Ashwin HaridasAsem Ali AshrafAdam Ebrahim

DefinitionsStroke
Clinical syndrome of rapid onset of focal deficits of brain function lasting more than 24 hours or leading to death
Transient Ischemic attack (TIA)Clinical syndrome of rapid onset of focal
deficits of brain function which resolves within 24 hours
Amaurosis fugax

DefinitionsProgressive Stroke
A stroke in which the focal neurological deficits worsen with time
Also called stroke in evolution
Completed StrokeA stroke in which the focal neurological deficits
persist and do not worsen with time

EpidemiologyThird most common cause of death after
cancer and ischeamic heart diseaseMost common cause of severe physical
disabilityPrevalence of stroke in India is about 1.54
per 1000Death rate is about 0.6 per 1000Incidence and prevalence of stroke is on the
rise due to increasing adoption of unhealthy lifestyle & an increasing life expectancy

Stroke Risk Factors
FixedAgeGender
(Male>Female)Race (Afro-
Caribbean>Asian>European)
HeredityPrevious vascular
event eg. MI, peripheral embolism
High fibinogen
ModifiableHypertensionHeart disease
(Atrial fibrillation, endocarditis)
Diabetes mellitusHyperlipidaemiaSmokingExcess alcohol
consumptionOral contraceptives

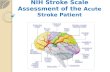
Anterior Circulation
Posterior Circulation

Middle Cerebral Artery

Anterior Cerebral Artery

Posterior Cerebral Artery

Types of StrokeIschemicHemorrhagic

Ischemic Stroke80% of strokesArterial occlusion of an intracranial vessel
leads to hypoperfusion of the brain region it supplies
Two etiological typesThromboticEmbolic

Etiology of ischemic strokeThrombotic
Lacunar strokeLarge vessel
thrombosisHypercoagulable
disorders
EmbolicArtery to artery
Carotid bifurcation Aortic arch
Cardioembolic Atrial fibrillation Myocardial infarction Mural thrombus Bacterial endocarditis Mitral stenosis Paradoxical embolus

Thrombotic Stroke
Atherosclerosis is the most common pathology leading to thrombotic occlusion of blood vessels
Hypercoagulable disorders – uncommon causeAntiphospholipid syndromeSickle cell anemiaPolycythemia veraHomocysteinemia
Vasculitis: PAN, Wegener’s granulomatosis, giant cell arteritis

Lacunar strokeAccounts for 20% of all strokesResults from occlusion of small deep
penetrating arteries of the brainPathology: lipohyalinosis & microatheromaThrombosis leads to small infarcts known as
lacunesClinically manifested as lacunar syndromes
Thrombotic Stroke

Embolic StrokeCardioembolic stroke
Embolus from the heart gets lodged in intracranial vessels
MCA most commonly affectedAtrial fibrillation is the most common causeOthers: MI, prosthetic valves, rheumatic heart disease
Artery to artery embolismThrombus formed on atherosclerotic plaques gets
embolized to intracranial vesselsCarotid bifurcation atherosclerosis is the most common
sourceOthers: aortic arch, vertebral arteries etc.

Etiology of ischemic stroke

Blood supply to the brain is autoregulatedBlood flow
If zero leads to death of brain tissue within 4-10min
<16-18ml/100g tissue/min infarction within an hour
Ischemia leads to development of an ischemic core and an ischemic penumbra
Pathophysiology of Ischemic Stroke


Ischemic Penumbra
Tissue surrounding the core region of infarction which is ischemic but reversibly dysfunctional
Maintained by collateralsCan be salvaged if reperfused in
timePrimary goal of revascuralization
therapies

ATP depletion
Hypoperfusion
Failure of Na+/K+ ATPase membrane ionic pump
Calcium entryGlutamate release
Activation of lipid peroxidases, proteases & NO synthase
Destruction of intracellular organelles, cell membrane & release of free radicals
Free fatty acid release
Activation of pro-coagulant pathways
Liquefactive necrosis
Thrombus/embolus
Membrane depolarization & cytotoxic cellular edema

Hemorrhagic Stroke
Two typesIntracerebral
hemorrhage(ICH)Subarachnoid
hemorrhage(SAH)Higher mortality
rates when compared to ischemic stroke

Intracerebral Hemorrhage• Result of chronic hypertension• Small arteries are damaged due to
hypertension• In advanced stages vessel wall is disrupted
and leads to leakage• Other causes: amyloid angiopathy,
anticoagulant therapy, cavernous hemangioma, cocaine, amphetamines

Subarachnoid HemorrhageMost common cause is rupture of saccular or
Berry aneurysmsOther causes include arteriovenous
malformations, angiomas, mycotic aneurysmal rupture etc.
Associated with extremely severe headache

Pathophysiology Of Hemorrhagic Stroke
Explosive entry of blood into the brain parenchyma structurally disrupts neurons
White matter fibre tracts are splitImmediate cessation of neuronal functionExpanding hemorrhage can act as a mass
lesion and cause further progression of neurological deficits
Large hemorrhages can cause transtentorial coning and rapid death

CLINICAL FEATURES

HistoryAsk for onset and progression of neurological
symptoms – completed stroke or stroke in evolution
History of previous TIAs & amaurosis fugax
History of hypertension & diabetes mellitus
History of heart conditions like arrhythmias, RHD & prosthetic valves

History of seizures & migraine
History of anticoagulant therapy
History of oral contraceptive use
History of any hypercoagulable disorders like sickle cell anemia & polycythemia vera
Substance abuse: cocaine, amphetamines
History

Examination of a stroke patientThe neurological examination is highly
variable and depends on the location of the vascular lesion.
Skin: look for xanthelasma,rashes (arteritis,splinter haemorrhages,livedo reticularis),limb ischemia(DVT)
Eyes:look for diabetic changes,retinal emboli,hypertensive changes,arcus senilis(refer to ophthalmologist)

Examination of a stroke patientCVS: hyper/hypotension, abnormal
rhythm(atrial fibrillation),murmurs(valvular anomaly),raised JVP(heart failure),peripheral pulses and bruits(generalised arteriopathy)
Respiratory system: pulmonary edema, infection
Abdomen: urinary retentionLocomotor system: injuries sustained
during collapse with stroke, comorbities which influence functional abilities.

General featureMost cerebrovascular diseases are manifest
by the abrupt onset of a focal neurologic deficit, as if the patient was "struck by the hand of God.”
The clinical manifestations of stroke are highly variable because of the complex anatomy of the brain and its vasculature.

‘HAND OF GOD’

CLINICAL CLASSIFICATION


Stroke SyndromesStroke syndromes are divided into: (1) large-
vessel stroke within the anterior circulation (2) large-vessel stroke within the posterior
circulation,and (3) small-vessel disease of either vascular
bed.

Stroke Within the Anterior CirculationThe internal carotid artery and its branches
comprise the anterior circulation of the brain i.e the anterior and middle cerebral arteries

Middle cerebral arterySigns and symptoms: Structures involvedParalysis of the contralateral face, arm, and
leg; sensory impairment over the same area: Somatic motor area
Motor aphasia: Motor speech area of the dominant hemisphere
Central aphasia:Central, suprasylvian speech area and parietooccipital cortex of the dominant hemisphere
Conduction aphasia: Central speech area (parietal operculum)

Cont….Homonymous hemianopia (often homonymous inferior
quadrantanopia): Optic radiation deep to second temporal convolution
Paralysis of conjugate gaze to the opposite side: Frontal contraversive eye field or projecting fibers
Central aphasia:Central, suprasylvian speech area and parietooccipital cortex of the dominant hemisphere
Conduction aphasia: Central speech area (parietal operculum)
Homonymous hemianopia (often homonymous inferior quadrantanopia): Optic radiation deep to second temporal convolution

Cont..Apractognosia(agnosia +apraxia) of the nondominant
hemisphere:Nondominant parietal lobe (area corresponding to speech area in dominant hemisphere); loss of topographic memory is usually due to a nondominant lesion, occasionally to a dominant one.
Apraxia is a neurological disorder characterized by loss of the ability to execute or carry out learned purposeful movements, despite having the desire and the physical ability to perform the movements. It is a disorder of motor planning.
Agnosia (a-gnosis, "non-knowledge", or loss of knowledge) is a loss of ability to recognize objects, persons, sounds, shapes, or smells while the specific sense is not defective nor is there any significant memory loss

Deficits Due To ACA OcclussionOcclusion of the anterior cerebral artery may result
in the following defects:If stroke occurs prior to the anterior communicating
artery it is usually well tolerated secondary to collateral circulation
Paralysis of the contralateral foot and leg Sensory loss in the contralateral foot and leg Left sided strokes may develop transcortical motor
aphasia Gait apraxia Urinary incontinence which usually occurs with
bilateral damage in the acute phase

Internal Carotid ArteryThe clinical picture of internal carotid
occlusion varies depending on whether the cause of ischemia is propagated thrombus, embolism, or low flow. The cortex supplied by the MCA territory is affected most often. With a competent circle of Willis, occlusion may go unnoticed.

Internal Carotid ArteryIf the thrombus propagates up the internal
carotid artery into the MCA or embolizes it, symptoms are identical to proximal MCA occlusion.
Sometimes there is massive infarction of the entire deep white matter and cortical surface.

Internal Carotid ArteryWhen the origins of both the ACA and
MCA are occluded at the top of the carotid artery, abulia or stupor occurs with hemiplegia, hemianesthesia, and aphasia or anosognosia. When the PCA arises from the internal carotid artery (a configuration called a fetal posterior cerebral artery), it may also become occluded and give rise to symptoms referable to its peripheral territory

Internal Carotid ArteryIn addition to supplying the ipsilateral brain,
the internal carotid artery perfuses the optic nerve and retina via the ophthalmic artery. In ~25% of symptomatic internal carotid disease, recurrent transient monocular blindness (amaurosis fugax) warns of the lesion. Patients typically describe a horizontal shade that sweeps down or up across the field of vision

Internal Carotid ArteryA high-pitched prolonged carotid bruit fading
into diastole is often associated with tightly stenotic lesions. As the stenosis grows tighter and flow distal to the stenosis becomes reduced, the bruit becomes fainter and may disappear when occlusion is imminent.

Posterior CirculationDYSARTHRIA & FACIAL
NUMBNESSATAXIA & HORNER’S SYNDROMEFACIAL WEAKNESS(LMN)HEMIPARESISHEMISENSORY LOSSHEMIANOPIALOSS OF CONSCIOSNESSDIPLOPIA, VERTIGO, VOMITING

CLASSICAL PRESENTATIONSTHROMBOTICH/O TIASTROKE IN
EVOLUTIONUSUALLY HAPPENS
EARLY MORNING
EMBOLICPATIENTS WITH
KNOWN HEART DISEASE LIKE IHD, VALVULAR HEART DISEASE
RAPID RECOVERYHAEMORRHAGIC STROKE IN
HYPERTENSIVE PATIENTS
ASSOCIATED WITH EMOTIONAL EXCITEMENT
HEADACHE & VOMITING

DIFFERENTIAL DIAGNOSISSPACE OCCUPYING LESION(TUMOR)SEIZUREMIGRAINESUBDURAL HAEMATOMAMETABOLIC DISTURBANCE LIKE
HYPOGLYCAEMIA

HypoglycemiaThat transient hypoglycemia may produce
a stroke like picture with hemiplegia and aphasia has been known for years.
The wide use of bedside rapid laboratory testing for glucose now makes this easily detectable and treatable. The hemiplegia may resolve immediately with the administration of intravenous glucose but resolution over a hours is also reported

Space Occupying LesionsSubacute or chronic duration of symptoms,
however some patients may present with acutely probably due to bleeding into a tumour
Associated with deep seated bursting headache, projectile vomiting due raised ICT

SEIZURES AND POST ICTAL STATESTraditional thought is that these postictal
symptoms are manifestations of seizure-induced alterations in neuronal function that are reversible; structural neuronal alterations are not present. The postictal weakness or Todd’s paralysis usually follows partial motor seizures but may follow generalized seizures as well. Duration is usually brief but may last 48 hours

MIGRAINEMigraine may actually precipitate a stroke, but
there is also a variant of migraine, hemiplegic migraine, where unilateral hemiparesis outlasts the headache. This is difficult if not impossible to diagnose correctly at first presentation when it must be regarded as a diagnosis of exclusion; only with recurrent, stereotypic attacks can this be suspected. Cases with alternating hemiplegia have been reported. At times this disorder has been shown to be familial.

SUMMARYRapid onset focal deficit of brain function
confirms strokeOnset and progression will decide the
aetiologyPrecise history of deficit will decide the site
of lesion


INVESTIGATION OBJECTIVES To confirm the vascular nature of the lesion
The pathological type of the vascular lesion
The underlying vascular disease
Risk factors present

INVESTIGATION MODALITIES: BRAIN
NON-INVASIVECT ScanMRI ScanMR AngiographyDoppler UltrasoundEEGPETSPECT
INVASIVELumbar PunctureContrast Angiography (Cerebral
Arteriography)CT Angiography

PATHOLOGICAL TYPES
STROKE
HAEMORRHAGIC ISCHAEMIC

CT SCANMandatory initial investigationHaemorrhage appears instantly as a hyperdense
areaInfarct appears as a hypodense areaInfarct may not appear before 48 hrsMRI may be done instead but ct scan is more
sensitive for detecting haemorrhageDiffusion weighted MRI is good for identifying
ischaemic lesion


ISCHAEMIC LESION

STROKE PATIENT
CT SCAN/MRI
VASCULAR NATURE CONFIRMED
HAEMORRHAGE ISCHAEMIA
Cont’d…

SEARCH FOR SOURCE
CEREBRAL ARTERIOGRAPHY MRA/CTA DOPPLER PET/SPECT
SEARCH FOR SOURCE
Cont’d…


Carotid Artery Ultrasound Showing a Completely Calcified Atherosclerotic Plaque


3-D reconstruction of CT angiogram showing stenosis at the carotid bifurcation

Intra-arterial angiography showing arteriovenous malformation

MR angiogram showing giant aneurysm at the middle cerebral artery bifurcation

NORMAL CT SCAN
HAEMORRHAGESUSPECTED
LUMBAR PUNCTURE
CSF WITH BLOOD/XANTHOCHROMIA
HAEMORRHAGE CONFIRMED

UNDERLYING DISEASECerebral vasculature
Abnormalities like aneurysms orAV malformations
Cerebral angiographyVascular imaging – MRA/CTA or doppler (non
invasive)

CARDIOVASCULAR
Like MI, atrial fibrillation, valvular diseases etc.
ElectrocardiogramChest X-RayEchocardiographyTransesophageal ultrasoundHolter monitoring(paroxysmal nocturnal
arrhythmia)Blood cultures
UNDERLYING DISEASE

UNDERLYING DISEASESerum lipids for hyperlipidemiaANA for SLEMR Angiography for arterial dissectionLupus anticoagulant for antiphospholipid
antibody syndromeESR, CRP, ANCA for vasculitisPT, aPTT, Platelet count for bleeding
disordersProteins C & S for hypercoagulability

TREATMENT OBJECTIVES
1. MINIMIZE VOLUME OF BRAIN IRREVERSIBLY DAMAGED
2. PREVENT COMPLICATIONS
3. REHABILITATION
4. REDUCE RISK OF RECCURENCE

MANAGEMENT OF A TRANSIENT ISCHAEMIC ATTACK (TIA) MEDICAL MANAGEMENT (if diffuse atherosclerotic disease or poor operative
candidates)
1.Stop smoking2.Concurrent medical problems to be addressed:
Emboli from heart and other parts of cardiovascular system
(a) anti coagulants: Heparin(IV), Warfarin(oral)(b) anti platelet drugs: Aspirin(oral), Ticlopidine Diabetes, Hypertension, Hyperlipidemia

MANAGEMENT OF A TRANSIENT ISCHAEMIC ATTACK(TIA) – Cont’d
SURGICAL MANAGEMENT
CAROTID AND CEREBRAL ARTERIOGRAPHY
STENOSISMild to Moderate Severe
Regular Follow Up Carotid Endarterectomy
All above can be done only if there is relatively little atherosclerosis elsewhere in cerebrovascular system.

MANAGEMENT OF AN ACUTE EPISODE OF STROKE
AIRWAY - Maintain airway, prevent aspiration, keep nil per oral
BREATHING - Maintain oxygen saturation > 97% - Supplementary oxygen
CIRCULATION - Adequacy of pulse and BP - Fluid, Anti Arrhythmics, Ionotropes
HYDRATION - Prevent dehydration ; give adequate fluids - Parenteral or via nasogastric tube
NUTRITION - Nutritional supplements and Nasogatric feeding
MEDICATION - Administer medication also by routes other than oral

MANAGEMENT OF AN ACUTE EPISODE OF STROKE Cont’d
BLOOD PRESSURE - unless indicated (heart or renal failure,hypertensive encephalopathy or aortic dissection) it should not be lowered for the fear of expansion of infarct.Ischaemic stroke - maintain 180/110 mm Hg Haemorrhagic stroke – keep MAP <115 mm Hg
BLOOD GLUCOSE - INSULIN to treat hyperglycaemia(can increase infarct size)
- maintain < 200mg% TEMPERATURE - early use of antipyretics PRESSURE AREAS – To prevent occurrence of decubitus
ulcers INCONTINENCE

EARLY MANAGEMENT


ISCHAEMIC STROKETHROMBOLYTICS and REVASCULARISATION - - tPA (alteplase)-0.9mg/kg(max 90mg) 10% of dose – initial IV bolus remainder infused over one hour - to be used < 3 hrs of onset of symptoms (for maximum efficacy) - haemorrhage to be ruled out
NEUROPROTECTIVE AGENTS

ANTI PLATELET THERAPYAsprin, Clopidogrel - act by inhibiting platelet aggregation and
adhesion. - aspirin 300mg single dose to be given
immediately following diagnosis. - if alteplase given it can be with held for 24 hrs. - later aspirin at a dose of 75 mg in combination
with clopidogrel 75 mg daily for about one year duration.

ANTI COAGULANTSHEPARINS , WARFARIN -heparins act by accelerating the inhibition of
factor II and factor X of coagulation cascade -warfarin antagonises vitamin K to prevent
activation of clotting factors -decrease risk of recurrence and venous
thromboembolism -intra cranial haemorrhage to be excluded before
therapy -more useful if stroke is evolving

ANTI COAGULANTS - Cont’dHYPEROSMOLAR AGENTS - reduce cerebral oedema - 20% mannitol IV – 100ml TID - oral glycerol if swallow is normalConcurrent medical problems such as atrial
fibrillations to be tackledOTHERS: - PENTOXYPHYLLINE (hemorrheology modifier) to be used within 12 hrs -NEUROPROTECTIVE AGENTS

HAEMORRHAGIC STROKE
Control of hypertensionControl coagulation abnormalities (esp due to
oral anticoagulants)Surgical decompressionSurgery for aneurysms and arterio-venous
malformationsAnti platelet Anti platelet and anti coagulants anti coagulants are
contraindicated

REHABILITATIONPHYSIOTHERAPY - as early as
possible - initially passive moments - later active movements - in every case early
mobilization - prevents contractures,
spasticity and atrophy
OCCUPATIONAL THERAPY

REHABILITATION - Cont’dSPEECH THERAPY
IMPROVE QUALITY OF LIFE WITH MOTOR AIDS -leg brace, toe spring , cane , walking stick

STROKE UNITS – A MULTIDISCIPLINARY APPROACHImmediate resuscitation , prevent
complications and recurrenceEmergency 24 hr evaluation and
comprehensive care Improves neurological outcomeReduces mortality1000 patients admitted to stroke units
saves the lives of atleast 5o patients at end of 6 months

SECONDARY PREVENTIONBlood pressure
controlDiabetes ManagementLipid ManagementSmoking CessationAlcohol Moderation Weight
Reduction/Physical Activity
Carotid Artery Interventions
Anti platelet agents / Anti coagulants
StatinsDiuretics +/- ACE
inhibitors

COMPLICATIONSDue to cortical brain injury(immediate) - Epilepsy/seizures - Cerebral oedema Residual deficits from stroke - Paralysis - Aphasia

COMPLICATIONS – Cont’d Due to immobility - Chest infections - Pressure sores - Deep vein thrombosis / pulmonary embolism - Painful shoulder - Urinary infection/constipation - Depression and anxiety

PROGNOSISISCHAEMIC STROKE
Mortality rate in first 30 days is 8-12% Can vary depending upon size, location,
symptoms of stroke Time that elapses from the event to medical
interventionFirst 3 hrs after stroke - GOLDEN PERIOD

PROGNOSIS – Cont’dINTRACEREBRAL HAEMORRHAGE
Mortality rate in first 30 days is almost 50%Site and extent of hematoma also plays a role in
determining the prognosisHamorrhagic strokes have a poor prognosis
compared to ischaemic type .