CME Program for Family CME Program for Family
PhysiciansPhysicians
Ambulatory BP MonitoringAmbulatory BP Monitoring
Brian Gore, MD CCFP Dip Epid.Brian Gore, MD CCFP Dip Epid.
2004 Series 2004 Series

CME Program for Family CME Program for Family
PhysiciansPhysicians Ambulatory BP Ambulatory BP
MonitoringMonitoring
Brian Gore, MD CCFP Dip Epid.Brian Gore, MD CCFP Dip Epid.
Part IPart IEpidemiology Epidemiology
OBP Measurement OBP Measurement

PREVALENCE PREVALENCE ofof
HIGH BLOOD PRESSURE HIGH BLOOD PRESSURE
Whole Population Whole Population 15%15%
Subjects > 65 years Subjects > 65 years 30%30%

Canadian data on Canadian data on hypertensionhypertension::
22% PREVALENCE 22% PREVALENCE (4.2 million people)(4.2 million people)
16% are controlled (<140/90) 16% are controlled (<140/90) 39% 39% (40%)(40%)
23% treated but not controlled 23% treated but not controlled (60%)(60%)
19% aware but not treated 19% aware but not treated 61%61%
42% are unaware42% are unaware
Adapted from: Adapted from: Am J HypertensAm J Hypertens 1997; 10:1097-1102. 1997; 10:1097-1102.

What are the controversies in What are the controversies in office blood pressure office blood pressure
measurements?measurements?

Common Errors in Blood Common Errors in Blood Pressure EvaluationPressure Evaluation
Observer BiasObserver Bias Technique FailuresTechnique Failures Equipment ErrorEquipment Error

Observer BiasObserver Bias
habitually reading higher or lower than habitually reading higher or lower than actual pressureactual pressure
terminal digit preference (150/90)terminal digit preference (150/90) bias for normal valuesbias for normal values prejudice against certain valuesprejudice against certain values variable speed of observer reactionvariable speed of observer reaction differences in interpretation of Korotkoff differences in interpretation of Korotkoff
soundssounds Bailey RH, Arch Int Med: 1993, 152:2741-2748Bailey RH, Arch Int Med: 1993, 152:2741-2748 Pickering TG, Lancet:1994,344:31-35Pickering TG, Lancet:1994,344:31-35
Technique FailuresTechnique Failures
no rest period prior to BP measureno rest period prior to BP measure one arm, one position measuresone arm, one position measures inappropriate cuff sizeinappropriate cuff size poor environmental control: talking, tense.poor environmental control: talking, tense. inappropriate rate of deflationinappropriate rate of deflation
Bailey RH, Arch Int Med: 1993, 152:2741-2748Bailey RH, Arch Int Med: 1993, 152:2741-2748 Pickering TG, Lancet:1994,344:31-35Pickering TG, Lancet:1994,344:31-35

Equipment ErrorEquipment Error
mercury devices not calibrated or faulty mercury devices not calibrated or faulty componentscomponents
aneroid devices as aboveaneroid devices as above mechanical and electrical devices: mechanical and electrical devices:
numerous potential problemsnumerous potential problems
Bailey RH, Arch Int Med: 1993, 152:2741-2748Bailey RH, Arch Int Med: 1993, 152:2741-2748 Pickering TG, Lancet:1994,344:31-35Pickering TG, Lancet:1994,344:31-35

CHS Recommended Technique CHS Recommended Technique for Measuring BPfor Measuring BP

2000 Canadian Recommendations for the Management of Hypertension
Recommended Technique for Measuring Blood Pressure
Standardized technique:
• Have the patient rest for 5 minutes
• Use an appropriate cuff size
• Use a mercury manometer or a recently calibrated electronic device

• Patient seated, feet on floor, back against wallPosition cuff appropriately• Increase pressure rapidly• Support arm at heart level• Exclude possibility of auscultatory gap by increasing cuff pressure rapidly to 30 mmHg above level of disappearance of radial pulse• Place stethoscope over the brachial artery
Recommended Technique for Measuring Blood Pressure (cont.)

Recommended Technique for Measuring Blood Pressure (cont.)
• Drop pressure by 2 mmHg / beat:- appearance of sound (phase I Korotkoff) = SBP- disappearance of sound (phase V Korotkoff) =
DBP• Take 2 blood pressure measurements, 1 minute apartMeasure BP in both arms, different positionsRepeated visits (3-5)
THE PINHOLING EFFECT THE PINHOLING EFFECT OF OBP MEASUREMENTOF OBP MEASUREMENT

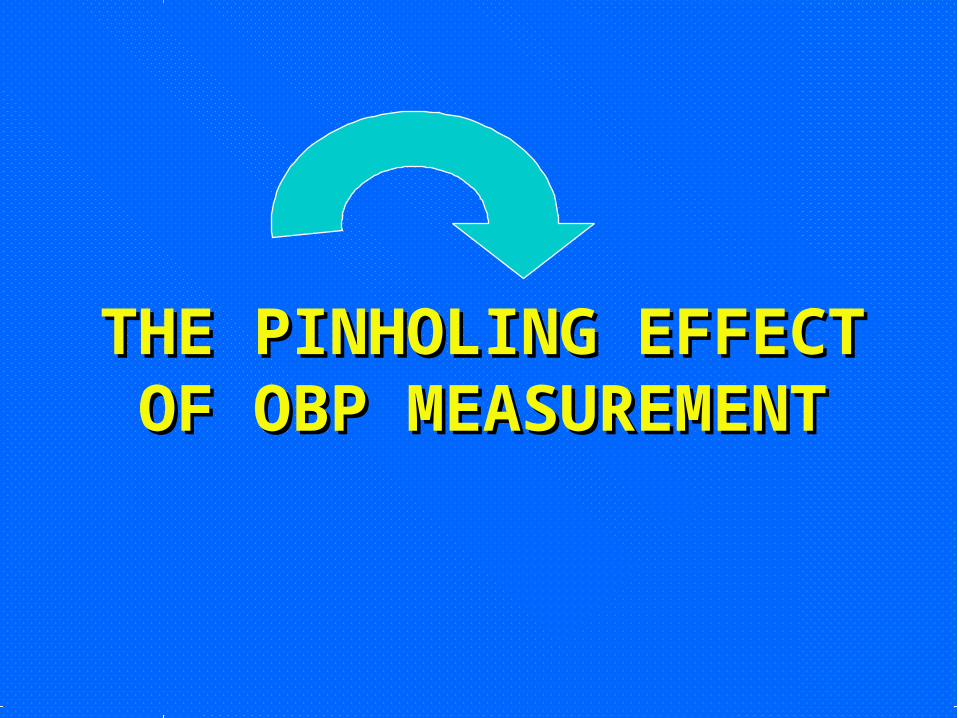
Casual OBP: representative?

Casual OBP: representative?
Casual OBP: representative?

CASUAL OFFICE CASUAL OFFICE READINGSREADINGS
repeated visits, blood pressure repeated visits, blood pressure variability, common errorsvariability, common errors

Casual Blood PressureCasual Blood Pressure
“just the tip of the iceberg”“just the tip of the iceberg”

24 hour ABP: representative?
Event-Based Cohort Studies Event-Based Cohort Studies with ABPMwith ABPM
cardiovascular disease risk ABP > OBPcardiovascular disease risk ABP > OBP
Perloff et al. 1983Perloff et al. 1983 Zweiker et al. 1994Zweiker et al. 1994 Ohkubo et al. 1997Ohkubo et al. 1997 Nakano et al. 1998Nakano et al. 1998 Yamamoto et al. 1998Yamamoto et al. 1998
Redon et al. 1998Redon et al. 1998 Verdecchi et al. 1998Verdecchi et al. 1998 Khattar et al. 1999Khattar et al. 1999 Staessen et al. 1999Staessen et al. 1999 Verdecchi et al. 2002Verdecchi et al. 2002

24 HOUR ABPM24 HOUR ABPM

Which BP is representative?Which BP is representative?

Which BP is representative?Which BP is representative?

Inherent Variability of BP

Reflective moment.…..Reflective moment.…..• Daily average no. of heartbeats: 103,680 Daily average no. of heartbeats: 103,680 • No of beats per OBPM: <15No of beats per OBPM: <15• Sampling ratio is 1:6912 or .0145%Sampling ratio is 1:6912 or .0145%• Clinical decision in 3 to 5 office visitsClinical decision in 3 to 5 office visits• Include the BP variabilityInclude the BP variability• Include the other common errors in BP Include the other common errors in BP
measurementmeasurement• Include the concept of WCE/WCHInclude the concept of WCE/WCH

What is your level of What is your level of confidence that you have confidence that you have
representative BP representative BP measurements upon which you measurements upon which you
can make a clinical and can make a clinical and therapeutic decision??therapeutic decision??

Inaccurate DiagnosisInaccurate Diagnosis
ImplicationsImplications
Inappropriate TreatmentInappropriate Treatment