CTG MasterclassAVMA Annual Clinical
Negligence Conference 2012
Professor Tim Draycott, Consultant ObstetricianHealth Foundation Improvement Science Fellow

Birth care not always easy

Introduction
• Cerebral Palsy – Pattern of injury– Relationship with low Apgar score
• Standard of care– Intermittent Auscultation– Electronic Fetal Monitoring
• Interpretation• Action required
• Cases

Low Apgars and CP
• Base Excess ≤12 likely to be normal• Apgar score <7
– Odds ratio for CP after low (<7) Apgar scores at 5 minutes in tern infants is 3.72
– Proportion of CP in the population that could be attributed to a low Apgar score (<7) at 5 minutes is 10.9%
– At least 50% of Low Apgar scores could be prevented with better care

Recurring Themes
• Failure to perform EFM• Failure to recognise CTG
abnormalities• Failure to respond to CTG
abnormalities:• Fetal blood sampling• Expedite delivery

Cerebral Palsy
Proportion CP
Spastic Diplegic 26%Hemiplegic 35%Ataxic 4%Athetoid (Dyskinetic)
7-15%
Spastic Tetraplegic 18-20%

..and Clinical Negligence
Proportion CP
Intrapartum
Spastic Diplegic 26% <1%
Hemiplegic 35% 0%
Ataxic 4% 0%
Athetoid (Dyskinetic)
7-15% 80%
Spastic Tetraplegic
18-20% 45% +

Clinical Negligence
• Standard of care• Breach in duty of care
– Midwives– Obstetricians– Paediatricians
• Did that breach cause the injury ?

Causation
• Athetoid Dyskinetic Cerebral Palsy– Acute profound hypoxia
• Spastic Tetraplegic Cerebral Palsy– Chronic partial ischaemia

Athetoid CP
• Profound acute hypoxia - ‘lack of oxygen’– Uterine Rupture
– VBAC
– Cord Prolapse– Abruption

Hypoxia
• Oxygen sensitive parts of body– Kidneys– Heart– Brain

MRI findings
• Areas of brain with high metabolic rate– Deep grey matter
• Posterior parts of lentiform nuclei• Ventro-lateral nuclei of thalami• Hippocampus

MRI

Spastic Tetraplegic CP
• Mechanism of injury less established
• Prolonged period of mild – moderate hypotension– Cord Compression– Head Compression
• Watershed areas of brain

Chronic Partial Ischaemia• Low blood pressure in cerebral
arteries• Perfusion at peripheries
reduced• Lawn Sprinkler

MRI Findings

Intrapartum
• Monitoring fetal heart rate in labour– Intermittent Auscultation– Cardiotocograph
• Baseline rate• Baseline variability• Accelerations• Decelerations
• Introduction only

Intermittent Auscultation• Normal Labour
– The RCOG EFM guideline recommends:• In the active stages of labour, intermittent
auscultation (IA) should occur after a contraction, for a minimum of 60 seconds, and at least.
– every 15 minutes in the first stage – every 5 minutes in the second stage
• Failure to perform IA as above is substandard care

When to change to EFM ?

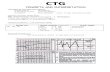
Cardio-tocography
• Abdominal palpation• Maternal pulse• Name/number/time/paper speed• Technically adequate • Documentation (actions & opinion) • Interpret in light of clinical setting

Reassuring CTG
• 4 Features: – Baseline rate
110-160– Baseline
variability - 5bpm or more
– Accelerations– No
decelerations

Intrapartum
• Standard of care– NICE EFM May 2001– NICE Intrapartum Guideline Sept 2007
– Pre 2001 – FIGO guidance published in 1987

NICE EFM

Coalface
Reassuring Non- reassuring AbnormalBaseline rate(bpm)
110 – 160 100 – 109161 - 180
<100>180
Comments:-
Variability(bpm)
5 bpm or more <5 for 40 mins ormore but <90 min
< 5 for 90 mins ormore
Comments:- CTG onfor 60 mins so far
Accelerations Present None Comments:-
Decelerations None EarlyVariableSingle prolongeddeceleration up to 3mins
Atypical variableLateSingle prolongeddeceleration > 3mins
Comments:-Unprovokeddecelerations
Opinion Normal CTG(All f our featuresreassuring)
Suspicious CTG(One non-reassuringfeature)
Pathological CTG(two or more non-reassuring or one ormore abnormal features)
Dilatation Not assessed Comments:- Not contracting Contractions ….:10Action Urgent transf er to tertiary unit and review by senior obstetrician
Date ……………………… Time………………… Signature………………………………………………. Status………………………….

Classification

Actions - Suspicious

Action - Pathological

NICE IP ‘Guide’line

New Sticker

Antenatal Sticker

Dr C BRAVADO
• Discuss risk• Contractions• Baseline Rate• Accelerations• Variability• Accelerations• Decelerations• Outcome

However……….
• DrCBravado not consistent with:– Electronic Fetal Monitoring
Guideline, published in 2001– NICE Intrapartum Guideline in 2007
• Therefore its use is substandard care

Breach of Duty
• Assessment of CTG• Classification into NICE
category• Documentation, each hour• Appropriate action for CTG
category

Causation – CP Template• Fetal, umbilical arterial cord, or very
early neonatal blood: pH <7.00 & base deficit >12 mmol/l
• Severe or moderate neonatal encephalopathy in infants >34 weeks
• Spastic quadriplegic or dyskinetic CP• Exclusion of other identifiable causes

CP Template contd
• Sentinel hypoxic event• Sustained fetal bradycardia or poor
variability in the presence of late or variable decelerations
• Apgar scores of 0-3 beyond 5 minutes (previously <7).
• Onset of multi-system involvement within 72 hours of birth.

Causation and timing
• Paediatric expert• Use of umbilical artery base excess:
Algorithm for the timing of hypoxic injury
Ross and Gala. Am JOG. 2002
– >10% infants born with Base Excess ≥16 will have cognitive defects at 1 yr
– Almost all infants born with base excess ≤ 12 are normal

Timing of Injury
• Normal Labour• Fetus enters labor with a base excess of –2
mmol/L– 1 mmol/L per 3 to 6 hours in normal first stage of
labour– 1 mmol/L per hour of second stage
• Abnormal CTG– 1 mmol/L per 30 minutes with repetitive typical
severe variable decelerations– 1 mmol/L per 6 to 15 minutes in subacute fetal
compromise– 1 mmol/L per 2 to 3 minutes with acute, severe
compromise (eg, terminal bradycardia)

Timing
• A guide, not an exact science • At what time would delivery
have avoided injury ?• Work backwards through trace
• Intermittent Auscultation

Pitfalls
• Cord Gas better than expected– Venous sample– Complete cord compression
• MRI– Other causes
• Chronic Partial – May not have sentinel event

Conclusion
• Breach of duty of care– Use NICE EFM & IP Template– Action also defined by national
guidance• Causation
– ACOG & International consensus template

Problem ?
• 50% adverse outcomes preventable with better care
CESDI – 4th Annual Report. 1997CEMD – Why Mothers Die. 1998
CEMACH – Saving Mothers Lives 2007
• UK Apgar <7 at 5 mins• Ranges from 0.4% of term infants to
1.96%• 5 fold variation !

Neonatal Outcomes
5’ Apgar p=0.00042 (Chi2 test for trend)HIE p=0.0176 (Chi2 test for trend)

National Results