7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 1/27
ADCS-CGICOverview
1

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 2/27
ADCS-CGIC Overview
• General Information
– ADCS-CGIC Overview
• ADCS-CGIC
Administration &Testing Procedures
• NeuroCog TrialsProcedures
2

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 3/27
A New Clinical Global Rating Scale forAlzheimer's Clinical Trials
Lon S. Schneider, M.D. University of Southern California
Jason T. Olin, Ph.D. University of Southern California
Christopher M. Clark, M.D. University of Pennsylvania
Rachelle S. Doody, M.D., Ph.D. Baylor College of Medicine
Steven Ferris, Ph.D. New York University
John C. Morris, M.D. Washington University, St. Louis
Barry Reisberg, M.D. New York University
Frederick Schmitt, Ph.D. University of Kentucky

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 4/27
National Institute on Aging-Alzheimer$s DiseaseCooperative Study
#
Leon Thal, M.D., Principal Investigator Instrumentation Committee
Steven Ferris, Ph.D., Chair Global Scales Committee
Lon S. Schneider, M.D., Chair
Christopher M. Clark, M.D.
Rachelle S. Doody, M.D., Ph.D.
Steven Ferris, Ph.D.
John C. Morris, M.D.
Jason T. Olin, Ph.D.
Barry Reisberg, M.D.
Frederick Schmitt, Ph.D.

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 5/27
Introduction #
Clinical Global Impressions of Change
• Historically important outcome in clinical trials
! 14/17 controlled AD trials used global ratings (Lehmann, 1984)
! Traditionally used in depression, anxiety, schizophrenia trials
• Important indicator of clinical significance
! Efficacy observed without systematic measurement
! Change on a CGI is clinically significant -- by definition
• Global Rating in antidementia research
!
Modest efficacy of current medications affects sensitivity
! Lack of structure limits reliability (Dahlke et al., 1992)
! Lack of consensus regarding clinically significant change
! Many sources of bias

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 6/27
Historical Trends
•
1970s--CGIC (Guy 1976)
– Minimal guidelines assume appropriate inferences by clinician
– Based on "total clinical experience" or "how much has he changed?"
• 1986-90--NIA Mt. Sinai tacrine trial uses original CGIC (Davis et al., 1992)
– Improvement found on ADAS-Cog, none on CGIC
• 1991--Tacrine 30-week trial introduces CIBIC (CIBI, Knapp et al., 1994)
– Informant and subject interviewed at BL with 8 items, follow-up of subjectonly
– CIBI detects treatment effect
•
1991--FDA draft guidelines
– CGIC should not include informant information, should remain holistic
• 1992-93--NIA-ADCS, instrument protocol establishes goal to develop newCGIC
– ADCS-CGIC instrument developed

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 7/27
Current Issues: Global Ratings
• Structure vs. no structure
• Control of information sources (subject vs.informant)
• Severity vs. change measures
• Need for consensus

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 8/27
Rationale for use
If a experienced and unbiasedclinician can detect a global change in
an AD patient solely on an interview…then that change is assumed to be
clinically relevant
(FDA, 1991 and others)

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 9/27
Global Change Rating
• CIBIC -- based solely on subject interview,was originally recommended by FDA for
AD trials
• CIBIC+ -- includes a caregiver interview toprovide more complete information onsubject status

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 10/27
ADCS-CGIC Rating
• Marked improvement (1)
• Moderate improvement (2)
• Minimal improvement (3)
• No change (4)
• Minimal worsening (5)
• Moderate worsening (6)
• Marked worsening (7)

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 11/27
Development of ADCS-CGIC
Consensus identified among clinicians
• Survey sent to ADCS global raters
• Clinicians agreed that a CGIC should include:
! Interview of subject and informant
! Mental status examination
! Take approximately 20 minutes per interview
! Assess a common set of areas
Format for ADCS-CGIC based on survey results:
• ADCS-CGIC requires separate interviews of subject and informant
• Worksheets created
! Include domains with specific areas and sample probes
! Content adapted from existing severity rating scales
! Space included for notes
! Not required to fill out forms or to assess every item
Thus, consistency is permitted without forcing a structure on raters

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 12/27
ADCS-CGIC Format • Instructions
– Note-taking as one would clinically
– Assess mental status
– Assessment of side effects prohibited
– 20 minutes recommended per interview
– Ratings made with reference to baseline
• Baseline
– Separate interview of subject and informant
• Follow-up/Subsequent Visit
– Separate interview of subject and informant
– Interview subject or informant first
– Global change rating made after 2nd interview (subsequent visit)

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 13/27
ADCS-CGIC Validation Study
• N=242 AD subjects stratified by Mini Mental State Examination(MMSE) and 64 controls
• Alzheimer's Disease Cooperative Study – Clinical Global
Impression of Change (ADCS-CGIC) administered at BL, 1, 2, 6,and 12 months
• MMSE, Clinical Dementia Rating (CDR), Geriatric DepressionScale (GDS), Functional Assessment Staging of Alzheimer$sDisease (FAST) administered at BL and 12 months
• ADCS-CGIC rating made after interview with subject and
informant
• Order of interviews randomly assigned for each subject
• Global rating is made after each interview; 2nd is the overallrating

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 14/27
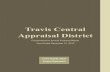
ADCS-CGIC Results • ADCS-CGIC distinguished AD subjects from controls (F(1,114)=55.86,
P<0.0001)
• ADCS-CGIC significantly worsened over time (F(3,240)=68, p<0.0001)
• Time x level of cognitive impairment interaction (F(12,240)=1.93, p<0.03)
! Subjects with an MMSE > 10 showed linear worsening
! Subjects with MMSE < 10 showed the most rapid change at 6 months
0
10
20
30
40
50
60
Percent
1 2 3 4 5 6 7
ADCS-CGIC Rating
Frequency Distribution over Time
1 month2 month
6 month
12 month

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 15/27
ADCS-CGIC#
Outcome Distributions Over Time
ADCS-CGIC Outcome Distribution Over Time
0
10
20
30
4050
60
1 2 3 4 5 6 7
ADCS-CGIC Rating
P e r c e n t
1 month 2 month 6 month 12 month

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 16/27
CGIC ADMINISTRATION &TESTING PROCEDURES
16
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 17/27
General Issues
• Purpose:
– To detect clinically significant globalchange from baseline
• Different versions:
– Differ with respect to the amount of
structure (ADCS-CGIC versus theNYU Version in AD trials)
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 18/27
List of Domains Assessed
• Relevant History
• Observation/Evaluation
• Attention/Concentration
• Orientation
• Memory
• Language/Speech
• Praxis
• Judgment/Problem
solving/Insight
• Thought Content/ Hallucinations
• Behavior/Mood
•
Sleep/Appetite
• Neurological/PsychomotorActivity
• Basic and Complex
(Instrumental) Function
• Social Function
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 19/27
!""#$" &' (')"*+$, -.(/0(1!(
• Subjects may not be the primary (or best)source of information for some items
• Observe behavior of subjects with andwithout informant (dynamics/conflicts)
• The informant is not always correct
– Depression, frustration
– Small changes may be perceived as large
effects or rationalized
• At the beginning of the interview, remind the
interviewee not to mention any side effectsthat the subject may be experiencing
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 20/27
Procedure
• Baseline interviews with subject andinformant
• Follow-up interview with subject and
informant at defined intervals
• Clinical Rating Review and recording of
the CIBIC rating using a 7-point Likert-type
scale
• Monitors must see evidence that it hasbeen performed correctly
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 21/27
Basic Worksheet Structure
Area Probes Caregiver’s orPatient’s Notes
Individual domains within each
of four areas:General, Mental/CognitiveState, Behavior, Functioning
Assessment probes and
history probes are onlysuggestions—Use yourskills!
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 22/27
Administration Overview
Three parts of the ADCS-CGIC administration:
1. Part I – Baseline evaluations
a) Includes information from both subject and caregiver
b) Used as a future reference for subsequent visits
2. Part II – Subsequent Visit evaluations
a) Includes information from both subject and caregiver
b) Used to gather information necessary to assess change from Baseline
3. Part III – Clinician$s Impression of Change
a) Completed at subsequent visits from Part II worksheets/notes
b) Change Rating used to rate clinical impression of change from Baseline
22
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 23/27
Baseline Evaluation
• Interview the subject and informant separately
• Record any relevant information that was usedonto notes section of the CGIC
– Clinical information from any source can beused for this interview
– Assessment of mental/cognitive state must bedone
– If psychometric scales are employed, these
must be recorded on the CGIC work sheets
– All domains must be assessed, however thereis no prescribed order or recommendedtechnique
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 24/27
Follow-up Evaluations
• Domains for evaluation are same as at Baseline
• Record the use of any formal tests
•
Rater may not consult any other member of theteam or use any information from the rest of theclinic visit
• Rater should avoid asking opinions of thesubject or caregiver, and may not ask about sideeffects
• Rater may only refer to the Baseline evaluation
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 25/27
Summary
• Stability over short intervals
• Sensitivity to change over time
• Effective method of generating a CGIC/ CIBIC
• Commonly used in clinical trials
• Rating of change from Baseline , not arating of severity
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 26/27
Key Administration Points
Baseline Evaluation
• Clinical information about the subject from the screening
visit, medical history, physical exam, and neurological
exam may be usedSubsequent Visits
• Subjects should be reminded to avoid mentioning any
potential side effects
• Rater can refer to the information s/he collected at
baseline when determining the assessment of change
26
CONFIDENTIAL

7/17/2019 ADCS TCAD CGIC Training-slides 11Apr2014
http://slidepdf.com/reader/full/adcs-tcad-cgic-training-slides-11apr2014 27/27
Key Administration Points
• Subject should not be present during thecaregiver interview
• Interview for baseline should occur with thepatient first and study partner second
•
In order to ensure consistent data throughout thestudy, the same trial partner/caregiver should beinterviewed at all visits
27
CONFIDENTIAL