



Alpha and Auger-emitting radionuclides in Therapeutic
Nuclear MedicineDr Ganesh Kumar
Deptt of Nuclear MedicineAIIMS
Currently the predominant class of radiopharmaceuticals that is used in nuclear medicine therapy
Have improved outcome of many benign and malignant lesions that are usually not amenable to other modalities of management
Beta emitter therapy

The emissions usually have a long range and energies distributed over a range rather than discrete single energy emissions
Beta-emitters: disadvantages

Also, the radiobiological effects at a cellular level lead to relatively lower cell-kill

A relatively long range and low LET account for more likelihood of unwanted side effects that can be dose-limiting
These properties have also been attributed to incidences of second malignancies in patients treated with beta emitters

Alpha emitters
Auger and conversion electron emitters
Positron emitters

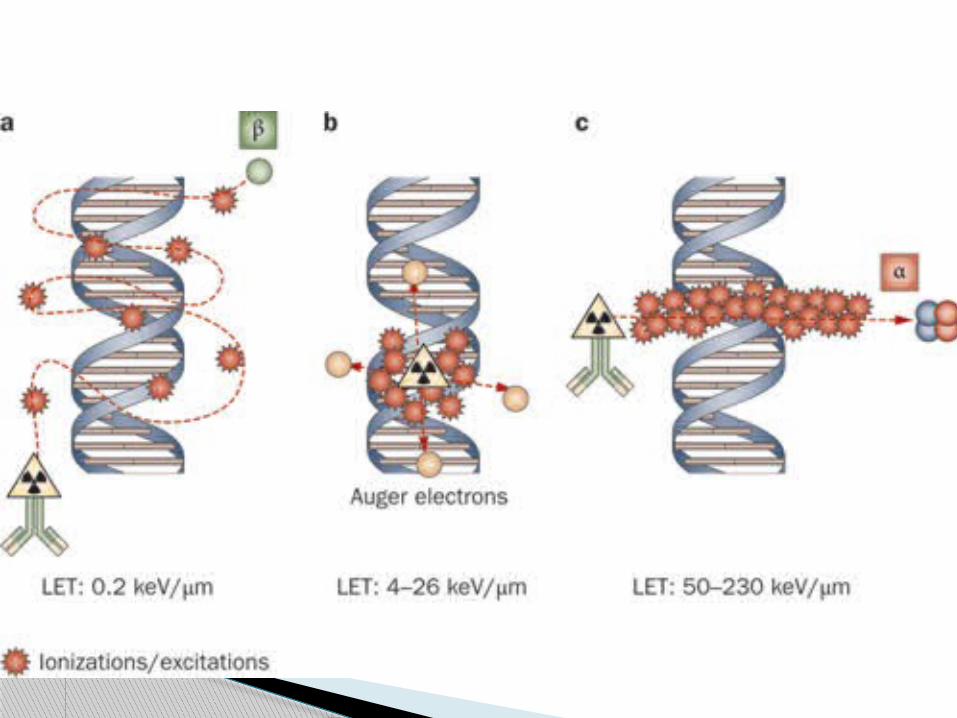
comparatively short range of alpha particles in tissue
high LET
Therefore radiation burden to the surrounding healthy
tissues is low when compared to beta emitters
very effective treatment regimen for microscopic and small volume tumors
Alpha Emitters: properties



Alpha-emitters: radiobiology

Penetrating powers

Sources of alpha-emitters

Common therapeutic alpha-emitters

Discovered by Marie and Pierre Curie in 1898
Elemental form was isolated in 1910 by electrolysis
heaviest of the earth alkaline elements, and all isotopes are radioactive
Radium-226 has the longest half-life (t1/2 = 1600 years), is the most abundant radium isotope in nature
Radium (L. Radius, ray)

Otherwise known as Xofigo (Raclopride)
natural bone-seeker that decays with aphysical half-life of 11.4 days by releasing alpha-particles
Ra-223 dichloride

Source material: Ac-227; from irradiated samples of Ra-226
Separated by means of cation and anion exchange methods
Ra-223 eluted from the resin with high purity
Dissolved in physiologically compatible NaCl/Na-citrate buffer followed by sterile filtration
Ra-223: production



radium cations are incorporated within the bone matrix of metabolically active bone
probably by inclusion in the calcium phosphate and hydroxyapatite crystals
Biodistribution corresponds to Sr-89 chloride in pre-clinical and clinical models
Ra-223: Mechanism of Action

indicated for the treatment of patients with castration-resistant prostate cancer (CRPC), symptomatic bone metastases and no known visceral metastatic disease
50 kBq/kg body wt q4wk; a course of upto 6 injections
ANC ≥ 1500/cc; Hb ≥ 10 g%; plt ≥ 1lac/cc prior to first administration
ANC ≥ 1000/cc and plt ≥ 50000/cc prior to subsequent dosages
Indications and dosage


6 cycles of Ra-223 (50 kBq/kg q4wk) in CRPC patients who did not respond to docetaxel
Interim analysis: 223Ra significantly improved survival versus placebo (14.0 months vs. 11.2 months; P = .00185)
Cross-over analysis (n = 528 deaths) of all randomized patients the median OS benefit was 3.6 months; P = .00007
Outcome (ALSYMPCA Trial)
With alpha-emitters, the endostealbone surface received high radiation doses
considerable fractions of the bone marrow were spared
much more energetic and localized radiation
Hence, produces densely ionizing tracks and predominantly non-reparable double DNA-strand breaks
Advantages over beta-emitters

Transient and mild myelosuppression (no cumulative toxicity over 6 months of Rx)
Neutropenia more common than thrombocytopenia (vs beta-emitters)
Other common side effects include nausea, diarrhoea, vomitign and pedal edema
Side effects

Has many desirable properties for RIT
Half-life of 7.2 hrs: reasonable match with the pharmacokinetics of mAbs, particularly in non-IV setting
More rapid exposure of the tumor cells to the labelled mAbs can be achieved
Astatine-211
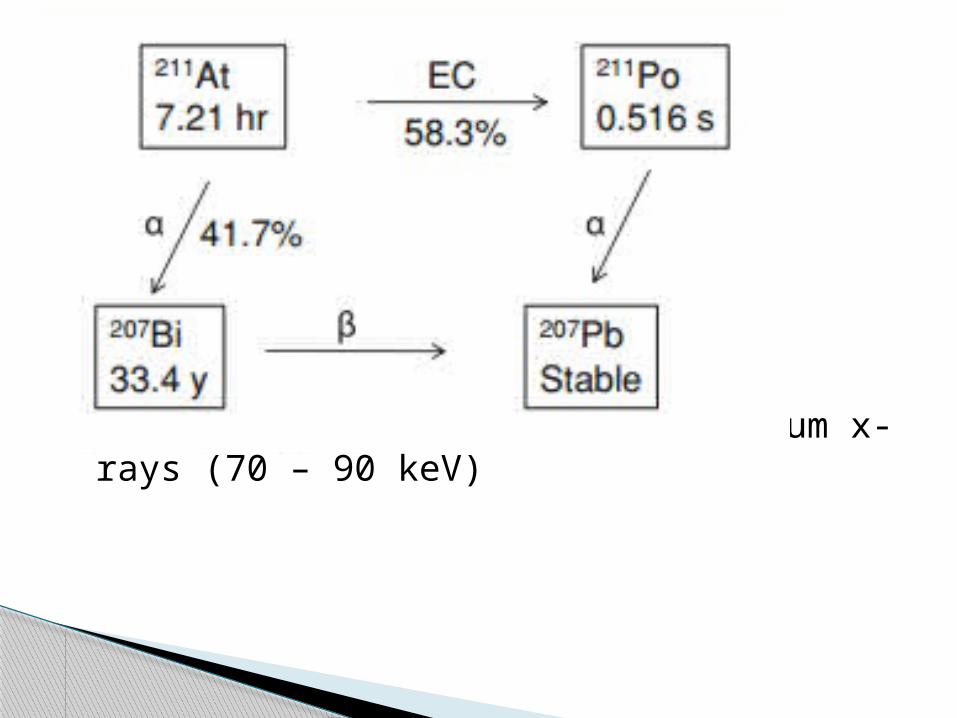
Imaging can be done using polonium x-rays (70 – 90 keV)

Limited clinical data have been published to validate the role of At-211 immunoconjugates
Have shown promising results with a significant increase in survival of the study samples
At-211: clinical applications

Treatment of recurrent brain tumor patients with 211At-labeled chimeric antitenascin monoclonal antibody 81C6 (Zalutsky et al, J Nucl Med. 2008 Jan;49(1):30-8)
GM + anaplastic ODG (n = 18) 71 – 347 MBq in post-surgical cavity Biodistribution with g-camera monitoring: 96.7 ±
3.6% decays within cavity; < 0.05% leakage into blood
Median OS: 54 wks vs 31 wks with no limiting dose toxicity


Bi-213

213Bi-CHX-DTPA conjugated with anti-PSMA mAb J591 has been experimentally shown effective in killing prostate cancer cell lines
Can potentially be employed as an effective therapeutic agent in CRPC and prostatic cancer with micro-metastatic disease
Potential clinical applications
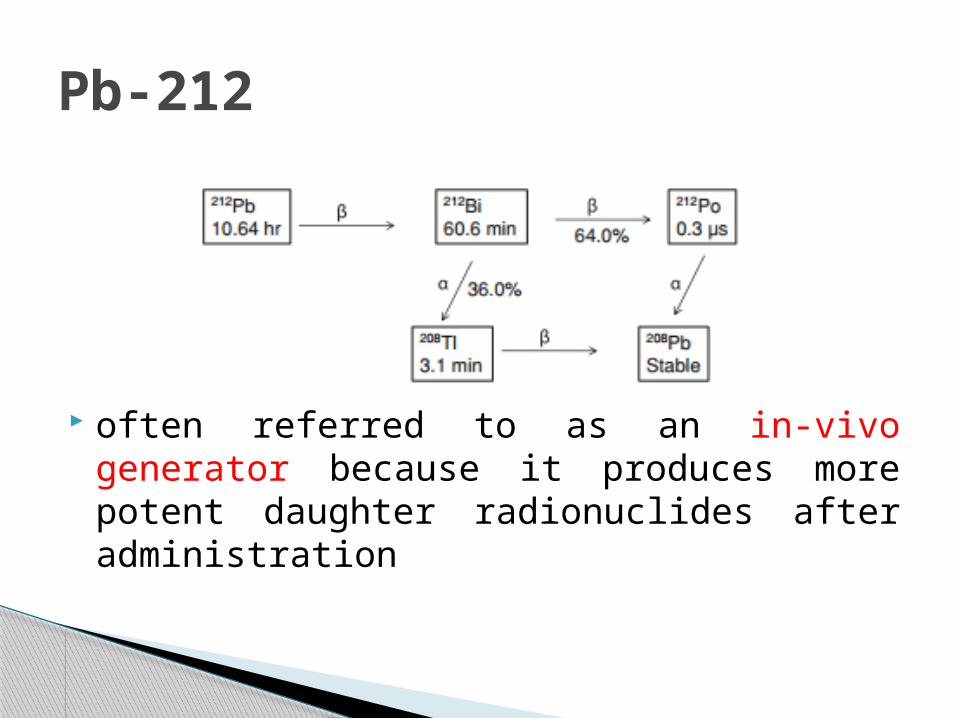
often referred to as an in-vivo generator because it produces more potent daughter radionuclides after administration
Pb-212

Has been tried in pre-clinical studies as early as 1989 where intraperitoneal inoculation in mice bearing virulent Ovarian carcinoma cell line strain
Prolonged survival and eradicated tumor cells in 24% of the inoculated mice sample
Yet to find a mainstream clinical application in oncology management

Represent an attractive alternative to beta-emitters for cancer therapy
Auger electrons are emitted by isotopes that decay by electron capture (EC) or have internal conversion (IC) in their decay
In each decay of these isotopes, a cascade of very low energy electrons is emitted
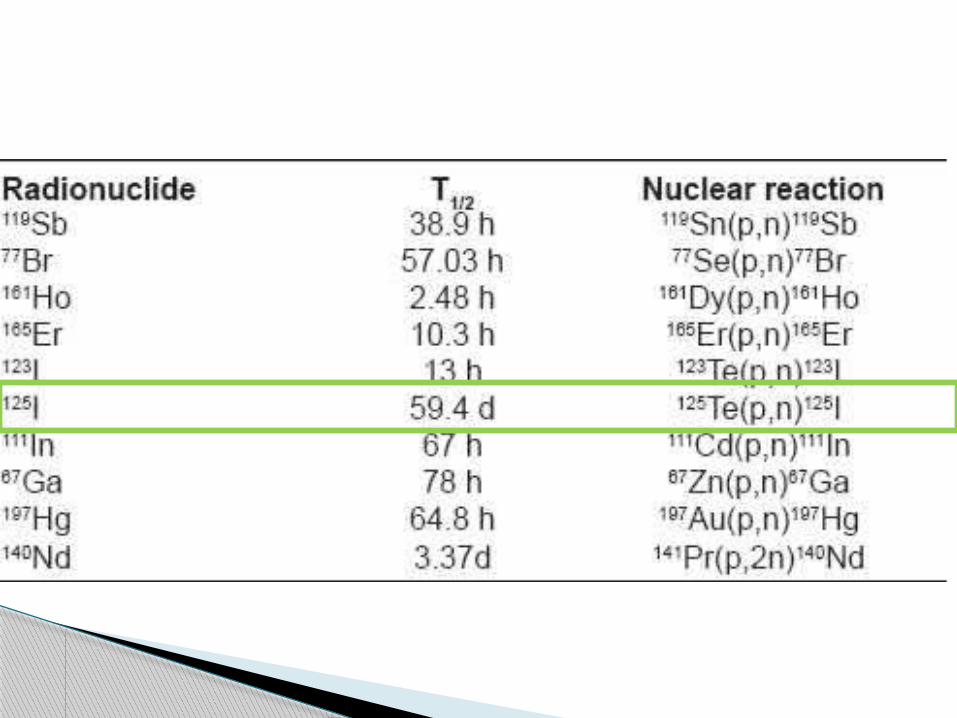
Auger emitters

Multiplicity
Low energ
ies
Short range
in tissue
svery high energy density created in the immediate vicinity of the decay site
• “High LET-like” effect
highly localized absorbed radiation dose to the target region



Feasible option if they can be placed intracellularly, especially in close proximity to (or within) nuclear DNA
This has been experimentally achieved pre-clinical and phase I clinical studies by using 125IUDR (5-radioiodo 2’ deoxyuridine)

Cell-cycle specific radiosensitizer
Incorporated into the cellular DNA only in cells that are actively dividing in S-Phase
This can lead to toxicities when the radiolabelled compound is administered by systemic route
Circumvented by: loco-regional administration into the tumor volume/cavity
Co-administration with MTX (increase in % of cells in S-phase)
Problem with IUDR

Possible target tumor groups:
Brain Urinary bladder Ovarian Intra-capsular Liver Intra-arterial Gastric and colorectal Endoscopic Breast Sonography
Intra-cavitary

Production is expensive and the technology of source material enrichment is limited to a very limited number of nuclear reactors in the world
Availability is limited
Pre-clinical and clinical data are still evolving to validate their role for a more widespread clinical application
Why so less

THANK YOU
















![URANIUM - National Film Board of Canada1].pdf · alpha emitters are the least harmful while gamma emitters are more dangerous than beta emitters. Inside the body, however, alpha emitters](https://static.cupdf.com/doc/110x72/604a60e06cb0dd2c8f04d503/uranium-national-film-board-of-1pdf-alpha-emitters-are-the-least-harmful-while.jpg)













