




Edwards Enhanced Surgical Recovery

ESR = 4 phases to implement the enhanced surgical recovery
WHY an ESR program
“No monitoring device no matter how accurate or insightful will
improve outcome unless its is coupled to a treatment which
itself improves outcome”
Michael Pinsky

ESR Program
Phase 1 Phase 2 Phase 3 Phase 4
Select Surgical
Procedures
Build core team Train and develop
competencies
Analyze morbidity rates
and / or length of
hospital stay
Assess current
morbidity rate and / or
length of hospital stay
Choose PGDT treatment
protocol
Establish PGDT as a
new SOP and add to
checklist
Measure clinical and
economic outcome
benefit
Estimate the potential
clinical and economic
benefits of PGDT
Choose a hemodynamic
monitoring platform
Quantify and track
compliance
Publish your results both
internally and / or
externally
Assess Align Apply Measure
3

Owner and tools Steps
Clinical champion Review applicable procedure list
Consider extending PGDT to other medium or high risk
procedures
Review where other institutions have applied PGDT
ASSESS

Patient risk assessment can be based on ASA score,
PPOSUM score, or other surgical score tools.
ASSESS
High Risk
Patients who are “expected” to develop significant complications
At Risk
Patients who “could” develop complications
Of note
Consider applying PGDT for ASA risk score of 2b
+ 1 comorbidity or higher

Applicable Procedures List Sample Procedure Lists
ASSESS
Tools

Owner and tools Steps
Clinical champion
and/or quality person
Identify a reliable data source for hospital metrics
Understand the available data reporting capabilities
ASSESS

Specifying the types of complications to measure before and after
PGDT implementation can help to ensure a direct comparison.
ASSESS
Key metrics
Morbidity
Length of stay
Variable cost per case
Other metrics to consider tracking
Mortality
30-day readmission rate
Patient satisfaction score
Return on investment

ASSESS
Consider if the hospital tracks and can report on the following measures:
Post-Op Mechanical Ventilation > 24h Renal failure requiring dialysis
Hypotension requiring pharmacological treatment Upper gastro-intestinal bleed
Cardiac arrhythmia requiring pharmacological treatment Anastomotic leak (GI surgery)
Wound infection Paralytic ileus
Abdominal infection (GI surgery) Length of stay
Urinary tract infection ICU Admission
Bacterial pneumonia Duration of ICU stay (if ICU admission)
Deep Vein Thrombosis (DVT) Post-operative mechanical ventilation
Pulmonary embolism Lactate at end of surgery or at ICU admission
Pulmonary edema Maximum ICU lactate
Myocardial infarction Re-intervention
Cardiac arrest (exclusive of fatal outcome) Maximum ICU Sequential Organ Failure Assessment (SOFA) score
(or any other organ failure score)
Postoperative delirium Cumulative ICU Therapeutic Intervention Scoring System (TISS)
score (or any other resource utilization score)
Stroke

Hospital Data Form
ASSESS
Tools

Owner and tools Steps
Clinical champion
and/or quality person
Inputs hospital data into Benefit Estimator to calculate
potential improvement in clinical and economic outcomes
based on results from published literature
ASSESS
PGDT Benefits Estimator Business Case Template
ASSESS
Tools
PGDT Literature


ESR Program
Phase 1 Phase 2 Phase 3 Phase 4)
Select Surgical
Procedures
Build core team Train and develop
competencies
Analyze morbidity rates
and / or length of
hospital stay
Assess current morbidity
rate and / or length of
hospital stay
Choose PGDT
treatment protocol
Establish PGDT as a
new SOP and add to
checklist
Measure clinical and
economic outcome
benefit
Estimate the potential
clinical and economic
benefits of PGDT
Choose a
hemodynamic
monitoring platform
Quantify and track
compliance
Publish your results both
internally and / or
externally
Assess Align Apply Measure
16

Owner and tools Steps
Clinical champion Builds a cross-functional, action-oriented team
Team members should be chosen on their abilities to
support the projects needs
Complete the Project Charter helping to define the
program goals
ALIGN
Hemodynamic Optimization through
Perioperative Goal-Directed Therapy
Why and How?
Dr X
Hospital Y

Owner and tools Steps
Clinical champion or
clinical leads
Review protocol summaries which have demonstrated
benefit
Discussion amongst the core team to decide
Possibility to compare with other institutions
ALIGN
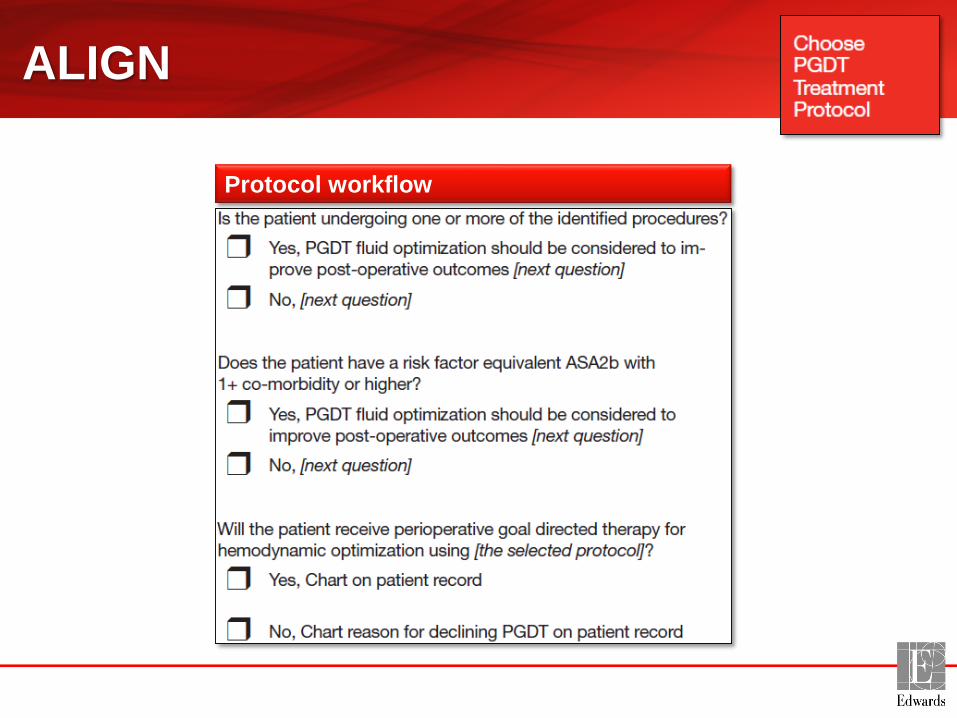
ALIGN
Protocol workflow

ALIGN
Owner and tools Steps
Clinical champion
and/or clinical lead
Base monitoring platform designation on patient risk profile
A-line based monitoring can be utilized when arterial line
placement is necessary
Non-invasive monitoring can be used when no arterial line
is needed

Make sure you are aligned

ESR Program
Phase 1 Phase 2 Phase 3 Phase 4
Select Surgical
Procedures
Build core team Train and develop
competencies
Analyze morbidity rates
and / or length of
hospital stay
Assess current morbidity
rate and / or length of
hospital stay
Choose PGDT treatment
protocol
Establish PGDT as a
new SOP and add to
checklist
Measure clinical and
economic outcome
benefit
Estimate the potential
clinical and economic
benefits of PGDT
Choose a hemodynamic
monitoring platform
Quantify and track
compliance
Publish your results both
internally and / or
externally
Assess Align Apply Measure

APPLY
Owner and tools Steps
Clinical champion or
clinical leads
Initial Team Meeting – reveal ‘The Plan’
Training – protocol / compliance / device
Reconnaissance visit to the OR

END OF SURGERY
VASOPRESSORS / INOTROPS RECORDED
ON FORM
ADDITIONAL FLUIDS RECORDED
ALL EVENTS RECORDED DOWNLOAD EV1000 DATA
TO USB STICK
BEFORE INDUCTION
PATIENT DATA ENTERED IN EV1000
USB STICK INSERTED INTO EV1000
ZERO FLOTRAC / MONITOR
CROSS CHECK DATE/TIME ON EV1000
BEFORE PATIENT ARRIVES
ADDITIONAL INFUSION PUMP
FLOTRAC TRANSDUCER
ADD PARAMETERS TO ANESTHETIC
RECORD
EV1000 STAND / DATA BOX / CABLES
50ML LEURLOCK SYRINGE
APPLY

Compliance depends on:
1. Understand the ‘how’ of
compliance
2. Follow the protocol
completely
3. Record ‘what they did’
accurately
APPLY

PHASE 1 only begins when first ABG taken and first skin incision
PHASE 1 - Climbing phase
• EV1000 data entered
• CHECK EV1000 DATE / TIME CORRECTED – USE EV1000 TIME THROUGHOUT OPTIMISATION
• FLOTRAC sensor zero / level
• Insert EV1000 memory stick
• Baseline SV / SBP / DBP / MAP values and time recorded
• CLIMBING:
– 1st COLLOID BOLUS (ALWAYS 250 ml x Tetraspan)
– Increase in SV > 10%
• YES – 2nd COLLOID BOLUS
• NO – MONITOR SV (NOTE THIS AS TRIGGER VALUE ON FORM)
– Increase < 10%
• YES – MONITOR SV
• NO – go back to a)
APPLYCompliance SOP Example

PHASE 2 - Cruising phase
• Monitor SV
• If SV < TRIGGER
– 1st COLLOID BOLUS (ALWAYS 250 ml x Tetraspan)
– Increase in SV > 10%
• YES – 2nd COLLOID BOLUS
• NO – MONITOR SV
– Increase < 10%
• YES – MONITOR SV
• NO – go back to a)
APPLYCompliance SOP Example
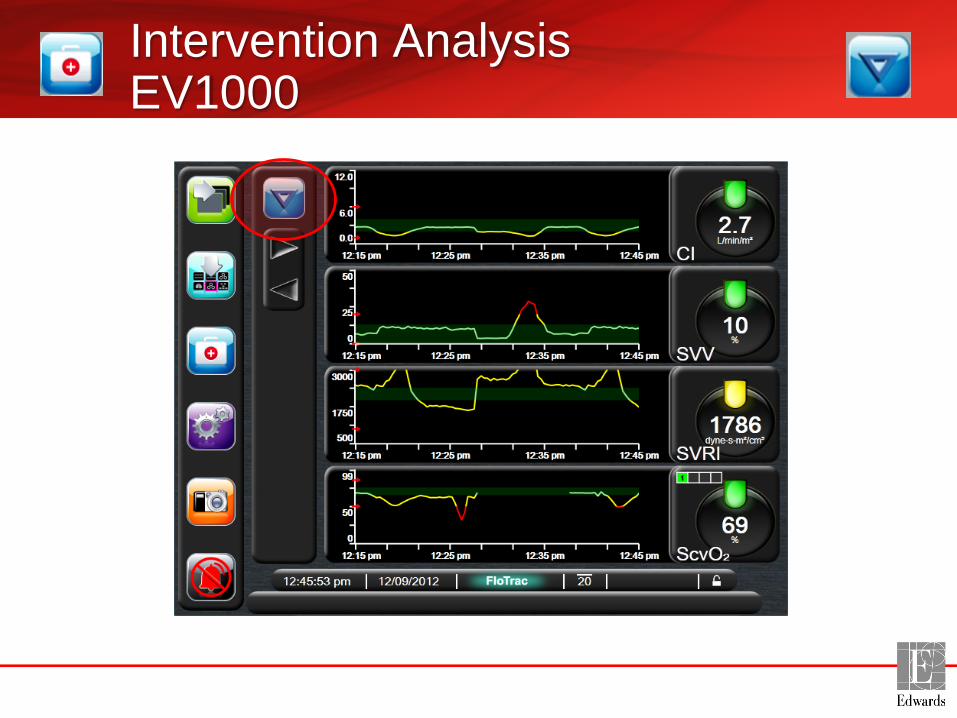
Intervention AnalysisEV1000

Intervention AnalysisEV1000

Intervention AnalysisTrack % Change

Apply successful recipe!

ESR Program
Phase 1 Phase 2 Phase 3 Phase 4
Select Surgical
Procedures
Build core team Train and develop
competencies
Analyze morbidity
rates and / or length of
hospital stay
Assess current morbidity
rate and / or length of
hospital stay
Choose PGDT treatment
protocol
Establish PGDT as a
new SOP and add to
checklist
Measure clinical and
economic outcome
benefit
Estimate the potential
clinical and economic
benefits of PGDT
Choose a hemodynamic
monitoring platform
Quantify and track
compliance
Publish results
internally and / or
externally
Assess Align Apply Measure

Measuring results…

ESR Program Status
ASSESS ALIGN APPLY MEASURE
Number of
Hospitals84 56 40 6
Countries

Main surgery type COLON
Driven by Anaesthetist (primarely) & Surgeon
Number of patients 100
Protocol used SVV
Results / experience so far Very positive feedback from both anesthetist
and surgeon
Next steps Measure complication rate after one year with
protocol
Some examplesGermany: Eberswalde

Some examplesItaly: Ospedale Molinette, Torino
Main surgery type UPPER GI (Pancreatectomy-Gastrectomy)
Driven by 2 Anesthetists + OR nurses + surgical team
Protocol used Kuper (NICE)
Results / experience so
far
- Changes behavior in fluid mangement
- Less or more fluids but in different timing
- Patient’s outcome seems better
Next steps - Goal :100 patients and check (B/A)
-Extend to different patient population (Kidney)
-Peer to Peer education

Main surgery type VASCULAR (AAA; ThAAA; Leriche; P-
POSSUM>5% ; ASA IV)
Driven by Surgeon + chief of Anaesthesia + 3
anaestetists
Protocol used PUVAS protocol (Pomeranian University
VAScular)
Technology Used Non Invasive- Avoiding Arterial line
Results / experience so far - Reduction in complication ratio, cost of
treatment and LOS
Next steps - Goal :240 patients and check (B/A)
- Publish on complications & costs
Some examplesPoland: Szczecin
ESR Program Key Learnings
Right patient population
Motivatedchampion /
team
Keep it simpleStart small
(1 procedure)
ASK for support
Others may have done it before !

Edwards Confidential - Internal Use Only. Do not reproduce or distribute.
For professional use. See instructions for use for full prescribing information, including indications, contraindications, warnings,
precautions and adverse events.
Edwards Lifesciences devices placed on the European market meeting the essential requirements referred to in Article 3 of the Medical Device
Directive 93/42/EEC bear the CE marking of conformity.
Edwards, Edwards Lifesciences, the stylized E logo, Enhanced Surgical Recovery Program and EV1000 are trademarks of Edwards Lifesciences
Corporation. All other trademarks are the property of their respective owners.
© 2014 Edwards Lifesciences Corporation. All rights reserved. E5306/11-14/CC

Helping Patients is Our Life’s Work, and





























