


Community based Management of Acute Malnutrition
Module 1: Introduction
Dr. M. Najeeb Piracha

CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
2
2 IIInnntttrrroooddduuuccctttiiiooonnn
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
3
3 IIInnntttrrroooddduuuccctttiiiooonnn
Table of Contents OBJECTIVES OF THIS MODULE ................................................................................................................. 4
Introduction ............................................................................................................................................ 5
Malnutrition ............................................................................................................................................ 7
UNDERNUTRITION ............................................................................................................................... 7
MALNUTRITION AND SOME DEFINITIONS ............................................................................................ 8
ACUTE MALNUTRITION ........................................................................................................................ 8
Acute Malnutrition: Criteria ................................................................................................................. 9
Micronutrient deficiencies ................................................................................................................. 10
COMMUNITY BASED MANAGEMENT OF ACUTE MALNUTRITION (CMAM) ............................................. 11
LOGICAL BASIS OF CMAM. ................................................................................................................. 11
Advantages of community therapeutic care ....................................................................................... 11
Four Components of CMAM .............................................................................................................. 12
Organization of CMAM ...................................................................................................................... 12
Setting up CMAM in a Community ..................................................................................................... 12
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
4
4 IIInnntttrrroooddduuuccctttiiiooonnn
OBJECTIVES OF THIS MODULE
1. To identify global and national effects of malnutrition
2. To understand malnutrition and acute malnutrition
3. To comprehend the principles behind CMAM
4. To learn components of CMAM
5. To explore how different components of CMAM work
together
6. Field visit to Stabilization Center
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
5
5 IIInnntttrrroooddduuuccctttiiiooonnn
Introduction
Situation in Pakistan
The level of socioeconomic development is low in Pakistan; human development index is 142nd in the world and 24% of the population lives below poverty line with 17% earning less than a dollar a day1. The health profile of Pakistan is characterized by high population growth rate, high infant mortality and child mortality rates of 78 and 97 respectively2, a high maternal mortality ratio of 320 per 100,000 live births1 and a high burden of communicable diseases. All this is visibly evident in Province Sindh as well.
Nutritional assessment
Several large and small scale nutritional surveys3 have been conducted and all point towards serious systemic deficits in nutritional status. At the national level, 24% of the population is under the calorie based food plus non-food poverty line and more than 41% children less than 5 are under weight for their age. Over half the children are affected by stunting and about 9% by wasting4. Sindh has the greatest prevalence of malnutrition, 49.4% of children under 5 are underweight while prevalence of stunted children is 44.2%5. A recent study of 1407 households in two districts in Sindh conducted by Action against Hunger has placed the prevalence of acute malnutrition at 22%6.
The chain of events
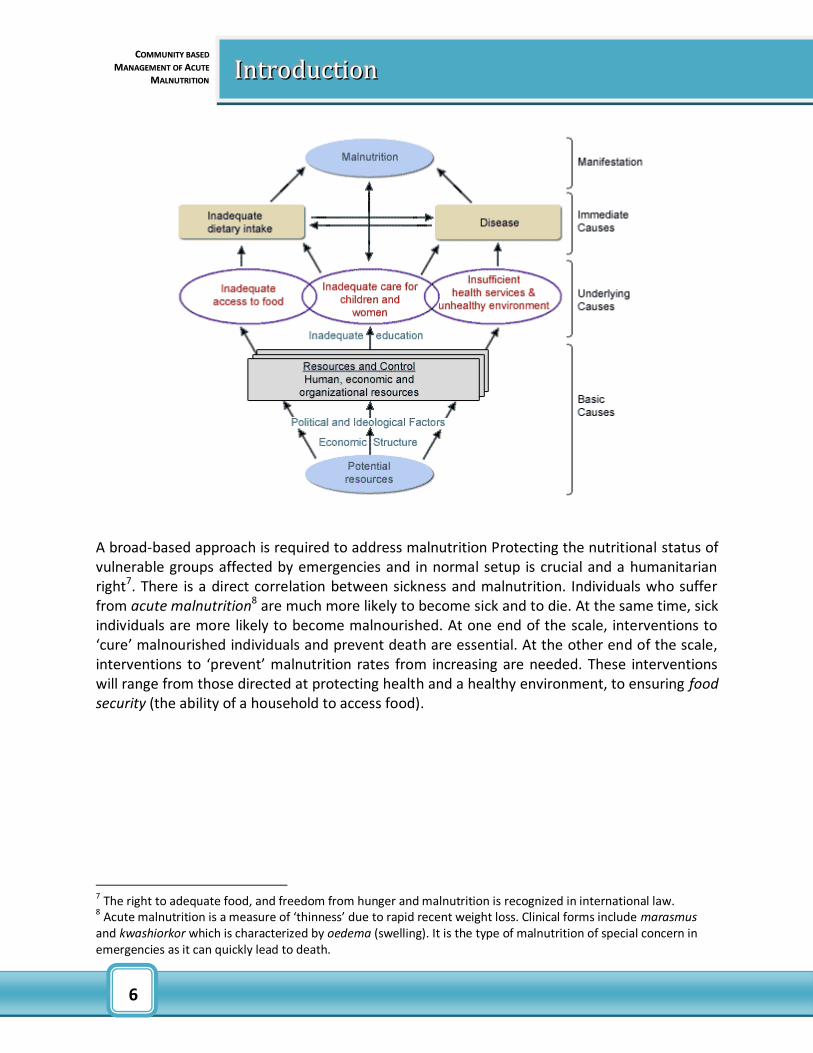
Malnutrition does not result simply from lack of food but from a complex mix of factors. Emergencies have an impact on a whole range of factors that can increase the risk of malnutrition, illness (morbidity) and death (mortality). These factors work on a number of levels affecting populations, households and finally individuals. Unicef’s conceptual framework on malnutrition explains the chain of events. Three levels of causes of child malnutrition are detailed:
child malnutrition, death and disability are the manifestation of a problem;
inadequate dietary intake, disease are the immediate causes;
the underlying causes are insufficient access to food, inadequate maternal and child-care practices, poor water/sanitation and inadequate health services.
1 World Health Statistics, 2008 2 Pakistan Demographic Health Survey(PDHS) 2007 3 National Nutrition Survey, 2001 – 2002, Unicef,
4 Pakistan MDG report, 2006 GoP
5 National Nutrition Survey 2001-2002, Unicef
6 Nutritional Assessment on Flood-Affected Populations Kamber-Shahdadkot and Dadu Districts, Sep, 2007
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
6
6 IIInnntttrrroooddduuuccctttiiiooonnn
A broad-based approach is required to address malnutrition Protecting the nutritional status of vulnerable groups affected by emergencies and in normal setup is crucial and a humanitarian right7. There is a direct correlation between sickness and malnutrition. Individuals who suffer from acute malnutrition8 are much more likely to become sick and to die. At the same time, sick individuals are more likely to become malnourished. At one end of the scale, interventions to ‘cure’ malnourished individuals and prevent death are essential. At the other end of the scale, interventions to ‘prevent’ malnutrition rates from increasing are needed. These interventions will range from those directed at protecting health and a healthy environment, to ensuring food security (the ability of a household to access food).
7 The right to adequate food, and freedom from hunger and malnutrition is recognized in international law.
8 Acute malnutrition is a measure of ‘thinness’ due to rapid recent weight loss. Clinical forms include marasmus
and kwashiorkor which is characterized by oedema (swelling). It is the type of malnutrition of special concern in emergencies as it can quickly lead to death.
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
7
7 IIInnntttrrroooddduuuccctttiiiooonnn
Malnutrition Malnutrition comprises both undernutrition and overnutrition.
UNDERNUTRITION
Undernutrition is defined as the outcome of insufficient food intake and repeated infectious diseases and can take the form of:
Wasting (dangerously thin for one’s height)
Stunting (too short for one’s age)
Underweight (being underweight for one’s age)
Micronutrient deficiencies (deficient in vitamins and minerals) All four types of undernutrition can overlap in the same child. Undernutrition in all its forms is a considerable public health apprehension and an underlying factor in over 50 percent of the deaths from preventable causes among children under 5 each year globally. Malnutrition comprises both overnutrition (obesity) and undernutrition, but the term malnutrition is often used for forms of undernutrition (e.g., acute malnutrition).
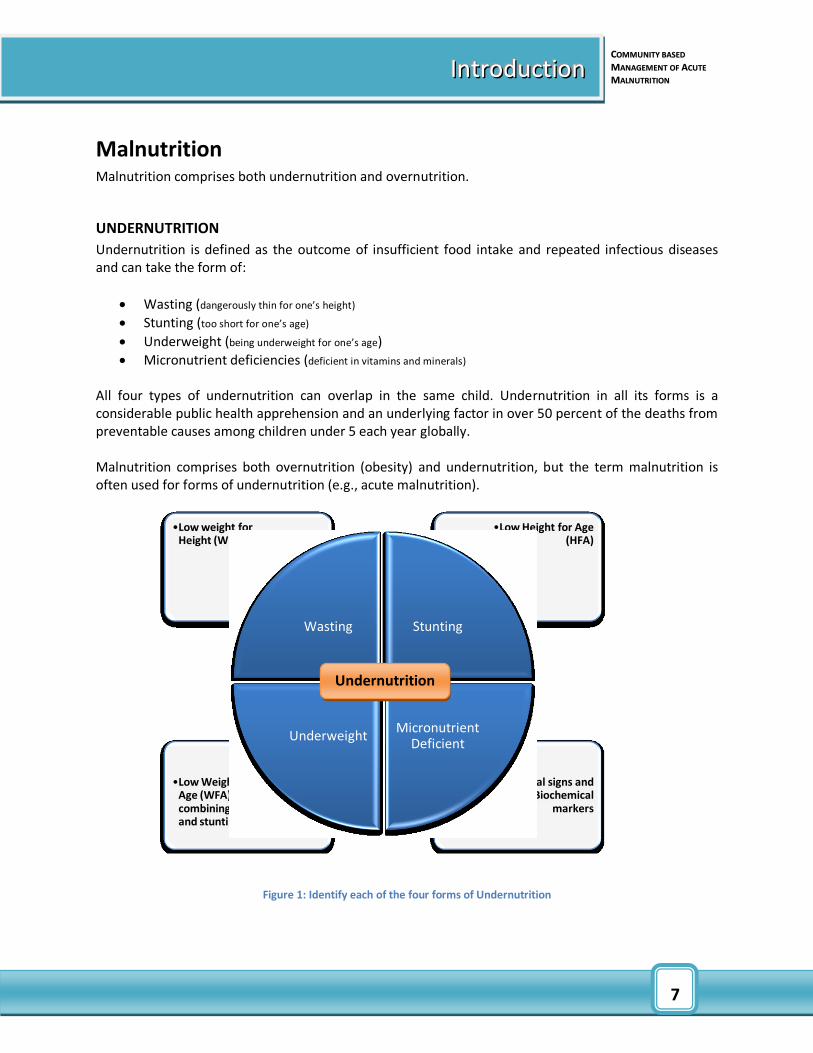
Figure 1: Identify each of the four forms of Undernutrition
•Clinical signs and Biochemical
markers
•Low Weight for Age (WFA). combining wasting and stunting
•Low Height for Age (HFA)
•Low weight for Height (WFH)
Wasting Stunting
Micronutrient Deficient
Underweight
Undernutrition
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
8
8 IIInnntttrrroooddduuuccctttiiiooonnn
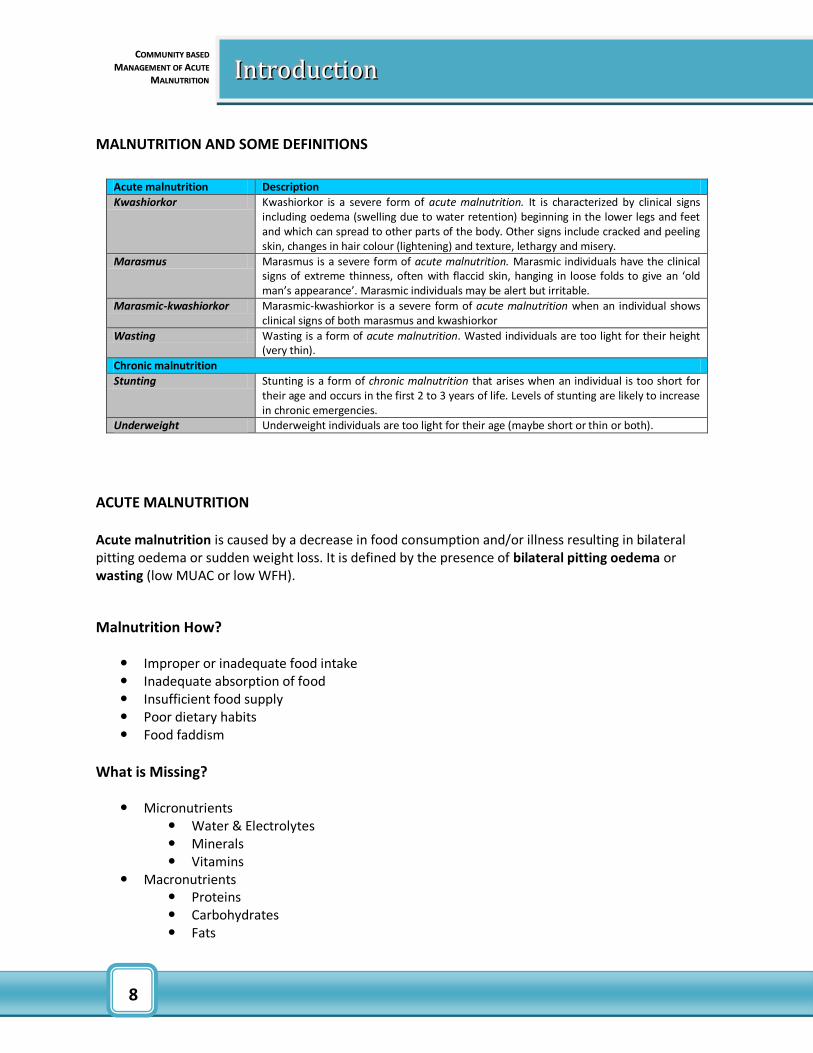
MALNUTRITION AND SOME DEFINITIONS
Acute malnutrition Description
Kwashiorkor Kwashiorkor is a severe form of acute malnutrition. It is characterized by clinical signs including oedema (swelling due to water retention) beginning in the lower legs and feet and which can spread to other parts of the body. Other signs include cracked and peeling skin, changes in hair colour (lightening) and texture, lethargy and misery.
Marasmus Marasmus is a severe form of acute malnutrition. Marasmic individuals have the clinical signs of extreme thinness, often with flaccid skin, hanging in loose folds to give an ‘old man’s appearance’. Marasmic individuals may be alert but irritable.
Marasmic-kwashiorkor Marasmic-kwashiorkor is a severe form of acute malnutrition when an individual shows clinical signs of both marasmus and kwashiorkor
Wasting Wasting is a form of acute malnutrition. Wasted individuals are too light for their height (very thin).
Chronic malnutrition
Stunting Stunting is a form of chronic malnutrition that arises when an individual is too short for their age and occurs in the first 2 to 3 years of life. Levels of stunting are likely to increase in chronic emergencies.
Underweight Underweight individuals are too light for their age (maybe short or thin or both).
ACUTE MALNUTRITION
Acute malnutrition is caused by a decrease in food consumption and/or illness resulting in bilateral pitting oedema or sudden weight loss. It is defined by the presence of bilateral pitting oedema or wasting (low MUAC or low WFH).
Malnutrition How?
Improper or inadequate food intake Inadequate absorption of food Insufficient food supply Poor dietary habits Food faddism
What is Missing?
Micronutrients Water & Electrolytes Minerals Vitamins
Macronutrients Proteins Carbohydrates Fats
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
9
9 IIInnntttrrroooddduuuccctttiiiooonnn
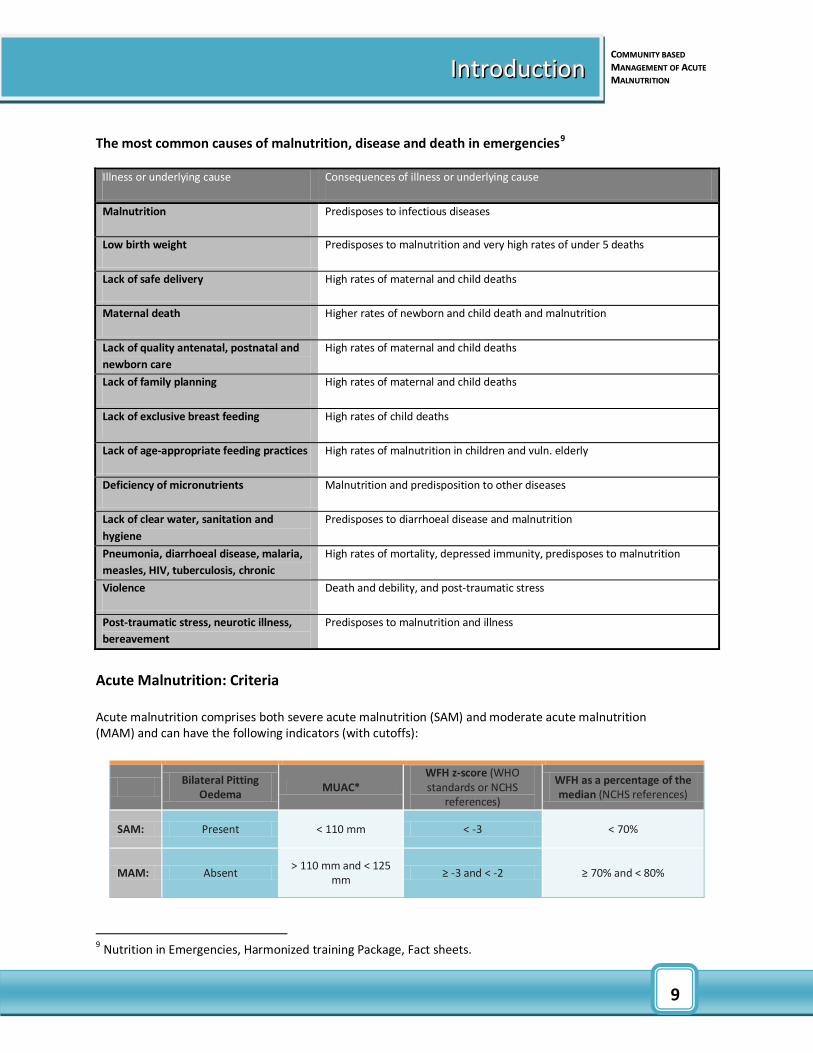
The most common causes of malnutrition, disease and death in emergencies9
Acute Malnutrition: Criteria Acute malnutrition comprises both severe acute malnutrition (SAM) and moderate acute malnutrition (MAM) and can have the following indicators (with cutoffs):
Bilateral Pitting
Oedema MUAC*
WFH z-score (WHO standards or NCHS
references)
WFH as a percentage of the median (NCHS references)
SAM: Present < 110 mm < -3 < 70%
MAM: Absent > 110 mm and < 125
mm ≥ -3 and < -2 ≥ 70% and < 80%
9 Nutrition in Emergencies, Harmonized training Package, Fact sheets.
Illness or underlying cause Consequences of illness or underlying cause
Malnutrition Predisposes to infectious diseases
Low birth weight Predisposes to malnutrition and very high rates of under 5 deaths
Lack of safe delivery High rates of maternal and child deaths
Maternal death Higher rates of newborn and child death and malnutrition
Lack of quality antenatal, postnatal and
newborn care
High rates of maternal and child deaths
Lack of family planning High rates of maternal and child deaths
Lack of exclusive breast feeding High rates of child deaths
Lack of age-appropriate feeding practices High rates of malnutrition in children and vuln. elderly
Deficiency of micronutrients Malnutrition and predisposition to other diseases
Lack of clear water, sanitation and
hygiene
Predisposes to diarrhoeal disease and malnutrition
Pneumonia, diarrhoeal disease, malaria,
measles, HIV, tuberculosis, chronic
disease, physical or mental disability
High rates of mortality, depressed immunity, predisposes to malnutrition
Violence Death and debility, and post-traumatic stress
Post-traumatic stress, neurotic illness,
bereavement
Predisposes to malnutrition and illness

CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
10
10 IIInnntttrrroooddduuuccctttiiiooonnn
Micronutrient deficiencies
Micronutrient deficiencies Iron deficiency (anaemia) Lack of iron eventually results in iron-deficiency anaemia. Typical signs are: paleness, tiredness,
headaches and breathlessness
Vitamin A deficiency (xeropthalmia)
Lack of vitamin A results in xeropthalmia. The signs in order of presentation are: night blindness, Bitots spots (dryness and foamy accumulations on the inner eyelids), corneal xerosis (dullness or clouding of the cornea), keratomalacia (softening and ulceration of the cornea), permanent blindness.
Iodine deficiency (goitre and cretinism)
Iodine deficiency causes a range of abnormalities including goitre (swelling of the thyroid gland in the neck) and cretinism (mental and physical disability)
Vitamin C deficiency (scurvy)
Vitamin C deficiency results in scurvy. Typical signs include: swollen and bleeding gums, minute haemorrhages (bleeding), brittle hair, slow healing of wounds
Niacin deficiency (pellagra)
Niacin deficiency results in pellagra which affects the skin, gastro-intestinal tract and nervous systems. For this reason, it is sometimes called the 3Ds: dermatitis, diarrhoea and dementia. Dermatitis is the most distinctive feature causing redness and itching on areas of the skin exposed to sunlight.
Thiamin deficiency (beri-beri)
Thiamin deficiency results in beri-beri of which there are eight clinically recognisable syndromes.
Riboflavin deficiency Riboflavin deficiency leads to ariboflavinosis, a deficiency disease characterised by angular stomatitis that affects the corners of the mouth which can become split or cracked. Cheilosis, scaling and cracking of the surface of the lips may be seen. Glossitis, inflammation or swelling of the tongue is also sometimes reported.
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
11
11 IIInnntttrrroooddduuuccctttiiiooonnn
Advantages
Simple
Acceptable
Low cost
Accurate
Prolonged care
COMMUNITY BASED MANAGEMENT OF ACUTE MALNUTRITION (CMAM)
LOGICAL BASIS OF CMAM.
Acute malnutrition develops over a relatively short period of time. While more serious physiological consequences of acute malnutrition appear late. As the condition develops, metabolic and immunological consequences become more marked, and treatment becomes more difficult, more costly and more likely to fail. Because treating malnutrition may take a long period of time, Therapeutic Feeding Center programmes often have low coverage and high default rates, and inpatient services are inadequate. If, severe malnutrition is caught in the early stages, the treatment is very simple: all that is required is a balanced diet of sufficient quantity and quality in terms of proteins, carbohydrates, fats and micro-nutrients. Which can be given as a part of home based therapy. CMAM programmes therefore focus on finding and addressing acute malnutrition early in the progression of the condition, before its metabolic and immunological aspects become marked and require inpatient treatment.
Advantages of community therapeutic care
Simplicity : Simple methodology which can be easily managed by non-clinicians in emergency and in non-emergency setting as well. Acceptability : Home based method has greater acceptability among masses as compared to the hospital based management. Cost : Cost towards the patients is greatly reduced. Accuracy : The treatment and therapy is based on reliable results, and hence produce results. Prolonged Care : By ensuring the access of the programme to the patient’s home may result in prolonged presencein programme, while number of defaulters can be reduced.
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
12
12 IIInnntttrrroooddduuuccctttiiiooonnn
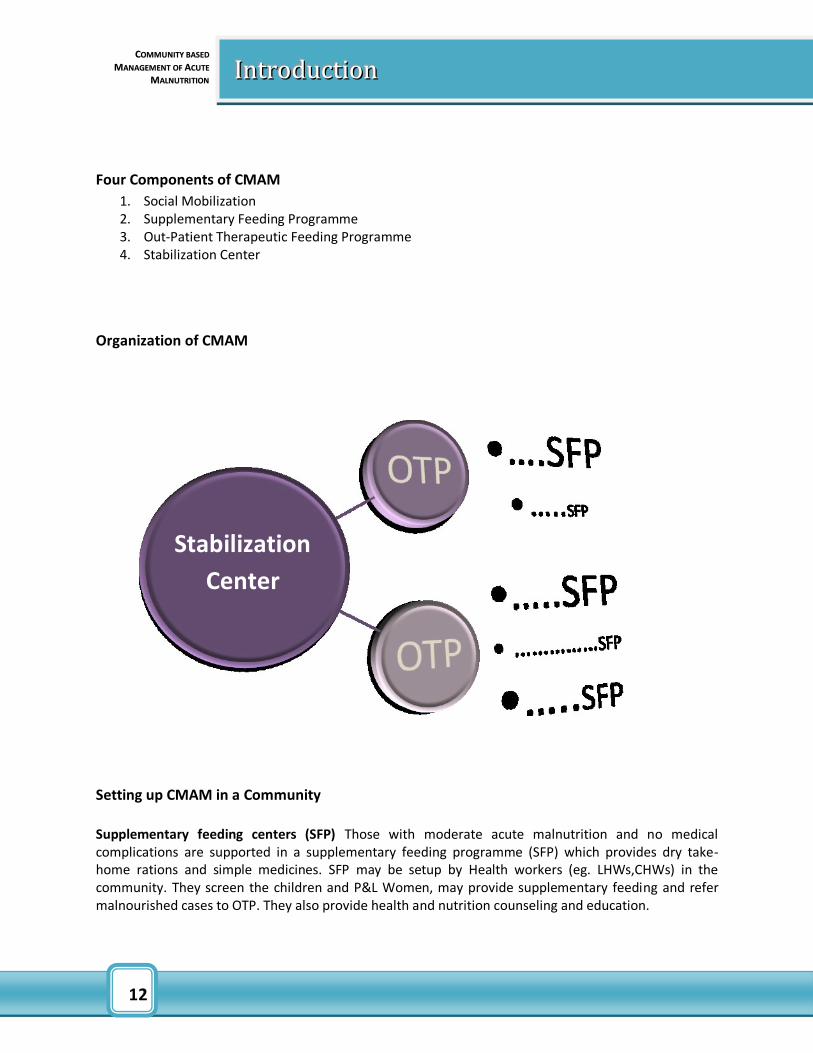
Four Components of CMAM
1. Social Mobilization 2. Supplementary Feeding Programme 3. Out-Patient Therapeutic Feeding Programme 4. Stabilization Center
Organization of CMAM
Setting up CMAM in a Community
Supplementary feeding centers (SFP) Those with moderate acute malnutrition and no medical complications are supported in a supplementary feeding programme (SFP) which provides dry take-home rations and simple medicines. SFP may be setup by Health workers (eg. LHWs,CHWs) in the community. They screen the children and P&L Women, may provide supplementary feeding and refer malnourished cases to OTP. They also provide health and nutrition counseling and education.
Stabilization
Center
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
13
13 IIInnntttrrroooddduuuccctttiiiooonnn
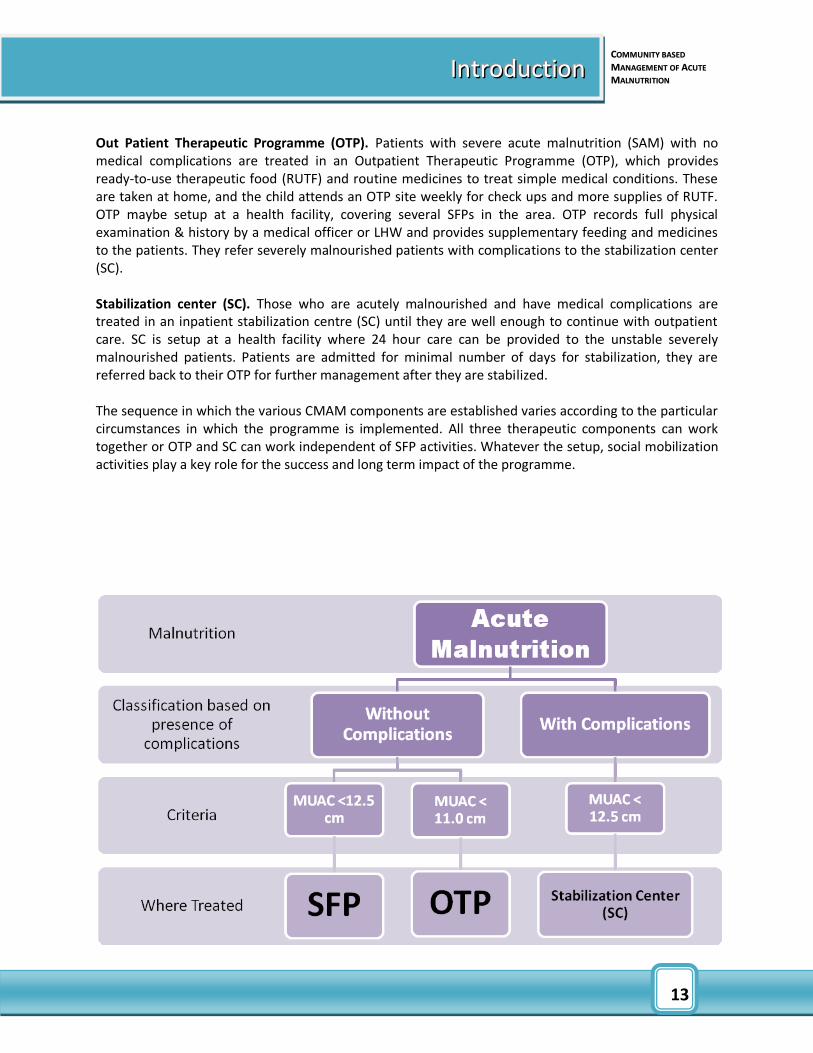
Out Patient Therapeutic Programme (OTP). Patients with severe acute malnutrition (SAM) with no medical complications are treated in an Outpatient Therapeutic Programme (OTP), which provides ready-to-use therapeutic food (RUTF) and routine medicines to treat simple medical conditions. These are taken at home, and the child attends an OTP site weekly for check ups and more supplies of RUTF. OTP maybe setup at a health facility, covering several SFPs in the area. OTP records full physical examination & history by a medical officer or LHW and provides supplementary feeding and medicines to the patients. They refer severely malnourished patients with complications to the stabilization center (SC). Stabilization center (SC). Those who are acutely malnourished and have medical complications are treated in an inpatient stabilization centre (SC) until they are well enough to continue with outpatient care. SC is setup at a health facility where 24 hour care can be provided to the unstable severely malnourished patients. Patients are admitted for minimal number of days for stabilization, they are referred back to their OTP for further management after they are stabilized. The sequence in which the various CMAM components are established varies according to the particular circumstances in which the programme is implemented. All three therapeutic components can work together or OTP and SC can work independent of SFP activities. Whatever the setup, social mobilization activities play a key role for the success and long term impact of the programme.

CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
14
14 IIInnntttrrroooddduuuccctttiiiooonnn
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
15
15 IIInnntttrrroooddduuuccctttiiiooonnn
REFERENCES.
Management of severe malnutrition; a manual for physicians and other senior health workers. WHO,
Geneva.
Training course on the management of severe malnutrition; WHO, Department of Nutrition for Health
and Development.
Community based therapeutic Care. A Field Manual by Valid International. First Edition, 2006.
Community-based Therapeutic Care (CTC). ENN Special Supplement Series, No. 2, November 2004.
Compiled and edited by Tanya Khara & Steve Collins, Valid International
Lancet. Management of severe acute malnutrition in children, by, Steve Collins, Nicky Dent, Paul Binns, Paluku Bahwere, Kate Sadler, Alistair Hallam. Severe Acute Malnutrition, An opportunity to dramatically improve child survival by Steve Collins, Valid International / CIHD. For Royal Society of Tropical Medicine and Hygiene Meeting 20th March 2007.
Community-based management of acute malnutrition, FANTA, Emergency Nutrition Network (ENN) et al. 2004. Module 2 in Infant Feeding in Emergencies (December). www.ennonline.net. WHO, WFP, UN/SCN and UNICEF. 2006. “Informal consultation on the community-based management of severe malnutrition in children,” Food and Nutrition Bulletin, Vol. 27, No. 3 (supplement). www. fantaproject.org. WHO. 2000. Management of Nutrition in Major Emergencies. Geneva: WHO.
SUMMARY OF Community Based Therapeutic Care (CTC) by Dr Steve Collins MBE MD MBBS Director
Valid Nutrition & Valid International.
The sustainability of Community-based Therapeutic Care, (CTC) in non-acute emergency contexts by
Valerie Gatchell, Vivienne Forsythe and Paul-Rees Thomas, Concern Worldwide, 52-55 Camden street,
Dublin 2, Ireland.
Treating Severe acute malnutrition (SAM), 2001 and 2005, Valid international study.
Pakistan National guidelines for CMAM
CCOOMMMMUUNNIITTYY BBAASSEEDD
MMAANNAAGGEEMMEENNTT OOFF AACCUUTTEE
MMAALLNNUUTTRRIITTIIOONN
16
16 IIInnntttrrroooddduuuccctttiiiooonnn
A review of methods to detect cases of severely malnourished children in the community for their
admission into community based therapeutic care programs. Mark Myatt1, Tanya Khara and Steve
Collins
Efficacy and effectiveness of community-based treatment of severe malnutrition, Professor Ann
Ashworth Nutrition and Public Health Intervention Research Unit, London School of Hygiene & Tropical
Medicine, London, UK
Life skills – based hygiene education, Leonie Postma, Renate Getke and Christine van Wijk, IRC Water
and sanitation Center, Netherlands.
Nutrition in Emergencies, Harmonized training Package
Emergency Nutrition Network (ENN). 2005. Operational Challenges of Implementing Community Therapeutic Care, ENN Report on an Interagency Workshop (Washington: February 28-March 2).
WHO. 2003. Guidelines for the inpatient treatment of severely malnourished children. Geneva.
WHO. 1999. Management of Severe Malnutrition: A Manual for Physicians and Other Senior Health Workers. Geneva. www.who.int/nut/publications
WHO/UNICEF. 2000. Management of the Child with Serious Infection or Severe Malnutrition: Guidelines for Care at the First-Referral Level in Developing Countries. www.who.int/child-adolescent-health/ publications/CHILD_HEALTH/WHO_FCH_CAH_00.1.htm






























