Anti-Aging Benefits of
CREATINENew Research Suggests Creatine Combats Muscle Loss,
Improves Brain Function, and May Modulate Inflammation
By Will Brink
C reatine is a nutrient with a long list of potential medical, exercise-enhancing, and anti-aging
applications. As discussed in the March 2003 issue o^ Life Extension, creatine may play a role in
preventing and treating diseases such as muscular dystrophy that affect the neuromuscular sys-
tem.' Creatine has potential therapeutic apphcations in aging populations and against disorders such as
wasting syndromes, muscle atrophy, fatigue, Parkinson's disease, and Huntington's disease, as well as mito-
chondrial disorders and brain pathologies. Another article in the September 2003 issue oi Life Extension
examined creatine's potential role in increasing growth hormone levels, reducing homocysteine levels, and
improving the symptoms of chronic fatigue syndrome.^
In this article, we will examine exciting new research on the use of creatine by older adults to fight age-
related muscle loss (sarcopenia), improve function in both healthy and damaged brains, and perhaps mod-
ulate inflammation. Crearine is proving ro be one of the most promising, well-researched, and safest
supplements ever discovered for an exceptionally wide range of uses. > > >
42
• * . j i ;^*-" C&.S?


What is creatine? In a nutshell,creatine helps the body generateenergy. Adenosine triphosphate(ATP), formed in the mitochon-dria, is often referred to as thebody's "universal energy molecule."When ATP loses a high-energyphosphate molecule to becomeadenosine diphosphate (ADP), itmust be converted back to ATPbefore it can be used again to pro-duce energy. Creatine, stored inthe body as creatine phosphate, candonate a phosphate group to ADP,thus recharging it to energy-pro-ducing ATP. By promoting fasterand more efficient recycling ofATP, creatine helps provide thefuel our bodies need to accomplishphysical and metabolic tasks.'
THE SCOURGE OE AGING:SARCOPENIA
In literally dozens of studies,creat ine has been shown toincrease strength and muscle massin young adults and to aid in reha-bilitative strength training."' Untilrecently, data concerning crea-tine's effects on older adults was
very limited. One of the greatestthreats faced by aging adults is thesteady loss of lean body mass(muscle) needed to maintain ahealthy, functional lifestyle. Themedical term for this loss of mus-cle tissue is sarcopenia, a conditionthat is only now getting the recog-nition it deserves by the medicaland scientific community.
Sarcopenia can be defined asthe age-related loss of musclemass, strength, and function. Fordecades, the medical communityhas focused on the loss of bonemass (osteoporosis) in agingadults, but has paid little attentionto the loss of muscle mass thatoccurs with aging. This loss ofmuscle mass can affect a person'sability to be functional, perhapseven more so than a loss of bonemass. As with most medical condi-tions, it is easier, less expensive,and more effective to prevent orslow the progression of this condi-tion than it is to treat it later inlife. Sarcopenia generally appearsin adults after the age of 40 andaccelerates after the age ofapproximately 75.
Although sarcopenia is mostlyseen in physically inactive adults, itis not uncommon in people whoremain physically active through-out their lives. Thus, while remain-ing physically active is essential toavoiding sarcopenia, physical inac-tivity is not the only contributingfactor to its development. Likeosteoporosis, sarcopenia is a multi-factorial process whose contribut-ing factors may include decreasedhormone levels (particularly ofgrowth hormone, insulin-likegrowth factor 1, and testosterone),lack of adequate protein and calo-ries in the diet, oxidative stress,inflammatory processes, and loss ofmotor nerve cells."'"
HOW CREATINE AFEECTSOLDER ADULTS
With aging and inactivity, musclewasting or atrophy most often occursin fast-twitch muscle fiber. Thesefibers, which are recruited duringhigh-intensity, low-endurance move-ments such as weight lifting andsprinting, are the most profoundlyaffected by creatine.
In a study examining creatine'seffect on isometric strength andbody composition, 28 healthy menand women over the age of 65received either five grams of crea-tine daily or a placebo.'̂ In this ran-dom, double-blind study, both thecreatine and placebo groups wereput on a resistance (weight) train-ing regimen. Fourteen weeks oftraining resulted in significantincreases in all measurements ofstrength, functional tasks, andmuscle fiber area in both groups.However, the creatine groupexperienced significantly greaterincreases in fat-free muscle mass,isometric knee extension strength,isometric dorsiflexion (ankle)strength, and intramuscular crea-tine levels. The researchers con-cluded, "the addition of creatine
44 LIFE EXTENSION April 2005

suppletnentation to the exercisestitnulus enhanced the increase intotal atid fat-free mass and gains inseveral indices of isometric musclestrength."^^
An abundatice of recent studieshas found creatine to have benefi-cial effects in older adults, espe-cially when combined with arcsistatice training protocol. Onestudy examined the effects of crea-tine supplementation on muscularperformance in older men over abrief time period." The studyauthors concluded, " . . . seven daysof creatine supplementation iseffective at increasing severalindices of muscle performance,including functional tests in oldermen without adverse side effects.Creatine supplementation may bea useful therapeutic strategy forolder adults to attenuate loss itimuscle strength and performanceof functional living tasks."
One especially noteworthy studyfound that crealine's positiveeffects on strength and lean tissuein older adults continued for atleast 12 weeks after they stoppedusing it.-" According to the studyauthors, "withdrawal from creatinehad no effect on the rate ofstrength, etidurancc, and loss of
lean tissue mass with 12 weeks ofreduced-volume training." Formost creatine users, however, opti-mal benefits occur with continuoususe of creatine, which is both safeand well tolerated.
THE SECRET TO AGING:CELLULAR ENERGY
What is one important differ-ence between an older and ayounger adult? The answer is cellu-lar energy: each cell's ability to pro-duce energy, detoxify harmfulcompounds, and defend itselfagainst free radical damage andother assaults. An increase inoxidative stress, coupled with acell's inability to produce essentialenergy molecules such as ATP, is ahallmark of aging and is present inmany disease states.''"^" While ayounger person's cells can effi-ciently meet these challenges, anolder person's cells are poorlyequipped to do so. Over time, dam-age accumulates in older cells, andcell death can occur. In youngerhealthy adults, healthy new cellsrapidly repair or replace older cells,but this process slows with age,
A decline in muscle mass withaging, or sarcopenia, may be relat-ed to a decline in mitochondrialfunction. Without optimal func-tioning of these energy generatorsthat arc found in every human cell,both the cell and the entire bodyexperience a decline in function.Research has established that olderadults tend to have lower tissue lev-els of creatine phosphate, ATP,and other essential high-energymolecules. Older adults are alsoless adept at replenishing theseessential molecules after exercise.
One study examined skeletalmuscle mitochondrial functionand lean body mass in healthy,exercising elderly adults.^' Thestudy measured mitochondrialfunction and recovery time in 45
older adults (with an average ageof 73) and 20 younger subjects(average age of 25) who werematched for body mass. The inves-tigators then had the two groupsexercise at different intensity lev-els. As other studies have found,the older adults had lower base-line creatine phosphate and ATPlevels than did their younger coun-terparts, and they were slower toreplenish tissue levels after exer-cise. As the researchers reported,"Our data suggest that mitoehon-drial function declines with age inhealthy, exercising elderly adultsand that the decline appears to beinfluenced by the level of physicalactivity," Thus, the older subjectsnot only had lower levels of essen-tial high-energy compounds tobegin with, but those levels werefurther diminished with moreintense exercise.
As studies in older adults show,creatine in supplemental form canameliorate some of the physiologi-cal decline that occurs with aging.Creatine may be one of the safest,most effective non-prescriptioncompounds currently available toimprove cellular energy.
April 2005 LIFE EXTENSION 45
CREAllNE'SANTI-INFLAMMATORY
EFFECTS
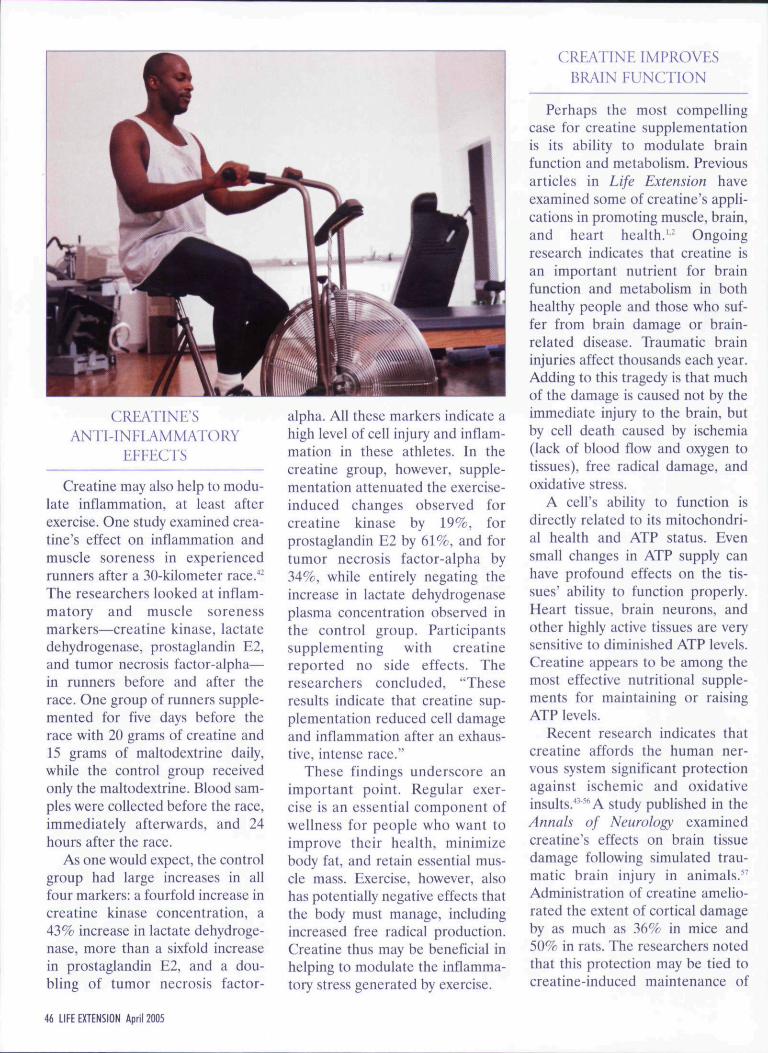
Creatine may also help to modu-late inflammation, at least afterexercise. One study examined crea-tine's effect on inflammation andmuscle soreness in experiencedrunners after a 30-kiIometer race.""-The researchers looked at inflam-matory and muscle sorenessmarkers—creatine kinase, lactatedehydrogenase, prostaglandin E2,and tumor necrosis factor-alpha—in runners before and after therace. One group of runners supple-mented for five days before therace with 20 grams of creatine and15 grams of maltodextrine daily,while the control group receivedonly the maltodextrine. Blood sam-ples were collected before the race,immediately afterwards, and 24hours after the race.
As one would expect, the controlgroup had large increases in allfour markers: a fourfold increase increatine kinase concentration, a43% increase in lactate dehydroge-nase, more than a sixfold increasein prostaglandin E2, and a dou-bling of tumor necrosis factor-
alpha. All these markers indicate ahigh level of cell injury and inflam-mation in these athletes. In thecreatine group, however, supple-mentation attenuated the exercise-induced changes observed forcreatine kinase by 19%, forprostaglandin E2 by 61%, and fortumor necrosis factor-alpha by34%, while entirely negating theincrease in lactate dehydrogenaseplasma concentration observed inthe control group. Participantssupplementing with creatinereported no side effects. Theresearchers concluded, "Theseresults indicate that creatine sup-plementation reduced cell damageand inflammation after an exhaus-tive, intense race."
These findings underscore animportant point. Regular exer-cise is an essential component ofwellness for people who want toimprove their health, minimizebody fat, and retain essential mus-cle mass. Exercise, however, alsohas potentially negative effects thatthe body must manage, includingincreased free radical production.Creatine thus may be beneficial inhelping to modulate the inflamma-tory stress generated by exercise.
CREATINE IMPROVESBRAIN FUNCTION
Perhaps the most compellingcase for creatine supplementationis its ability to modulate brainfunction and metabolism. Previousarticles in Life Extension haveexamined some of creatine's appli-cations in promoting muscle, brain,and heart health.'^ Ongoingresearch indicates that creatine isan important nutrient for brainfunction and metabolism in bothhealthy people and those who suf-fer from brain damage or brain-related disease. Traumatic braininjuries affect thousands each year.Adding to this tragedy is that muchof the damage is caused not by theimmediate injury to the brain, butby cell death caused by ischemia(lack of blood flow and oxygen totissues), free radical damage, andoxidative stress.
A cell's ability to function isdirectly related to its mitochondri-al health and ATP status. Evensmall changes in ATP supply canhave profound effects on the tis-sues' ability to function properly.Heart tissue, brain neurons, andother highly active tissues are verysensitive to diminished ATP levels.Creatine appears to be among themost effective nutritional supple-ments for maintaining or raisingATP levels.
Recent research indicates thatcreatine affords the human ner-vous system significant protectionagainst ischemic and oxidativeinsults.̂ '"'''A study published in theAnnals of Neurology examinedcreatine's effects on brain tissuedamage following simulated trau-matic brain injury in animals."Administration of creatine amelio-rated the extent of cortical damageby as much as 36% in mice and50% in rats. The researchers notedthat this protection may be tied tocreatine-induced maintenance of
46 LIFE EXTENSION April 2005
mitochondrial bioenergetics. Theyconcluded that creatine ". . . mayprovide clues to the mechanismsresponsible for neuronal loss aftertraumatic brain injury and may finduse as a neuroprotective agentagainst acute and delayed neurode-generative processes." This studysuggests that creatine therapyshould be initiated as soon as possi-ble after traumatic brain injury.People who have already beenusing creatine regularly may beafforded considerable protectionagainst additional brain damagefollowing such an injury.
Research also indicates thatcreatine improves brain functionin healthy adults. A recent dou-ble-blind, placebo-controlledcrossover study examined how sixweeks of ereatine supplementa-tion affected cognitive function inadult vegetarians.'" Subjects weregiven five grams of creatine daily.Following creatine supplementa-tion, the study participants demon-
strated improved scores on testsassessing intelligence and workingmemory. Creatine's effects may bedue to its ability to increase the cel-lular energy available to the brain.Although creatine supplementa-tion may have a less dramatic effecton non-vegetarians who obtainsome creatine from dietary sourcessuch as meat, it is likely that crea-tine benefits brain function in meateaters and vegetarians. Supple-mental creatine thus appears toimprove function and performancein healthy and injured brains alike.
CONCLUSION
Through its role in promoting anabundant pool of cellular energy,creatine helps support the healthyfunctioning of muscle, brain, andother body tissues. A substantialbody of research demonstrates thatcreatine is a safe and effective toolfor managing a wide range ofpathologies, and may be a powerful
COMBINING NUTRIENTS TO COMBAT SARCOPENIA
Creatine helps to build muscle mass, but may work even better when combinedwith other nutrients. Whey protein is well known for its ability to augment athletictraining, boost immunity, and increase levels of the body's primary Intracellular antiox-idant, glutathione."^" Many athletes and health-conscious people have made wheyprotein a regular part of their diet in order to reap its vast array of benefits. Glutamine,the body's most abundant amino add, is essential in supporting muscle mass, immu-nity, gut health, and more.'"" Together, creatine, whey protein, and giutamine offerpowerful anabolic support for building musde.
Life Extension has combined this dynamic trio of nutrients in its Creatine Whey Glu-tamine Powder formula. Unlike other formulas that contain minimal amounts of nutri-ents, two scoops of Creatine Whey Glutamine Powder provide 30 grams of CFM^^whey isolate, 6 grams of glutamine, and 4 grams of German micronized creatine. Thisformula is indicated not only for those fighting the muscle loss of sarcopenia, but forall adults who seek to optimize their body composition and protect against age-relat-ed disease.
A healthy meal substitution recipe that tastes great and contains an impressivearray of health benefits is one to three scoops of Creatine Whey Glutamine Powder,one cup of filtered water, one-half cup of juice, and one-half cup of frozen strawber-ries or other fruit blended to taste. For a true meal replacement beverage, add onetablespoon of an oil rich in omega-3 fatty adds, such as flaxseed oil or Udo's ChoiceOil Blend, and one to three scoops of Life Extension Mix^^ powder. This creates a trulyhealthy meal containing virtually every nutrient needed for optima! health and diseaseprevention.
anti-aging nutrient. Healthy adultsmay benefit from supplementingwith two to three grams of creatinedaily, while those seeking toaddress specific health concernssuch as muscle loss or brain injurymay benefit from five to ten gramsof creatine daily. •
Additional information on howcreatine and other supplements may
benefit athletes is available atwww. Muscle BuildingNutdtion. com.
REFERENCES
1. Available at: http:/Avww.lef.org/niagazine/mag2{)(B/mag2U03_03.html. AccessedDecember 17. 2004.
2. Available at: http://ww-w.lef.orgymagazinc/
mag2003/mag2()03_09.html. AccessedDecember 17. 2004.
3. Racette SB. Creatine supplementation andathletic performance. J Orthop Sports Pliys-
Tlier. 2003 Oct;33(10):615-21.
4. Hespel R Op't EB. Van Leemputte M. et al.
Oral creatine supplementation facilitates
the rehabilitation of disuse atrophy andalters the expression of muscle myogenicfactors in humans. J/'/i>'i/(;/. 2001 Oct
15:536(P( 2);625-33.
5. Jowko E, Ostaszewski P. Jank M. ct al. Cre-atine and beta-hydro.\y-beta-methylbutyrate
(HMB) additively increase lean body massand muscle strength during a weight-train-ing program. Nutrition. 2001 Ju!;17(7-8):558-
66.
April 2005 LIFE EXTENSION 47
SYNERGISTIC ACTIONOF WHEY AND CREATINE
Whey and creatine work better
together tban either does alone,
according to study results presented at
tbe 2003 Experimental Biology Meet-
ing in San Diego, CA."
Researchers at Victoria University
in Australia conducted a double-blind
trial in which 33 male subjects trained
in resistance exercise were assigned to
one of four groups receiving either
whey isolate, creatine and whey iso-
late, creatine and carbohydrate, or car-
bohydrate only. All participants
performed the same supervised exer-
cise regimen for 11 weeks.
While all groups demonstrated
increases in strength, those using
whey alone or in combination with
creatine had significantly larger gains
in strength, lean tissue mass, and
muscle fiber cross-sectional area. In
addition, the group using the creatine-
whey combination demonstrated a
greater increase in strength, lean
mass, and muscle fiber cross-sectional
area than did the whey-only group.
Tbe study reported a strong correla-
tion between tbe magnitude of
strength gained and increases in tbe
cross-sectional area of muscle fibers.
Commenting on the report, the Ameri-
can Physiological Society noted,
"...dietary strategies that enhance
the effects of resistance training have
important implications to athletes, an
aging population, and others that suf-
fer from debilitating conditions that
cause muscle wasting.""
6. Tarnopolsky MA, Parise G, Yardley NJ, et
al. Creatine-dextrose and protein-dextrose
induce similar strength gains during train-
ing. Med Sci Sports Exerc. 2O01
Dec;33(12):2(M4-52.
7. Becque MD, Lochmann JD. Melrose DR.
Effects of oral creatine supplementation on
muscular strength and body composition.
Med Sci Sports Exerc 2000 Mar;32(3):654-8.
8. Francaux M, Poortmans JR. Effects of train-
ing and creatine supplement on muscle
strength and body tnass. EurJAppl Physiol
Occup Physiol. 1999 JuI;80(2):165-8.
9. Clarkson PM, Rawson ES. Nutritional sup-
pletnents to increase muscle mass. Crit Rev
Food Sci NulK 1999 Jul;39(4):317-28.
10. Kreider RB, Ferreira M, Wilson M. el al.
Effects of creatine supplementation on body
composition, strength, and sprint perfor-
mance. A/eJ .Sd 5porr,v Etf/r. 1998
Jan;30(l):73-82.
11. Vandenberghe K, Gorls M. Van Hecke P, et
al. Long-term creatine intake is heneficial to
muscle performance during resistance train-
ing. J Appl Physiot. 1997 Dec;83{6):2055-63.
12. Balsom PD, Soderlund K, Sjodin B, Ekblom
B. Skelelal muscle metabolism during short
duration high-intensity exercise: influence of
creatine supplementation./icW Fhysiol
Scand. 1995 Jul;154(3):303-10.
13. Harris RC, Soderlund K, Hultman E. Eleva-
tion of creatine in resting and exercised
muscle of normal subjects by creatine sup-
plementation. Clin Sci (Land). 1992
Sep;83(3):367-74.
14. Fulle S, Protasi F, Di Tano G. et ai. The con-
tribution of reactive oxygen species to sar-
copenia and muscle ageing. Kxp Oeroniol.
2004Jan;39(l):17-24.
15. Yarasheski KE. Exercise, aging, and muscle
protein metabolism. J Gerontol A Biol Sci
Med Sci. 2003 Oct:58(10):M918-22.
16. Semba RD, Blaum C, Guralnik JM, et al.
Carotenoid and vitamin E status are associ-
ated with indicators of sarcopenia among
older women living in the community. Aging
Clin Exp Re.s. 2(103 Dec;15(6):482-7.
17. Volpi E, Kobayashi H, Sheffield-Moorc M,
Mittendorfcr B, Wolfe RR. Essential amino
acids are primarily responsible for the
amino acid stimulation of muscle protein
anabolism in healthy elderly adults. Am J
Clin Nutr. 2003 Aug;78(2):250-8.
18. DohertyTJ. Invited review: Aging and %&x-
copcnia. J App! Physiol. 2003
Oct;95(4):17l7-27.
19. Vanitallic TB. Frailty in the elderly: contri-
butions of sarcopenia and visceral protein
depletion. Metabolism. 2003 Oct;52(lO
Suppl 2):22-6.
20. Kamel HK, Maas D, Duthie EH, Jr. Role of
hormones in the pathogenesis and manage-
ment of sarcopenia. Drugs Aging.
2002;19(ll):865-77.
21. Lawler JM, Barnes WS, Wu G, Song W,
Demaree S. Direct antioxidant properties of
creatine. Biochem Biophys Res Commun.
2002 Jan ll;290(l)i47-52.
22. Ji LL. Exercise-induced modulation of
antioxidant defense. Ann NY Acad Sci. 2002
Apr;959:82-92.
23. Carmeli E, Colcman R, Reznick AZ. The
biochemistry of aging muscle. Exp Gerontol
2002 Apr;37(4):477-89.
24. Welle S. Cellular and molecular basis of
age-related sarcopenia. Can JAppl Physio!.
2OO2Feh;27(l):19-41.
25. Lio D, Scola L, Crivello A, et al. Allclc fre-
quencies of -f874T: A single nucleotide
polymorphism at the first intron of interfer-
on-gamma gene in a group of Italian cente-
narians. Exp Geronlol 2002
Jan;37(2-3):315-9.
26. Bonafe M, Olivieri F, Cavallone L, et al. A
gender-dependent genetic predisposition to
produce high levels of IL-6 is detrimental
for longevity. Eur J Immunol 2001
Aug;31(8):2357-61.
27. Bruunsgaard H. Pedersen M, Pedersen BK.
Aging and proinflammatory cytokines. Curr
Opin Hematoi 2001 May;8(3):131-6.
28. Marcell TJ, Harman SM, Urban RJ. et al.
Comparison of GH, IGF-I, and testosterone
with mRNA of receptors and myostatin in
skeletal muscle in older men. Am J Physiol
Endocrinol Metab. 2001 Dec;281(6):En59-
E64.
29. Persky AM, Brazeau GA. Clinical pharma-
cology of the dietary supplement creatine
vn.ono]\y<iia.ie,. Pharmacol Rev. 2(H)1
Jun;53(2): 161-76.
30. Parise G, Mihic S, MacLennan D, Yarashes-
ki KE, Tarnopolsky MA. Effects of acute
creatine monohydrate supplementation on
leucine kinetics and mixed-muscle protein
s^nihc?As. J Appl Physiol. 2001
Sep;91(3):104I-7.
31. Brod SA. Unregulated inflammation short-
ens human functional longevity. Inflamm
Res. 2000Nov;49(ll):56l-70.
32. Rogers MA, Evans WJ. Changes in skeletal
muscle with aging: effects of exercise train-
ing. Exerc Sport Sci Rev. 1993;21:65-102.
33. Hutter E, Renner K. Pfister G, et al. Senes-
cence-associated changes in respiration and
oxidative phosphorylation in primary human
fibroblasts. Biochem J. 2004 Jun 15;380(Pt
3):919-28.
48 LIfE EXTENSION April 2005
34. Brose A. Parise G. Tarnopolsky MA. Crea-
tine supplementation enhances isometric
strength and body composition improve-
ments following strength exercise training in
older adults. J Geronlol A Biol Sci Med Sci.
2003Jan;58(l):Il-9.
55. Gotshalk LA. Volek JS, Staron RS, cl al.
Creatine supplementation improves muscti-
lar performance in older men. Med Sci
Sports Exerc. 2(102 Mar:34(3):537-43,
3(1. Candow DG. Chilibeck PD. Chad KE, et al.
Effect of ceasing creatine supplementation
while maintaining resistance training in
older men. J Aging Phys Act. 2004
Jul:l2(3):219-3I.
37. Emerit J, Edeas M. Bricairc F. Nourodegen-
erative diseases and oxidative stress. Hiomcd
Phamuicoiher. 2(K)4 Jan:58( I ):?9-4f>.
38. Kang D, Hamasaki N. Mitochondrial oxida-
tive stress and mitochondrial DNA. Clin
Chem Eab Med. 2003 Oct;4I(10):l2Sl-H.
39. Szibor M and Holtz J, Mitochondria! age-
ing. Basic Res Cardiol 2003 Jul;98(4):210-8.
40. Wc-i YH. Lcc HC. Oxidative stress, mito-
chondrial DNA mutation, and impairment
of antioxidant enzymes in aging. Exp Biol
Med (Mtiywood.). 2002 Ocl;227(y):f)71-82.
41. Waters DL. Brooks WM. Quails CR. Baiim-
gartncr RN. Skeletal muscle mitochondria!
function and lean body mass in healthy exer-
cising elderly. Mech Ageing Dev. 2003
Mar:124(3):301-9.
42. Santos RV Bassit RA, Caperuto EC. Costa
Rosa LE The effect of creating supplemen-
tation upon intlammalory and muscle sore-
ness markers after a 30km race. Life .Sci.
2Q04Sep3;75(16):I917-24.
43. Klivenyi P. Calingasan NY. Starkov A, et a!.
Neuroprotective mechanisms of creatine
occur in the absence of mitochondrial crea-
tine kinase. Neurobiol Dis. 2()(!4
Apr:15(3):6I0-7.
44. Zhu S, Li M, Eigueroa BE, el al. Prophylac-
tic creatine administration mediates neuro-
protection in cerebral ischemia in mice. 7
Neurosci. 2004 Jun 30:24(26):5'J0y-l2.
45. Dedeoglu A, Kubitus JK. Yang L, et al. Cre-
atine therapy provides neuroprotection after
onset of clinical symptoms in Huntington's
disease transgcnic imcc.J Neitrochem. 2003
Jun;85(6):L'559-67.
Ah. Rabchevsky AG, Sullivan PG. Ftigaccia L
Schcff SW. Creatine diet supplement for
spinal cord injury: influences on functional
recovery and tissue sparing in rats. J Neuro-
iraiima. 2003 Jul:20(7):65y-69.
47. Adcotk KH. Ncdclcu J. Locnncker X ct al.
Neuroprotection of creatine supplementa-
tion in neonatal rats with transient cerebral
hypoxia-isehemia. Dev Neurosci.
2002:24(5 ):382-8.
48. Hausmann ON. Fouad K. Wallimann T,
Schwab ME. Protective effects of oral crea*
tine supplementation on spinal cord injury
in rats. Spinal Cord. 2002 Sep;4lH9):449-5().
4y. Sec D, Mason S. Roshan R, Increased
tumor necrosis factor alpha (TNF-alpba)
and naliiral killer cell (NK) function using
an integrative approach in late stage ean-
cers. Imimiiiol Invest. 2002 May;31(2):137-
53.
50. Andreassen OA, Dedeoglti A, Fcrrantc RJ.
et al. Creatine increase survival and delays
motor symptoms in a transgenic animal
model of Huntington's disease. Neurobiol
Dis. 2001 Jun:8(3):479-Ql.
51. Tarnopolsky MA, Bea! ME Potential for
creatine and olhcr ihcrapies targeting cellu-
lar energy dysfunction in neurological disor-
ders./1/m M'Hra/. 2001 May:49(5):561-74.
52. Walter MC. LochmtiUer H. Rcilich P et al.
Creatine monohydrate in muscular dystro-
phies: A double-blind, plaeebo-controlled
clinical study. Neuro!og\: 2000 May
9;54{9): 1848-50.
53. Tarnopolsky M, Martin J. Creatine monohy-
drate increases strength in patients with
neuromuscular disease. Ncumhgy. 1999 Mar
!0:52{4):854-7.
54. Klivenyi P, Ferrante RJ, Matthews RT, et al.
Neuroprotective effects of crealine in a
transgenic animal mode! of amyotrophic lat-
eral sclerosis. Nat Med. 1999 Mar:5(3):347-
50.
55. Matthews RT, Fcrranlc RJ, Klivenyi P, et al.
Creatine and cyclocreatine attenuate MPTP
neurotoxieity. Exp Neurol. 1999
May:!57(l):142-9.
56. Matthews RT, Yang L, Jenkins BG, et a!.
Neuroprotective effects of creatine and
eyc!ocrcaline in animal models of Hunting-
ton's disease. / Neurosci. 1998 Jan
57. Sullivan FG, Geiger JD. Maitson MP, Scheff
SW. Dietary supplemeni ereatine protects
against Iraumatic brain injury,/l/iAi Neiirol.
2000 Nov:48(5):723-9.
58. Rac C Digney AL. McEwan SR, Bates TC.
Oral creatine monohydrate supplementation
improves brain performance: a double-
blind, placebo-controlled, cross-over trial.
Proc R Soc Lotid B Biol Sci. 2003 Oct
22:270(!529):2I47-50.
59. Marshall K. Therapeutic applications of
whey protein. Allern Med Rev. 2004
Jun;9(2):136-56.
60. Bounous G. Whey protein concentrate
(WPC) and glutathione modulation in can-
cer treatment. Aniicancer Res. 2000
Nov:20(6C):4785-92.
61. Bounous O, Gold P The biological activity
of undenaiured dietary whey proteins: role
of glutathione. Clin Ime.s! Med. 199f
Atig:14(4):296-309.
62. Tsai WY, Chang WH, Chen CH, Lu EJ.
Enchancing effuct of patented whey protein
isolate (Immunocal) on cytotoxicity of an
anticancer drug. Nutr Cancer.
2000:38(2):200-8.
63. Baruchc! S, Viaii G. !n vitro selective modu-
lation of eellular glutathione by a human-
ized native miik protein isolate in normal
cells and rat mammary carcinoma model.
Anticancer Res. 1996 May;16(3A):1095-99.
64. Mclnlosh GH, Regester GO, Le Leu RK,
Roylc PJ, Smithcrs GW. Dairy proteins pro-
tect against dimethylhydrazine-induced
intestinal cancers in rats. J Nutr. 1995
Apr;125(4):SI)9-16.
65. Stumvoll M. Perriello G, Meyer C, Gerich J.
Role of giutamine in human carbohydrate
metabolism in kidney and other tissues. Kid-
ney Int. 1999Mar:55(3):778-92.
66. Walsh NP Blannin AK, Robson PJ, Gleeson
M, Giutamine, exercise and immune func-
tion. Links and possible mechanisms. Sports
Med. 1998Sep:2fi(3):177-91.
67. De Bandt JP, Cynober LA. Amino acids
with anabolic properties. Curr Opin Clin
Nutr Metab Care. 1998 May;l(3):263-72.
68. Balzola FA, Boggio-Bertinet D. The
metabolic role of giutamine. Minen-ii
Gasiroetiierol Dielol. 1996 Mar;42(l):17-26.
69. Roth E, Spitt!er A, Oeh!er R. Giutamine:
effects on the immune system, protein bal-
ance and intestinal functions. Wien Klin
Wochenschr. 1996:!08(21):669-76.
70. Furst P. Albers S, Stehle P Evidence for a
nutritional need for giutamine in eatabolic
patients. Kidney hit Suppl. 1989
Nov;27:S287-92.
71. Available at: http://www.the-Lips.org/
press/confercncc/cb03/12.htm, Accessed
December 17, 2004.
April 2005 LIFE EXTENSION 49



![The Use of Creatine Monohydrate · 2021. 2. 25. · 4 Creatine Monohydrate Creapure [Fig. 1] Fig.1.Body-own Creatine synthesis and Creatine metabolism gradient by a sodium dependent](https://static.cupdf.com/doc/110x72/6108e3bc190f19375e7bfe13/the-use-of-creatine-monohydrate-2021-2-25-4-creatine-monohydrate-creapure-fig.jpg)