




1
CRITICAL CARE RN
NEUROANATOMY &
COMPLETE
NEUROASSESSMENT
Navaz Karanjia, M.D.
Director, UCSD Neurocritical Care
UC-San Diego School of Medicine
October 20, 2011
Purpose
Review basic neuroanatomy relevant to critical
care patients
Review the objective complete neuroassessment
of the critical care patient
Understand how each part of the
neuroassessment correlates to neuroanatomy
Practice the neuroassessment to become
comfortable, consistent, and efficient with the
exam
Objectives
The participant will be able to:
Describe the functions of major parts of the nervous
system
Describe the major components of the complete
neurological examination of the awake and comatose
critical care patient
Accurately, consistently, efficiently, and confidently
perform the complete neurological assessment for
awake and comatose critical care patients
Report exam findings and trends objectively
Describe exam findings indicative of increasing ICP

2
Why do I want nurses to understand
neuroanatomy/neuroassessment?
Why do I want nurses to understand
neurocritical care physiology and assessment?
Brain Code
Don’t forget,
if the pt has
had an acute
neuro change
in <12h, also
call a stroke
code!

3
Brain Code Pager and Brain Code Box
Webpage Brain, Code (or Hillcrest pharmacy code pager 2619)
Code pharmacist, NCC team will arrive in <3 minutes with brain code box
Contains: 100g 20% mannitol, 30 cc 23% saline, 500 cc 3% saline, phenylephrine premixed syringes (100mcg/1mL), syringes, filters
Code sheet for documentation
>80 episodes of herniation treated
using BrainCodeBox at Hillcrest
in 2 years
75% episodes herniation reversed
60% survivors independent
at 6 mos
Brain Code
Why do I want nurses to understand
neuroanatomy/neuroassessment?
We are a team! We need to speak the same language!
Your serial OBJECTIVE neuroassessments are THE most
important marker of our neuro-ICU patients’ progress, and
should drive physicians' clinical decision-making
If you can tie anatomy to assessment, you will know:
Where is the lesion?
What is the lesion?
Structural: pathology that changes structure or exerts
pressure on structure (tumor, hemmorhage,
hydrocephalus)
Physiologic: ischemia, seizure, change in cerebral
metabolism
Why do I want nurses to understand
neuroanatomy/neuroassessment?
With this knowledge, you can better understand:
What is wrong with my patient?
How is my patient doing now?
What changes might I expect to see in my patient if
they start to decline?
What effect on outcome will this have on my patient?

4
Today’s fun
Neuroanatomy (1:20) Overview
Skull
Meninges
Ventricles
Cellular neuroanatomy
Brain
Vasculature
Spine
Neuroassessment (1:20)
Awake
Unconscious
Spinal
Hands on practice (1:00)
The Nervous System: divisions
CNS: brain & spinal cord
PNS: cranial nerves &
spinal nerves
Somatic/voluntary nervous
system
Autonomic nervous system
Parasympathetic
Sympathetic
The Nervous System: autonomic
Sympathetic Nervous System
Fight/Flight: HR, BP, RR, pupillary dilation
Inhibits: Peristalsis, urination, defecation
Parasympathetic Nervous System
Rest/Digest: HR, RR, BP, pupillary constriction
Stimulates: Peristalsis, urination, defecation
Sympathetic storm

5
Today’s fun
Neuroanatomy (1:20) Overview
Skull
Meninges
Ventricles
Cellular neuroanatomy
Brain
Vasculature
Spine
Neuroassessment (1:20)
Awake
Unconscious
Spinal
Hands on practice (1:00)
Skull anatomy
Skull is a rigid box that contains brain, blood, CSF
Cranium has 8 bones
Frontal
Occipital
Sphenoid
Ethmoid
Parietal (2)
Temporal (2)
Face has 14 bones
Sutures
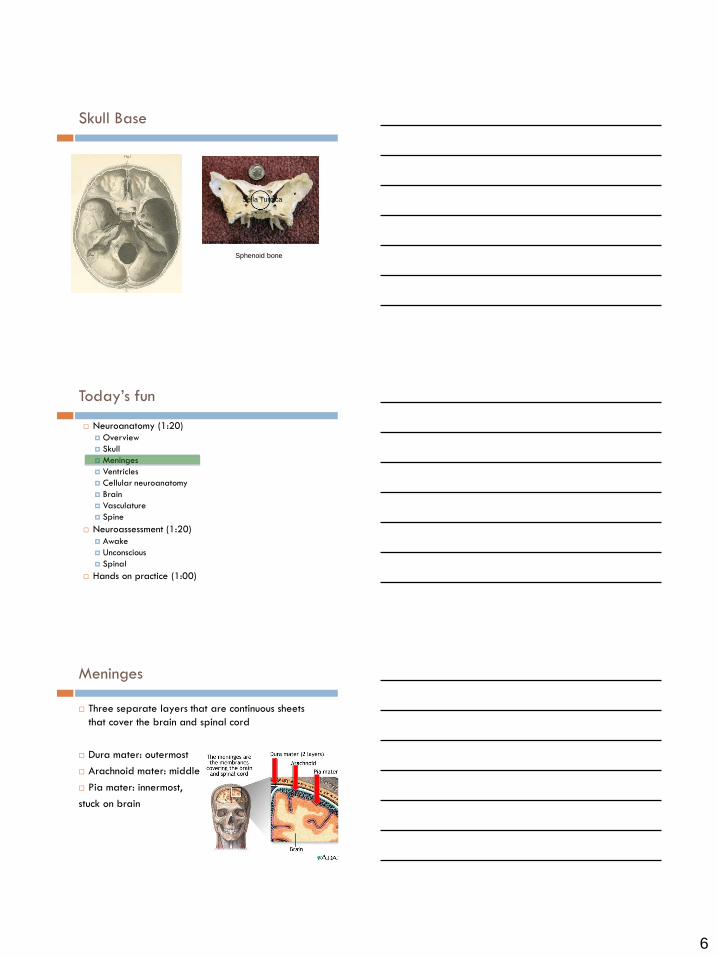
Skull Base
6
Skull Base
Sphenoid bone
Sella Turcica
Today’s fun
Neuroanatomy (1:20) Overview
Skull
Meninges
Ventricles
Cellular neuroanatomy
Brain
Vasculature
Spine
Neuroassessment (1:20)
Awake
Unconscious
Spinal
Hands on practice (1:00)
Meninges
Three separate layers that are continuous sheets
that cover the brain and spinal cord
Dura mater: outermost
Arachnoid mater: middle
Pia mater: innermost,
stuck on brain

7
Meninges: Dura Mater (outermost)
Tough, thick, inelastic to protect and support brain
Double layer: periosteal, meningeal
Meninges: Dura Mater
Subfalcine Herniation
Cerebral cortex under
falx
Leg weakness
mental status
Central/Upward
Herniation
Brainstem down/up
through tentorium
mental status
Dilated pupil, eye
“down and out” (CN3)
Weakness/posturing
Basilar stroke
Tonsillar Herniation
Cerebellar tonsils in foramen
magnum
Awake, pharynx weakness,
quadriparesis
Arrhythmia/cardiac arrest
Respiratory arrest
Uncal Herniation
Uncus over tentorial
notch
mental status
Dilated pupil, eye
“down and out” (CN3)
Weakness/posturing
PCA stroke

8
Meninges: Arachnoid Mater (middle)
Thin, weblike, avascular membrane under the dura
Subarachnoid space
Between arachnoid and pia
CSF, arachnoid villi (absorb CSF)
Subarachnoid hemorrhage
Meninges: Pia Mater (innermost)
Delicate membrane, contains blood vessels, exiting
nerves
Stuck to the brain
Hugs each gyrus, sulcus of the brain
Meninges: arteries and veins

9
Today’s fun
Neuroanatomy (1:20) Overview
Skull
Meninges
Ventricles
Cellular neuroanatomy
Brain
Vasculature
Spine
Neuroassessment (1:20)
Awake
Unconscious
Spinal
Hands on practice (1:00)
Ventricular System: anatomy
Ventricles: fluid filled chambers that contain/circulate CSF
Lateral ventricles (2)
3rd ventricle
4th ventricle
Choroid plexus:
produces CSF,
in the ventricles
Arachnoid villi:
resorbs CSF from
subarachnoid
space

10
Ventricular system: CSF
Function: Cushion in which brain “floats” When ICP , some CSF can be pushed out of the skull to lower ICP
Composition: Color: clear Protein: 16-45 mg/dl Glucose: 40-80 mg/dl (50-80% serum glucose) WBC: 0-5 cells/mm3 Lactate: 10-20 mg/dl
Formation: Produced by choroid plexus/ependymal cells 500 mL/day, 25 ml/hr 150 mL in circulation at any given time
Resorption: By arachnoid villi into the cerebral sinuses (veins)
1. Lateral ventricle
2. Interventricular foramen
3. Third ventricle
4. Cerebral aqueduct
5. Fourth ventricle
6a. Median aperture 6b. Lateral aperture 6c. Central canal (spinal cord)
7. Subarachnoid space
8. Arachnoid villi
9. Dural sinuses
Marieb 12.26b
CSF CIRCULATION

11
Today’s fun
Neuroanatomy (1:20) Overview
Skull
Meninges
Ventricles
Cellular neuroanatomy
Brain
Vasculature
Spine
Neuroassessment (1:20)
Awake
Unconscious
Spinal
Hands on practice (1:00)

12
Cellular neuroanatomy: CNS
2 main cell types: neurons and neuroglia
Neuron: basic anatomic functional unit of the nervous system
Dendrites
Cell body
Axon
Myelin
Cellular neuroanatomy: CNS
Neuroglia: support the neurons, mitotic
Astrocytes
BBB
Astrocytoma, GBM
Oligodendrocytes
Myelin
Oligodendroglioma
Ependymal cells
Produce CSF
Ependymoma
Microglia
Immune protection, phagocytic
Cellular neuroanatomy: PNS
Neurons (ganglia)
Schwann cells
Myelin
Multiple
sclerosis
13
BREAK FOR 5 MINUTES
Neuroanatomy (1:20) Overview
Skull
Meninges
Ventricles
Cellular neuroanatomy
Brain
Vasculature
Spine
Neuroassessment (1:20)
Awake
Unconscious
Spinal
Hands on practice (1:00)
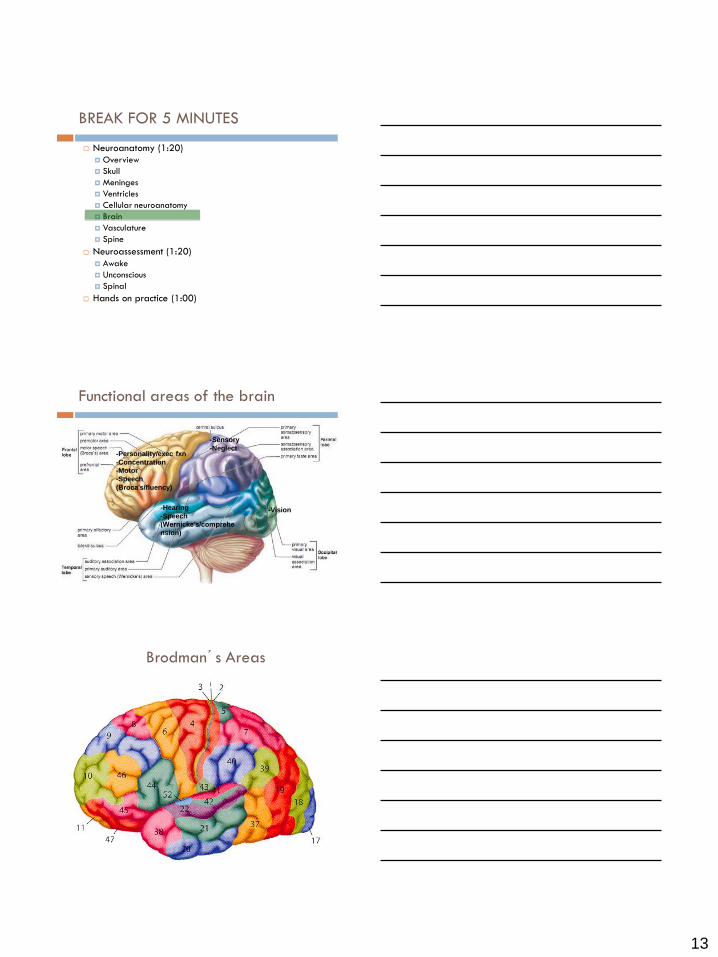
Functional areas of the brain
-Personality/exec fxn
-Concentration
-Motor
-Speech
(Broca’s/fluency)
-Hearing
-Speech
(Wernicke’s/comprehe
nsion)
-Sensory
-Neglect
-Vision
Brodman’s Areas

14
Cerebral Hemispheres: frontal lobes
High level cognitive function: personality, reasoning,
judgement, attention, social graces, moral behaviors
Level of consciousness
Motor control
motor cortex=just anterior to central sulcus
Motor Speech (Broca’s area)
Broca’s (expressive/nonfluent) aphasia: broken
speech
“I...can’t..can’t…talk!!!” (but follows commands)
Long term memory
Cerebral Hemispheres: parietal lobes
Sensory
Sensory cortex (posterior to central sulcus)
Attention to space, spatial relations, L vs R
Hemineglect after parietal stroke
Calculation
Reading, writing
THE HOMUNCULUS
MOTOR HOMUNCULUS SENSORY HOMUNCULUS
15
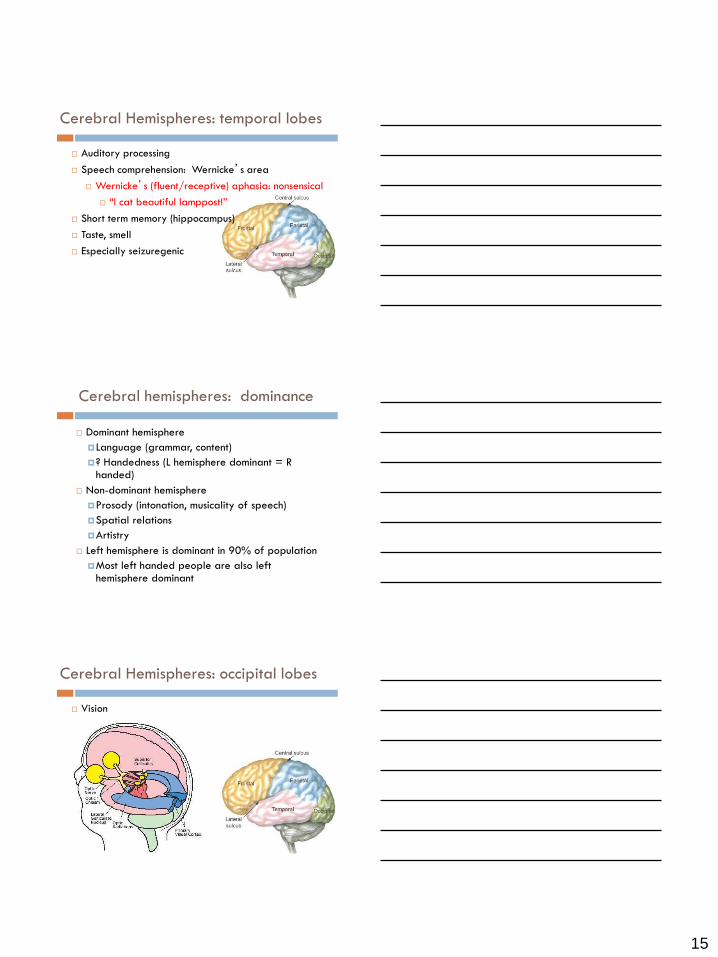
Cerebral Hemispheres: temporal lobes
Auditory processing
Speech comprehension: Wernicke’s area
Wernicke’s (fluent/receptive) aphasia: nonsensical
“I cat beautiful lamppost!”
Short term memory (hippocampus)
Taste, smell
Especially seizuregenic
Cerebral hemispheres: dominance
Dominant hemisphere
Language (grammar, content)
? Handedness (L hemisphere dominant = R handed)
Non-dominant hemisphere
Prosody (intonation, musicality of speech)
Spatial relations
Artistry
Left hemisphere is dominant in 90% of population
Most left handed people are also left hemisphere dominant
Cerebral Hemispheres: occipital lobes
Vision

16
Vision pathway
Deep Structures and connections
Brainstem
Diencephalon (thalamus, hypothalamus, pituitary)
Basal Ganglia
Deep Structures: basal ganglia
Masses of gray matter deep within the cerebrum
caudate, putamen, globus pallidus, substantia nigra, subthalamic nucleus
Regulate movement
Refines gross movements to fine motor
Tremors, Parkinson’s, Huntington’s
Reward learning, motivation
addiction, obsessive-compulsive disorder
Susceptible to spontaneous ICH

17
Deep Structures: diencephalon
Thalamus
Hypothalamus
Posterior pituitary
Pineal gland
Deep Structures: diencephalon
Thalamus
Relay station of the brain: all sensory pathways have connections here (except olfactory). Susceptible to ICH.
Hypothalamus
Homeostasis
Temperature control
Water balance: ADH
Feedback loop with pituitary: GH, FSH, oxytocin
Sleep-wake cycle
Pituitary
Anterior: GSH, ACTH, TSH, FSH, LH, prolactin
Posterior: ADH, oxytocin
Sits on top of optic chiasm
Connections: white matter
Corpus Callosum Big axon bundle connecting
hemispheres (MS)
Internal capsule
Tiny concentrated bunch of
axons connecting motor and
sensory cortex w/
deep
structures
and
spinal
cord
(stroke)
18
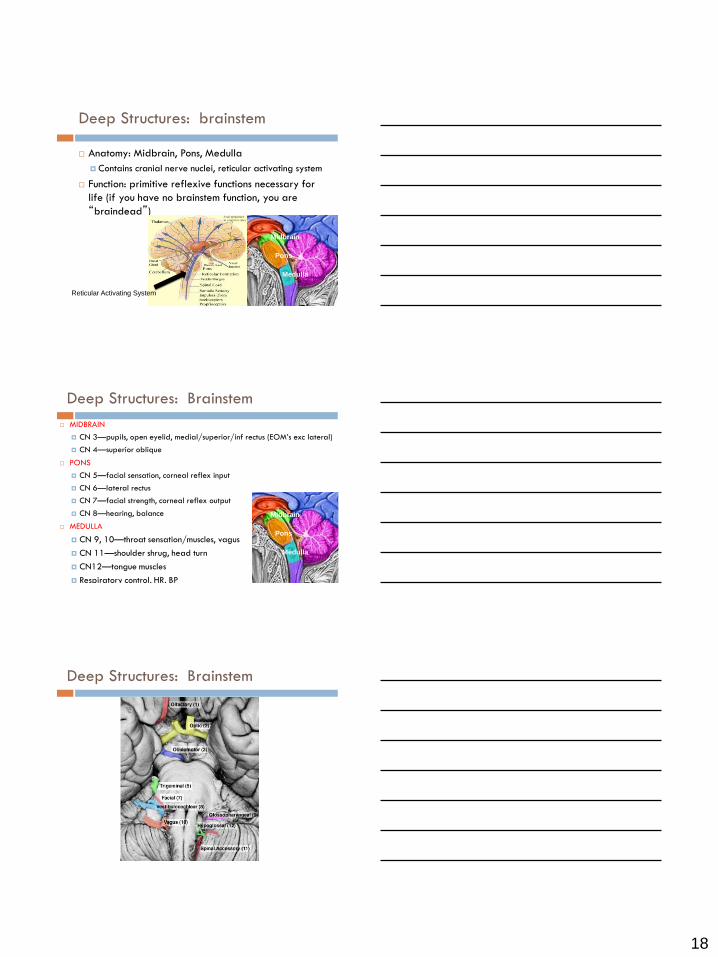
Deep Structures: brainstem
Anatomy: Midbrain, Pons, Medulla
Contains cranial nerve nuclei, reticular activating system
Function: primitive reflexive functions necessary for
life (if you have no brainstem function, you are
“braindead”)
Midbrain
Pons
Medulla
Reticular Activating System
MIDBRAIN
CN 3—pupils, open eyelid, medial/superior/inf rectus (EOM’s exc lateral)
CN 4—superior oblique
PONS
CN 5—facial sensation, corneal reflex input
CN 6—lateral rectus
CN 7—facial strength, corneal reflex output
CN 8—hearing, balance
MEDULLA
CN 9, 10—throat sensation/muscles, vagus
CN 11—shoulder shrug, head turn
CN12—tongue muscles
Respiratory control, HR, BP
Deep Structures: Brainstem
Midbrain
Pons
Medulla
Deep Structures: Brainstem
Pons
Medulla

19
Herniation syndromes
Subfalcine Herniation
Cerebral cortex under
falx
Leg weakness
mental status
Central/Upward
Herniation
Brainstem down/up
through tentorium
mental status
Dilated pupil, eye
“down and out” (CN3)
Weakness/posturing
Basilar stroke
Tonsillar Herniation
Cerebellar tonsils in foramen
magnum
Awake, pharynx weakness,
quadriparesis
Arrhythmia/cardiac arrest
Respiratory arrest
Uncal Herniation
Uncus over tentorial
notch
mental status
Dilated pupil, eye
“down and out” (CN3)
Weakness/posturing
PCA stroke
Cerebellum
Anatomy: posterior fossa, attached to brainstem by
cerebellar peduncles, sits behind 4th ventricle and
brainstem
Function:
Coordination
Equilibrium/balance
Herniation syndromes
Subfalcine Herniation
Cerebral cortex under
falx
Leg weakness
mental status
Central/Upward
Herniation
Brainstem down/up
through tentorium
mental status
Dilated pupil, eye
“down and out” (CN3)
Weakness/posturing
Basilar stroke
Tonsillar Herniation
Cerebellar tonsils in foramen
magnum
Awake, pharynx weakness,
quadriparesis
Arrhythmia/cardiac arrest
Respiratory arrest
Uncal Herniation
Uncus over tentorial
notch
mental status
Dilated pupil, eye
“down and out” (CN3)
Weakness/posturing
PCA stroke

20
Purpose of nursing neuroassessment
Herniation: early detection saves lives
MA Koenig, M Bryan, JL Lewin, III, MA Mirski, RG Geocadin and RD Stevens
Neurology 2008;70;1023-1029; originally published online Feb 13, 2008
Long-term outcome after medical reversal of transtentorial herniation
in patients with supratentorial mass lesions Qureshi,,Geocadin,Suarez, Ulatowski, CRITICAL CARE MEDICINE 2000;28:1556-1564
11/28 (40%) survived to discharge
7/11 (59%) survivors functionally independent
253 cases TTH (acute onset uni/bilateral pupillary dilation, loss of
reactivity, GCS decrease >2 pts, intracranial space occupying lesion)
30cc 23.4% saline bolus reversed clinical signs of TTH in 75% of pts
Herniation: early detection saves lives

21
Today’s fun
Neuroanatomy (1:20) Overview
Skull
Meninges
Ventricles
Cellular neuroanatomy
Brain
Vasculature
Spine
Neuroassessment (1:20)
Awake
Unconscious
Spinal
Hands on practice (1:00)
Cerebral Vasculature: arterial
ACA
PCA
MCA
Cerebral Vasculature: arterial
Anterior circulation (fed by internal carotid)
Anterior cerebral arteries (ACA)
Anterior communicating artery (A. Com)
Middle cerebral arteries (MCA)
Posterior circulation:
Posterior cerebral arteries (PCA)
Posterior communicating arteries (P. Com)
Basilar artery
Vertebral arteries

22
Cerebral Vasculature: venous
Today’s fun
Neuroanatomy (1:20) Overview
Skull
Meninges
Ventricles
Cellular neuroanatomy
Brain
Vasculature
Spine
Neuroassessment (1:20)
Awake
Unconscious
Spinal
Hands on practice (1:00)
Spinal anatomy
Vertebral Column
Discs
Spinal Nerves
Spinal Cord

23
Spinal anatomy
Vertebral Column
33 bony vertebrae 7 cervical- C1-C7
12 thoracic- T1-T12
5 lumbar- L1-L5
5 sacral (fused)-S1-S5
4 coccygeal (fused)
Separated by intervertebral disks
Connected by ligaments
Function
Body's basic structural support
Protects the spinal cord
Spinal anatomy: vertebrae
Spinous process
Spinal anatomy: discs
Anatomy: Stiff jello like center (nucleus
pulposa) surrounded by layers of connective fibers (annulus fibrosis)
Function: Shock absorbers
Shrivel with age (1-2 inches)

24
Spinal anatomy: spinal nerves
31 spinal segments/pairs of spinal nerve roots
8 cervical
12 thoracic
5 lumbar
5 sacral
Spinal anatomy: spinal nerves
Deltoids (C5)
Biceps (C5-6)
Triceps (C6-7)
Wrist extension (C6-7)
Finger extension (C8)
Hip flexion (L2-3)
Hip extension (L3-4)
Knee extension (L3-4)
Knee flexion (L5-S1)
Foot dorsiflexion (L4-5)
Foot plantarflexion (S1-2)
Toe extension/EHL (L5)
Spinal anatomy: spinal cord
Spinal cord:
ends at L1 or L2
conus medullaris: bulbous end of spinal cord
cauda equina (horse’s tail): collection of nerve roots

25
Spinal anatomy: spinal cord
ANTERIOR
POSTERIOR
Sensory
Motor
Spinal anatomy: spinal cord
S
E
N
S
O
R
Y MOTOR
MOTOR Motor tracts
Corticospinal
Voluntary
movement
Medial=arms
Lateral=legs
Rubrospinal,
reticulospinal,
vestibulospinal,
tectospinal
Postural reflexes
Spinal anatomy: spinal cord
S
E
N
S
O
R
Y MOTOR
MOTOR Sensory tracts
Spinothalamic
Pain, temp, light touch
Contralateral
Posterior columns
Proprioception,
vibration, discrim. touch
Ipsilateral
Spinocerebellar
Unconscious
proprioception
Spinoreticular
Deep pain
26
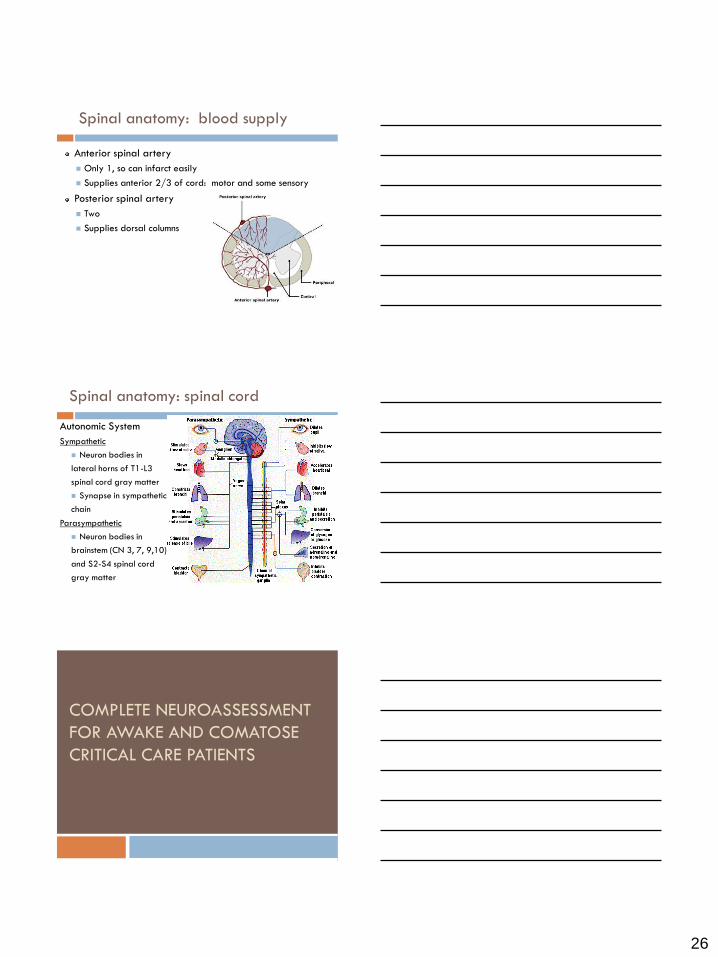
Spinal anatomy: blood supply
Anterior spinal artery
Only 1, so can infarct easily
Supplies anterior 2/3 of cord: motor and some sensory
Posterior spinal artery
Two
Supplies dorsal columns
Autonomic System
Sympathetic
Neuron bodies in
lateral horns of T1-L3
spinal cord gray matter
Synapse in sympathetic
chain
Parasympathetic
Neuron bodies in
brainstem (CN 3, 7, 9,10)
and S2-S4 spinal cord
gray matter
Spinal anatomy: spinal cord
COMPLETE NEUROASSESSMENT
FOR AWAKE AND COMATOSE
CRITICAL CARE PATIENTS
27
Objectives
The participant will be able to:
Describe the major components of the complete
neurological examination of the awake and
comatose critical care patient
Accurately, consistently, efficiently, and confidently
perform the complete neurological assessment for
awake and comatose critical care patients
Report exam findings and trends objectively
Describe assessment findings that are indicative of
increasing ICP.
Purpose of complete RN neuroassessment
Serial objective evaluation and trending of nervous
system function: the nervous system vitals monitor
Identifies exam changes that require intervention and
may be life-threatening
Provides basis for patient management and
prognostication
Monitors treatment response
Identifies etiology and location of pathological processes
Evaluates patient’s functional ability and capacity for self-
care
Evaluates impact of disability on patient and family
Purpose of RN complete neuroassessment
28
Common RN neuroassessment pitfalls
Inadequate stimulus to achieve best response
Inadequate baseline assessment
Failure to use objective terminology
Failure to recognize subtle clues in time for
successful intervention
Failure to have confidence in your assessment skills
and go up the chain of command. If you know
something is wrong with your patient, be persistent
in getting help!
Components of the RN complete
neuroassessment
History
Level of Consciousness
Cranial Nerves
Motor exam
Sensation
Coordination
Reflexes
Gait
Not generally done in
neuro-ICU nursing
assessment
Level of consciousness: GCS. Awake/lethargic/obtund/stupor.
Orientation: Name? Date? Place? What brought you in?
Language: Fluency? Name watch, pen. Commands. Repetition.
Neglect: Tactile? Spatial?
Cranial Nerves: Pupils. Visual fields. Acuity. Eye & lid position.
EOMs. Facial sensation. Facial strength. Hearing. Speech.
Cough. Shrug. Head turn. Tongue protrusion.
Motor: Pronator drift. Deltoids. Biceps. Triceps. Grip. Hip flex.
Hip ex. Knee flex. Knee ex. Dorsi/Plantarflex. EHL.
Sensation: Light touch in all 4’s.
Cerebellum: Finger to nose. Heel to Shin.
Complete neuroassessment: awake
29
History
Chief Complaint/History of Present Illness
Past Medical/Surgical History
Cataract surgery?
What are their seizures like?
What were their symptoms with their old strokes?
Social History
When was their last EtOH, tobacco, drugs?
Medications
Coumadin, dabigitran, aspirin, plavix, garlic/ginko,
antiepileptics, sedatives
What time was their last dose?
Review of Systems
Level of Consciousness: principles
Level of consciousness consists of 2 parts:
1. AROUSAL/AWAKENESS 2. CONTENT
Level of Consciousness: principles
MOST SENSITIVE AND SPECIFIC INDICATOR OF NEUROLOGICAL CHANGE
Objective
Can change rapidly (neurological deterioration)
Any change for the worse requires immediate physician evaluation and possible intervention
Can be confounded by medications (sedatives, antiepileptics) and withdrawal
Pause sedative drips for exams with physician approval
Frequently reevaluate lowest amount of sedative/pain meds needed to achieve goals

30
Level of Consciousness: arousal
Reticular Activating System THINGS THAT AROUSAL
Diffuse cortical dysfunction
Metabolic changes (hypoxia,
hypoglycemia, pH abnl,
hyponatremia)
Medications
Hypotension (decreased CBF)
Increased ICP
Big structural lesions
Lesions of RAS (brainstem or
bilateral thalamus)
Level of consciousness: GCS
Coma = GCS<8
E2
V2
M4
Level of Consciousness: arousal
LEVEL OF AROUSAL
Awake (E4)
Awake/arouses easily from sleep with quick, normal cognition
Lethargic (E4)
Awake/arouses easily but slow cognition or motor activity
Obtunded (E3)
Drowsy
Requires non-painful stim to open eyes. May say few words, follow simple commands
Stuporous (E2)
Unresponsive except when stimulated
Requires painful stim to open eyes. May mutter incomprehensible sounds
Comatose (E1)
Unresponsive
No eye opening. Localizes, withdraws, postures, or no response to pain

31
Level of Consciousness: arousal
Follows commands-M6
Localizes: LOCAtes stimulus & combats it (some cortex)-M5
Withdraws: pulls away from pain (thalamus)-M4
Flexor postures (brainstem)-M3
Extensor postures (brainstem)-M2
No response or leg triple flexion (spinal cord)-M1
Triple flexion: flexion at ankle, knee, hip
Level of Consciousness: assessing arousal
Maximum stimulus for maximum response
Voice
↓
Shout
↓
Shake
↓
Central Pain
↓
Peripheral Pain
Central Pain: more
reliable indicator of
arousal
Trapezius squeeze
Supraorbital notch
Biceps tendon
Peripheral Pain:
Inner bicep/axilla
Inner thigh
Nailbed pressure
(only as last resort)
Level of Consciousness: arousal
ADDITIONAL AROUSAL DESCRIPTORS
Posturing
FLEXOR
EXTENSOR

32
-Personality/exec fxn
-Concentration
-Motor
-Speech
(Broca’s/fluency)
-Hearing
-Speech
(Wernicke’s/comprehe
nsion)
-Sensory
-Neglect
-Vision
Level of Consciousness: content
Orientation
Language
Fluency
Naming
Comprehension/commands
Repetition
Neglect
Visual
Tactile
Personal
Orientation: A&O x 1, 2, 3, 4
What is your name? What is the date? (if they hesitate, ask year, month, then day) Where are we? What brought you into the hospital?
Language:
Fluency: listen as pt talks. (Normal I…can’t……talk! mute)
Naming: point to a watch and pen and ask pt to name
Comprehension/commands: Close eyes/stick out tongue, show 2 fingers, wiggle toes; “point to the ceiling and then to the door” (complex)
Repetition: Repeat after me, “It is a sunny day in San Diego”
Neglect: (normalneglect to 1 modalityneglect to >1)
Tactile: Ask pt to close their eyes, then touch R arm, ask “where am I touching you?” Then repeat w/ L arm. Then touch both simultaneously.
Spatial: Observe pt as you move around room; see if they prefer 1 side. If multiple people in the room, you can ask how many they see.
Personal: They ignore 1 half of their body even though they’re not weak
Level of Consciousness: assessing content
How to report level of consciousness
Pt is awake and oriented x 4
Pt is awake and oriented to name and place
Pt is lethargic/obtunded/stuporous, opens eyes to
voice/shake/painful stim
Speech is fluent/nonfluent, follows simple/complex
commands, naming and repetition intact/not intact
Pt has no/R sided/L sided neglect
Level of Consciousness: assessment

33
Cranial Nerves: what they do
CN 2: acuity, visual fields, pupils
CN 3: pupils, eyelid opening, EOM’s
CN 3/4/6: EOM’s, oculocephalic, cold calorics
CN 5: facial sensation, corneals
CN 7: facial strength, eyelid closure, corneals
CN 8: hearing, balance, oculocephalic, cold calorics
CN 9/10: speech, cough, gag
CN 11: shrug, head turn
CN 12: tongue protrusion, speech
Cranial Nerves: assessment
AWAKE PATIENT
Pupils (2, 3)
Visual fields, acuity (2)
Eye position, eyelid, EOMs (3, 4, 6)
Facial sensation (5)
Facial strength (7)
Hearing (8)
Speech/Cough/Gag (9,10)
Shrug, head turn (11)
Tongue protrusion (12)
COMATOSE PATIENT
Pupils (2, 3)
Threat (2)
Eye position (3, 4, 6)
Oculocephalic (3, 4, 6, 8)
Corneals (5, 7)
Cough (9, 10)
Vitals (10)
Cranial Nerves: awake assessment
PUPILS—CN 2, 3
Size
Normal: 2-5mm
Abnormal: pinpoint <2mm (pontine dysfxn, meds), dilated >5mm
(CN3/midbrain dysfxn from ICP >18, atropine, epinephrine), any
change in size >1mm
Shape
Normal: round, may be irregular from cataract surgery
Abnormal: ovoid (CN3 dysfxn from ICP. Precedes dilated pupil.)
Equality
Normal: equal, may have physiologic anisocoria (1 mm difference)
Abnormal: >1mm difference between two pupils

34
Cranial Nerves: awake assessment
PUPILS—CN 2, 3
Reactivity to light
Direct (look at the pupil you’re shining the light into)
Normal: brisk pupil constriction when light is shone in,
dilation when light is taken away
Abnormal: sluggish or no pupil constriction when light is
shone in (increased ICP, hypothermia, high doses of
sedatives), any decrease or inequality in reactivity
Consensual (look at the pupil you’re NOT shining the light into)
Normal: opposite pupil also constricts when light is shone in
Abnormal: opposite pupil does nothing or dilates when
light is shone in
Cranial Nerves: awake assessment
PUPILS—CN 2, 3
How to assess:
Turn the lights off
Ensure the same ambient light as the previous tester
Observe size and shape of both pupils before you shine light in
Swing a bright (non-LED) flashlight quickly onto one eye and
observe reactivity in that eye and the opposite eye
Do the opposite eye
How to report:
“Pupils were 4 mm, equal and briskly reactive”
“Pupils were small, equal, and briskly reactive” (PERRL)
“R pupil was 4mm and briskly reactive, L pupil was 5mm and
sluggish”
Cranial Nerves: awake assessment
PUPILLARY BADNESS TO REMEMBER
During early increased ICP (pressure on CN3)
1 or both pupils become less reactive than before (catch it!)
1 or both pupils gradually dilate
1 or both pupils may become ovoid
During later increased ICP (pressure on midbrain)
1 or both pupils become fixed and dilated
During really late increased ICP (midbrain is dead, pressure on pons)
Both pupils become pinpoint and fixed
Braindeath
Pupils may stay fixed and dilated/pinpoint, or may return to midposition (2-3mm) and fixed
35
Cranial Nerves: awake assessment
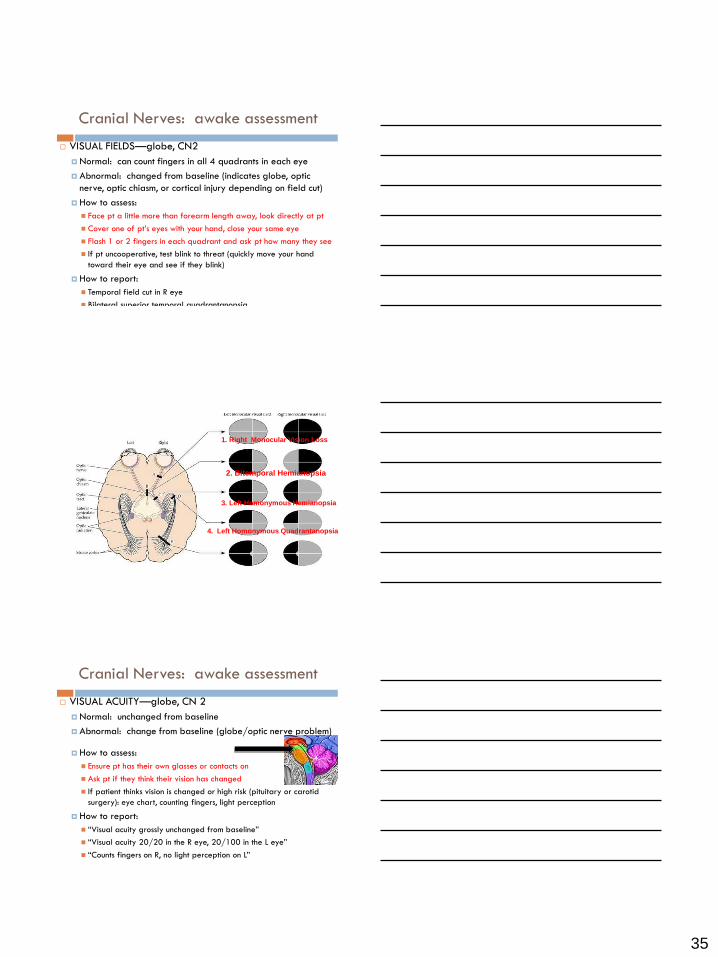
VISUAL FIELDS—globe, CN2
Normal: can count fingers in all 4 quadrants in each eye
Abnormal: changed from baseline (indicates globe, optic
nerve, optic chiasm, or cortical injury depending on field cut)
How to assess:
Face pt a little more than forearm length away, look directly at pt
Cover one of pt’s eyes with your hand, close your same eye
Flash 1 or 2 fingers in each quadrant and ask pt how many they see
If pt uncooperative, test blink to threat (quickly move your hand
toward their eye and see if they blink)
How to report:
Temporal field cut in R eye
Bilateral superior temporal quadrantanopsia
1. Right Monocular Vision Loss
2. Bitemporal Hemianopsia
3. Left Homonymous Hemianopsia
4. Left Homonymous Quadrantanopsia
Cranial Nerves: awake assessment
VISUAL ACUITY—globe, CN 2
Normal: unchanged from baseline
Abnormal: change from baseline (globe/optic nerve problem)
How to assess:
Ensure pt has their own glasses or contacts on
Ask pt if they think their vision has changed
If patient thinks vision is changed or high risk (pituitary or carotid
surgery): eye chart, counting fingers, light perception
How to report:
“Visual acuity grossly unchanged from baseline”
“Visual acuity 20/20 in the R eye, 20/100 in the L eye”
“Counts fingers on R, no light perception on L”

36
Cranial Nerves: awake assessment
EYE POSITION—CN 3, 4, 6, & EYELID OPENING—CN 3
Normal: midposition eyes, eyelids symmetrically open
Abnormal: any change from baseline or asymmetry, ptosis
(eyelid drooping) (CN 3, 4, or 6 pathology)
How to assess:
Observe pt’s eye position and eyelids for
symmetry when they are looking directly at you
How to report:
Often not reported if normal
Pt has R ptosis
“At rest, L eye is laterally deviated”
“At rest, both eyes are down and out”
Cranial Nerves: awake assessment
EXTRAOCULAR MOVEMENTS (EOM’s)—CN 3, 4, 6
Normal: smooth movements w/ full excursion up, down, R,
L (iris buries w/ lateral gaze), a little nystagmus upon end
gaze
Abnormal:
any asymmetry
impaired mobility (CN 3/4/6, midbrain/pons pathology)
forced gaze (stroke/seizure)
jerky movements or nystagmus
(CN8, cerebellum, vestibular system)
double vision
•inferior oblique (IO) •—cranial nerve III
•medial rectus (MR) •cranial nerve III
•superior oblique (SO) •—cranial nerve IV
•inferior rectus (IR) •—cranial nerve III
•lateral rectus (LR) •—cranial nerve VI
•superior rectus (SR) •—cranial nerve III
Cranial Nerves: awake assessment
37
Cranial Nerves: awake assessment
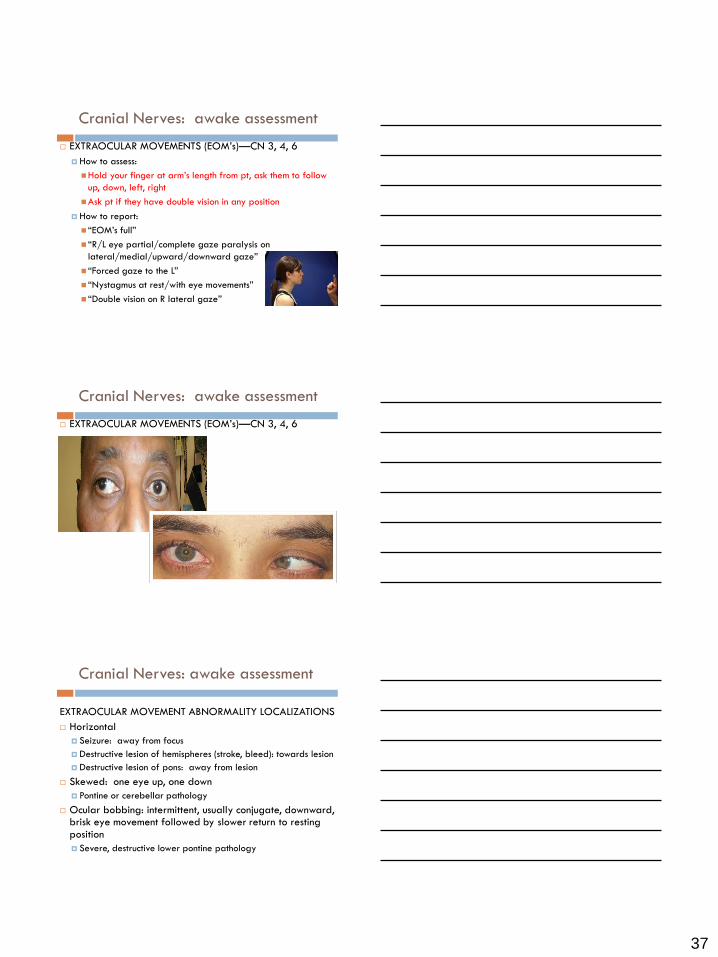
EXTRAOCULAR MOVEMENTS (EOM’s)—CN 3, 4, 6
How to assess:
Hold your finger at arm’s length from pt, ask them to follow
up, down, left, right
Ask pt if they have double vision in any position
How to report:
“EOM’s full”
“R/L eye partial/complete gaze paralysis on
lateral/medial/upward/downward gaze”
“Forced gaze to the L”
“Nystagmus at rest/with eye movements”
“Double vision on R lateral gaze”
Cranial Nerves: awake assessment
EXTRAOCULAR MOVEMENTS (EOM’s)—CN 3, 4, 6
Cranial Nerves: awake assessment
EXTRAOCULAR MOVEMENT ABNORMALITY LOCALIZATIONS
Horizontal
Seizure: away from focus
Destructive lesion of hemispheres (stroke, bleed): towards lesion
Destructive lesion of pons: away from lesion
Skewed: one eye up, one down
Pontine or cerebellar pathology
Ocular bobbing: intermittent, usually conjugate, downward, brisk eye movement followed by slower return to resting position
Severe, destructive lower pontine pathology
38
Cranial Nerves: awake assessment
FACIAL SENSATION—CN 5
Normal: symmetric sensation to light touch on forehead (V1),
cheeks (V2), chin V3)
Abnormal: any asymmetry or change from baseline
How to assess:
Lightly stroke both sides of pt’s forehead once, then cheeks,
then chin, asking each time “does this feel the same on both
sides?”
How to report:
“Face has normal sensation”
“Face has decreased sensation in R V2”
Cranial Nerves: awake assessment
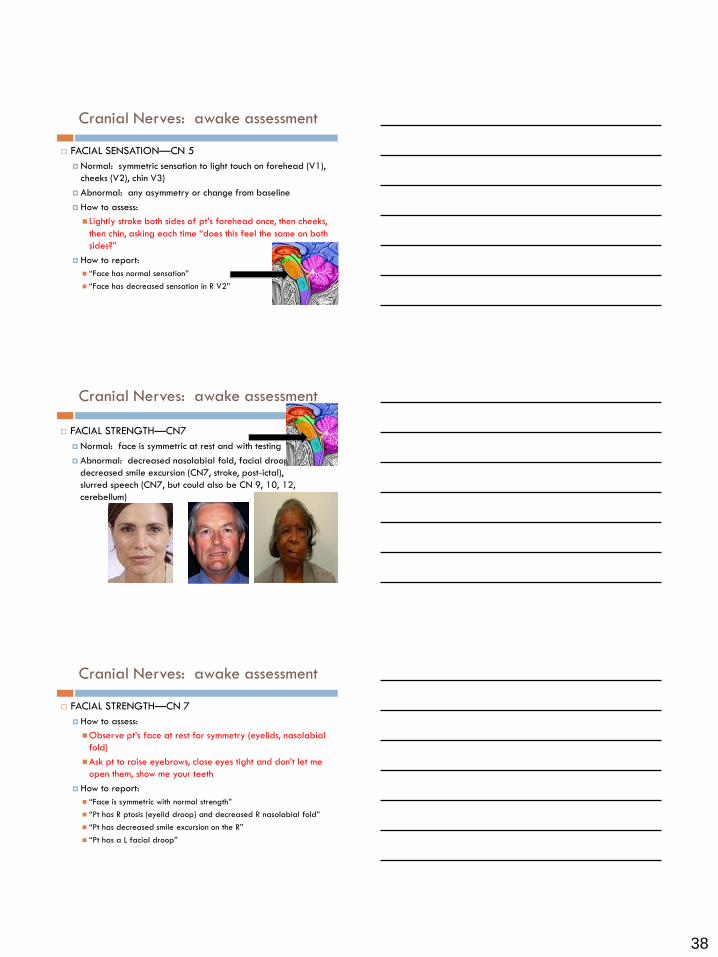
FACIAL STRENGTH—CN7
Normal: face is symmetric at rest and with testing
Abnormal: decreased nasolabial fold, facial droop,
decreased smile excursion (CN7, stroke, post-ictal),
slurred speech (CN7, but could also be CN 9, 10, 12,
cerebellum)
Cranial Nerves: awake assessment
FACIAL STRENGTH—CN 7
How to assess:
Observe pt’s face at rest for symmetry (eyelids, nasolabial
fold)
Ask pt to raise eyebrows, close eyes tight and don’t let me
open them, show me your teeth
How to report:
“Face is symmetric with normal strength”
“Pt has R ptosis (eyelid droop) and decreased R nasolabial fold”
“Pt has decreased smile excursion on the R”
“Pt has a L facial droop”

39
Cranial Nerves: awake assessment
HEARING—CN 8
Normal: no asymmetry in hearing
Abnormal: any asymmetry or change from baseline (CN8,
earwax, ear canal pathology)
How to assess:
Rub 2 fingers lightly together near pt’s R ear and ask “can
you hear this?”, repeat on the L, then ask “is there any
difference between the two sides?
How to report:
“Hearing is normal”
“Decreased hearing in R ear”
Cranial Nerves: awake assessment
SPEECH/COUGH/GAG—CN 9, 10
Normal: speech clear, does not cough w/ drinking,
uvula midline, palate elevates symmetrically
Abnormal: slurred/soft/hoarse speech, coughs while
drinking/eating, weak cough, uvula deviates to one side, palate
does not elevate, any asymmetry or change from baseline
How to assess:
Listen to pt’s speech and observe pt while eating/drinking
Ask pt to say “ah” and observe uvula/palate
With qtip, gently touch back of pt’s throat, once on each side
How to report:
“Uvula deviates to the R and decreased gag on R”
Cranial Nerves: awake assessment
SHRUG/HEAD TURN—CN 11
Normal: strong and symmetric
Abnormal: weak or asymmetric
How to assess:
Observe pt’s neck muscles for asymmetry at rest
Ask pt to shrug shoulders while you push down
Ask pt to turn their head against your hand
How to report:
“Shrug and head turn full strength”
“R shoulder shrug 4 out of 5”
“L head turn 3 out of 5”
40
Cranial Nerves: awake assessment
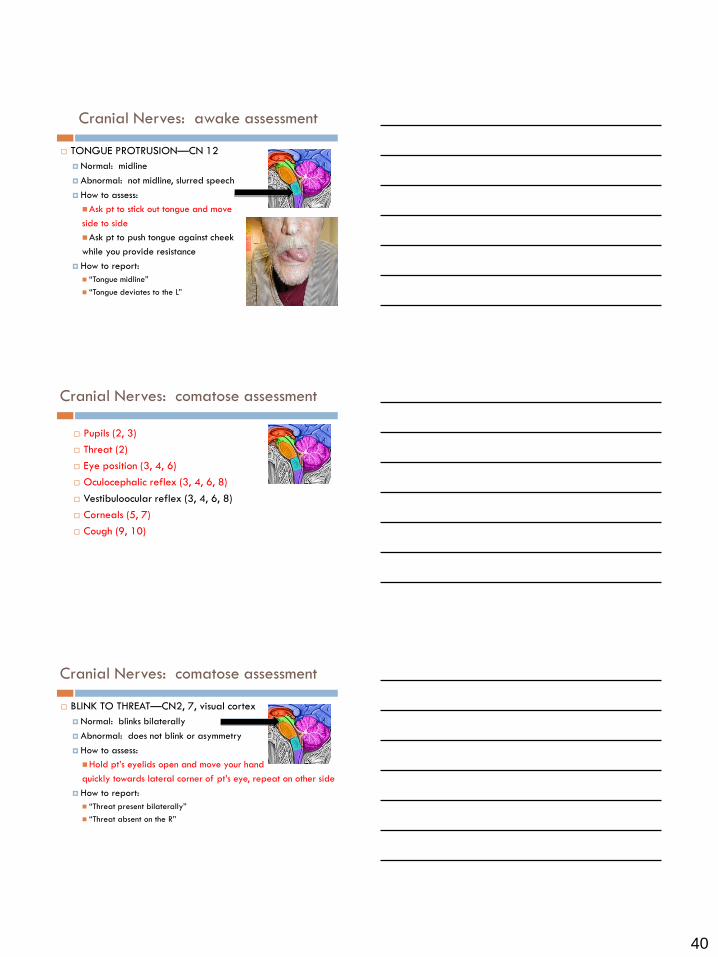
TONGUE PROTRUSION—CN 12
Normal: midline
Abnormal: not midline, slurred speech
How to assess:
Ask pt to stick out tongue and move
side to side
Ask pt to push tongue against cheek
while you provide resistance
How to report:
“Tongue midline”
“Tongue deviates to the L”
Cranial Nerves: comatose assessment
Pupils (2, 3)
Threat (2)
Eye position (3, 4, 6)
Oculocephalic reflex (3, 4, 6, 8)
Vestibuloocular reflex (3, 4, 6, 8)
Corneals (5, 7)
Cough (9, 10)
Cranial Nerves: comatose assessment
BLINK TO THREAT—CN2, 7, visual cortex
Normal: blinks bilaterally
Abnormal: does not blink or asymmetry
How to assess:
Hold pt’s eyelids open and move your hand
quickly towards lateral corner of pt’s eye, repeat on other side
How to report:
“Threat present bilaterally”
“Threat absent on the R”

41
Cranial Nerves: comatose assessment
OCULOCEPHALIC REFLEX (“Doll’s Eyes”)—3, 4, 6, 8
Normal: eyes move away from
direction of turning as if to stay
looking at examiner
Abnormal: eyes do not move in their sockets
How to assess (DO NOT assess in cspine patients!)
Ensure pt’s ET tube firmly taped and has slack
Hold pt’s eyelids open and quickly turn head to R, then L,
observing movement of eyes
How to report:
“Oculocephalic reflex present”
“Oculocephalic reflex absent”
Cranial Nerves: comatose assessment
VESTIBULOOCULAR REFLEX (cold calorics)—3, 4, 6, 8
Normal: eyes move away from
direction of cold water
Abnormal: eyes do not move
How to assess (usually by MD, only during braindeath exam)
Examine ear canal for wax or TM perforation
Hold eyelids open, inject 60cc of ice cold saline through
flexible tubing attached to slip tip syringe in 1 ear, watch for
eye movement for 30 seconds, then do other ear
How to report:
Vestibuloocular reflex present/absent
Cranial Nerves: comatose assessment
CORNEALS—CN5, 7
Normal: strong blink reflex bilaterally
Abnormal: weak or absent blink
How to assess:
Brush eyelashes on each eye
Saline eyedrop in each eye
If no response, try wisp off of cotton qtip
How to report:
“Corneals present bilaterally”
“Corneals present bilaterally, but R weaker than L”
“R corneal present, L absent”

42
Cranial Nerves: comatose assessment
COUGH
Normal: strong cough to suction
Abnormal: weak, absent, or any change
How to assess:
suction patient (ask physician if ok to do if pt has
unsecured aneurysm or ICP problems)
How to report:
“Cough present”
“Weak cough present”
“Cough absent”
Cranial Nerves: comatose assessment
VITALS
Normal: normal HR, BP, RR and pattern
Abnormal: brady/tachycardia, arrhythmia
(usually tachy/brady, PAC/PVC’s),
Increased/decreased RR, changing respiratory
pattern, any change in baseline
How to assess:
Watch for trends—change of HR from 80 to 60 could indicate
worsening medullary function
How to report:
You know how
Motor Exam: assessment
1. QUALITY of motor response (GCS motor)
-identifies level of nervous system dysfunction
2. STRENGTH of motor response (5/5 strength)
-trends nervous system function

43
Motor Exam: assessment
QUALITY OF MOTOR RESPONSE
Follows commands (lots of cortex)-GCS M6
Localizes: LOCAtes stimulus & combats it (some cortex)-M5
Withdraws: pulls away from pain (thalamus)-M4
Flexor postures (brainstem)-M3
Extensor postures (brainstem)-M2
No response or leg triple flexion (spinal cord)-M1
Triple flexion: flexion at ankle, knee, hip
Motor Exam: Strength
STRENGTH OF MOTOR RESPONSE
5: Normal; full strength against resistance
4: Some resistance; examiner can overcome patient
3: Can lift body part (antigravity), but provides no resistance
2: Cannot lift body part, but can move it laterally (with gravity eliminated)
1: Muscle contraction detectable
0: No muscle contraction detectable
Motor Exam: awake assessment
Pronator Drift: most sensitive sign of upper extremity weakness
Close eyes
Ask pt to hold arms up like holding a pizza, palms up to ceiling and flat
20-30 seconds
Observe for trembling, finger curl, arm turning inward(pronation), actual drift
Deltoids: arms up like chicken wings, don’t let me push them down
Biceps: pull in towards you
Triceps: push me away
Wrist extension: cock your wrists back
Finger extension: spread fingers out
Grip: squeeze my fingers

44
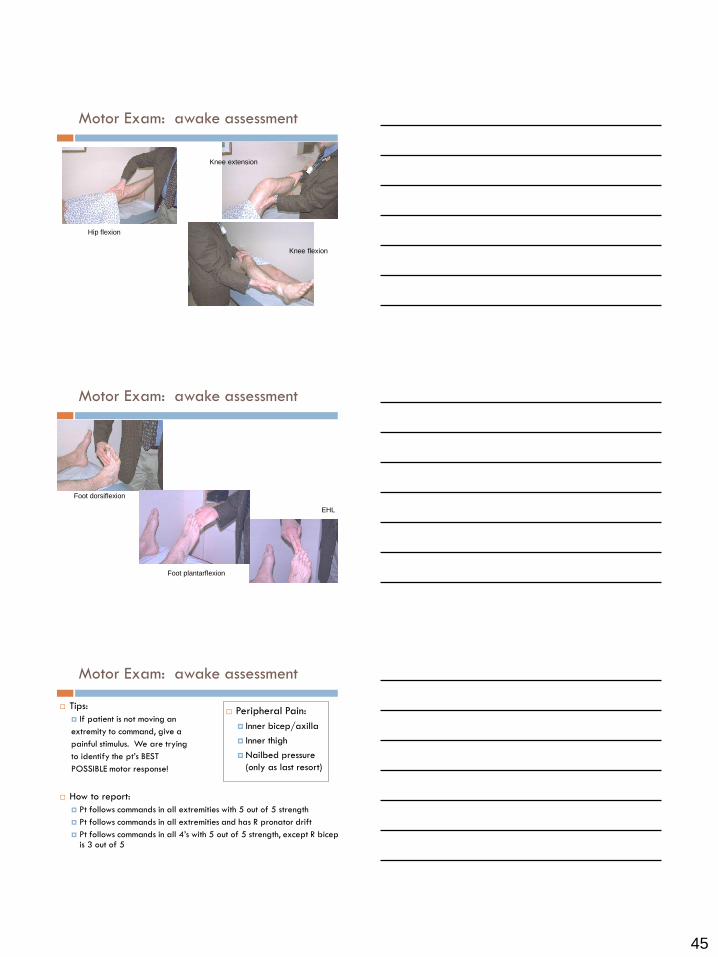
Motor Exam: awake assessment
Hip flexion: ask pt to bend their knee, put your hand on their knee, then ask them to push up on your hand
Hip extension: put one hand under their thigh and ask them to press down on your hand
Knee extension: ask pt to straighten their leg and keep it straight, while you support them with your arm under their knee. With your other hand push down on ankle
Knee flexion: ask pt to keep their knee bent while you try to straighten their leg
Foot Dorsiflexion: ask pt to pull their toes up to nose, or cock foot back at the ankle, while you push down on the top of their foot
Foot Plantar Flexion: push down on gas
Toe extension/EHL: ask pt to pull big toe up to nose against your hand
Motor Exam: awake assessment
Pronator Drift
Bicep
Tricep
Motor Exam: awake assessment
Grip Finger extension
45
Motor Exam: awake assessment
Hip flexion
Knee extension
Knee flexion
Motor Exam: awake assessment
Foot dorsiflexion
Foot plantarflexion
Knee flexion
EHL
Motor Exam: awake assessment
Tips:
If patient is not moving an
extremity to command, give a
painful stimulus. We are trying
to identify the pt’s BEST
POSSIBLE motor response!
How to report:
Pt follows commands in all extremities with 5 out of 5 strength
Pt follows commands in all extremities and has R pronator drift
Pt follows commands in all 4’s with 5 out of 5 strength, except R bicep is 3 out of 5
Peripheral Pain:
Inner bicep/axilla
Inner thigh
Nailbed pressure
(only as last resort)

46
Motor Exam: comatose assessment
How to assess:
Put pt’s forearms resting on their belly
Uncover pt completely
Give central painful stim first; if
pt does not do something in all 4’s,
proceed to peripheral pain
How to report:
Pt localizes to central pain in all 4’s
Pt withdraws in the uppers and
triple flexes in the lowers
Central Pain: more
reliable indicator
of arousal
Trapezius squeeze
Supraorbital notch
Peripheral Pain:
Inner bicep/axilla
Inner thigh
Nailbed pressure
(only as last resort)
Sensation: awake assessment
Light touch (sufficient unless pt needs spinal checks)
Normal: feels the same in all 4 extremities
Abnormal: any asymmetry
How to assess:
Touch pt once lightly on R arm, then L, then ask “does this
feel the same on both sides?” Repeat with legs.
If pt says they feel different, ask “If the good side is 100%,
what percent is the bad side?”
How to report:
Sensation intact in all 4’s
Pt has decreased sensation in RUE
Sensation: comatose assessment
Assessed during level of consciousness/motor

47
Cerebellum: awake assessment
Normal: accurate, smooth, quick movements
Abnormal: inaccurate, jerky, slow movements
How to assess:
Face: watch EOM’s for nystagmus, jerky eye movements
Listen to speech for dysarthria
Upper extremities: finger to nose, finger tapping
Dysmetria: horizontal wobbling
Past-pointing: overshooting the mark
Lower extremities: heel to shin, foot tapping
How to report:
Pt has normal finger to nose and heel to shin
Pt with dysmetria on R finger to nose
Cerebellum: comatose assessment
Watch eyes for nystagmus and jerky movements
Comatose Patient Assessment Recap
1. Observe meds, vitals
2. Observe patient
3. Level of consciousness/motor
4. Cranial nerves

48
Comatose Patient Assessment Recap
MEDS AND VITALS
Pause sedation if possible (propofol for 5 minutes,
versed for 15)
Keep in mind if pt had any long acting sedatives
Vitals are part of your brainstem exam! (medulla)
HR: bradycardia can indicate increased ICP,
tachycardia/arrhythmia can indicate pain or severely
increased ICP
BP: unusual HTN can indicate rebleed or stroke
RR: are they overbreathing the vent? (they may have the
capacity to if you turn the mandatory rate down…) If not,
they may be braindead…
Comatose Patient Assessment Recap
OBSERVE PATIENT
Take off sheets to observe spontaneous movements
or seizure-like activity
Notice if patient’s HR or BP goes up when they hear
you talking—it’s possible a patient who looks
comatose can hear you talking
Comatose Patient Assessment Recap
LEVEL OF CONSCIOUSNESS/MOTOR
Voice
↓
Shout
↓
Shake
↓
Central Pain
↓
Peripheral Pain
LOCALIZES
WITHDRAWS
FLEXES
EXTENDS
NO
RESPONSE/TRIPLE
FLEXION

49
Comatose Patient Assessment Recap
CRANIAL NERVES
Pupils (2, 3)
Threat (2)
Eye position (3)
Oculocephalic (3, 4, 6, 8)
Corneals (5, 7)
Cough (9, 10)
Vitals (10)
Findings of Increased ICP
Earliest: Decreasing LOC, loss of orientation, forgetful,
restless
Early: Headache, nausea, vomiting, blurred/
double vision, sudden quietness
Later: pupils more sluggish, unequal, enlarging,
worsening motor exam
Late: dilated fixed pupils, posturing, unarousable to
deep pain, losing corneals, blood pressure, HR,
irregular respirations
Cushing’s triad: bradycardia, HTN, irregular respirations
Spinal Assessment
Only done if specially ordered
Typical patients:
Spinal cord injury
Polytrauma, head trauma
s/p back surgery
Consists of:
Motor exam
Sensory exam
50
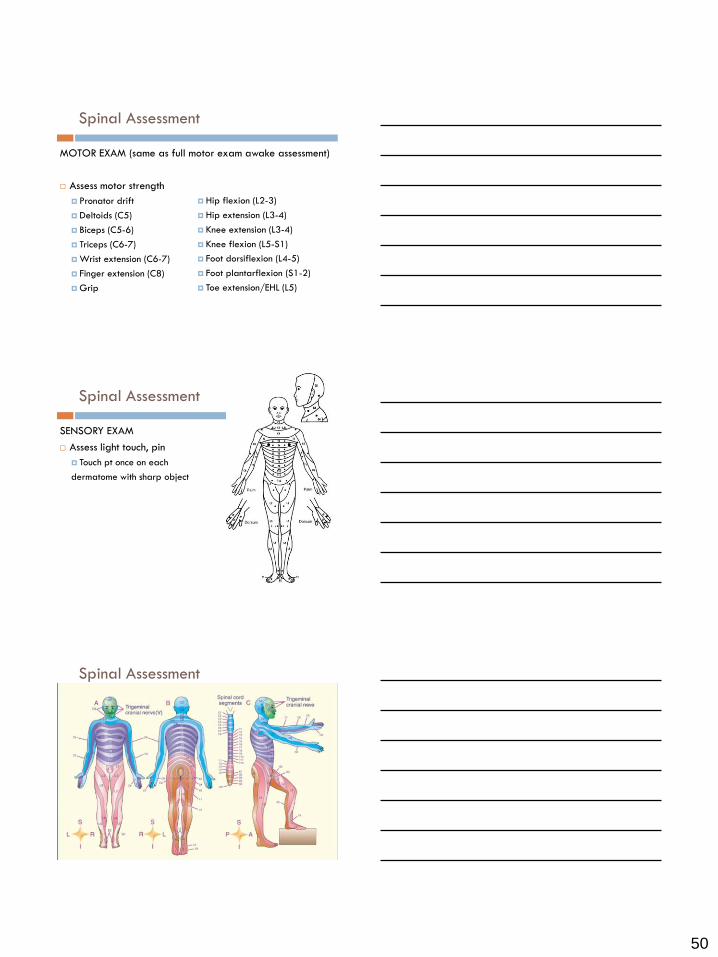
Spinal Assessment
MOTOR EXAM (same as full motor exam awake assessment)
Assess motor strength
Pronator drift
Deltoids (C5)
Biceps (C5-6)
Triceps (C6-7)
Wrist extension (C6-7)
Finger extension (C8)
Grip
Hip flexion (L2-3)
Hip extension (L3-4)
Knee extension (L3-4)
Knee flexion (L5-S1)
Foot dorsiflexion (L4-5)
Foot plantarflexion (S1-2)
Toe extension/EHL (L5)
Spinal Assessment
SENSORY EXAM
Assess light touch, pin
Touch pt once on each
dermatome with sharp object
Spinal Assessment
Hip flexion (L2-3)
Hip extension (L3-4)
Knee extension (L3-4)
Knee flexion (L5-S1)
Foot dorsiflexion (L4-5)
Foot plantarflexion (S1-2)
Toe extension/EHL (L5)

51
When your patient’s exam changes
THINK:
What do I see?
What does it mean?
How does it relate to my baseline/previous exams?
Should I call somebody?
Who should I call?
What now?
PRACTICE, PRACTICE, PRACTICE
Find a system that works for you and memorize it
You can complete a focused neuro exam that tells you
everything you need to know about that patient’s
neurologic status in a few minutes
Always report changes, even if you’re not sure if it’s
significant
Don’t be afraid to ask questions
Don’t be afraid to call up the chain of command
Don’t be afraid to call my cell phone 650-906-9521 or
email me [email protected]
TIME IS BRAIN!
52
Remember, it’s all about our patients
Mr. C. was in NCSE x 73
days.
He underwent treatment
with ativan, valium,
clonazepam, versed,
propofol, phenytoin,
topamax, lacosamide,
depakote, phenobarbital,
pentobarbital, keppra,
lamictal, isoflurane,
lidocaine, ECT, ketamine,
hypothermia,
immunosuppressants, and
epilepsy surgery. The
ketogenic diet stopped his
seizures within 24 hours.
Thank you!
Cassia Chevillon
Laura Dibsie
Patricia Graham
Juana Burkhart
Mobe Montesa
Shannon Hall
Margarita Baggett
Filissa Casserta, Betsy Zink and all the Hopkins NCCU and
University of Maryland Shock Trauma RN’s
UCSD Departments of Surgery, Neurosciences, Anesthesia
Level of consciousness: GCS. Awake/lethargic/obtund/stupor.
Orientation: Name? Date? Place? What brought you in?
Language: Fluency? Name watch, pen. Commands. Repetition.
Neglect: Tactile? Spatial?
Cranial Nerves: Pupils. Visual fields. Acuity. Eye & lid position.
EOMs. Facial sensation. Facial strength. Hearing. Speech.
Cough. Shrug. Head turn. Tongue protrusion.
Motor: Pronator drift. Deltoids. Biceps. Triceps. Grip. Hip flex.
Hip ex. Knee flex. Knee ex. Dorsi/Plantarflex. EHL.
Sensation: Light touch in all 4’s.
Cerebellum: Finger to nose. Heel to Shin.
Complete neuroassessment: awake

53
Vitals
Observe patient
Level of consciousness/motor: voice/shout/shake/painful
stim to see if pt
localizes/withdraws/flexes/extends/nothing
Cranial nerves: Pupils. Threat. Eye position. Oculocephalic.
Corneals. Cough.
Complete neuroassessment: comatose





























