Ta u s s i g C a n c e r I n s t i t u t e | A S H 2 0 0 8 E d i t i o n
Cancer Consult
Highlightsfrom the 2008American Society of HematologyAnnual Meeting
CAnCer ConSult ASH 2008 edition
Dear Colleagues and Friends:
This issue of Cancer Consult is devoted to the Taussig Cancer Institute’s
participation in the American Society of Hematology (ASH) Annual
Meeting, which took place in December 2008 in San Francisco.
This was a noteworthy meeting for ASH as it represented the 50th
anniversary of the society. This annual meeting has become our
department’s most important scientific meeting. It is a wonderful mix
of educational lectures, and offers a unique blend of basic, translational
and clinical research presentations. Twenty-four-thousand people
attended, with close to 6,000 abstracts submitted for consideration.
The Cleveland Clinic Taussig Cancer Institute sponsored our first Friday
Educational Symposium: “Bone Marrow Failure Syndromes: Optimizing
Outcomes Worldwide Through Disease Understanding.” These “Super
Friday” symposiums are competitively awarded by ASH, and we were
proud to be selected as a sponsor. Drs. Mikkael Sekeres and Jaroslaw
Maciejewski were the co-directors of this international symposium that
reached more than 400 participants.
The Taussig Cancer Institute presented 16 oral and 49 poster presen-
tations. Our Lymphoma Program co-authored an abstract that was
accepted for the Plenary Session. Dr. Yogen Saunthararajah presented
data concerning the genesis of cancer that was accepted as one of the
“Best of ASH” abstracts. In addition, Drs. Sekeres, Smith and I had the
privilege of serving as abstract reviewers for this year’s meeting.
I hope you find this edition of Cancer Consult valuable, as it highlights
many of theTaussig Cancer Institute’s presentations during the ASH
Annual Meeting. Our strong presence at this important event is indica-
tive of continued recognition of our research efforts and points to the
strength of the Department of Hematologic Oncology and Blood Disor-
ders. Our most important mission is to deliver outstanding care to our
patients and ultimately to win the war on cancer. I would like to thank
all of our colleagues and friends for your ongoing support. A directory of
our physicians is included with this newsletter. Please feel free to con-
tact any of us about your patients.
Sincerely yours,
Brian J. Bolwell, MD
Chairman, Department of Hematologic Oncology and Blood Disorders
ClevelAnd CliniC | tAuSSig CAnCer inStitute | CAnCer ConSult
clinical Trials 10
Bone Marrow Failure Syndromes:
Optimizing Outcomes Worldwide
Through Disease Understanding 1
Clinical Trials Under Way to
Improve Outcome in AML 4
Partnership Streamlines Drug
Development 5
Myeloma Program Expands with
Return of Researcher 6
Clinical Trial Shows Promise
in Some Non-Hodgkin’s
Lymphomas 7
Study Shows that Future Cancer
Treatments Could Be Less
Damaging, Toxic to Patients 8
Study Questions Timing of
Induction Therapy in Older AML
Patients 9
CLINICAL TRIALS 10
Fellow Highlights New
Technology at ASH 12
PUBLICATIONS 13
REFERRALS 14
S AT E L L I T E S Y M P O S I U M American Society of Hematology
Bone Marrow Failure Syndromes:
optimizing outcomes Worldwide through disease understanding
CAnCer ConSult ASH 2008 edition
Understanding of the molecular underpinnings of
these disorders has exploded in the past decade,
and with it pathobiologically-driven therapies and
predictors of response to therapies, the availability
of which also vary across the world.
Cleveland Clinic hosted a well-attended satellite
symposium during the 50th ASH Annual Meeting
to share current understanding of bone marrow
failure syndromes, directed by Mikkael Sekeres,
MD, MS, Department of Hematologic Oncology
and Blood Disorders at Taussig Cancer Institute.
“This symposium evolved from the close collabora-
tion we have achieved at Taussig Cancer Institute
between clinical and translational researchers,”
says Dr. Sekeres, who co-designed the CME with
Jaroslaw Maciejewski, MD, PhD, Chairman of
the Department of Translational Hematologic
and Oncologic Research. “We included both the
basic and clinical aspects of these diseases, which
attracted each of us to devote our careers to their
study. We showcased the interplay between clinical
and translational research, and how it can result in
concrete changes. Some aspects of our collabora-
tion have earned international recognition.”
He pointed to both the recognition of the RARS-T
abnormality by the World Health Organization,
and upcoming revisions to the international
prognostic scoring system (IPSS) that have grown
out of Dr. Maciejewski’s application of innovative
technologies in translational research.
“In the past, we were able detect genetic abnor-
malities in about 50 percent of patients with bone
marrow failure syndromes,” says Dr. Sekeres. “But
by using SNP-Array technology, Dr. Maciejewski is
able to detect these abnormalities in 80 percent of
patients. These abnormalities are clandestine but
real, and they have prognostic implications.”
Several international experts joined the faculty
for the course, including Pierre Fennaux, MD,
PhD, from the University of Paris, France, who
addressed Preventing AML Transformation; and
Aristoteles A.N. Giagoudidid, MD, PhD, of St.
Johannes Hospital in Duisburg, Germany, who
shared his experience in Rationally Targeting the
Molecular Underpinnings of the Disease.
Dr. Sekeres says the international scope of the
symposium showcased the robust collaboration
among specialists from throughout the world
in studying and treating bone marrow failure
disorders. “We have strong relationships around
the U.S. and throughout the world,” he says. “We
recognize that there is strength in numbers.”
By including presentations from the Leukemia
& Lymphoma Society and the Aplastic Anemia
& Myelodysplastic Syndromes Foundation, Dr.
Sekeres says the event also addressed the need to
include patients in clinical trials.
“In adult oncology as a whole, less than 10 percent
of patients participate in clinical trials,” he says.
“Our speakers highlighted the resources avail-
able to patients through patient advocacy groups,
including direct economic support for travel and
participation in clinical trials.”
To discuss the sym-posium or to refer a patient to Dr. Sekeres, call 216.444.5385 or email [email protected]
Bone Marrow Failure Syndromes affect hundreds of thousands of people worldwide.
The epidemiology, risk factors, and molecular characterization of these diseases vary among
different countries, with incidence rates for aplastic anemia ranging from 2 per million in the U.S.,
Europe, and Israel to 7 per million in some Chinese provinces. Myelodysplastic syndromes are even
more prevalent, with an incidence ranging from 1 per 100,000 in Japan to 12 per 100,000 in
areas of the United Kingdom, and 3.4 per 100,000 in the U.S.
S Y M P O S I U M
( c o n t i n u e d )
CAnCer ConSult ASH 2008 edition
“We showcased the interplay
between clinical and transla-
tional research, and how it can
result in concrete changes.”
2 | 3 | clevelandclinic.org/cancerconsult
CAnCer ConSult ASH 2008 edition
The possibility of employing biological targeted
therapies with or without chemotherapy in
the treatment of hematological malignancies
has generated excitement over the last few
years. Members of the Taussig Cancer Institute
Department of Hematologic Oncology and Blood
Disorders are among investigators evaluating these
therapies in AML. A team led by Anjali Advani,
MD, presented results of a Phase I trial of imatinib
mesylate with daunorubicin and cytarabine for
patients with c-kit positive relapsed AML at the
2008 ASH Annual Meeting.
“Although AML is not associated with one specific
mutation, AML cells do share biological charac-
teristics that may allow the application of molecu-
lar targeted therapies,” says Dr. Advani. C-kit, a
tyrosine kinase receptor expressed on more than
90 percent of relapsed AMLs, mediates leukemic
proliferation and anti-apoptotic effects. Signaling
pathways including STAT3 and STAT5 may be acti-
vated downstream of c-kit. Higher c-kit expression
is associated with a shorter time to relapse and
shorter overall survival.
“Therefore, targeting the c-kit receptor in AML
may improve the outcome for patients,” says Dr.
Advani.
C-kit inhibitors are not active enough as single
agents in AML. However, it is possible that c-kit
inhibitors may be effective when used in combina-
tion with other therapies, including chemotherapy.
“Imatinib mesylate is a potent c-kit inhibitor that
has demonstrated some activity in relapsed/refrac-
tory AML,” says Dr. Advani. “In this trial, we com-
bined imatinib mesylate with standard induction
therapy for patients with c-kit+ relapsed AML.”
Twenty-one patients had enrolled at the time of the
presentation. “Eleven of the 19 evaluable patients
achieved complete remission (CR) or complete
remission with incomplete platelet recovery (CRp),
an encouraging result that merits evaluation in a
larger Phase II study,” says Dr. Advani.
Dr. Advani and her colleagues continue to open
clinical trials to improve the outcome for patients
with AML.
Acute myeloid leukemia (AML) is a difficult disease to treat. Although 65 percent of patients
achieve complete remission with chemotherapy, only 15 to 30 percent remain free of the disease
for five years. New treatment medications and approaches are desperately needed.
Clinical trials under Way to improve outcome in AMl
For more informa-tion or to contact Dr. Advani, call 216.445.9354or [email protected].
A Phase 1 Trial of Imatinib
Mesylate
with Daunorubicin
and Cytarabine
forPatients with C-Kit Positive Relapsed Acute Myeloid Leukemia
Anjali S Advani, MD1, Ed Copelan, MD1, Ronald Sobecks, MD1, Mikkael A Sekeres, MD, MS1, Jennifer Bates1, Mary Lynn Rush1, Barbara Tripp1, Elysa Noon, PhD2, Matthew Howard, MD3, Tao Jin4, Eric Hsi, MD3, Matt Kalaycio, MD11Hematologic Oncology and Blood Disorders, Taussig
Cancer Center, Cleveland Clinic, Cleveland, OH 44195, 2Novartis Pharmaceuticals, 180 Park Ave., Florham Park, NJ 07932,3Clinical Pathology, Cleveland Clinic, Cleveland, OH 44195, 4Quantitative Health Sciences, Cleveland Clinic, Cleveland, OH 44195
Taussig Cancer Center
BackgroundTargeting the c-kit receptor in AML represents a potential therapeutic strategy. C-kit is expressed on more than 10% of blasts in 95% of patients with relapsed AML1. C-kit mediates proliferation and anti-apoptotic effects in AML2, 3. Signaling pathways, such as STAT3 and STAT5, may be activated downstream of c-kit.
Methods Results
ConclusionsThe MTD of imatinib
in combination with 7+3 was 300 mg. Since the hyperbilirubinemia
appeared to be reversible with discontinuation of imatinib, it may be possible to escalate imatinib
doses further and re-
challenge. The CR rate is encouraging and merits evaluation in a Phase 2 study. In particular, patients with no nuclear P-STAT3 had a high CR rate; whereas patients with nuclear P-STAT3 had a lower CR rate. STAT3 may be activated independently of c-kit; therefore, directly targeting STAT3 in this latter group of patients may potentially
improve prognosis.
References1.
Hans CP, Finn WG, Singleton TP, et al. Usefulness of anti-CD117 in the flow cytometric
analysis of acute leukemia. American Journal of Clinical Pathology 2002; 117: 301-5.
2.
Ikeda H, Kanakura
Y, Tamaki T, et al. Expression and functional role of the proto-oncogene c-kit in acute myeloblastic
leukemia cells. Blood 1991; 2962-8. 3.
Hassan H, Zander
A. Stem cell factor as a survival and growth factor in human normal and malignant hematopoiesis. Acta
Haematol
1996; 95: 257-62. 4.
Kindler T, Breitenbuecher
F, Marx A, et al. Efficacy and safety of imatinib
in adult patients with c-kit positive acute myeloid leukemia. Blood 2004; 103: 3644-54.
5.
Fang C, Kim C, Perkins C, et al. CGP57148B (STI-571) induces differentiation and apoptosis and sensitizes Bcr-Abl-
positive
leukemia cells to apoptosis due to antileukemic
drugs. Blood 2000; 96: 2246-53.
Table 3 Patient Characteristics
Median Age
47 years (range 24-75
)Sex
48% maleMedian time from CR to relapse
439 days (range 216-1100)CG risk group
Poor
14%
Intermediate
71%
Good
14%Median percentage of c-kit + blasts
89% (range 52-98)
Imatinib
mesylate, a c-kit inhibitor, has demonstrated complete and partial hematologic responses in relapsed/ refractory AML in
a Phase 2 study4. In vitro, co-treatment with imatinib
significantly increases cytarabine
or doxorubicin induced apoptosis of Bcr-Abl
positive leukemia cell lines5. This apoptosis is accompanied by downregulation
of anti-apoptotic proteins5. Thus, combining imatinib
with chemotherapeutic agents such as cytarabine
and daunorubicin
may be synergistic in the apoptosis of AML cells. This Phase 1 trial evaluated the safety and efficacy of combining imatinib
mesylate
with daunorubicin
and cytarabine
in patients with c-kit positive AML.
Cell survivalProliferation
AdhesionChemotaxis
Signalingproteins
CellSurface
Stem cell factor
P
P
P
P
P
P
P
P
P C-KITC-KIT
All patients were treated at the Cleveland Clinic from 2003-2008. Cytogenetic (CG) risk was defined by CALGB criteria. Phosphorylated
(P) activated STAT3 (nuclear and cytoplasmic) was assessed by immunohistochemistry
(IHC) on pre-treatment samples. IHC studies for P-STAT5 are ongoing.
Table 1 Eligibility Criteria
Relapsed AML (excluding APL)Relapse more than 6 months from induction therapyECOG performance status 0-2≥20% c-kit+ blasts (CD117+ by flow cytometry)Age ≥
18 yearsNot pregnant or lactatingCreatinine
≤
2 mg/dLAST and ALT ≤
2 x upper limits of normal, bilirubin
≤
2 mg/dL.
Treatment Plan: All patients received daunorubicin
45 mg/m2
IV for 3 days, and cytarabine
100 mg/m2/d continuous IV infusion for 7 days (7+3). Imatinib
dose was escalated using a standard 3 x 3 design. Dose levels are listed in Table 2.
Table 2 Dose Levels of Imatinib
Mesylate
-1 (300 mg)1 (400 mg)
Imatinib
mesylate
was administered with the first dose of chemotherapy and continued daily until disease progression, intolerance, removal from study for another treatment (including
alloBMT), or dose-limiting toxicity (DLT). DLT was defined as any non-hematologic toxicity ≥
Grade 3 excluding alopecia/ constitutional symptoms; any treatment-related death; and greater than 45 days to recover an absolute neutrophil
count of 500/ μL.
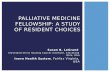
21 patients have been enrolled.
STAT3 expressionIn patients expressing nuclear P-STAT3, 2-6% of the blasts stained positiveEleven patients had no nuclear P-STAT3No patients had cytoplasmic
P-STAT3
Because there were 2 DLTs, subsequent patients were treated at dose level -1. One DLT was seen (bilirubin
5.5 mg/ dL) out of 6 patients, making 300 mg/ d the MTD. Enrollment to the expanded cohort at the MTD is currently complete. One patient died during induction and was not evaluable for response. Response data for
the other 20 patients is shown in Figure 1.
Patients received imatinib
mesylate
for a median 23 days (range 9-574+). Three discontinued imatinib
to proceed to alloBMT. Two patients continue on imatinib
and remain in a remission at 52+ and 574+ days.
2 (600 mg)3 (800 mg)
% o
f Pat
ient
s
Figure 1.Responses
Anjali Advani received research support from Novartis. Matt Kalaycio
is on the Speakers Bureau for Novartis. Elyssa
Noon is an employee of Novartis.
Nine patients were treated at dose level 1 (400 mg) because 3 patients discontinued imatinib
before DLT could be evaluated (2 due to nausea, 1 due to persistent leukemia on a Day 14 bone marrow). Of the 6 evaluable patients, 2 patients had a DLT. Both of these were > Grade 3 hepatotoxicity.
Predictors of ResponseC-kit expression did not correlate with achievement of CR. However, patients with no nuclear P-STAT3 had a higher CR rate (82%) than patients with P-STAT3 nuclear expression (33%) (p=0.18).
Dose Escalation
Disclosures
CR/ CRp0
20
40
60
No CR
ClevelAnd CliniC | tAuSSig CAnCer inStitute | CAnCer ConSult
The partnership, designed under the guidance of
John Sweetenham, MD, Brad Pohlman, MD, and
Chairman Brian Bolwell, MD, of the Department
of Hematologic Oncology and Blood Disorders,
streamlines the complex processes involved in
developing and advancing new anticancer treat-
ments through clinical studies. The goal is to
accelerate the development of successful therapies
for hematologic malignancies.
While most national clinical trials are conducted
by cooperative groups — vast networks of physi-
cians, researchers, medical centers and universi-
ties across the country — the Clinical Trial Center
for Hematologic Malignancies will expedite the ad-
vancement of new drugs, since the trials will all be
conducted by a single clinical center with access to
a large volume of patients. The partnership plans
to undertake more than six clinical trials over the
next three years, enrolling 100 to 150 patients,
increasing the number of trials typically completed
for these types of cancers in this timeframe.
Investigator Stephen Smith, MD, Associate Staff
in the Department of Hematologic Oncology
and Blood Disorders, says the Taussig Cancer
Institute brings a team of highly capable clinical
researchers and a strong research infrastructure to
the partnership, while the Leukemia & Lymphoma
Society has a long history of involvement in major
breakthroughs in treating hematologic cancers
nationwide. Since its launch, the center has
opened one study for treating lymphoma, and
expects to launch another this spring.
“The first study combines two new drugs — consid-
ered ‘targeted therapies’ due to the specific manner
they affect tumor cells — to find out if they are safe
and effective together in patients with relapsed
B-cell lymphoma,” says Dr. Smith. “This study
builds upon recent advances in understanding the
complex processes that keep tumor cells alive.”
Dr. Smith says that research has shown that
lymphoma cells live and grow in a precarious
state, relying on a delicate balance of proteins that
perform the tasks that keep tumor cells alive.
The two medications are known for disrupting
the cell’s handling of proteins, which offsets
this balance and pushes cancerous cells toward
self-destruction. This study is the first to use
these specific medications together (even though
each has shown promise against lymphoma
alone), to determine the combination’s safety and
effectiveness.
The second trial, beginning enrollment this
spring, is slated to start at the Cleveland Clinic
main campus as well as regional Cleveland Clinic
Cancer Centers at Hillcrest and Fairview hospitals.
“This study is designed to test one of the most
specific types of anticancer therapies ever
developed — a drug that blocks a particular
genetic ‘message’ telling a lymphoma cell to pro-
duce a cancer-stimulating protein. By blocking
this message, the drug removes a major impetus
for tumor cell growth,” says Dr. Smith. “We’ll be
enrolling patients with certain non-Hodgkin’s
lymphomas that have relapsed after initial
treatment.”
He says news of the partnership generated excite-
ment at this year’s ASH meeting, where he served
as a reviewer of abstracts in the category of chemo-
therapy treatments for lymphoma. “ASH is fertile
ground for the development of promising new
therapies for lymphoma,” he says.
Partnership Streamlines drug development
In 2008, the Leukemia & Lymphoma Society and the Cleveland Clinic Taussig Cancer Institute
launched a groundbreaking partnership, the Clinical Trial Center for Hematologic Malignancies,
aimed at increasing access and participation in clinical trials among adult cancer patients.
For more information on the Clinical Trial Center for Hematologic Malignancies or to discuss patient enroll-ment, please call 866.246.5937, or email Dr. Smith at [email protected].
4 | 5 | clevelandclinic.org/cancerconsult
CAnCer ConSult ASH 2008 edition
Dr. Reu graduated from the Eberhard-Karls Univer-
sitat Tubingen in Tubingen, BW, Germany, before
completing his internship, residency and fellow-
ship training at Cleveland Clinic. He returned to
Germany for two years to head the AML Task Force
at the University of Heidelberg, but welcomed the
opportunity to return to Cleveland Clinic.
“I like the way medicine is practiced at Cleveland
Clinic,” says Dr. Reu. “This environment provides
a unique setting to pursue my epigenetic research
and continue to deliver high quality patient care.”
Dr. Reu is leading basic and clinical research in
myeloma. His lab in the Taussig Cancer Institute
focuses on DNA methylation, regarded as one of
the most significant epigenetic events. Cytosine-
phosphate-guanine (CpG) methylation in the
promoter region of certain genes may be the
earliest alteration in some cancers. It is correlated
with silencing of genes.
“Medications that can inhibit the shutdown of
these tumor suppressor genes are already FDA ap-
proved for myelodysplastic syndomes (MDS), and
they’re being tested for other cancers,” says Dr.
Reu. “They are incorporated into the DNA and bind
the enzyme that is responsible for methylation,
thereby inactivating it.”
Taussig Cancer Institute is pleased to announce the return of Frederic Reu, MD, to the Chronic
Leukemia and Myeloma Program in the Department of Hematologic Oncology and Blood Disorders.
Myeloma Program expands with return of researcher
But cell division in myeloma is significantly slower
than in MDS, which suggests that dosing schedules
would need to be altered to get the same effect. Dr.
Reu has approval to open a clinical trial of a prom-
ising epigenetic drug in multiple myeloma.
In his lab, Dr. Reu is involved in basic research to
uncover agents that reactivate specific genes.
“Currently available drugs will reactivate any gene
that is silenced by DNA methylation,” he explains.
“I’m working to find the pathways necessary for
reactivation of only the genes that we want to reac-
tivate. Ultimately, this could lead to the develop-
ment of agents that are far more specific.”
In addition to his work in cancer research, Dr. Reu
is collaborating with colleagues in cardiology to
establish an amyloid center.
“Amyloidosis is a disease where abnormal proteins
are deposited in the tissue between cells, thereby
disrupting organ function,” says Dr. Reu. “The
most common form, AL amyloidosis, is very simi-
lar to multiple myeloma because it is caused by the
same cells.”
Dr. Reu and Mazen Hanna, MD, a cardiologist with
advanced training in heart failure, plan to incor-
porate multiple disciplines and offer treatment
approaches that include novel systemic therapies,
heart and stem cell transplantation.
For more information on Dr. Reu’s studies or to refer a patient, call 216.636.0200 or email [email protected].
CAnCer ConSult ASH 2008 edition
While he cautions that the data are preliminary,
Dr. Sweetenham says that the fact that this is
an orally available molecule with a new target is
generating excitement.
The drug, fostamatinib, targets a new pathway
known as Syk (spleen tyrosine kinase), which is
tumor specific and may selectively kill tumor cells
while decreasing potential side effects.
“The results were particularly impressive in chron-
ic lymphocytic leukemia (CLL) and diffuse large
B-cell lymphoma (DLBCL), which in many ways
are on opposite ends of the spectrum. Patients can
live with CLL for a very long time before it becomes
resistant to chemotherapy, whereas DLBCL is rela-
tively aggressive and fast-growing,” he says.
“Normally in these very preliminary studies, we’re
looking to determine toxicity of the treatment rath-
er than necessarily seeing responses to the drug.
But there were a significant number of responses
in these two groups.”
In a heavily pretreated population with few thera-
peutic options, the overall response rate was 55
percent in CLL and 22 percent in DLBCL.
Besides the encouraging results, Dr. Sweetenham
says that the fact that it can be offered as a pill is
very attractive to patients and favorably impacts
compliance. “With so many of the new agents
being intravenous treatments that carry problems
with drug delivery, this is a welcome alternative,”
he says.
However, he describes himself as naturally
cautious.
“There’s no such thing as a free lunch and it did
have side effects, including quite marked fatigue
and diarrhea,” he says. “And what we don’t know
yet is how easy it is going to be to combine this
drug with other types of chemotherapy, which cer-
tainly is where its future impact is going to be.”
Dr. Sweetenham expects that larger studies will
help experts determine the future applications
of fostamatinib. But, he says, the most important
thing may not be the drug itself, but its concept.
“We’re now in a position where we are assessing
drugs that have been designed to work in a par-
ticular way, so this is no longer chance observation
that something works. These are designer drugs,”
he says. “It’s an important step on the way to indi-
vidualized therapy.”
Results of the study also point to the importance of
enrolling patients in clinical trials.
“Patients who participated in this study truly ben-
efited from this drug, which they couldn’t have got-
ten without being part of a clinical trial,” he says.
Clinical trial Shows Promise inSome non-Hodgkin’s lymphomas
A Phase II clinical trial of a novel drug for relapsed/refractory Non-Hodgkin’s Lympoma presented during a
plenary session at the ASH Annual Meeting showed promising results according to study co-investigator
John Sweetenham, MD, Department of Hematologic Oncology and Blood Disorders.
To refer a patient to Dr. Sweetenham, or to dis-cuss this or another trial, call 216.445.6707 or email [email protected].
6 | 7 | clevelandclinic.org/cancerconsult
“These are designer drugs. It’s
an important step on the way
to individualized therapy.”
CAnCer ConSult ASH 2008 edition
The researchers found that they could alter an
existing chemotherapy drug to stop the growth of
cancer cells and encourage the growth of healthy
cells. Current treatments kill both cancer cells and
healthy cells, which leads to numerous side effects.
The results of the studies suggest that the mecha-
nisms that cause cancer cells to divide and grow
uncontrollably are often different from the mecha-
nisms that drive the growth of healthy stem-cells.
This difference can be exploited to selectively stop
the growth of the cancer cells without stopping the
growth of healthy stem-cells.
“Today, most cancer chemotherapy works the
margins — the chemotherapy is marginally more
poisonous to cancer cells than normal cells,” said
lead investigator Yogen Saunthararajah, MD, of
Taussig Cancer Institute. “Therefore, treatment is
Study Shows that Future Cancer treatments Could Be less damaging, toxic to Patients
Cleveland Clinic researchers presented findings at the 50th Annual ASH Meeting that
suggest cancer could be treated in a novel way that is much less toxic.
difficult and risky for patients and can only be given
for a few days at a time, with long periods without
treatment during which the cancer can regrow.
“Using this alternative approach, which in the
test-tube has opposite effects on cancer cells
versus healthy stem cells, perhaps therapy can be
given regularly and for longer periods, to get the
maximum benefits of treatment. We are excited
that we can modify the use of existing drugs to
produce this effect, which will allow us to start
clinical trials soon.”
The research team studied bone marrow samples
of myelodysplastic syndrome (MDS) and leuke-
mia patients as well as healthy blood stem cells to
discover that the enzyme known as DNMT1 plays
opposite roles in the healthy stem cells versus the
cancerous cells. Therefore, inhibiting the function
of this enzyme produced opposite effects on the
healthy cells versus the cancerous cells. The drug
used to inhibit this enzyme, decitabine, is already
available for clinical use, allowing for clinical stud-
ies to be conducted in the next year to determine if
using decitabine in this new method can repro-
duce the effects seen in the test tube in patients.
The research team emphasized that this work
needs to undergo the peer review process and
publication, and that clinical trials must be
conducted to further test this approach in
patients. This study was highlighted as a “Best
of ASH” presentation by the American Society
of Hematology, the world’s largest professional
association of blood specialists.
The U.S. Department of Defense has agreed to fund
further preclinical studies to continue to improve
this approach as a treatment of cancer.
To reach Dr. Sauntha-rarajah, please call 216.444-8170 or email [email protected].
DNMT1 depletion, using non-DNA damaging levels of the nucleoside analogue decitabine (DAC), has opposite effects on acute myeloid leukemia and normal stem cell self-renewal.
ClevelAnd CliniC | tAuSSig CAnCer inStitute | CAnCer ConSult
The study included more than 1,300 patients with
acute myeloid leukemia (AML) and showed that
every day of delay from diagnosis to the start of
therapy worsens survival in younger adults, while
delay does not impact survival in the elderly.
“In an ideal patient, who is younger than 60 with
a core binding factor cytogenetic abnormality,
standard induction chemotherapy will achieve
complete remission (CR) nearly 85 percent of
the time,” says Dr. Sekeres. “But most patients
are older, with other cytogenetic abnormalities
or secondary AML. In this group, outcome from
standard therapy is much worse, with CR rates less
than 50 percent and treatment mortality rates that
approach 25 percent.”
The combined database from Cleveland Clinic and
M.D. Anderson included 1,660 AML patients treat-
ed from 1994 to 2005. Excluded patients included
those with promyelocytic leukemia, those under
age 17, those with white blood cell counts more
than 50,000/mm³, those diagnosed more than
three months before therapy, those who began
therapy immediately on the date of diagnosis, and
those with incomplete data. The final dataset con-
sisted of 1,317 patients who were all treated with a
remission induction regimen that included cytara-
bine. These patients were typical of other large
AML studies in the distribution of pretreatment
covariates, the rates of CR and overall survival (OS),
and the effect of covariates on outcome.
Cytogenetics were determined using metaphase
karyotyping based on analysis of 20 or more cells.
Patients with complex cytogenetics or -7 abnor-
malities were classified as “unfavorable”; those
with core binding abnormalities were classified
as “favorable”; and remaining patients, including
those with insufficient metaphase to determine
cytogenetic abnormalities, were placed in the
“intermediate risk” category. Both univariate and
multivariate analyses were completed.
“Our data suggest that in younger patients with
WBC less than 50,000/mm³, AML should continue
to be considered an oncologic emergency. Out-
comes were worse in the 41 percent of younger
patients whose treatment was delayed for five or
more days,” says Dr. Sekeres. “The findings raise
the question of whether it is prudent to delay
therapy in younger patients to determine eligibility
for clinical trials that may or may not offer better
outcomes.”
However, in patients 60 or older, the time from
diagnosis to treatment did not appear to affect
complete remission or overall survival rates.
“Since indirect data suggest that older patients
derive very little benefit from standard induction
therapy, waiting until cytogenetic or molecular
results become known and offering individualized,
investigational therapy to this group is probably
beneficial,” says Dr. Sekeres.
Study Questions timing of inductiontherapy in older AMl Patients
Research completed by Mikkael Sekeres, MD, MS, Department of Hematologic
Oncology and Blood Disorders, and investigators from M.D. Anderson was
featured in the Jan. 1, 2009 issue of Blood.
To refer a patient to Dr. Sekeres, call 216.444.5385 or email [email protected].
8 | 9 | clevelandclinic.org/cancerconsult
CAnCer ConSult ASH 2008 edition
Acute Myeloid Leukemia (AML)
A Phase II Study of Imatinib Mesylate (Gleevec) as Maintenance Therapy after Induction and Consolidation Chemotherapy in Patients with Newly Diagnosed C-kit Postitive AML Less than 60 Years of Age
PI: Anjali Advani, MD
A Phase IIB, Randomized, Double-Blinded, Placebo-Controlled Study of Low Dose Cytara-bine and Lintuzumab Compared to Low Dose Cytarabine and Placebo in Patients 60 Years of Age and Older with Previously Untreated AML
PI: Mikkael Sekeres, MD, MS
Acute Lymphocytic Leukemia (ALL)
An Intergroup Phase II Clinical Trial for Adoles-cents and Young Adults with Untreated Acute Lymphoblastic Leukemia (ALL)
PI: Anjali Advani, MD
Bone Marrow Transplant
Multiple Unit Unrelated Donor Umbilical Cord Blood Transplantation for Patients with Hema-tologic Diseases
PI: Ronald Sobecks, MD
A Study of Outcomes and Toxicity of Busulfex as Part of a High Dose Chemotherapy Prepara-tive Regimen in Autologous Hematopoietic Stem Cell Transplantation for Patients with Plasma Cell Myeloma
PI: Ronald Sobecks, MD
A Phase II Trial Evaluating Modified High Dose Melphalan (100 mg/m2) and Autologous Pe-ripheral Blood Stem Cell Supported Transplan-tation (SCT) for Patients with AL Amyloidosis or High Risk (greater than or equal to Age 70 or Poor Renal Function) Patients With Multiple Myeloma (A BMT Study)
SWOG study
Chronic Lymphocytic Leukemia (CLL)
A Phase I/II, Multi-Center, Open-Label Study of the Safety and Efficacy of a Stepwise Dose-Escalation Schedule of Lenalidomide Monotherapy in Subjects with Relapsed or Re-fractory B-Cell Chronic Lymphocytic Leukemia
PI: Mikkael Sekeres, MD, MS
A Phase I Trial of Bendamustine plus Alem-tuzumab for the Treatment of Fludarabine Refractory Chronic Lymphocytic Leukemia
PI: Matt Kalaycio, MD
Myelodysplastic Syndromes (MDS)
A Phase I/II Study of Revlimid in Combination with Azacitidine in Patients with Advanced MDS
PI: Mikkael Sekeres, MD, MS
A Phase II Trial of RAD001 in Low and Inter-mediate-1 Risk Myelodysplastic Syndrome
PI: Anjali Advani, MD
A Phase IIa, Open-Label, Dose Confirmation Study of Oral Clofarabine in Previously Treated Adult Patients with Myelodysplastic Syndromes (MDS)
PI: Mikkael Sekeres, MD, MS
Cleveland Clinic Taussig Cancer Institute is at the forefront of the cancer
drug discovery and development revolution. Through our cancer research
projects led by some of the world’s leading scientists, we have identified new
molecules with anti-tumor effect, which may lead to new drug therapies.
Key collaborative relationships with the world’s top biotech firms, university
research labs, renowned scientists, and major health organizations enhance
our research initiatives.
Hematologic Oncology and Blood Disorders
Cancer Consult provides information from Cleveland Clinic Taussig Cancer Institute specialists about innovative research and diagnostic and management techniques.
Please direct correspondence to Brian Bolwell, MD, Medical Editor [email protected]
Taussig Cancer Institute/R35 Cleveland Clinic 9500 Euclid Avenue Cleveland, OH 44195
Cleveland Clinic Taussig Cancer Institute annually serves more than 26,000 cancer patients. More than 250 cancer specialists are committed to researching and applying the latest, most effective techniques for diagnosis and treatment to achieve long-term survival and improved quality of life for all cancer patients. Taussig Cancer Institute is part of Cleveland Clinic, an independent, not-for-profit, multispe-cialty academic medical center.
Cancer Consult Medical EditorBrian Bolwell, MD, Chairman, Hematologic Oncology and Blood Disorders
Cancer Consult Editorial Board
Derek Raghavan, MD, PhD, Chairman, Taussig Cancer Institute
Robert Dreicer, MD, Chairman, Solid Tumor Oncology
Brian Rini, MD Solid Tumor Oncology
Timothy Spiro, MD, Chairman, Regional Oncology
John Suh, MD, Chairman, Radiation Oncology
Gene Barnett, MD, Director, Brain Tumor and Neuro-Oncology Center
Eric Klein, MD, Head, Urologic Oncology,Glickman Urological & Kidney Institute
Managing Editor Marjie Heines
DesignerAmy Buskey-Wood
PhotographyRussell Lee, Tom Merce, Don Gerda
Marketing
Lori Schmitt, RN, Andrew Kraynak,Melissa Raines
Cancer Consult is written for physicians and should be relied upon for medical education purposes only. It does not provide a complete overview of the topics covered and should not replace the independent judgment of a physician about the appropriateness or risks of a procedure for a given patient.
© 2009 The Cleveland Clinic Foundation
07-CNR-042
ClevelAnd CliniC | tAuSSig CAnCer inStitute | CAnCer ConSult
S E L EC T E D C L IN I C A L T R I A L S
10 | 11 | clevelandclinic.org/cancerconsult
Multiple Myeloma
An Open-Label, Single-arm, Phase II Study of Carfilzomib in Patients with Relapsed and Refractory Multiple Myeloma
PI: Fred Reu, MD
Non-Hodgkin’s Lymphoma
A Phase I/II Study of CMC-544 Administered in Combination with Rituximab in Subjects with Follicular or Diffuse Large B-Cell Non-Hodgkin’s Lymphoma
PI: Anjali Advani, MD
A Phase I Trial of the Combination of Everoli-mus (RAD001) and Bortezomib (Velcade) for Relapsed or Refractory Indolent and Mantle Cell Non-Hodgkin’s Lymphoma
PI: Stephen Smith, MD
A Phase I/II Study of Clofarabine in Patients with Relapsed T-cell and NK-Cell Lymphomas
PI: Brad Pohlman, MD
A Phase I/II, Multicenter, Open-Label Study of the X-Linked Inhibitor Apoptosis (XIAP) Anti-sense AEG35156 in Patients with Relapsed or Refractory Chronic Lymphocytic Leukemia and B-cell Lymphomas
PI: John Sweetenham, MD
A Randomized Phase IIB Placebo-controlled Study of R-ICE Chemotherapy (Rituximab, Ifosfamide, Carboplatin and Etoposide) with and without SGN-40 (anti CD-40 human-ized monoclonal antibody) for Second-Line Treatment of Patients with Diffuse Large B-Cell Lymphoma (DLBCL)
PI: Brad Pohlman, MD
For more information on clinical
trials or to refer a patient, call
216.444.7923 or 866.223.8100.
CAnCer ConSult ASH 2008 edition
Dr. Tiu works under the tutelage of Jaroslaw P.
Maciejewski, MD, PhD, Chairman of the Depart-
ment of Translational Hematologic and Oncologic
Research. The primary focus of his research has
been on advancing cytogenetic diagnosis in AML
and MDS using SNP-A.
“What we have found is that we’re not just detect-
ing new abnormalities using SNP-A, but that these
new abnormalities are important clinically in
patient prognosis,” says Dr. Tiu.
SNP-A is a novel molecular tool initially intended
to detect changes in the human genome that can
help define specific predispositions to certain
types of diseases. “But what we have found is that
in addition to being a genotyping tool, SNP-A is a
good karyotyping tool that allows us to see specific
defects in the chromosomes that may be impor-
tant in disease pathogenesis. We found a group of
patients who had normal findings using standard
metaphase cytogenetics, but who actually had hid-
den chromosomal abnormalities,” says Dr. Tiu.
Two of Dr. Tiu’s abstracts were selected for oral
presentations at the ASH Annual Meeting.
Dr. Tiu’s presentation on “Chromosomal Defects
Detected by SNP-Array-Based Karyotyping Are In-
dependent Predictors of Survival in Acute Myeloid
Leukemia,” showcased research comparing stan-
dard metaphase cytogenetics to SNP-A.
In his second presentation, “SNP-Array Based
Karyotyping Complements Routine Cytogenetics
For second-year hematology/oncology fellow Ramon Tiu, MD, the ASH meeting provided a rare
opportunity to showcase his role in promising research using the latest technology, SNP-Array
(SNP-A) karyotyping, in acute myeloid leukemia (AML) and myelodysplastic syndromes (MDS).
Fellow Highlights new technology at ASH
in Diagnosis and Risk Stratification Schemes of
MDS,” Dr. Tiu showed the benefits of using both
standard and new technology in improving cytoge-
netic diagnosis and prognostication in MDS.
“There has been a lot of uncertainty in myelodys-
plastic syndromes, since they are highly heterog-
enous,” says Dr. Tiu. “For many years, it has sort
of been a wastebasket diagnosis for patients with
bone marrow failures issues that could not fit in a
specific nosologic category. But there has been a
recent move to try to modify the current prognostic
system in these diseases.
“As much as SNP-A is very good at detecting un-
balanced abnormalities, there are conventional
abnormalities that you can’t detect,” he says, “such
as balanced abnormalities exemplified by certain
types of translocations or rearrangements. So both
technologies have a place in the correct diagnosis
and risk stratification of AML and MDS patients.”
Dr. Tiu says his experience at ASH confirmed his
decision to pursue a career in cancer research.
As a young investigator, he sees the breadth and
depth of ongoing work in the field and the vast
opportunities ahead.
“It was a great honor to represent Cleveland Clinic
and the Taussig Cancer Institute in front of the
most prominent experts in the field and to have
them be pleased with our work,” says Dr. Tiu. “It’s
a testament to the commitment of my mentor who
has been so instrumental in my career and to the
hard work of everyone in the laboratory.”
CAnCer ConSult ASH 2008 edition
12 | 13 | clevelandclinic.org/cancerconsult
Advani AS, Rodriguez C, Jin T, Jawde RA, Saber W, Baz R, Kalaycio M, Sobecks R, Sekeres M, Tripp B, Hsi E. Increased C-kit intensity is a poor prognostic factor for progression-free and overall survival in patients with newly diagnosed AML. Leuk Res. 2008 Jun;32(6):913-918. [PM:17928050].
Advani AS, Jin T, Ramsingh G, Tiu R, Saber W, Theil K, Sobecks R, Sekeres M, Copelan E, Sungren S, Tripp B, Kalaycio M. Time to post-remission therapy is an independent prognostic factor in adults with acute lymphoblastic leukemia. Leuk Lymphoma. 2008 Aug;49(8):1560-1566. [PM:18766970].
Dean RM, Fry T, Mackall C, Steinberg SM, Hakim F, Fowler D, Odom J, Foley J, Gress R, Bishop MR. Association of serum interleukin-7 levels with the development of acute graft-versus-host disease. J Clin Oncol. 2008 Dec 10;26(35):5735-5741. [PM:19001329].
Dunbar AJ, Gondek LP, O’Keefe CL, Makishima H, Rataul MS, Szpurka H, Sekeres MA, Wang XF, McDevitt MA, Maciejewski JP. 250K single nucleotide polymorphism array karyotyping identifies acquired uniparental disomy and homozygous mutations, including novel missense substitutions of c-Cbl, in myeloid malignancies. Cancer Res. 2008 Dec 15;68(24):10349-10357. [PM:19074904].
Kalaycio M, Advani A, Pohlman B, Sekeres M, Tripp B, Rybicki L, Sobecks R. Timed sequential induction chemotherapy and risk-adapted postremission therapy for acute myelogenous leukemia. Am J Hematol. 2008 Nov;83(11):831-834. [PM:18756545].
Lee SJ, Kukreja M, Wang T, Giralt SA, Szer J, Arora M, Woolfrey AE, Cervantes F, Champlin RE, Gale RP, Halter J, Keating A, Marks DI, McCarthy PL, Olavarria E, Stadtmauer EA, Abecasis M, Gupta V, Khoury HJ, George B, Hale GA, Liesveld JL, Rizzieri DA, Antin JH, Bolwell BJ, Carabasi MH, Copelan E, Ilhan O, Litzow MR, Schouten HC, Zander AR, Horowitz MM, Maziarz RT. Impact of prior imatinib mesylate on the outcome of hematopoietic cell transplantation for chronic myeloid leukemia. Blood. 2008 Oct 15;112(8):3500-3507. [PM:18664621].
Maciejewski JP, Mufti GJ. Whole genome scanning as a cytogenetic tool in hematologic malignancies. Blood. 2008 Aug 15;112(4):965-974. [PM:18505780].
Mahindra A, Bolwell B, Sobecks R, Rybicki L, Pohlman B, Dean R, Andresen S, Sweetenham J, Kalaycio M, Copelan E. Elevated ferritin is associated with relapse after autologous hematopoietic stem cell transplantation for lymphoma. Biol Blood Marrow Transplant. 2008 Nov;14(11):1239-1244. [PM:18940678].
Marks DI, Perez WS, He W, Zhang MJ, Bishop MR, Bolwell BJ, Bredeson CN, Copelan EA, Gale RP, Gupta V, Hale GA, Isola LM, Jakubowski AA, Keating A, Klumpp TR, Lazarus HM, Liesveld JL, Maziarz RT, McCarthy PL, Sabloff M, Schiller G, Sierra J, Tallman MS, Waller EK, Wiernik PH, Weisdorf DJ. Unrelated donor trans-plants in adults with Philadelphia-negative acute lymphoblastic leukemia in first complete remission. Blood. 2008 Jul 15;112(2):426-434. [PM:18398065].
Natkunam Y, Farinha P, Hsi ED, Hans CP, Tibshirani R, Sehn LH, Connors JM, Gratzinger D, Rosado M, Zhao S, Pohlman B, Wongcha-owart N, Bast M, Avigdor A, Schiby G, Nagler A, Byrne GE, Levy R,
Hematologic Oncology and Blood Disorders
A Sampling of 2008 Journal Publications
Gascoyne RD, Lossos IS. LMO2 protein expression predicts survival in patients with diffuse large B-cell lymphoma treated with anthracy-cline-based chemotherapy with and without rituximab. J Clin Oncol. 2008 Jan 20;26(3):447-454. [PM:18086797].
Rizzo JD, Somerfield MR, Hagerty KL, Seidenfeld J, Bohlius J, Bennett CL, Cella DF, Djulbegovic B, Goode MJ, Jakubowski AA, Rarick MU, Regan DH, Lichtin AE. Use of epoetin and darbepoetin in patients with cancer: 2007 American Society of Hematology/American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2008 Jan 1;26(1):132-149. [PM:17954713].
Rodriguez CP, Baz R, Jawde RA, Rybicki LA, Kalaycio ME, Advani A, Sobecks R, Sekeres MA. Impact of socioeconomic status and distance from treatment center on survival in patients receiving remission induction therapy for newly diagnosed acute myeloid leukemia. Leuk Res. 2008 Mar;32(3):413-420. [PM:17727945].
Sekeres MA, List AF. Active treatment strategies improving outcomes in patients with myelodysplastic syndromes with the deletion 5q abnormality. Clinical Leukemia. 2008 Feb;2(1):28-33.
Sekeres MA, Schoonen WM, Kantarjian H, List A, Fryzek J, Paquette R, Maciejewski JP. Characteristics of US patients with myelodysplastic syndromes: results of six cross-sectional physician surveys. J Natl Cancer Inst. 2008 Nov 5;100(21):1542-1551. [PM:18957672].
Sekeres MA, Maciejewski JP, Giagounidis AA, Wride K, Knight R, Raza A, List AF. Relationship of treatment-related cytopenias and response to lenalidomide in patients with lower-risk myelodysplastic syndromes. J Clin Oncol. 2008 Dec 20;26(36):5943-5949. [PM:19018091].
Sobecks RM, Dean R, Rybicki LA, Chan J, Theil KS, Macklis R, Andresen S, Kalaycio M, Pohlman B, Ferraro C, Cherni K, Sweeten-ham J, Copelan E, Bolwell BJ. 400 cGy TBI with fludarabine for reduced-intensity conditioning allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2008 Dec;42(11):715-722. [PM:18711346].
Sobecks RM, Ball EJ, Askar M, Theil KS, Rybicki LA, Thomas D, Brown S, Kalaycio M, Andresen S, Pohlman B, Dean R, Sweetenham J, Macklis R, Bernhard L, Cherni K, Copelan E, Maciejewski JP, Bolwell BJ. Influence of killer immunoglobulin-like receptor/HLA ligand matching on achievement of T-cell complete donor chimerism in related donor nonmyeloablative allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2008 Apr;41(8):709-714. [PM:18195688].
Sweetenham JW. Minimizing late effects in children and adults with Hodgkin lymphoma - the beginning of the end for radiation therapy. Leuk Lymphoma. 2008 May;49(5):839-840. [PM:18464101].
Thakkar SG, Fu AZ, Sweetenham JW, McIver ZA, Mohan SR, Ramsingh G, Advani AS, Sobecks R, Rybicki L, Kalaycio M, Sekeres MA. Survival and predictors of outcome in patients with acute leukemia admitted to the intensive care unit. Cancer. 2008 May 15;112(10):2233-2240. [PM:18348307].
Tiu RV, Sekeres MA. The role of AMG-531 in the treatment of thrombocytopenia in idiopathic thrombocytopenic purpura and myelodysplastic syndromes. Expert Opin Biol Ther. 2008 Jul;8(7):1021-1030. [PM:18549331].
Viny AD, Lichtin A, Pohlman B, Loughran T, Maciejewski J. Chronic B-cell dyscrasias are an important clinical feature of T-LGL leukemia. Leuk Lymphoma. 2008 May;49(5):932-938. [PM:18452068].
7th Annual
innovation SummitImproving the Prognosis:Cancer Cures Through Innovation
October 5-7, 2009Cleveland, Ohio
Join top CEOs, venture investors, medical leaders
and journalists as they highlight new technologies,
economics and the newest innovations in cancer
therapeutics, diagnostics and disease manage-
ment. The 7th Annual Medical Innovation Summit
offers an exciting lineup of speakers, panel discus-
sions, live surgeries and clinical presentations to
learn about the latest trends in medical innovation
and what they mean to you.
The Summit provides an unrivaled perspective on
the newest medical technologies and the financial
drivers behind those innovations. It is dedicated to
providing singular insights, networking opportuni-
ties and actionable take away for all participants.
Once again, the summit also will include the
unveiling of the “Top 10” Medical Innovations for
2010, with moderator Michael Roizen, MD, Chair-
man of Cleveland Clinic’s Wellness Institute.
For more information or to register, please visitclevelandclinic.org/2009Summit
REFERRALS24/7 Hospital Transfers/Physician Consults800.553.5056
Taussig Cancer InstituteAppointments/Referrals216.444.7923 ortoll-free 866.223.8100
Bone Marrow Transplantation Appointments/Referrals216.445.5660 or800.223.2273, ext. 55600
Bone Marrow Failure Clinic Appointments/ReferralsThis subspecialty clinic offers expertise in aplastic anemia, myelodysplasia, single-lineage cytopenias, paroxysmal nocturnal hemoglobinuria, large granular lymphocytic leukemia and other immune mediated hematologic diseases.
216.445.5962 or800.223.2273, ext. 55962
Radiation OncologyAppointments/Referrals216.444.5571 or800.223.2273, ext. 45571
ONLINE ACCESSto Your Patient’s Treatment ProgressWhether you are referring from near or far, Cleveland Clinic’s DrConnect stream-lines communication from Cleveland Clinic physicians to your office. This online tool offers you secure access to your patient’s treatment progress at Cleveland Clinic. With one-click convenience, you can track your patient’s care using the secure DrConnect Web site.
To establish a DrConnect account, please visit clevelandclinic.org or email drconnect@ ccf.org.
INSTITUTE LOCATIONSCleveland ClinicTaussig Cancer Institute9500 Euclid Ave./R35Cleveland, OH 44195216.444.7923
BeachwoodFamily Health and Surgery Center26900 Cedar RoadBeachwood, OH 44122216.839.3000 or 800.801.2233
Fairview Hospital18101 Lorain AvenueCleveland, OH 44111216.476.7000
Hillcrest Hospital6780 Mayfield RoadMayfield Heights, OH 44124440.312.4500
IndependenceCancer Center6100 Westcreek Road, Ste. 15 & 16Independence, OH 44131216.524.7979, Medical Oncology216.447.9747, Radiation Oncology
LorainFamily Health and Surgery Center5700 Cooper Foster Park RoadLorain, OH 44053440.204.7400 or 800.272.2676
ParmaCommunity Hospital6525 Powers Blvd.Parma, OH 44129440.743.4747
StrongsvilleFamily Health and Surgery Center16761 SouthPark CenterStrongsville, OH 44136440.878.2500 or 800.239.1098
Willoughby HillsFamily Health Center2570 SOM Center RoadWilloughby Hills, OH 44094440.943.2500 or 800.807.2888
Wooster Family Health Center1740 Cleveland RoadWooster, OH 44691
330.287.4500 or 800.451.9870