Dr. Irfan Ahmad KhanAssistant Professor
Adrenergic agonists
Sympathomimetic drugs

• Drugs affect receptors that are stimulated by norepinephrine orepinephrine
• Act on adrenergic receptors,located either presynaptically on neuron or postsynaptically on effector organ
Adrenergic agonists

NEUROTRANSMITTERS
• 3 types→ Collectively called catecholamines
1. Noradrenaline(NA)→ postganglionic sympathetic sites (except sweat glands, hair follicles & some vasodilator fibres) & in certain areas of brain
2. Adrenaline(Adr)→ secreted by adrenal medulla
3. Dopamine(DA)→ transmitter in mammalian extrapyramidal system & of several mesocortical& mesolimbic neuronal pathways

NEP & EP modulate:
• Rate and force of contraction of heart
• Resistance (constriction and dilation) of blood vessels and bronchioles
• Release of insulin
• Breakdown of fat (lipolysis)
• Therefore, frontline therapies for hypertension, depression, shock, asthma, angina

Synthesis, Storage & Release of neurotransmitter in
Adrenergic System

SYNTHESIS OF TRANSMITTER
• Catecholamines are synthesized from amino acid→ Phenylalanine
• In liver, it is 4-hydroxylated to form tyrosine
• Tyrosine is 3-hydroxylated by Tyrosine hydroxylase (TH) to form DOPA
• Tyrosine hydroxylase → rate limiting enzyme & its inhibition by α-methyl-p-tyrosine leads depletion of CAs
• Enzymes are synthesized in nerve cell bodies

occurs in adrenergic neuronal
cytoplasm
occurs inside granules
occurs in adrenal medulla

STORAGE

• Stored in synaptic vesicles or granules
• NA stored in a complex with ATP(4:1)
• In adrenal medulla, Adr so formed is stored in separate granule→ Chromaffin granule
• MAO present on outer surface of mitochondria lowers cytoplasmic pool of CAs

RELEASE

Ligandgated
Releasable nucleotidases
peptidases
GPCRs
Vesicle ass. membrane
proteinSynaptosome
ass.protein

Uptake Vesicular reuptake
VMAT-2 (Vesicular monoamine transporter-2)-70%
• ATP dependent proton translocase
• In exchange of 2H+ →1 amine molecule
• Inhibitor-reserpine
Neuronal uptake
NET(NE transporter)→Uptake-1→87%
• Na+ coupled
• DA>NE>Epi
• Inhibitor-cocaine/desipramine

Non-neuronal(Uptake-2)
1.OCT-1(organic cation transporters)
• DA>Epi>NE
2.OCT-2
• DA>NE>Epi
3.ENT-extraneuronal transporter(OCT-3)
• Epi>NE>DA
→Not Na+ dependent
→Inhibitor - corticosterone

MetabolismTwo enzymes involved→
1. Monoamine oxidase (MAO)
outer surface of mitochondria
2. Catechol-O-methyltransferase (COMT)
present largely in cytoplasm except adrenal
medulla where present in membrane bound
• Also metabolized by sulfotransferases

ALDEHYDE DEHYROGENASE
ALDEHYDE REDUCTASE
ALCOHOL DEHYROGENASE
ALDEHYDE DEHYROGENASE
3,4-DIHYDROXYPHENYL GLYCOL 3,4-DIHYDROXYMANDELIC ACID
VANILLYL MANDELIC ACID
3-METHYL,4-HYDROXYPHENYLGLYCOL
DEAMINATION DEAMINATION

CLASSIFICATION OF ADRENOCEPTORS
HISTORICAL BACKGROUND
• In 1896, Oliver & Schafer demonstrated inj. of extracts of adrenal gland caused rise in arterial pressure
• Dale in 1913 that adrenaline causes two distinct kinds of effect
– Vasoconstriction
– Vasodilatation

• 1948 Ahlquist, showed clearly existence of several subclasses of adrenoceptor
• Postulated existence of 2 kinds of receptor, α & β, defined in terms of agonist potencies as follows:
– α: noradrenaline > adrenaline > Isoprenaline
– β: Isoprenaline > adrenaline > noradrenaline


• There are two main α-adrenoceptor subtypes (α1
and α2) & three β-adrenoceptor subtypes (β1, β2, β3)
• All are G-protein-coupled receptors
• 2nd messengers:
– α1- adrenoceptors activate phospholipase C, thus producing inositol trisphosphate & diacylglycerol
– α2- adrenoceptors inhibit adenylate cyclase & thus decrease cAMP formation
– All β-adrenoceptor stimulate adenylate cyclase


α- adrenoceptors

β-adrenoceptors






Receptor Regulation
• Responses mediated by adr. are not fixed & static
• One of studied examples of receptor regulation is desensitization of adr. that may occur after exposure to catecholamines & other sympathomimetic drugs for long period

Main effects of receptor activation

Tissues and effectsα1 α2 β1 β2 β3
Smooth Muscle
Blood vessels Constrict Constrict/dilate
Dilate
Bronchi Constrict Dilate
GI tract Relax Relax (presynaptic effect)
Relax
GI sphincters Contract
Uterus Contract Relax
Bladder detrusor Relax

α1 α2 β1 β2 β3
Bladder sphincter
Contract
Seminal tract Contract Relax
Iris (radial muscle)
Contract
Ciliary muscle
Relax
Heart:
Rate Increase
Force of contraction
Increase

α1 α2 β1 β2 β3
Skeletal muscle
TremorIncreased muscle mass and speed of contractionGlycogenolysis
Thermogenesis
Liver Glycogenolysis
Glycogenolysis
Fat LipolysisThermogenesis
Pancreatic islets
Decrease insulin secretion

α1 α2 β1 β2 β3
Nerve Terminal:
Adrenergic Decrease release
Increase release
Cholinergic Decrease release
Salivary gland
K+ release Amylase secretion
Platelets Aggregation
Mast cells Inhibition of histamine release
Brainstem Inhibits sympathetic outflow

α1 α2 β1 β2 β3
Second messengers and effectors
PLC activation ↓cAMP ↑cAMP ↑cAMP ↑cAMP
↑ IP3 ↓Calcium channels
↑DAG ↑Potassium channels
↑Ca2+
Agonist potency order
NA ≥A > ISO A > NA >ISO ISO > NA > A ISO > A > NA ISO > NA = A
Selective agonists
Phenylephrinemethoxamine
Clonidine Dobutamine Salbutamol, terbutaline, salmeterol, formoterol
BRL 37344
Selective antagonists
Prazosin, doxazocin
Yohimbine Atenolol, metoprolol
Butoxamine



ADRENERGIC DRUGS(Sympathomimetics)
• Direct sympathomimetics→ act directly as agonists on α and/or β adrenoceptors—Adr, NA, Isoprenaline (Iso), Phenylephrine, Methoxamine, Xylometazoline, Salbutamol and others
• Indirect sympathomimetics→ act on adrenergic neuron to release NA, which then acts on adrenoceptors—Tyramine, Amphetamine
• Mixed action sympathomimetics→ act directly as well as indirectly—Ephedrine, Dopamine, Mephentermine


Therapeutic Classification of Adrenergic Drugs• Pressure agents Noradrenaline
➢Ephedrine Dopamine Phenylephrine Methoxamine
• Cardiac stimulants
➢Adrenaline Dobutamine Isoprenaline
• Bronchodilators
➢ Isoprenaline Salbutamol Salmeterol Formoterol
• Nasal Decongestants
➢Phenylephrine Xylometazoline Oxymetazoline Naphazoline
• CNS Stimulants
➢Amphetamine Methamphetamine Dexamphetamine
• Anorectics
➢ Fenfluramine Sibutramine Dexfenfluramine
• Uterine relaxant & vasodilators
➢Ritodrine Isoxsuprine Salbutamol Terbutaline

Adrenergic Agonists
I.Direct-Acting
A. Epinephrine (α1, α2, β1, β2)At low doses, β effects (vasodilation) on vascular system predominate, whereas at high doses, α effects (vasoconstriction) are strongest
Cardiovascular• β1 action: positive inotropic & chronotropic
• α effects : constricts arterioles in skin, mucous membranes and viscera. Renal blood flow isdecreased.
• β2 effects: dilates vessels going to liver and skeletal muscle
• Therefore, increase in SBP, with a slight decrease in DBP

A. Epinephrine (α1, α2, β1, β2)
Respiratory
• β2 action: powerful bronchodilation
• Inhibits release of allergy mediators such as histamines from mast cells
• Physiological antagonist of histamine
• In anaphylactic shock, this can be lifesaving→ not only raises BP, but counteracts bronchospasm/laryngeal edema

A. Epinephrine (α1, α2, β1, β2)Therapeutic uses
• Anaphylactic shock: Epinephrine is DOC
• Glaucoma: Dipivefrine → open-angle glaucoma→reducing production of aqueous humor by vasoconstriction of ciliary body blood vessels
• Cardiac arrest: Epinephrine restore cardiac rhythm
• Anesthetics: Local anesthetic solutions usually contain 1:100,000 parts epinephrine→increase duration of localanesthesia
• Control oozing of capillary blood: epinephrine (1:100,000) used topically to vasoconstrict mucous membranes


• Transient restlessness, headache, palpitation,
anxiety, tremor and pallor may occur after s.c./ i.m.
injection
• Marked rise in BP leading to cerebral haemorrhage,
ventricular tachycardia/fibrillation, angina, MI →
large doses or inadvertant i.v. injection
• C/I: hypertensive, hyperthyroid and angina
• Not to be given during anaesthesia with halothane
(risk of arrhythmias) and in patients receiving β blockers (marked rise in BP → unopposed α action)
Adverse effects and contraindications of Adr.

B. Norepinephrine (α1, α2, β1)
• In therapeutic doses, α receptor is mostaffected
Cardiovascular actions:
• Vasoconstriction: α1 effect
• Both SBP and DBP increase
• Note: NE causes greater vasoconstriction than does epinephrine(no vasodilation via β2 receptors)
• Weak β2 activity of norepinephrine also explains why it is not useful in treatment of asthma

C. Isoprenaline (β1 and β2)
• Direct-acting synthetic catecholamine, stimulates both β1 and β2
• Nonselectivity is one of its drawbacks and reason why it is rarely used therapeutically
• Action on α receptors is insignificant
Therapeutic uses
• Stimulate heart in emergency situations

C. Isoprenaline (β1 and β2)Cardiovascular
• β1 effect: ↑heart rate and force of contraction→ CO. Useful in AV block or cardiac arrest
• β2 effect: dilates arterioles of skeletal muscle→↓ peripheral resistance
• Because of its cardiac stimulatory action, it increase SBP slightly, but it greatly ↓ mean arterial and DBP
• Other effects on β receptors, such as increased blood sugar and lipolysis

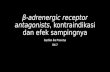
Effects of intravenous infusion
Slow, β2 Rapid, ⍺

Effect on BP:
• NA : rise in systolic, diastolic & mean BP; No vasodilatation, peripheral resistance ↑ due to α action
• Isoprenaline : ↑ systolic but marked fall in diastolic BP, mean pressure generally falls
• Adr
• slow i.v. infusion → rise in systolic but fall in diastolic BP, mean BP generally rise
• Rapid i.v. inj. →marked rise in both systolic & diastolic BP, BP returns to normal within a few minutes & secondary fall in BP follows
• When an α blocker has been given, only fall in BP is seen—vasomotor reversal of Dale

D. Dopamine (D1 and D2, β1,α1)
• High dose→ vasoconstriction → α1
• Moderate dose→ stimulates β1 cardiac receptors
• Low dose→ D1 and D2 occur in mesenteric and renal vascular beds→ dopamine produces vasodilation
• Cardiovascular: β1, α1 receptors
• Renal and visceral: Vasodilator thus increasing blood flow to kidneys and other viscera
• Therefore, useful in shock, in which significant increases in sympathetic activity might compromise renal function

D. Dopamine (D1 and D2, β1,α1)Therapeutic uses
• Shock: DOC and is given by continuous infusion. It raises BP by stimulating:
• β1 receptors → increase cardiac output,
• α1 receptors → increase total peripheral resistance
• Enhances perfusion to kidney and splanchnic areas→ enhances GFR and causes sodium diuresis
• So, dopamine is far superior to NE, which diminishes blood supply to kidney and may cause renalshutdown

E. Dobutamine (β1)• Synthetic, deivative of dopamine without D1/D2
effect
• Increases cardiac rate and output with few vascular effects
Therapeutic uses:
• CHF: to increase CO
• Inotropic support after cardiac surgery
• ↑ CO with little change in HR and it does not significantlyelevate oxygen demands of myocardium a majoradvantage over other sympathomimetic drugs

F. Oxymetazoline (α1 and α2)
• Direct-acting synthetic adrenergic agonist
• Used locally in eye or nose as a vasoconstrictor
• Used
• Nasal decongestant
• Ophthalmic drops for relief of redness of eyesassociated with swimming, colds or contact lens

G. Phenylephrine (α1)
• Direct-acting, synthetic adrenergic drug
• Vasoconstrictor : raises both systolic and diastolic BP
• No effect on heart but rather induces reflex bradycardia when given parenterally
• Used topically as nasal decongestant and in ophthalmic solutions for mydriasis without cycloplegia
• Reduces IOP by constricting ciliary blood vessels

H. Methoxamine (α1)
• direct-acting, synthetic adrenergic drug
• Resembles phenylephrine very closely

I. Clonidine (α2)
• α2 agonist; acts centrally to produce inhibition of sympathetic vasomotor centers, decreasing sympathetic outflow to periphery
• Used in essential hypertension to lower blood pressure

K. Salbutamol and terbutaline (β2)
• short-acting β2 agonists (3-6 hrs)
• used as bronchodilators
L. Salmeterol and formoterol (β2)
• long-acting bronchodilators (12hours)
• Salmeterol has delayed onset ofaction but not formoterol
• Not recommended as monotherapy and are highly efficacious when combined with acorticorsteroid

II. Indirect-Acting Adrenergic Agonists• cause norepinephrine release from presynaptic
terminals or inhibit uptake of norepinephrine
A. Amphetamine
• marked central stimulatory action of amphetamine is often mistaken by drug abusers as its only action
• can increase BP significantly by α-agonist action onvasculature as well as β-stimulatory effects on heart
• Exchange diffusion and reverse transport


• Uses: CNS stimulant
– Narcolepsy
– Appetite control
– Nocturnal enuresis
– Hyperkinetic child
• Drug of abuse

B. Tyramine
• Not clinically useful drug
• Found in fermented foods, such as ripe cheese
• Normally, oxidized by MAO in GIT, but if patient is taking MAO inhibitors, it can precipitate serious vasopressor episodes
• Like amphetamines, tyramine can enter nerve terminal and displace stored NE
• Released catecholamine then acts on adrenoceptors

C. Cocaine
• Ability to block Na+/K+-activated ATPase (required for cellular uptake of norepinephrine)
• Consequently, norepinephrine accumulates in synapticspace
• Like amphetamines, it can increase blood pressure by α-agonist actions and β- stimulatory effects
• Cocaine as a CNS stimulant and drug of abuse

III. Mixed-Action Adrenergic Agonists
1. Induce release of NE from presynaptic terminals
2. Activate adrenergic receptors on postsynaptic membrane
A. Ephedrine
• Plant alkaloids that are now made synthetically
• No effect of MAO→ Orally
• Penetrate into CNS→ Stimulation