Child with cyanosis

Presented by :
Group C4
5th year medical students
Tripoli university
Pediatric

Objectives
Definition of cyanosis
Types of cyanosis
Causes of cyanosis
Complications
Management

Cyanosis is derived from the colour ‘cyan’, which comes from ‘kyanous’, the Greek word for blue .
Definition:It is Bluish discoloration of skin and mucous membrane caused by increase concentration of reduced
hemoglobin > 5g/dl
so its not less pronounced if the child is anemic.

Types of cyanosis
CentralPeripheral

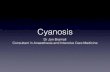
Peripheral cyanosis (blueness of hands &feet)
Normal systemic arterial oxygen saturation.
The increased extraction of oxygen results from sluggish movement of blood through the capillary circulation
Sites
Tip of nose
Ear lobules
Outer aspect of lips,chin,cheek
Tips and nailbeds of fingers,toes
Palms,soles Tongue is spared

Causes:
vasoconstriction ( exposure to cold)
polycythemia
low cardiac output

Central cyanosisPathologic condition caused by reduced arterial oxygen saturation.
due oxygenation defect in lung or admixture of venous and arterial blood
Involves highly vascularized tissues, through which blood flow is brisk .
Cardiac output typically is normal, and patients have warm extremities.
It is evident when O2 saturation falls below 90%
From 90_95% (desaturated)

Sites:
Tongue (margins & undersurface)
Inner aspect of lips
Mucous membranes of gums ,soft palate ,cheeks


Causes of central cyanosis 1_Respiratory disorders :
upper airway obstruction
Respiratory distress syndrome (RDS)
Meconium aspiration(MAS)
Pneumonia (sepsis)
PPHN_Failure of pulm.vascular resistance to fall after birth
Pulmonary hypoplasia
Bronchopulmonary dysplasia(mechanical ventilation)
Congenital diaphragmatic hernia
Asthma

2_CNS disorders:
ICH
Birth asphyxia
Seizures
Oversedation (direct or through maternal route)

3_Cardiac disorders:
Cyanotic congenital heart diseases (right to left shunt)
5Ts
Tetralogy of Fallot (TOF)
Transposition of great vessels(TGA)
Total anomalous pulmonary venous return
Truncus arteriosus
Tricuspid atresia
Note: persistant cyanosis in otherwise well infant is nearly always a sign of CHD

Ebstein malformation of the tricuspid valve
Left hypoplastic heart
Single ventricle
Critical pulmonary atresia
Heart failure/Cardiogenic Shock
othersPolycythemia
Methemoglobinemia
Metabolic diseases
Infection _septicemia
(physiological) : High altitude – Acrocyanosis “newborn”

examplecause
Cardiovascular disorders congenital cyanotic heart disease
Respiratory disorders - Pneumonia- Bronchiolitis
- RDS & meconium aspiration- Pneumothorax & pleural effusion
0CNS disorders - intra cranial hemorrhage0- Tonic clonic seizure
hematological disorders - Methemoglobinemia- Polycythemia
- Congenital cyanosis
other disorders - High Altitude- hypothermia - obstructive sleep apnea

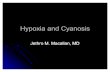
Differential CyanosisHands red (less blue) and feet blue seen in PDA with reversal of shunt (Differential Cyanosis) Requires pulmonary vascular resistance elevated to a systemic level and a patent ductus arteriosus
Left to right sunt pulmonary HT reversed shunt (Rt Lt shunt)
Desaturated blood from the ductus enters the aorta distal to the left subclavian artery, sparing the brachiocephalic circulation.

ManagementAim:
* Differentiate physiologic from pathologic cyanosis
* Differentiate cardiac from non- cardiac cause of cyanosis
* Find causes which needs urgent treatment or referral

Do :
1_complete maternal and newborn history
2_perform a full physical examination
3_ Investigation

Investigation* Pulse oximetry: (normal O2 sat. ≥ 95%)
* ABGs :
PaO2: to confirm central cyanosis
↑ PaCO2: may indicate pulmonary or CNS disorders.
↓ pH: sepsis, circulatory shock, severe hypoxemia
* Hyperoxia test (Is it due cardiac or pulmonary cause?)
placing the infant in 100% oxygen for 10 minutes. If he remains cyanotic after this period, the cyanosis is said to be secondary to cyanotic heart diseases(SaO2 not reach the normal value).

* CBC :
↑ or ↓ WBC : sepsis
Hematocrit > 65% : polycythemia
* Methemoglobinemia : ↓ SaO2, normal PaO2, chocolate-brown blood , HB-M
* Sepsis screening
* ECG: Dx for Tricusped atresia (Lt axis deviation only is seen)
* Echo: Dx for CHD
* Chest x-ray

Treatment* Warming of the affected area: in peripheral cyanosis
* Oxygenation & adequate ventilation
(PaO2 normalizes completely during artificial ventilation in infant with CNS disorder)
* IV fluidsChildren who have difficulty in feeding due to cyanosis
need fluids to be administrated.
* If sepsis is suspected or another specific cause is not identified, start on broad spectrum antibiotics then obtain a full septic screening

* Drugs: Prostaglandin E1
For ductal dependent CHD
IV Infusion of PGE1 at a dose of (0.05-0.1mcg/kg/min) to maintain patency
S/E- hypoventilation, apnea, edema and low grade fever
* Surgery

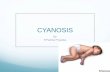
CCHD


Tetralogy of Fallot
Boot shape

Total Anomalous Pulmonary Venous Return(TAPVR)
Snowman

Transposition of Great Arteries
Egg on a string

Truncus arteriosus

Tricusped atresia

Complication of CCHD
Stunt of growth
Cyanotic spells (in TOF)
brain abscess
Cerebral thrombosis (CVA)
pulmonary TB (oligemic lung)
HF “rare”
Death

Tx of cyanotic spells:
Hold the baby in knee chest position
O2
Morphine (subcut.) : to relieve pain & anexiety
NaHco3 : for metabolic acidosis
Inderal (Beta blocker) : prevent recurrent attack

Thank you