AUTONOMY AND
COLLABORATION PRACTICES
AMONG CRITICAL CARE NURSES
IN CYPRUS
Ε. Georgiou BSc Hons, MSc, PhD Cand. (Cyprus University of Technology)
Α. Pavlakis PhD (Open University of Cyprus)
Ε. Papathanasoglou MSc, PhD (Cyprus University of Technology)
OPERATIONAL DEFINITIONS
Autonomy is a composite multi-factorial phenomenon spanning a wide array of behaviours hence it is complex to define and measure.
The comprehensive definition provided by Varjus et al (2003) is adopted: Autonomy is defined as independence, right and responsibility in decision-making, in actions and in values
OPERATIONAL DEFINITIONS
Collaboration/Co-operation is defined as
nurses and physicians working together,
sharing responsibility for solving problems,
and making decisions to formulate and
carry out plans for patient care. It may be
conceptualized both at the individual-
patient decision level and at the level of
ICU organization (Baggs et al 1999).

LITERATURE REVIEW
Nursing Autonomy has been found to be positively related to:– Improved patients Outcomes (Wade, 1999),
– Nurses job satisfaction (Erlen & Sereika 1997, Budgeet al. 2003)
– Recruitment and retain of nurses in the Profession (Curley 2002, Parahoo 2000)
– The practice of Evidence Based Nursing (Parahoo 2000).
Autonomy in ICU
ICU Nurses role in clinical decision making is crucial :
Care for critically ill patients that are vulnerable to crisis situations in a high technology unit that most of the times complicates decision making
The rapid changes of the health status of the patient that happen in ICU demand high level decisions from the Nurse in a climate of high time stress
– Bucknall (2000), reported that ICU nurses were likely to make a patient care decision every 30 seconds, including a wide range of decisions from grand to trivial ones.,
– Watson (1994) reported that nurses made approximately nine important patient-care decisions per hour.
Collaboration between Nurses and
Doctors in ICUBetter professional relationships and better patients outcomes
( Baggs et al 1999, Dechairo-Marino,et al 2001 )
Minimization of medical errors (Dougherty & Larson 2005).
Recruitment and retain of staff in ‘Magnet’ Hospitals
Collaboration may be regarded both as a precondition and an outcome of autonomy
Purpose of the study
To explore the level of critical and
intensive care nurses’ autonomy in Cyprus
and to assess potential associations with
nurse-physician collaboration.
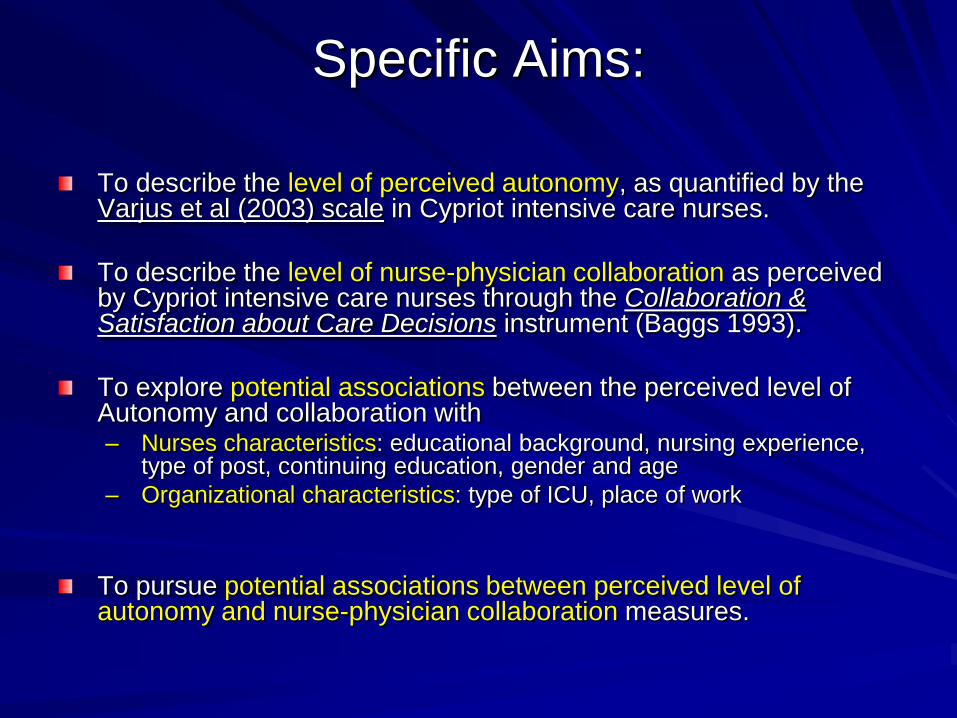
Specific Aims:
To describe the level of perceived autonomy, as quantified by the Varjus et al (2003) scale in Cypriot intensive care nurses.
To describe the level of nurse-physician collaboration as perceived by Cypriot intensive care nurses through the Collaboration & Satisfaction about Care Decisions instrument (Baggs 1993).
To explore potential associations between the perceived level of Autonomy and collaboration with– Nurses characteristics: educational background, nursing experience,
type of post, continuing education, gender and age
– Organizational characteristics: type of ICU, place of work
To pursue potential associations between perceived level of autonomy and nurse-physician collaboration measures.
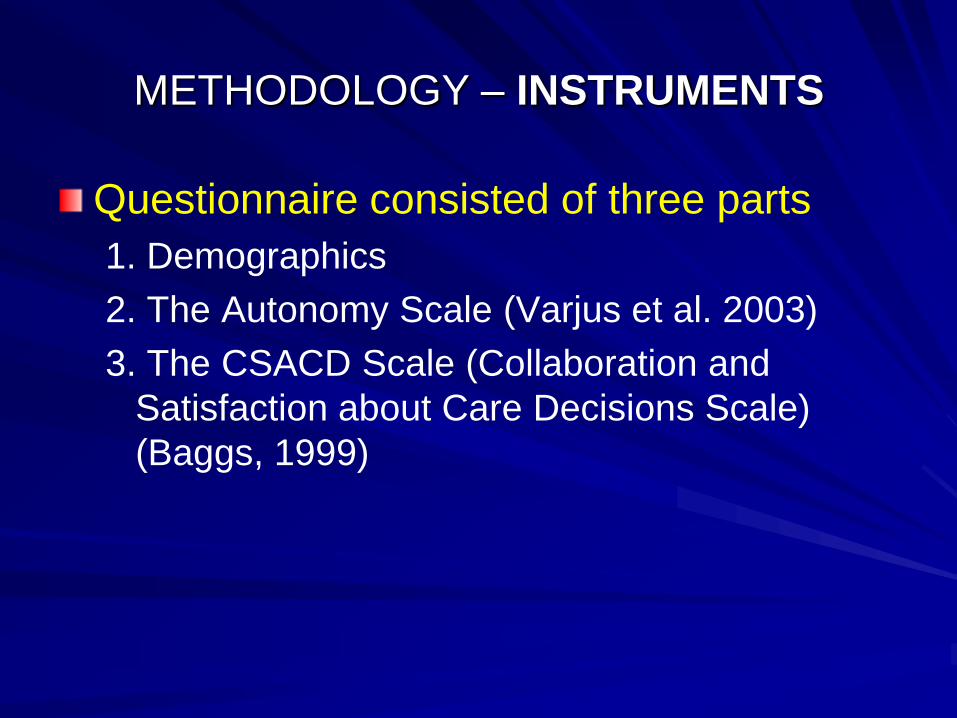
METHODOLOGY – INSTRUMENTS
Questionnaire consisted of three parts
1. Demographics
2. The Autonomy Scale (Varjus et al. 2003)
3. The CSACD Scale (Collaboration and
Satisfaction about Care Decisions Scale)
(Baggs, 1999)
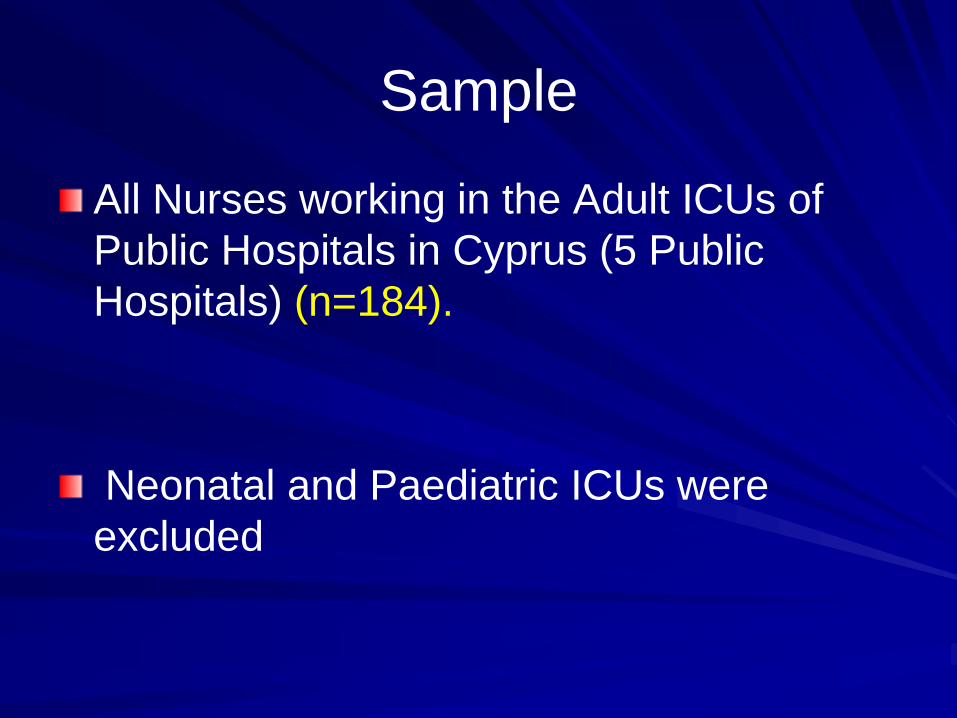
Sample
All Nurses working in the Adult ICUs of
Public Hospitals in Cyprus (5 Public
Hospitals) (n=184).
Neonatal and Paediatric ICUs were
excluded
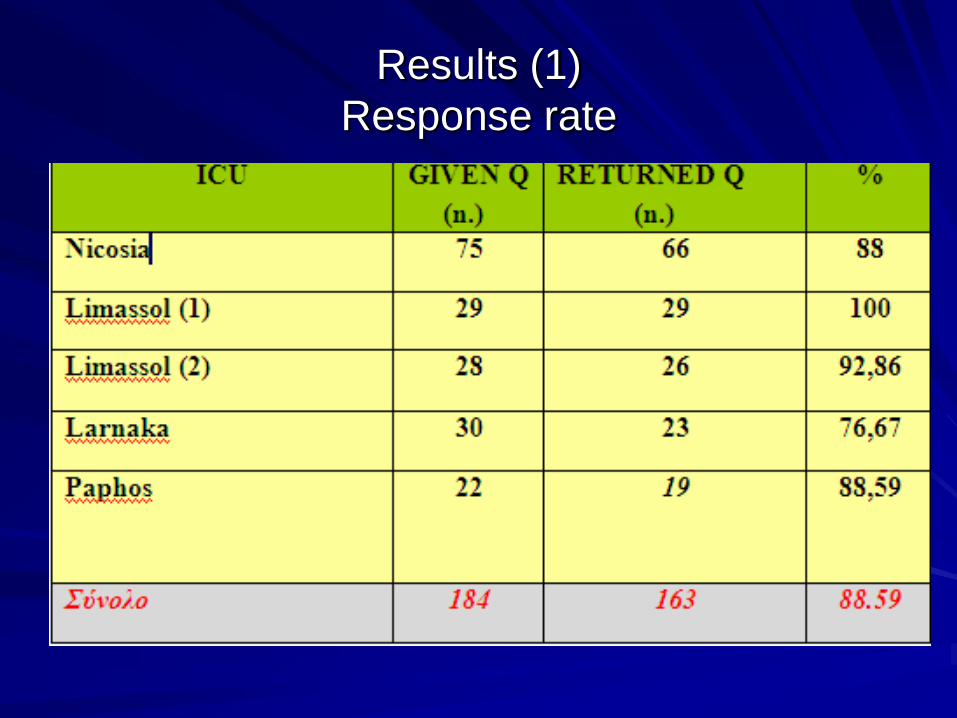
Results (1)
Response rate

Sample Characteristics
The age of participants
22 -57 years (Mean =33.8, SD =8.85).
Professional experience in the nursing profession
Mean = 11.56 years (SD 9.03)
Professional experience in ICU
Mean = 7.01 years (1 month - 30 years,
SD= 6.44).
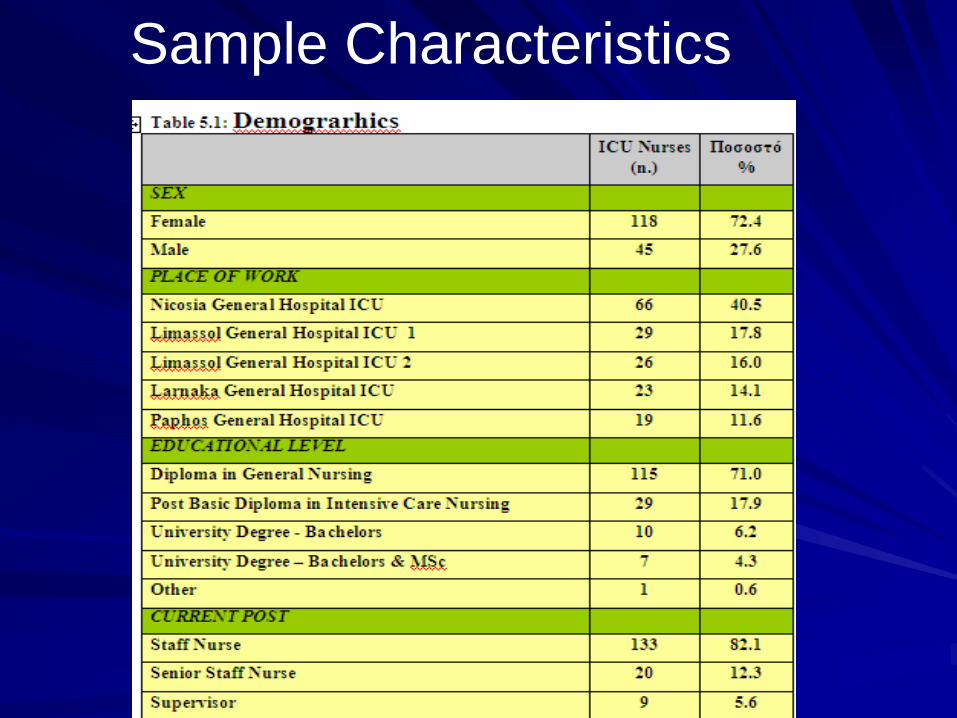
Sample Characteristics
Results (2)
Most of the nurses considered independence and
Autonomy in their job as important (Mean 8.33, Likert
Scale 1-10 10=very important, SD=1.48).
Almost all nurses (> 85%) felt responsible for their own
work and actions and the progress of their patients
However Autonomy level of Cypriot ICU Nurses is
moderate (Mean=4.23, Likert Scale 1-6, 6= Completely
agree SD=0.92).
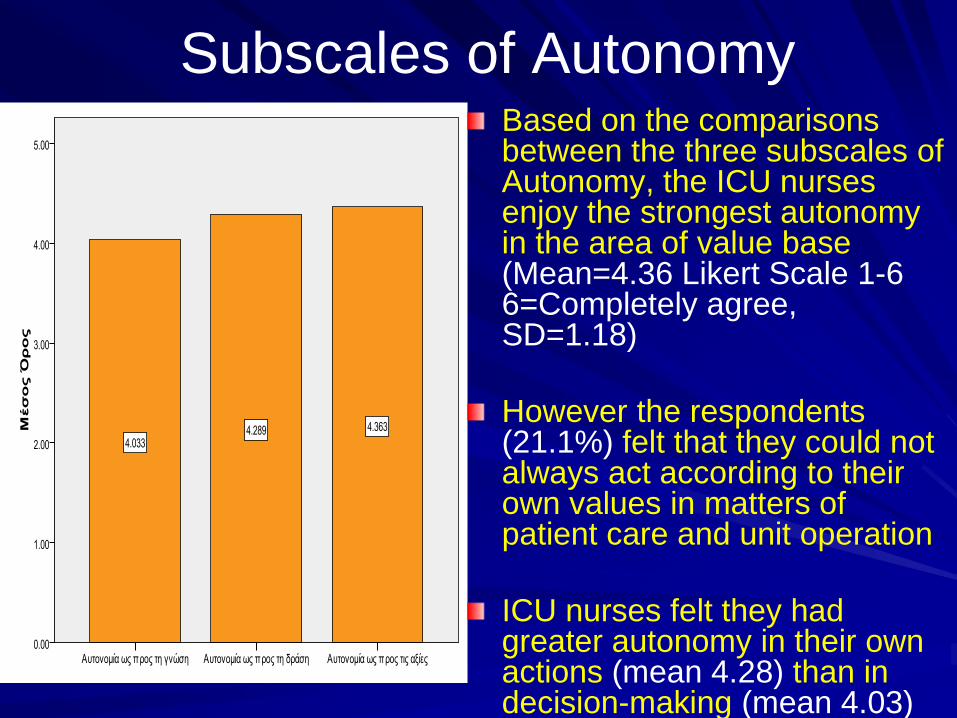
Subscales of Autonomy Based on the comparisons between the three subscales of Autonomy, the ICU nurses enjoy the strongest autonomy in the area of value base(Mean=4.36 Likert Scale 1-6 6=Completely agree, SD=1.18)
However the respondents(21.1%) felt that they could not always act according to their own values in matters of patient care and unit operation
ICU nurses felt they had greater autonomy in their own actions (mean 4.28) than indecision-making (mean 4.03)
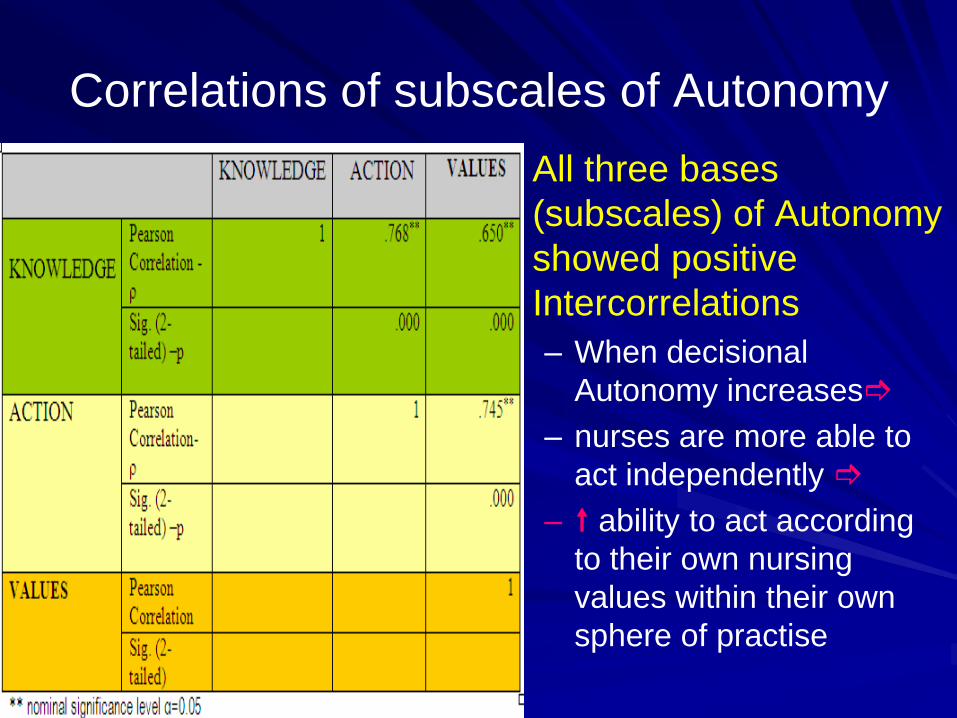
Correlations of subscales of Autonomy
All three bases
(subscales) of Autonomy
showed positive
Intercorrelations
– When decisional
Autonomy increases
– nurses are more able to
act independently
– ability to act according
to their own nursing
values within their own
sphere of practise
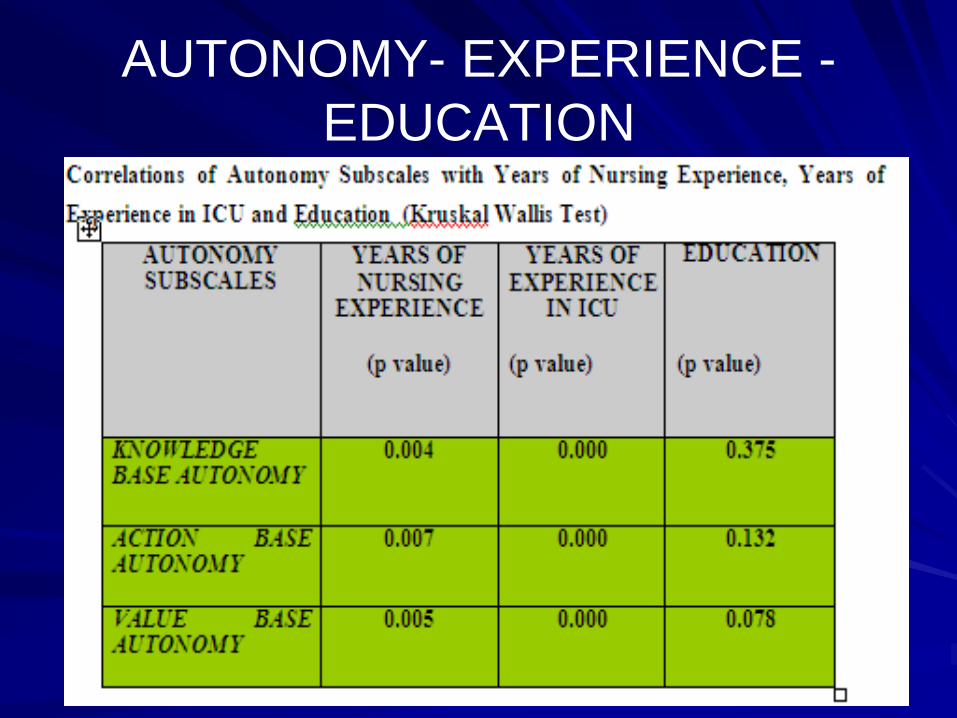
AUTONOMY- EXPERIENCE -
EDUCATION
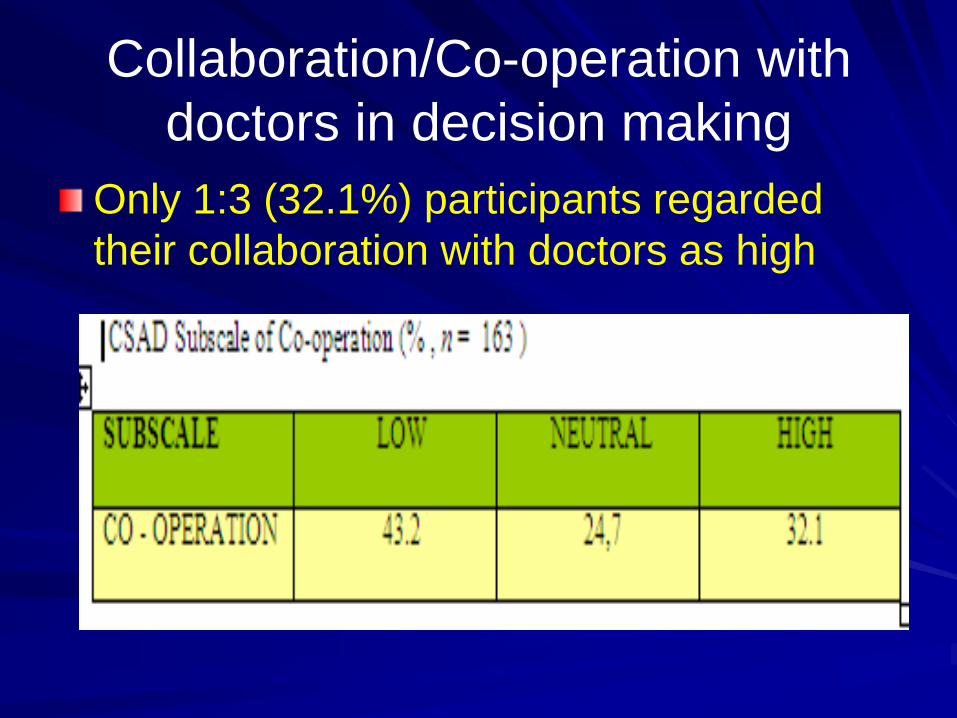
Collaboration/Co-operation with
doctors in decision making
Only 1:3 (32.1%) participants regarded
their collaboration with doctors as high
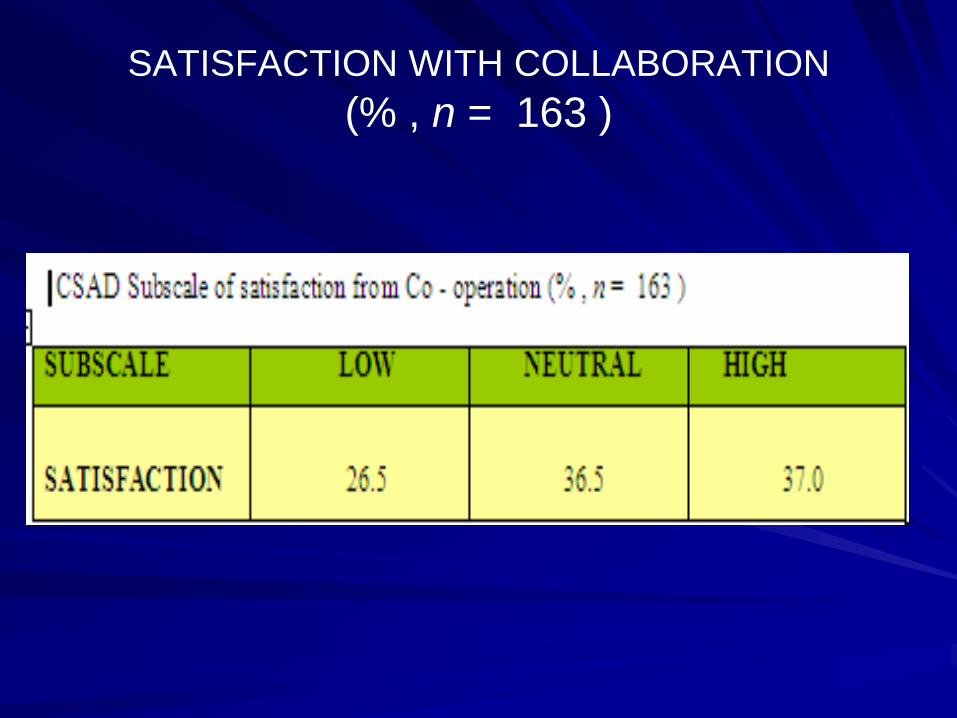
SATISFACTION WITH COLLABORATION
(% , n = 163 )
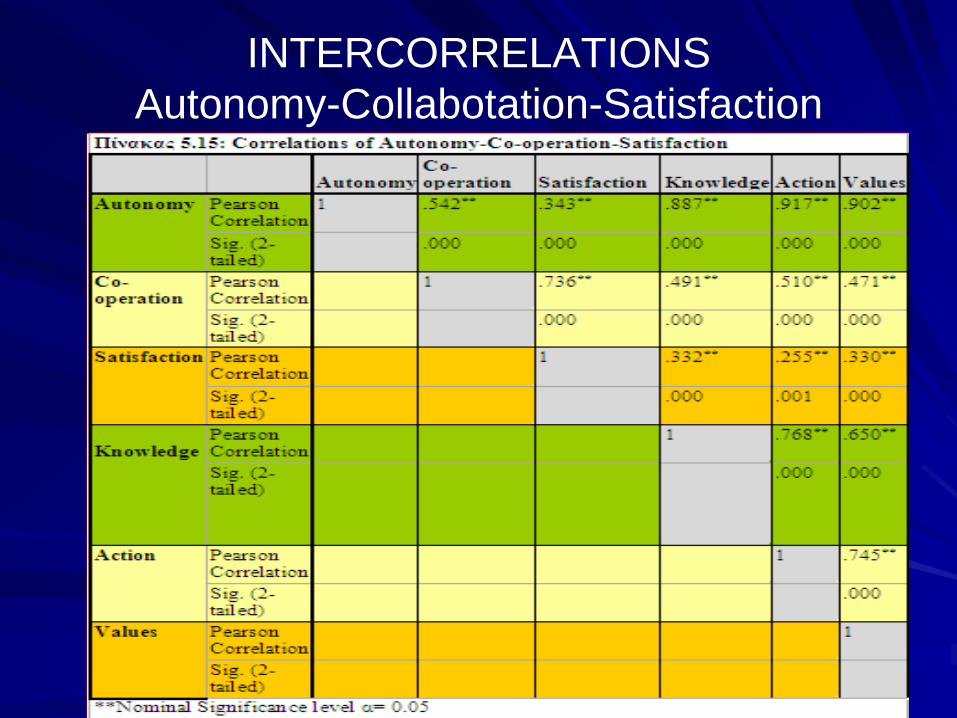
INTERCORRELATIONS
Autonomy-Collabotation-Satisfaction

Conclusions
The Cypriot ICU Nurses level of Autonomy is moderate
ICU nurses felt they had greater autonomy in their own actions than in decision-making.
Nurse-physician collaboration in the decision making process was low
Most of the nurses were dissatisfied with their collaboration with doctors regarding the decision making of patient care
Conclusions
The strong association observed between teamwork and autonomy suggests that synergy rather than conflict may empower nurses and enhance their autonomy.
Autonomous nursing practice and collegial/collaborative nurse-physician relationships are essential for ICU nurses’ satisfaction
Therefore……..
The ICU nurse managers in Cyprus need to implement strategies to promote, support and enhance:
1. nurses decisional autonomy, since clinical decision-making is a complex, constant and intensive aspect of ICU nursing.
2. collegial/collaborative nurse-physician relationships since they are strong determinants of healthy work environments.

This is how Cyprus looks this time
of the year
CYPRUS IN SPRING