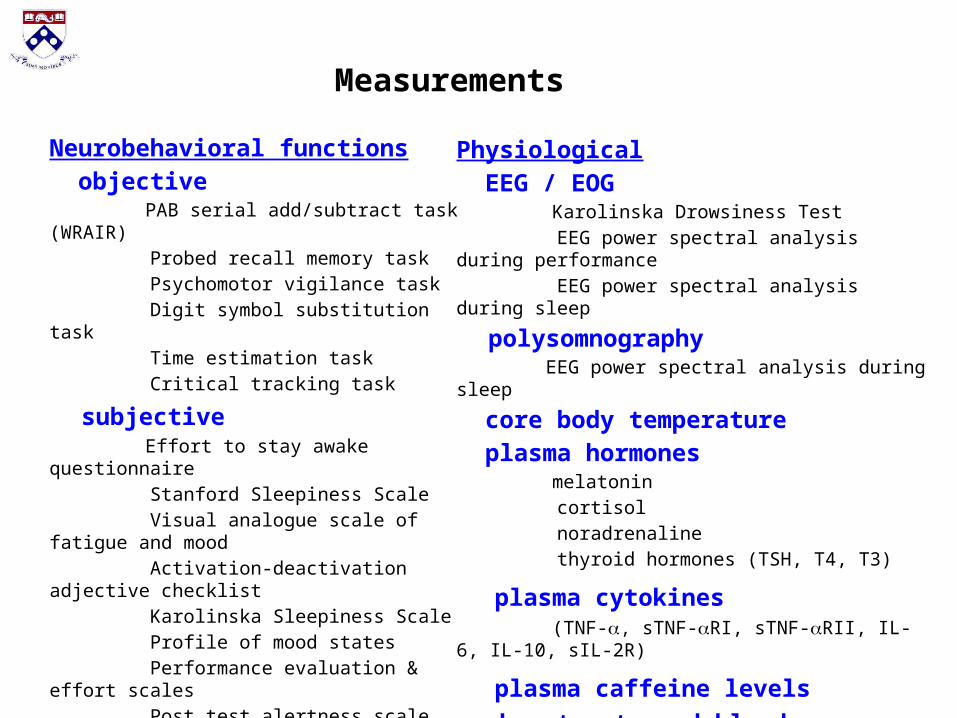
Neurobehavioral functions objective PAB serial add/subtract task (WRAIR) Probed recall memory task Psychomotor vigilance task Digit symbol substitution task Time estimation task Critical tracking task
subjective Effort to stay awake questionnaire Stanford Sleepiness Scale Visual analogue scale of fatigue and mood Activation-deactivation adjective checklist Karolinska Sleepiness Scale Profile of mood states Performance evaluation & effort scales Post test alertness scale
actigraphy sleep-wake log
Physiological EEG / EOG Karolinska Drowsiness Test EEG power spectral analysis during performance EEG power spectral analysis during sleep
polysomnography EEG power spectral analysis during sleep
core body temperature plasma hormones melatonin cortisol noradrenaline thyroid hormones (TSH, T4, T3)
plasma cytokines (TNF-, sTNF-RI, sTNF-RII, IL-6, IL-10, sIL-2R)
plasma caffeine levels
heart rate and blood pressure
Measurements
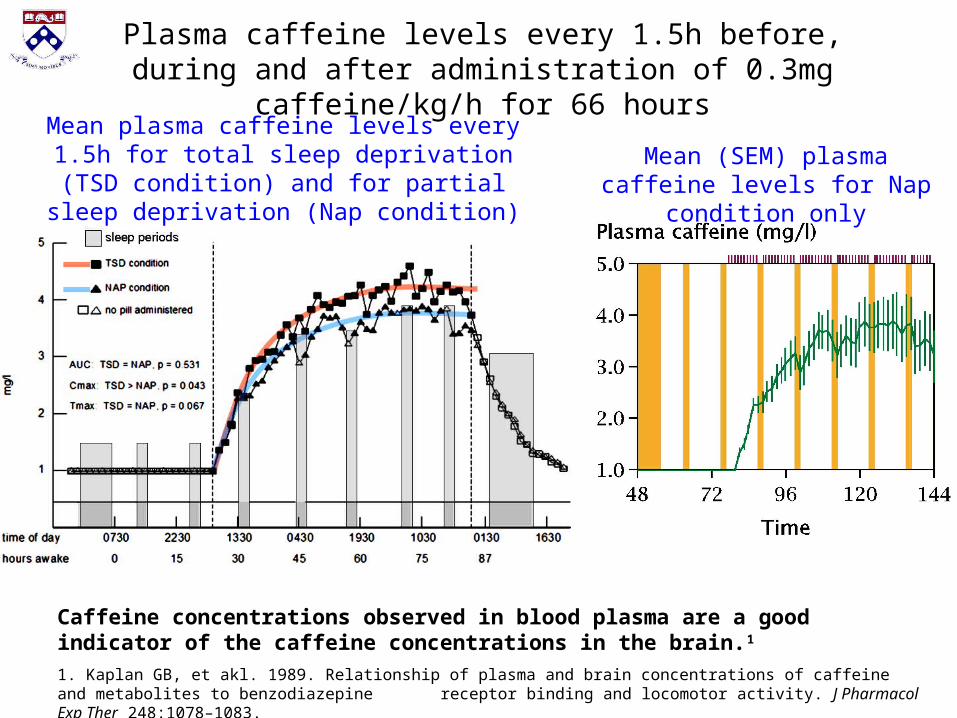
Mean plasma caffeine levels every 1.5h for total sleep deprivation (TSD condition) and for
partial sleep deprivation (Nap condition)Mean (SEM) plasma caffeine levels for Nap condition only
Plasma caffeine levels every 1.5h before, during and after administration of 0.3mg caffeine/kg/h for 66 hours
Caffeine concentrations observed in blood plasma are a good indicator of the caffeine concentrations in the brain.1
1. Kaplan GB, et akl. 1989. Relationship of plasma and brain concentrations of caffeine and metabolites to benzodiazepine receptor binding and locomotor activity. J Pharmacol Exp Ther 248:1078–1083.
Subjects’ perceptions of whether they received low-dose caffeine (0.3mg/kg/h) or placebo were inaccurate
Placebo condition: t12 = −0.599, p = 0.56
Caffeine condition: t14 = −1.480, p = 0.16
No difference between conditions (t26 = 0.259, p = 0.80).
• Subjects ingested pills every hour for 66h beginning 22h after the end of the final baseline night of sleep.
• Subjects were informed that the pill ingested could be caffeine or placebo and could vary at any hour.
• In fact the pill was always (100% of the time) either low-dose caffeine or placebo, depending on randomization.
• When they received a pill that were asked to check off whether the pill they received an hour earlier was placebo or caffeine.
• Their ability to determine what pill they received was not reliably better than chance.

condition ntotal # SAs
subjects with>1 SA (%)
# perf bouts with >1 SA
time to 1st SA
time of 1st SA
placebo + no naps 14 173 8 (57%) 29 23 hr 06:00
caffeine + no naps 12 59 5 (42%) 16 23 hr 06:00
placebo + naps 13 3 2 (15%) 3 72 hr 08:00
caffeine + naps 15 3 2 (13%) 2 50 hr 10:00
Sleep attacks (SA) during performance across 88h vigilSA = 30-sec of nonresponding to stimulus, followed by an alarm

Performancevariable
Caffeine effect(0.3 mg/kg/h)
Naps effect(2h nap/12h)
Naps interaction with caffeine
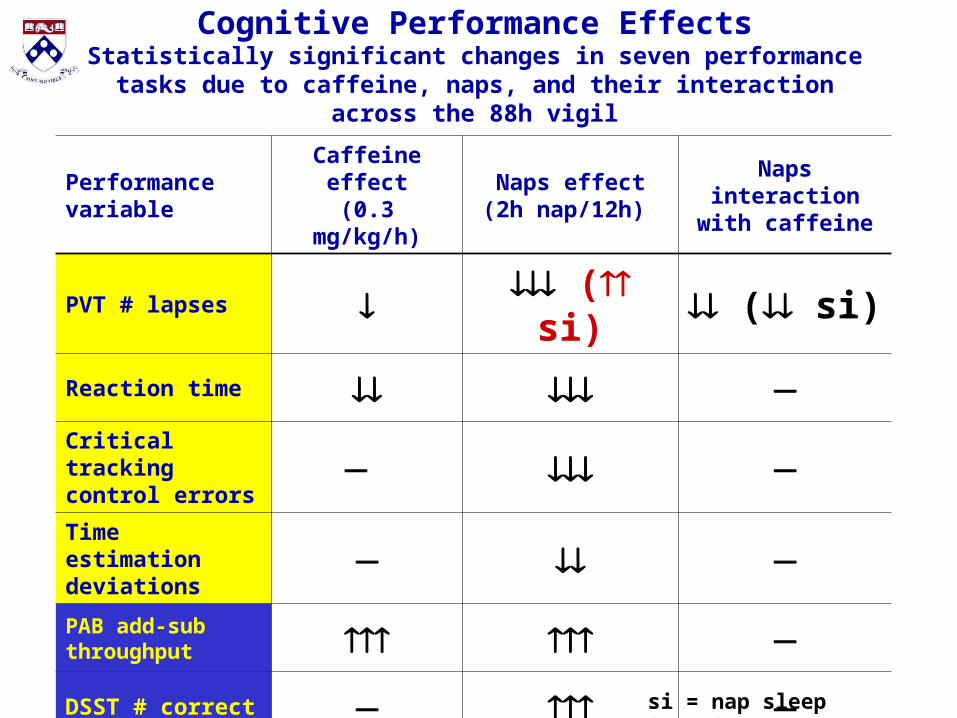
PVT # lapses ( si) ( si)
Reaction time Critical trackingcontrol errors Time estimationdeviations PAB add-sub throughput
DSST # correct Probed recall memory perfor.
Cognitive Performance EffectsStatistically significant changes in seven performance tasks due to
caffeine, naps, and their interaction across the 88h vigil
si = nap sleep inertia

Sustained low-dose caffeine without naps kept PVT lapses of attention lower than placebo
Better
performance
Mea
n P
VT
lap
ses
per
tes
t tr
ial

Naps combined with sustained low-dose caffeine reduced lapses of attention as measured by Psychomotor
Vigilance Test (PVT) performance: Caffeine particularly benefited immediate post-nap performance
Better
performance
Mea
n P
VT
lap
ses
per
tes
t tr
ial

Van Dongen et al. SLEEP 24 (7):813-819, 2001.
Effects of sustained low-dose caffeine on sleep inertia during chronic partial sleep deprivation (2h sleep every 12h for 66h)
Caffeine reduced PVT lapses of attention during post-nap sleep inertia
Caffeine had no effect on subjective sleepiness during post-nap sleep inertia
Caffeine (1,3,7-trimethylxanthine) and its major metabolite2 paraxanthine (1,7-dimethylxanthine) are known to antagonize adenosine receptors in the brain.1 This is caffeine’s main mechanism of action on the CNS.2
1 Radulovacki M, et al. Brain Res (1982). 2 Daly JW, et al. Current views and research trends. (1999).
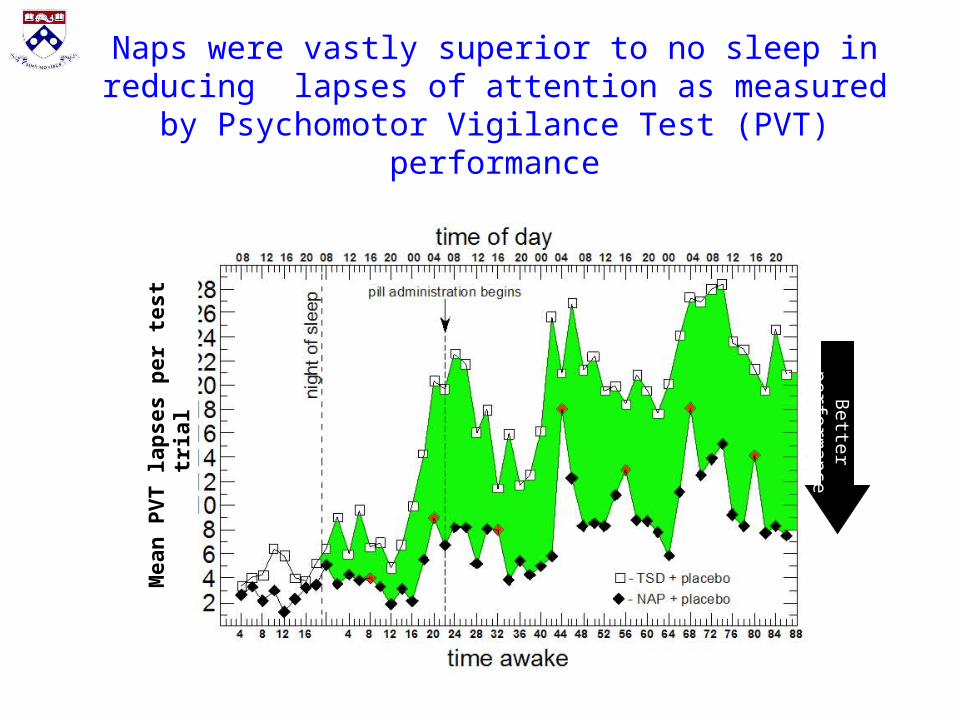
Naps were vastly superior to no sleep in reducing lapses of attention as measured by Psychomotor
Vigilance Test (PVT) performanceM
ean
PV
T la
pse
s p
er t
est
tria
l
Better
performance
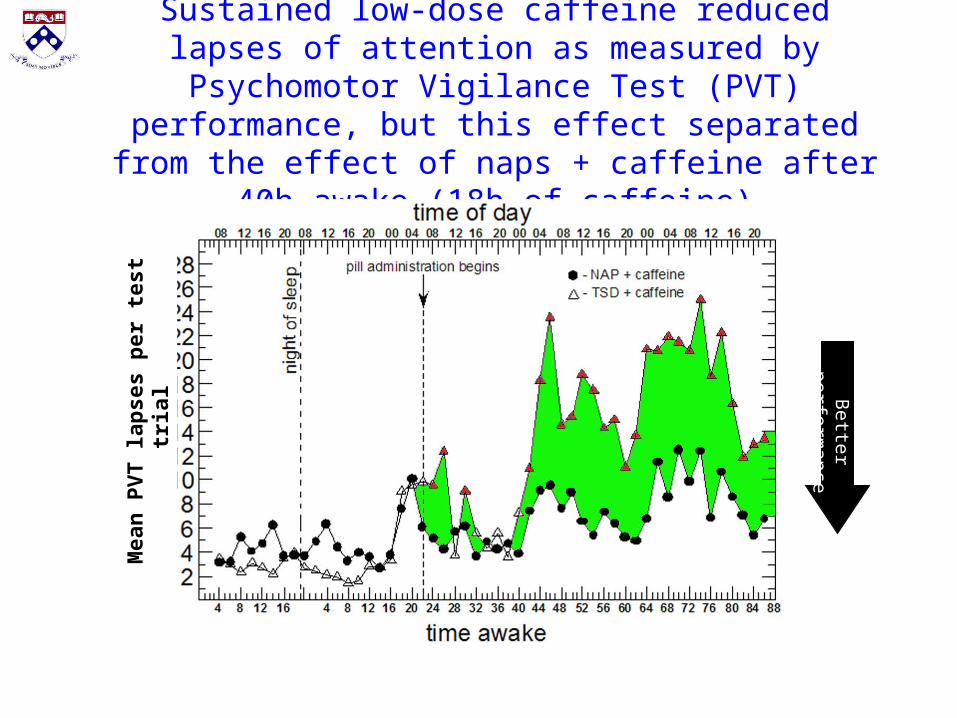
Sustained low-dose caffeine reduced lapses of attention as measured by Psychomotor Vigilance Test (PVT)
performance, but this effect separated from the effect of naps + caffeine after 40h awake (18h of caffeine)
Better
performance
Mea
n P
VT
lap
ses
per
tes
t tr
ial
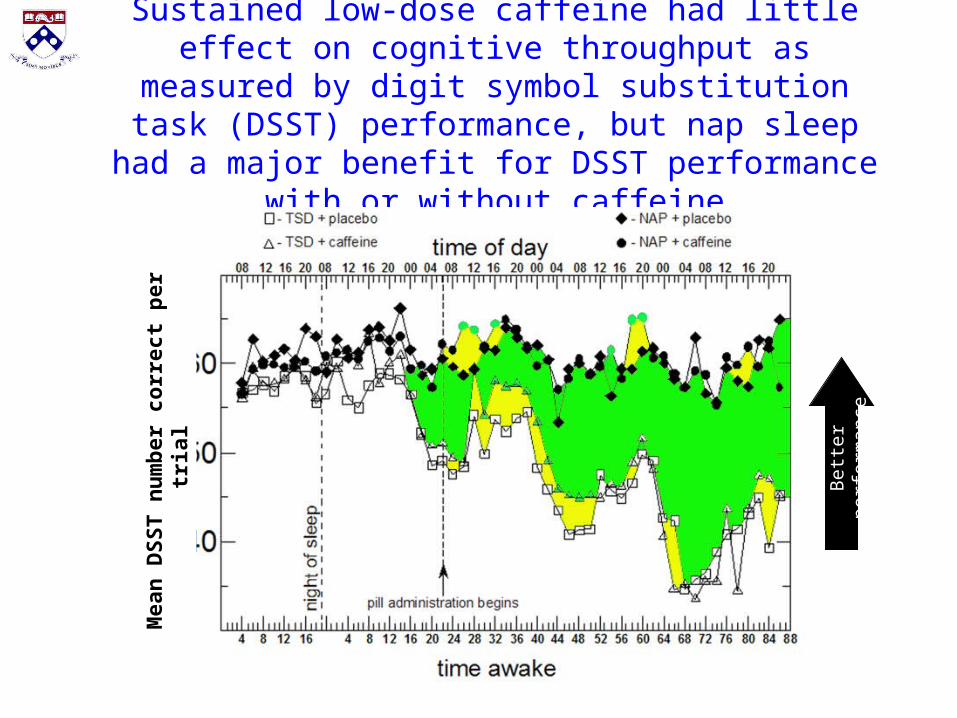
Sustained low-dose caffeine had little effect on cognitive throughput as measured by digit symbol substitution task (DSST) performance, but nap sleep had a major benefit for DSST performance with or without caffeine
Bet
ter
perf
orm
ance
Mea
n D
SS
T n
um
ber
co
rrec
t p
er t
rial

Effects of caffeine vs placebo in total sleep loss condition
hours awake
Hourly pill administration commences
Performancevariable
Caffeine effect(0.3 mg/kg/h)
Naps effect(2h nap/12h)
Naps interaction with caffeine
PVT # lapses ( si) ( si)
Reaction time Critical trackingcontrol errors Time estimationdeviations PAB add-sub throughput
DSST # correct Probed recall memory perfor.
Cognitive Performance EffectsStatistically significant changes in seven performance tasks due to
caffeine, naps, and their interaction across the 88h vigil
si = nap sleep inertia
Scale / ratingvariable
Caffeine effect(0.3 mg/kg/h)
Naps effect(2h nap/12h)
Naps interaction with caffeine
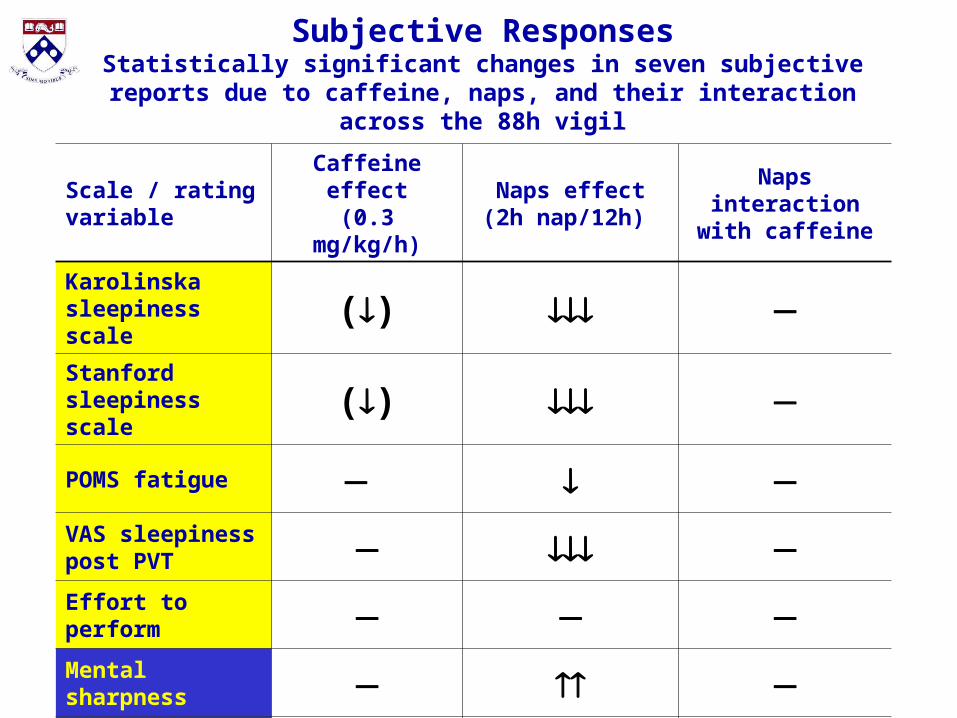
Karolinska sleepiness scale () Stanford sleepiness scale ()
POMS fatigue VAS sleepiness post PVT
Effort to perform
Mental sharpness
POMS vigor
Subjective ResponsesStatistically significant changes in seven subjective reports due to
caffeine, naps, and their interaction across the 88h vigil
Sle
epi
er
Mea
n K
SS
sle
epin
ess
rati
ng
per
tri
al
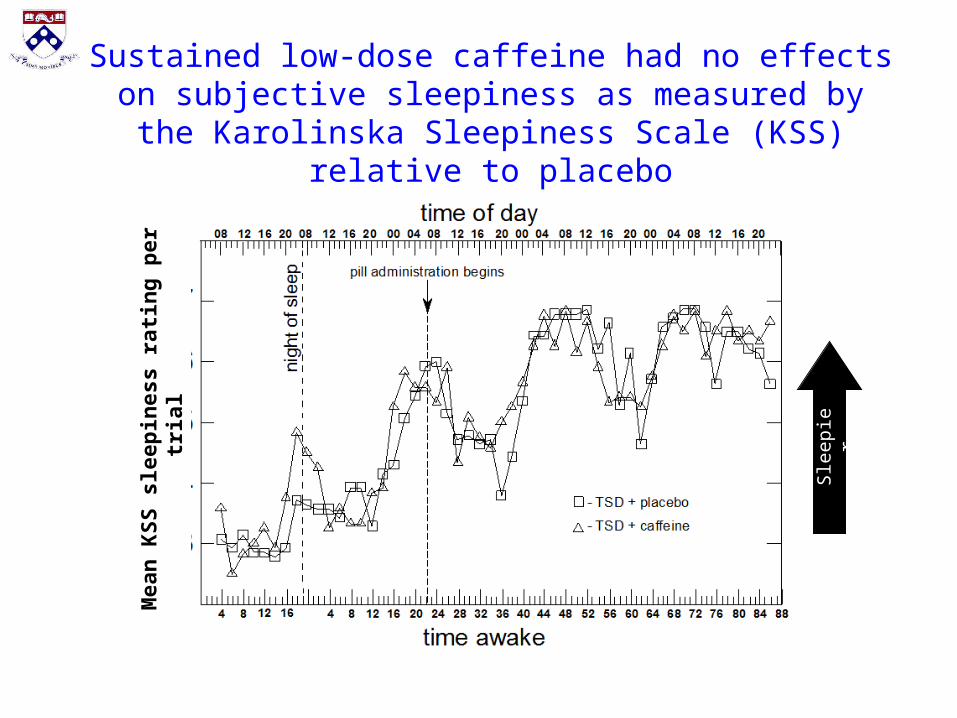
Sustained low-dose caffeine had no effects on subjective sleepiness as measured by the Karolinska Sleepiness
Scale (KSS) relative to placebo
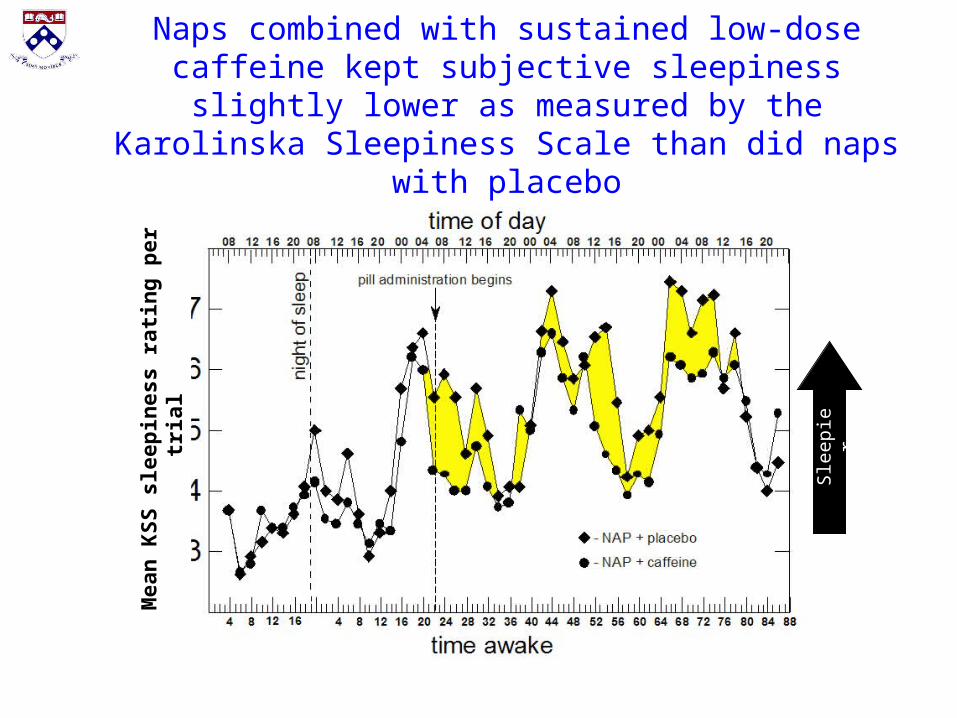
Naps combined with sustained low-dose caffeine kept subjective sleepiness slightly lower as measured by the Karolinska Sleepiness Scale than did naps with placeboM
ean
KS
S s
leep
ines
s ra
tin
g p
er t
rial
Sle
epi
er

Naps combined with sustained low-dose caffeine kept subjective sleepiness as measured by Karolinska Sleepiness
Scale (KSS) lower than did caffeine without naps
Sle
epi
er
Mea
n K
SS
sle
epin
ess
rati
ng
per
tri
al
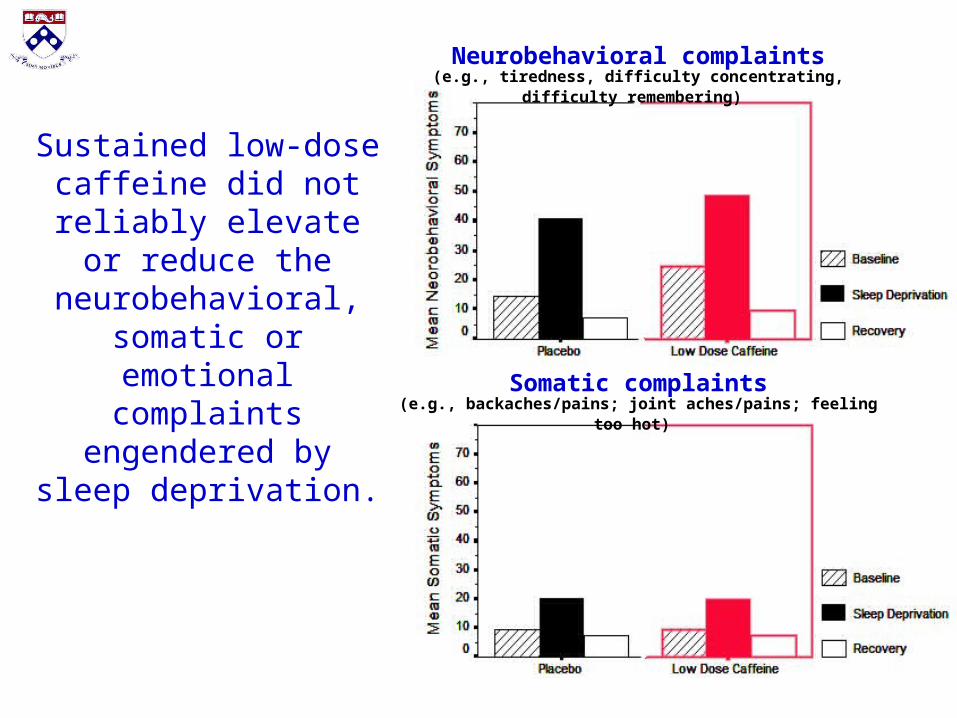
Sustained low-dose caffeine did not reliably elevate or reduce the
neurobehavioral, somatic or emotional
complaints engendered by sleep deprivation.
Neurobehavioral complaints(e.g., tiredness, difficulty concentrating, difficulty remembering)
Somatic complaints(e.g., backaches/pains; joint aches/pains; feeling too hot)

Scale / ratingvariable
Caffeine effect(0.3 mg/kg/h)
Naps effect(2h nap/12h)
Naps interaction with caffeine
Heart rate
Blood pressure
Plasma cortisol (si)
Plasma noradrenaline
Plasma melatonin Plasma cytokines(e.g., IL-6, sTNFα-RI)
Body temperature si = nap sleep inertia
Physiological EffectsStatistically significant changes in seven physiological measures due
to caffeine, naps, and their interaction across the 88h vigil
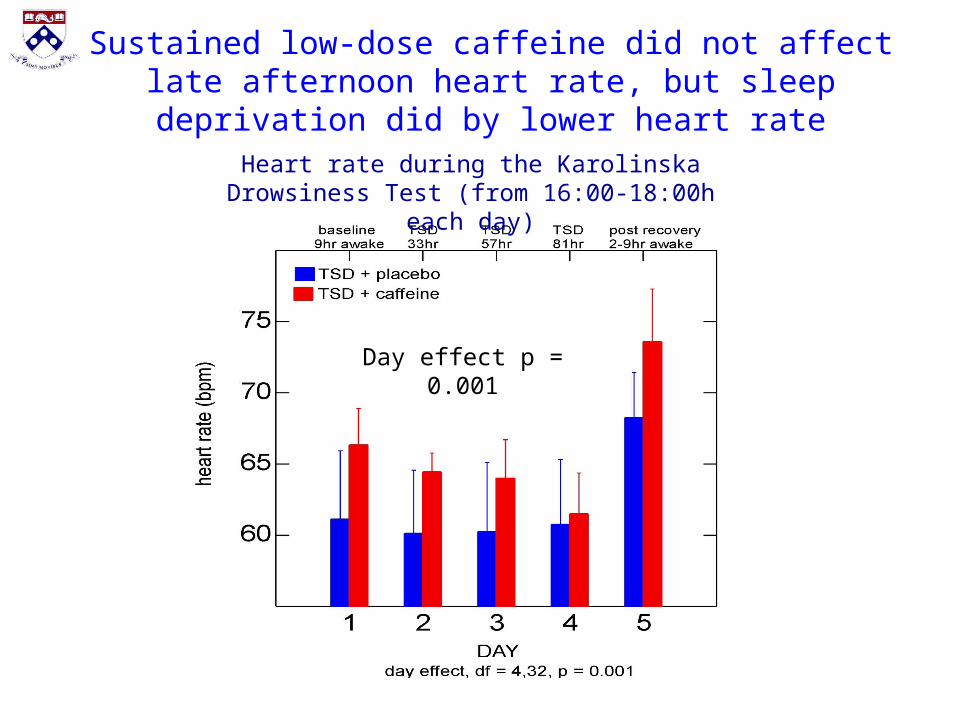
Heart rate during the Karolinska Drowsiness Test (from 16:00-18:00h each day)
Day effect p = 0.001
Sustained low-dose caffeine did not affect late afternoon heart rate, but sleep deprivation did by lower heart rate
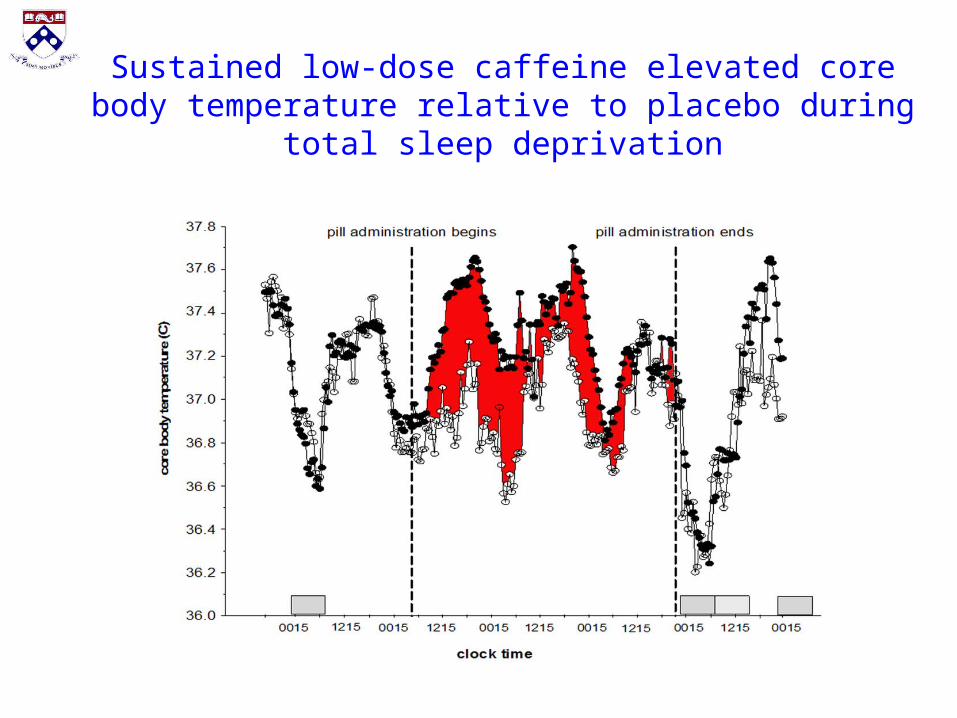
Sustained low-dose caffeine elevated core body temperature relative to placebo during total sleep deprivation
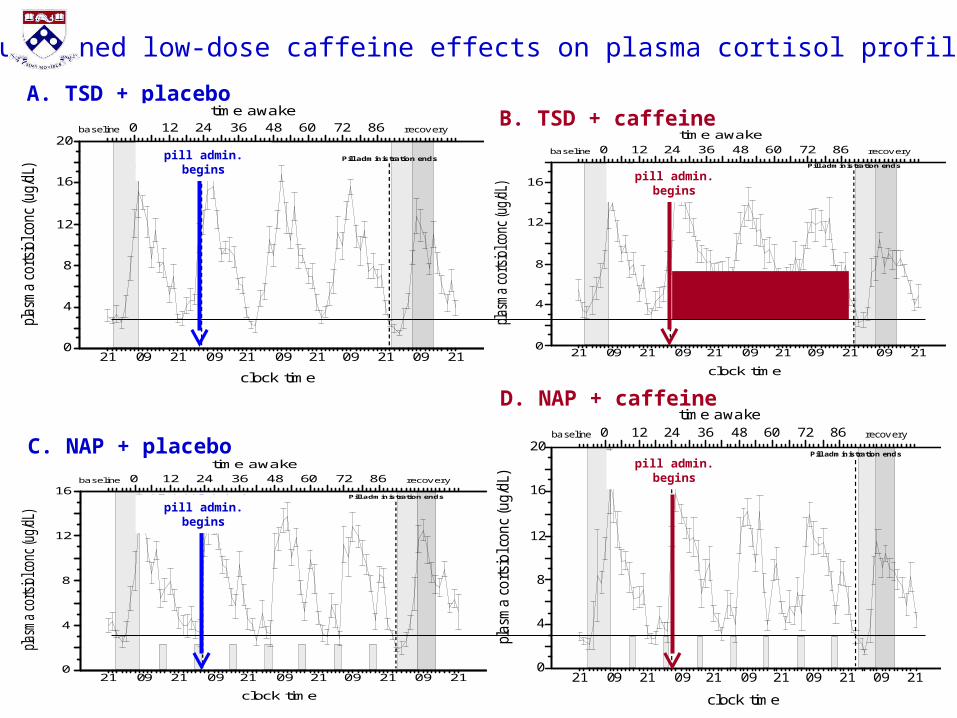
Sustained low-dose caffeine effects on plasma cortisol profiles
A. TSD + placeboB. TSD + caffeine
D. NAP + caffeine
C. NAP + placebo
20
16
12
8
4
0
plasm
aco
rtsi
olc
onc
(ug/d
L)
21 090921 21 2109 2109 2109
clock time
0 12 24 36 48 60 72 86time awake
recoverybaseline
Pill administration begins Pill administration ends
21 090921 21 2109 2109 2109
clock time
0 12 24 36 48 60 72 86time awake
recoverybaseline
12
16
0
4
8
Pill administration begins Pill administration ends
21 090921 21 2109 2109 2109
clock time
0 12 24 36 48 60 72 86time awake
recoverybaseline
16
12
8
4
0
Pill administration begins Pill administration ends
20
16
12
8
4
0
plasm
aco
rtsi
olc
onc
(ug/d
L)
21 090921 21 2109 2109 2109
clock time
0 12 24 36 48 60 72 86time awake
recov erybaseline
Pill administration begins Pill administration ends
Elevated cortisol in circadian nadir
pill admin. begins
pill admin. begins
pill admin. begins
pill admin. begins

Sustained low-dose caffeine elevated mean daily plasma noradrenaline levels during sleep
deprivation with and without naps

Relative to placebo, sustained low-dose caffeine affected nap sleep onset, sleep efficiency, total
sleep time, and SWS and REM sleep time
Effects of sustained low dose caffeine
• Neurobehavioral effects
– Vigilance attention was primarily affected (up to 48h), including blocking sleep inertia on awakening from naps
– Few effects on other cognitive tasks, but naps had large effects
– Subjective sleepiness was not affected
– Subjects were frequently not aware of receiving caffeine
• Nap sleep was disrupted by caffeine
• Plasma noradrenaline levels and cortisol levels were elevated
• Core body temperature was elevated by caffeine
• Neurobehavioral and somatic complaints were not elevated by caffeine
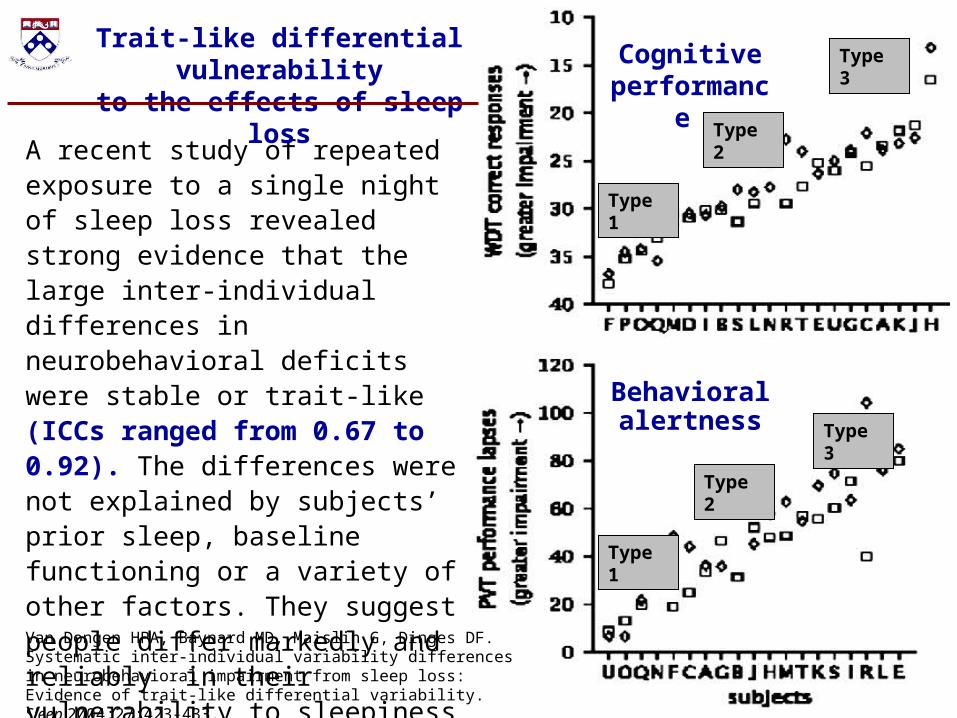
A recent study of repeated exposure to a single night of sleep loss revealed strong evidence that the large inter-individual differences in neurobehavioral deficits were stable or trait-like (ICCs ranged from 0.67 to 0.92). The differences were not explained by subjects’ prior sleep, baseline functioning or a variety of other factors. They suggest people differ markedly and reliably in their vulnerability to sleepiness and impairment from sleep deprivation.
Trait-like differential vulnerabilityto the effects of sleep loss
Cognitive performance
Behavioral alertness
Van Dongen HPA, Baynard MD, Maislin G, Dinges DF. Systematic inter-individual variability differences in neurobehavioral impairment from sleep loss: Evidence of trait-like differential variability. Sleep 2004;27:423-433.
Type 1
Type 2
Type 3
Type 1
Type 2
Type 3

Dose-response studies of sleep restriction reveal cumulative
increases in PVT lapses
Van Dongen et al. SLEEP (2003)
Belenky et al. J Sleep Res (2003)
40-64 hr TSD
24-40 hr TSD
TIB = sleep doseAB
But there are substantial individual differences in the response to sleep
restriction (Means ± SD)
PVT lapses in response to sleep restriction in healthy adults reveal large individual differences (some are very vulnerable to the effects of sleep loss and others less so)
4h TIB
8h TIB
6h TIB
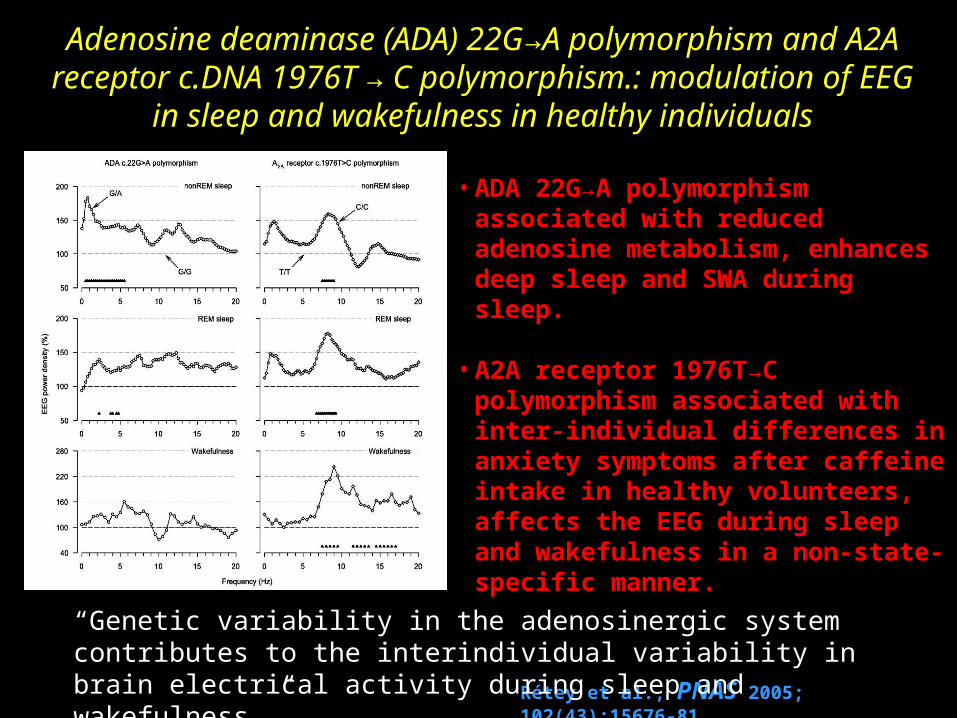
Adenosine deaminase (ADA) 22G→A polymorphism and A2A receptor c.DNA 1976T → C polymorphism.: modulation of EEG in
sleep and wakefulness in healthy individuals
• ADA 22G→A polymorphism associated with reduced adenosine metabolism, enhances deep sleep and SWA during sleep.
• A2A receptor 1976T→C polymorphism associated with inter-individual differences in anxiety symptoms after caffeine intake in healthy volunteers, affects the EEG during sleep and wakefulness in a non-state-specific manner.
Rétey et al., PNAS 2005; 102(43):15676-81
“Genetic variability in the adenosinergic system contributes to the interindividual variability in brain electrical activity during sleep and wakefulness.”

Genetic variation in sensitivity to caffeine (adenosine-binding drugs) appears to contribute substantially to the effects of
caffeine on sleep and waking in healthy individuals
Rétey et al., PNAS 2005; 102(43):15676-81
“Genetic variability in the adenosinergic system contributes to the interindividual variability in brain electrical activity during sleep and wakefulness.”
Sleep deprivation effects on PVT performance was counteracted by caffeine. Theta power in waking increased more in a frontal EEG derivation than in a posterior derivation. Caffeine attenuated this power gradient in caffeine sensitive subjects. Sleep loss also differently affected the power distribution <1 Hz in nonREM sleep between caffeine sensitive and insensitive subjects. This difference was mirrored by the action of caffeine. The effects of sleep deprivation and caffeine on sustained attention and regional EEG power in waking and sleep were inversely related. These findings suggest that adenosinergic mechanisms contribute to individual differences in waking-induced impairment of neurobehavioral performance and functional aspects of EEG topography associated with sleep deprivation. Rétey et al., J Neuroscience 2006;
26(41):10472-79
Research supported by AFOSR F49620-95-1-0388 and by NIH RR00040
“No thanks. I’m fine.
c





























