9/28/18
1
AcuteKidneyInjury:Drug-InducedUnlessProvenOtherwise
ElizaBorzadek,BSN,PharmD,BCPSAdvancedClinicalPharmacistEasternIdahoRegionalMedicalCenterSeptember28,2018
Disclosures• IdonothaveanydisclosuresorconflictsofinterestinregardstomypresentaKon
• Iwillnotdiscussoff-labelusesofanymedicaKons
LearningObjectives• SummarizedefiniKonandstagingcriteriaforacutekidneyinjury(AKI)
• OutlineeKologyanddiagnosisofacutekidneyinjury• Reviewmanagementofacutekidneyinjury• DiscussprevenKvestrategiesfordrug-inducedkidneyinjury
• SummarizethejobdescripKonforaPharmacist-Ninja

9/28/18
2
80y/ofemaleadmittedwithAMSand®footsurgicalwoundinfection• PMH:s/precentCharcotfootrepair,anemia,HTN,T2DM,peripheralneuropathy,COPD,hypothyroidism,OA,depression
• Drymucousmembranesnotedonphysicalexam• VS:T98.6F,BP141/67,P84,T98.6F,RR20• Height:5’1’’,weight105kg• Labs:glucose113,Na135,K5.2,Cl98,Bicarb27,BUN53,SCr1.5(baseline0.9),eGFR33,CRP26,wbc8,200,Hgb9.5/Hct29,plt219
• Woundculture:MRSA–sensiKvetoVancomycin(MICof1)• Bloodculture–nogrowthx48hrs• IsthispaKentexperiencingAKI?• WhatisthemostlikelyunderlyingcauseforherAKI?
80y/ofemaleadmittedwithAMSand®footsurgicalwoundinfection• Discharged5dayslatertoLTCFonVancomycin1.5gmIVevery24hrs,lasttroughpriorto3rddosewas15.2
• SCr0.9atdischarge
• WhatisyourassessmentofthispaKent’srenalfuncKon?• ShouldthispaKentconKnueonvancomycintherapy?
8/21/18 8/22/18 8/23/18 8/24/18 8/25/18
SCr(mg/dL) 0.9 0.8 0.9 1.0 0.9
TotalIntake(ml) 2,319 2,773 3,610 3,003 1,356
TotalOutput(ml)
3,950 1,900 1,125 850 450
Acutekidneyinjury(AKI)increasestheriskofsubsequentAKI,theriskofprogressiontochronickidneydisease(CKD)andmortality

9/28/18
3
Background• Formerlyknownasacuterenalfailureoracuterenalinsufficiency
• SyndromecharacterizedbyanabruptdeclineofrenalfuncKonmanifestedbyanaccumulaKonofcreaKnine,urea,andotherwasteproductswith/withoutreducedurineoutput
• Globalpublichealthconcernassociatedwithhighmorbidity,mortalityandhealthcarecosts
• AKIaffects~5-10%ofhospitalizedpaKents&upto60%ofpaKentsadmiledtoICU
• AKIisassociatedwithhigherincidenceofCKD• 18-27%ofAKIinhospitalizedpaKentsisdrug-induced
PavkovME,HardingJL,BurrowsNR.TrendsinHospitalizaKonsforAcuteKidneyInjury—UnitedStates,2000–2014.MMWRMorbMortalWeeklyRep2018;67:289–293.
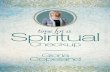
IncidenceofhospitalizationswithAKIamongmenandwomen≥20yearsofagewithandw/odiabetes:UnitedStates-2000-2014
PavkovMEetal.TrendsinHospitalizaKonsforAcuteKidneyInjury–UnitesStates,2000-2014.CentersforDiseaseControlandPrevenKon:MorbidityandMortalityWeeklyReports2018;67(10):289-293.
TrendsinHospitalizationforAKIAmongMenandWomenAged≥20YearswithandwithDiabetes
Characteris2c 2000 2006 2014 Absolutechange(95%CI)
Percentchange(95%
CI)
Allpersonswithdiagnoseddiabetes
WeightedNo. 11,863,011 17,109,522 21,871,994
AllAKINo. 364,527 666,060 1,571,265
HospitalizaKonRate(95%CI)
23.1(21.5–24.8)
28.5(27.0–29.9)
55.3(54.1-56.6)
32.2(30.1-34.3)
139.2(121.1-157.3)
Allpersonswithoutdiagnoseddiabetes
WeightedNo. 189,675,970 202,950,590 217,677095
AllAKINo. 589,399 1,156,994 2,388,295
HospitalizaKonRate(95%CI)
3.5(2.4-3.7)
6.5(6.3-6.7)
11.7(11.5-11.8)
8.1(7.9-8.3)
230.4(216.1-244.7)
PavkovMEetal.TrendsinHospitalizaKonsforAcuteKidneyInjury–UnitesStates,2000-2014.CentersforDiseaseControlandPrevenKon:MorbidityandMortalityWeeklyReports2018;67(10):289-293.

9/28/18
4
AKIDeSinition• Accordingto2012KDIGOguidelines,AKIisdefinedbyanyofthefollowing:• IncreaseinSCrby≥0.3mg/dLwithin48hrsOR• SCrincreaseto≥1.5Kmesbaselinewhichisknownorpresumedtohaveoccurredwithintheprevious7daysOR
• Urinevolume<0.5ml/kg/hrfor6hours
StagingofAKIRIFLECRITERIA COMMON
CRITERIAAKINCRITERIA
Classifica2on SCrorGFRCriteria UrineOutput Stage SCrorGFRCriteria
R RiskofrenaldysfuncKon
SCr↑1.5XbaselineORGFR↓>25%
<0.5ml/kg/hrfor6-12hrs
1 SCr↑≥0.3mg/dLOR1.5-1.9Xbaselinein48hrs
I Injurytokidney
SCr↑2XbaselineORGFR↓by>50%
<0.5ml/kg/hrfor≥12hrs
2 SCr↑to2-2.9Xbaseline
F FailureofkidneyfuncKon
SCr↑to3XbaselineORGFR↓by>75%ORSCr≥4mg/dLwithacute↑of≥0.5mg/dL
<0.3ml/kg/hrfor≥24hrsORanuriafor≥12hrs
3 SCr↑to≥3Xbaseline;ORSCr≥4mg/dLORiniKaKonofRRT
L LossofkidneyfuncKon
Completelossofkidneyfxnfor>4wks
E End-stagekidneydisease
Completelossoffxnfor>3mo
RiskFactorsforAKI• Advancedage• Sepsis• DiabetesMellitus• VolumedepleKon• VomiKng,diarrhea,poorfluidintake,fever,diureKcuse• Heartfailure,hepaKcfailurewithascites
• Pre-exisKngCKD(GFR<60)• Nephrotoxins• Aminoglycosidesandamphotericin• NSAIDs• ACEIs/ARBs• Cyclosporineandtacrolimus• Iodinatedcontrastmedia• CysplaKn• Amphotericin

9/28/18
5
46y/oMpresentstoEDwithgeneralizedweaknessx2wksandN/V• HPI:Pt.alsoreportschronicblurredvisionandpolyuria,althoughhisUOhasbeenlowrecently
• PMH:T2DM,dyslipidemia,hypertension,occasionalaches&pain(treatedwithibuprofen)
• VS:T101.5F,BP66/42,HR140,RR32,95%onRA• HomemedicaKons:• Lisinopril20mgpodaily• Ibuprofen200-400mgpoprnpain• RosuvastaKn20mgpodaily
• WhatarethispaKent’sriskfactorsforAKI?
ClassiSicationofAKIPrerenal/Func2onal Intrinsic(ATN&AIN) Postrenal
History&clinicalpresentaKon
VolumedepleKonRAS,HF,HypercalcemiaNSAID,ACEI/ARBuseCyclosporine
Long-standingrenalhypoperfusionNephrotoxins(contrast,anKbioKcs)VasculiKsGlomerulonephriKs
KidneystonesBPHCancers
Physicalexam HypotensionDehydraKon,AscitesPetechiaifthromboKc
Rash,fever(withAIN) DistendedbladderLargeprostate
SerumBUN/SCr >20:1 15:1 15:1
Urinesodium <20mEq/L >40mEq/L >40mEq/L
FENa <1% >2% >2%
Urineosmolality High Low Low
Urinesediment Normal Muddy,browngranularortubularepithelialcasts
Variable
UrineWBC NegaKve 2-4+ Variable
UrineRBC NegaKve 2-4+ 1+
Proteinuria NegaKve PosiKve NegaKve
FractionalExcretionofSodiumCalculation
FENa=(UrineNa/SerumNa)/(UrineCr/SerumCr)x100

9/28/18
6
UrineOutputClassiSications• Anuric:<50ml/24hrs• Associatedwithworseoutcomes
• Oliguric:50–500ml/24hrs• Nonoliguric:>500ml/24hrs• AssociatedwithbelerpaKentoutcomes• Easiertomanage–fewerproblemswithvolumeoverload
46y/omalepresentstoEDwithgeneralizedweaknessx2wksandintractableN/V• CBC:wbc17,400,Hgb11.0,Hct33.5,plt298• CMP:glucose566,Na130(corrected),K4.7,SCr5.4,BUN47,Alb1.6,Mag1.7,Phos0.7,lactate5.2,CRP21,procalcitonin28
• UA:SG1.020,protein500mg/dL,glucose250mg/dL,nitrite(+),leukocyteesterase500/ul,rbc>100,wbc–packedfield,2-5granularcasts
• Urine:randomNa91,randomcreaKnine25• Urinaryoutput:iniKal150mlayer8Loffluids;400mlinthefirst24hrs• Fourdayslater:SCr5.6• Urineculture:>100,000CFU/mlofEnterobactercloacae• Bloodculture:Enterobactercloacaein2of2bolles• AccordingtoAKINcriteria,whichstageofAKIisthispaKentexperiencing?• WhatisthispaKent’sAKIclassificaKonbasedonavailablelaboratorydata?
hlps://www.nursesKps.com/Kps-mnemonics/med-surg/causes-of-acute-renal-failure/

9/28/18
7
EtiologyofAKI• AmongthemostcommoncausesofAKIinhospitalizedpaKentsisexposuretonephrotoxins
• Prerenal• Characterizedbyrenalhypoperfusion
• DecreaseineffecKveintravascularvolume(HF,cirrhosiswithascites)• DehydraKon,hemorrhage• MedicaKons(NSAIDs,ACEIs/ARBs)
• Intrinsicrenal• Mostcommoncauseisacutetubularnecrosis(ATN)• Othercauses:acuteintersKKalnephriKs(AIN),acuteglomerulonephriKs,vasculiKs
• Postrenal• Inadequatedrainageofurinedistaltothekidneys• BladderoutletobstrucKonisthemostcommoncause
Diagnosis• EarlydiagnosisiscriKcalforimprovingoutcomes• OnceAKIisrecognized,acriKcalnextstepispromptevaluaKonforthecauseofAKI
• Carefulhistorytaking• Exposuretonephrotoxins
• Physicalexam&vitalsigns• Carefulassessmentofhemodynamicandvolumestatus
• Laboratorytests• Urinalysis:granularcastsonmicroscopyindicateATN• Renalpanel,CBC,uricacid• Urinestudies:osmolality,sodium,creaKnine
• Renalultrasound• UsedtoruleoutobstrucKon
• CTKUB(withoutiodinatedcontrast)• Usedforsuspectedurolithiasis
• Renalbiopsy• DefinitewaytoestablishdiagnosisforAINandATN
MonitoringofRenalFunction• InmostclinicalsezngsrenalfuncKonismonitoredviameasurementofserumcreaKnine• NotasensiKvemarker
• CreaKnineasaproductofmusclemetabolism• ProporKonaltomusclemass
• GlomerularfiltraKonrate(GFR)mustdeclineby~50%to60ml/minbeforeSCrrisesto1.5mg/dL• BytheKmeSCrbecomesabnormal,significantrenaldysfuncKonmayalreadybepresent
• GFRisanopKmalwaytomeasurekidneyfuncKon• CreaKnineclearanceisacumbersometest(24-hoururinecollecKon)thusnotrouKnelyperformed
• EsKmatedGFR(eGFR)–surrogatemarker• CalculatedusingMDRD(ModificaKonofDietinRenalDisease)calculaKon(age,gender,SCr,race),Cockcroy-GaultorCKD-EPI
• MoreaccuratepredictorofGFRthanserumcreaKninealone

9/28/18
8
NovelBiomarkersforAKI• BeingstudiesasmoresensiKvemarkersfordetecKonofAKI• MaybeabletodetectpresentlyundetectablemildtomoderaterenaldysfuncKon
• HavethepotenKaltodescribemechanismsandpredictanatomicalsitesofacutekidneyinjury
• CysC(CystaKnC)hasbeenusedforGFResKmaKon• ThoughttobemoreaccurateathigherGFRsandinthosewithreducedmusclemass
• LimitaKons:notaccurateifnotatsteady-state,impactofvolumeofdistribuKonhasnotbeenstudied
• Tubularinjurybiomarkers:NGAL(neutrophilgelaKnase-associatedlipocalin),KIM-1(kidneyinjurymolecule1),interleukin18(IL-18),liver-typefalyacidbindingprotein(L-FABP)
• Biomarkersthatreflectkidneystress:TIMP-2,IGFBP-7• RecentlyapprovedbyFDAtoIDpaKentsathighriskfordevelopingstage2and3AKIduringthenext12-24hrs
• MarketedasNephroCheckTest
ManagementofAKI
ManagementofEstablishedAKI• Generalmeasures• FluidresuscitaKon(balancedcrystalloids)
• Assessfluidresponsiveness• DisconKnuaKonandfutureavoidanceofnephrotoxicmedicaKons• AdjustmedicaKonsbasedonrenalfuncKon• Avoidanceofcontrastmediaexposure• CorrecKonofelectrolyteimbalance• Renalreplacementtherapy(CRRT,IHD)
• Prerenalazotemia:goalistocorrecthemodynamics• FluidresuscitaKonifvolumedepleted(LRvs.NS)
• Preferenceisforbalancedcrystalloids(LactatedRinger’ssoluKonorPlasma-LyteA)
• Bloodpressuremanagement• Bloodproductsifneeded• HoldorD/CmedicaKonswhichaffectrenalhemodynamics
• ACEIs/ARBs,NSAIDs

9/28/18
9
ManagementofEstablishedAKI• IntrinsicAKI• NospecifictreatmentfoundtobeuniversallyeffecKve• Eliminatethehemodynamicinstability• DisconKnuethecausaKvetoxin• AvoidaddiKonalinsults• Managefluidandelectrolytes• Avoid/treathyperglycemia
• NICE-SUGAR:nodifferenceinratesofRRTbetweengroups,highermortalityinintensiveglycemiccontrolgroup
• NutriKonsupport• AKIisacatabolicstate;ptsmayneedenteral/parenteralnutriKon
• MedicaKonmanagement• LoopdiureKcs–lackofevidencefortheirbenefitinAKIexceptinthesezngofvolumeoverload
• PostrenalAKI• EarlyidenKficaKoniscriKcal• RelievetheobstrucKon• Consulturologyorradiology
MoorePKetal.ManagementofAcuteKidneyInjury:CoreCurriculum2018.AmJKidneyDis.72(1):136-148.
FluidResuscitationforAKI:AnEmptyPromise
• MainstayofprevenKonandtreatmentofAKIhasbeenIVfluidtherapy• RaKonale:augmentsCO,maintainsurinaryflow,dilutesnephrotoxins,thusminimizingischemicandtoxicinsultstothekidneys
• IVfluidsarepotentdrugswithcomplexpharmacologicacKons• Only~20%offluidsremainsinintravascularspaceayer90min
• PosiKvefluidbalanceof5-10%ofbodyweighthasbeenassociatedwithorgandysfuncKonandpoorclinicaloutcomesincriKcallyillandayerrouKnesurgery• FluidoverloadisassociatedwithAKI,prolongedICUstay,worseningorganfuncKonandexcessmortality
• FluidoverloadappearstocauseendothelialdysfuncKon• Benefitsoffluidsareshort-livedandlimitedonlytoearlystagesofselectdiseasestates
WatkinsSCandShawAD.FluidresuscitaKonforacutekidneyinjury:anemptypromise.CurrOpinCritCare2016;22:527-532.

9/28/18
10
FluidResuscitationforAKI• EvidencesuggeststhatavoidanceoffluidoverloadmaybeassociatedwithreducedneedforRRT,lowerincidenceofAKI,increasedsurvivalfromsepKcshock• CertainfluidsimpairrenalfuncKonindependentofthequanKtyadministered• Isotonicsaline(0.9%NaCl)hasbeenlinkedtogreaterriskofAKI,morbidityandmortalitywhencomparedwithotherbalancedelectrolytesoluKons• Harmduetohyperchloremiaandmetabolicacidosis• HighchloridecausesvasocontracKonoftheafferentarterioleleadingtodecreasesrenalcorKcalperfusion
• ComposiKon,quanKtyandKmingoffluidsshouldbepersonalizedtoeachpaKentbasedonhis/herresponsetofluids
WatkinsSCandShawAD.FluidresuscitaKonforacutekidneyinjury:anemptypromise.CurrOpinCritCare2016;22:527-532.
46y/omalepresentstoEDwithgeneralizedweaknessx2wksandN/V
• HowwouldyoumanageacutetubularnecrosisinthispaKent?• WhatisyourplanregardinghishomemedicaKons?
IndicationsforRRT• Life-threatening/refractoryhyperkalemia(K>6.5)• BUN>100mg/dL• Refractoryfluidoverload(pulmonaryedema)• Signsofuremia:pericardiKs,pleuriKs,uremicencephalopathy• Refractorymetabolicacidosis(pH<7.1)

9/28/18
11
PreventiveStrategies• PrevenKonisthekey:team-based,standardizedapproach• AvoidanceofnephrotoxicmedicaKonswheneverpossible• EnsuringadequatehydraKon• PaKenteducaKon• Useofdrugtherapiestodecreaseincidenceofcontrast-inducednephropathy
KDIGORecommendationsforPractice• Low-dosedopamineisnotrecommendedfortheprevenKonortreatmentofAKI(LevelofEvidence1A)
• DiureKcsdonotimprovemorbidity,mortalityorrenaloutcomesandshouldnotbeusedtopreventortreatAKIintheabsenceofvolumeoverload(2C)
• KDIGOsuggestsnotusingaminoglycosidesfortreatmentofinfecKonsunlessnosuitable,lessnephrotoxictherapeuKcalternaKvesareavailable(2A)
• AminoglycosidesaretobeadministeredassingledailydoseratherthanmulKple-dosedailyregimensinpaKentswithnormalrenalfuncKon(2B)
• NACnotrecommendedfortheprevenKonofAKIincriKcally-illpaKentswithhypotension(2D)
• NACnotrecommendedfortheprevenKonofpostsurgicalAKI(1A)
DRUG-INDUCEDACUTEKIDNEYINJURY(DI-AKI)

9/28/18
12
BestReferenceforDrug-InducedDiseases
Background• ExposuretonephrotoxinsrepresentsanearlyubiquitouseventinthecourseofhospitalizaKon
• DI-AKIaccountsfor~7%ofalldrugtoxiciKes• 18-27%ofAKIcasesinhospitalizedpaKentsaredrug-induced• TrueincidencehasnotbeenwellcharacterizedbecauseoflackofconsistencyindefiningthecondiKon
• MostimplicatedmedicaKons:NSAIDs,ACEIs/ARBs,aminoglycosides,amphotericin,iodinatedcontrastmedia
• Kidneysareatriskoftoxicinjury:• Receive25%ofcardiacoutput• ConcentraKonoftoxinsintubules• Highintra-renaldrugmetabolism• AutoregulaKon/specializedbloodflowthroughglomerulus
RiskFactorsforDI-AKI• ConcomitantadministraKonofnephrotoxins• Pre-exisKngCKD• Advancedage• Diabetes• Dose/duraKonoftherapy• Prolongedtreatmentwithnephrotoxins
• Renin-dependentdiseasestates• Cirrhosis• Heartfailure• Over-diuresis• Hypovolemia

9/28/18
13
Pseudonephrotoxicity• MedicaKonsthatinhibittubularsecreKonofcreaKnine• Trimethoprim,cimeKdine
• MedicaKonsthatincreaseBUN• Tetracyclines,corKcosteroids
• MedicaKonsthatinterferewithserumcreaKnineassay• CefoxiKnandothercephalosporins
AgentsImplicatedinDI-AKIHemodynamic-mediated• DiureKcs• ACEIs/ARBs• Cyclosporine• NSAIDs/COX-2inhibitorsGlomerulonephri2s• Allopurinol• Hydralazine• Lithium• NSAIDs• Phenytoin• PTU• Rifampin
Nephrolithiasis• Acyclovir• Allopurinol• Topiramate• Zonisimide• Sulfonamides• Furosemide• Indinavir• Foscarnet
AcuteTubularNecrosis• Aminoglycosides• AmphotericinB• Radiocontrastmedia• CisplaKn• Ifosfamide
AcuteInters22alNephri2s• Allopurinol• AnKbioKcs• H2blockers/PPIs• Phenytoin,valproicacid• DiureKcs• NSAIDs
Tisdaleetal.Drug-inducedDiseases,2ndediKon.

9/28/18
14
ClinicalPresentationGeneralSignsandSymptoms• CVAtenderness• Edema• ElevatedSCr• Rapidweightgain• Fever• Malaise• Hypertension
AcuteTubularNecrosis• Oliguria• MagnesiumwasKngNephrolithiasis• Renalcolic• Hematuria
AcuteInters22alNephri2s• Eosinophilia• Eosinophiluria• Proteinuria• Pyuria• Skinrash• Arthralgias
Glomerulonephri2s• Foamyurine• FacialandLEpizngedema• Oliguria• Proteinuria• Skinrash
Tisdaleetal.Drug-inducedDiseases,2ndediKon.
Aminoglycosides:ATN• Typicallycauseacutetubularnecrosis• Incidenceofnephrotoxicity:1.7-58%ofpaKents• PresentaKon• GradualincreaseinSCrconcentraKonandadecreaseinGFR• Onset:6-10days• NonoliguricAKI• Hypokalemiaandhypomagnesemia
• Riskfactors• LargetotalcumulaKvedose• Prolongedtherapy• TroughconcentraKons>2mg/L• Recent,previousaminoglycosidetherapy• Concurrentuseofnephrotoxins• PaKent-related:CKD,advancedage,gram–bacteremia,liverdisease,hypoalbuminemia,dehydraKon,KandMagdeficiencies,shock,poornutriKon
Aminoglycosides:ATN• PrevenKon• AvoidinhighriskpaKents• MaintainadequatehydraKon• Useonce-dailydosing• Avoiduseofothernephrotoxins• LimitthetotalcumulaKvedose

9/28/18
15
IntravenousContrastMedia• ThirdleadingcauseofAKIamonghospitalizedpaKents• Incidence:2-50%ofpaKentsdependingonriskfactors• Associatedwithhighin-hospitalmortalityrisk(34%)• Iodine-containingcontrastmedia• UsedforCT,angiography,coronaryangiography,arthrography,myelography,GIfluoroscopicstudies
• CauseCI-AKI,specificallyATN• Gadolinium-basedcontrastagents(GBCAs)• UsedforMRIstudies• Causenephrogenicsystemicfibrosis(NSF)
IntravenousContrastMedia:ATN• Osmolalityofcontrastagents• High-osmolarcontrastmedia(HOCM):~1500-2000mOsm/kg• Oldestagents• RelaKvelyinexpensive
• Low-osmolarcontrastmedia(LOCM):500-800mOsm/kg• Non-ionic→donotdissociateinwater→fewerparKclesinsoluKon
• Examples:iohexanol240,iohexanol300(Omnipaque),iopamidol(Isovue-200,-300,-370)
• Iso-osmolarcontrastmedia(IOCM):290mOsm/kg• Non-ionicdimers• Newestclassofagents• Examples:iodixanol320(Visipaque)
Contrast-inducedAKI(CI-AKI)• Asosmolalityofcontrastagentsapproachesthatofserum,thetoxicitydecreases• Halflife:1-2hours,assumingnormalrenalfuncKon• Pathogenesis• ClearanceofcontractagentsisenKrelybyglomerularfiltraKon• Renalischemia• OsmoKcdiuresis–higherriskwithhigh-osmolarcontrastmedia• SystemichypotensiononinjecKonandrenalvasoconstricKon
• DirecttubulartoxicitycausedbyreacKveoxygenspecies• DirectlyinfluencedbyduraKonofexposureoftubules

9/28/18
16
Contrast-inducedAKI• ClinicalpresentaKon• IniKaltransientosmoKcdiuresis,thentubularproteinuria• SCrrisewithin24hrswithapeak2-5daysayerprocedure• 50%ofpaKentsexperienceoliguriaandsomemayneeddialysis
• Riskfactors• CKD• Diabetesmellitus• Age≥75years• Anemia• VolumedepleKon/dehydraKon• Hypotension• Othernephrotoxins• ConcomitantuseofdiureKcs• Repeatedand/orlargevolumeofcontrast(>140ml)• Hyperosmolarcontrastagents• HF,liverfailure
Contrast-inducedAKI(CI-AKI)• UncommoneventinpaKentswithnormalrenalfuncKonandnoaddiKonalriskfactors• NosignificantadvantagewithregardtoAKIhasbeendemonstratedbyusingLOCMoverHOCM
• ForpaKentswithrenalimpairment,severalstudieshavedemonstratedthatLOCMarelessnephrotoxic
• AdverseeffectsofcontrastareintensifiedindehydratedpaKents
• DiabetesincreasesCI-AKIevenwhenSCrisnormal• Amongallpredisposingfactors,paKentswithdiabeteswithpreexisKngCKDareathighestriskforCI-AKI
Contrast-InducedAKI• PrevenKon• CINRiskCalculator• VolumeexpansionwithIVNSat1ml/kg/hfor12hbeforeand12hayercontrastexposureor3ml/kg/hx1hourand1.5ml/kg/hx4-6h• NobenefittousingbicarbonateinhighriskpaKentsundergoingangiographywithrespecttocompositeendpointofdeath,RRTand50%reducKoninGFRat90days
• UsealternaKvenon-contrastimagingstudieswheneverpossible• DisconKnuenephrotoxicagentsatleast24hrspriortoprocedure• AvoidlaxaKvesanddiureKcs• Uselow-osmolaroriso-osmolarcontrastagents• UsethelowestnecessarydoseinpaKentswithrenalimpairment• N-Acetylcysteine(NAC):anKoxidantandvasodilatoryeffects
• Widelyused,conflicKngevidence,generallyconsideredsafe• MayuseoralNACincombinaKonwithIVhydraKon(KDIGO,2D)

9/28/18
17
Gadolinium-basedContrastAgents(GBCAs)• UsedforMRIstudies• Gadoliniumisretainedformonthstoyearsinbrain,bone,skin,kidney,liver,spleen
• LinearGBCAs• Examples:gadobenatedimeglumine,gadopentetatedimeglumine(Magnevist),gadoxetatedisodium
• ResultingreaterretenKonofgadoliniumthanmacrocyclicGBCAs• MacrocyclicGBCAs• Examples:gadobutrol,gadoteratemeglumine,gadoteridol
• Increaseriskofnephrogenicsystemicfibrosis(NSF)
NephrogenicSystemicFibrosis
• Onset:2-18daysayerexposure• PresentaKon:burning,itching,swelling,hardeningofskin,jointsKffness,muscleweakness
• NSFmayresultinfatalordebilitaKngsystemicfibrosisaffecKngskin,muscleandinternalorgans
• RiskofNSFishighestamongCKDstage4and5(GFR<30)andthosewithAKI• UseofMagnevist(gadopentetatedimeglumine),Omniscan(gadodiamide),OpKMARK(gadoversetamide)isconsideredinappropriateforuseinpaKentswithCKDandAKI
Gadolinium-basedContrastAgents
• PrevenKonofNSF• ScreenallpaKentsforAKIorothercondiKonswhichmayreducerenalfuncKon
• ObtainbaselineSCrandcalculateesKmatedGFRpriortocontrast-enhancedimaging
• Donotexceedtherecommendeddose• AllowsufficientperiodofKmeforeliminaKonofdrugfromthebodypriortore-administraKon
• InhemodialysispaKents,considerpromptiniKaKonofhemodialysisfollowingadministraKon

9/28/18
18
Cisplatin&Carboplatin:ATN• Incidence:6-13%• Directtubulartoxins• PresentaKon• SCrpeaks10-12daysayertherapyisiniKated• RenalmagnesiumwasKngiscommon;maybeaccompaniedbyhypokalemiaandhypocalcemia
• Maycauseirreversiblekidneydamage• Riskfactors:mulKplecoursesofcisplaKn,advancedage,dehydraKon,concurrentnephrotoxins,alcoholabuse
• PrevenKon• Avoidconcurrentnephrotoxins• Usesmallestdosepossible,decreasefrequencyofadministraKon• AggressivehydraKon:1-4Lwithin24hrsofhigh-dosestomaintainUOof125ml/h
• AmifosKne910mg/m2maybeadministered30minpriortocisplaKntoavoidnephrotoxicityinhighriskpaKents
AmphotericinB:ATN• DrugofchoiceforiniKaltreatmentofMucormycosis• IncidenceofAKIincreasesascumulaKvedoseincreases• ~80%withcumulaKvedose≥4grams
• CausesdirectproximalanddistaltubulartoxicityandafferentarteriolevasoconstricKon
• PresentaKon• Medianonsetis7days• ManifestsayeradministraKonof2-3grams• ElectrolytewasKng(K,Na,Mg)• SCrincreasesandGFRdecreasesduetovasoconstricKonanddecreaseinkidneybloodflow
• Riskfactors:exisKngCKD,highaveragedailydose,diureKcuse,concomitantnephrotoxins,rapidinfusion,dehydraKon
• PrevenKon:avoidnephrotoxins,limittotalcumulaKvedose,IVhydraKonwith0.9%NaCl,useofliposomalproducts
Hemodynamically-mediatedAKI• Mechanism:decreasedintraglomerularpressuresecondarytovasoconstricKonofafferentarteriolesorvasodilaKonofefferentarterioles
• ACEIs/ARBs• CausedecreaseinglomerularhydrostaKcpressureandadecreaseinGFR
• SCristypicallyexpectedtoriseupto30%• Onset:2-5days,shouldstabilizein2-3weeks• Increases>30%maybedetrimental• UsuallyreversibleupondisconKnuaKonofthedrug• Riskfactors:bilateralRAS,decreasedeffecKvebloodflowtokidneys(HF,liverfailure),preexisKngCKD,dehydraKon
• PrevenKon:startwithlowdoses,Ktrateslowly,switchtolong-acKngagents,monitorSCrdailyoninpaKentandweeklyforoutpaKents,avoidconcomitantdiureKcsandNSAIDs

9/28/18
19
Hemodynamically-mediatedAKI• NSAIDs• Incidence:500,000–2.5millionpeopledevelopNSAID-inducednephrotoxicityinUSannually
• CausevasoconstricKonofafferentarterioleandreducedglomerularbloodflow
• PresentaKon:onsetwithindaysofstarKngtherapy;lowurinevolume,edema,weightgain;increaseinSCr,BUN,andserumK
• Riskfactors:preexisKngCKD,highplasmareninacKvity,concomitantdiureKcs,advancedage
• PrevenKon:avoidNSAIDs• Treatment:DisconKnuedrug,providesupporKvecare,avoidconcomitantmedicaKonsaffecKngRAAS,recoveryistypicallyrapid
Hemodynamically-mediatedAKI
AcuteInterstitialNephritis• AINisresponsibleforupto3%ofallAKIcases• CausedbyallergichypersensiKvityreacKon• Commonculprits:β-lactamanKbioKcsandNSAIDs• PresentaKonforβ-lactamabx:• Onset:1-2weeksayertherapyiniKaKon• Fever,maculopapularrash,eosinophilia,pyuria,hematuria,proteinuria,eosinophiluria
• PresentaKonforNSAIDs:• Delayedonset:ayer6monthsoftherapy• Nosystemicsymptoms
• Kidneybiopsymaybeneededtoconfirmdiagnosis• Treatment:disconKnuetheoffendingagent,considercorKcosteroids

9/28/18
20
PostrenalAKI• ObstrucKonofurineflowayerglomerularfiltraKon• RenaltubularobstrucKon• CausedbyintratubularprecipitaKonofKssuedegradaKonproducts• UricacidprecipitaKonassociatedwithtumorlysissyndrome• Drug-inducedrhabdomyolysis(precipitaKonofmyoglobin)• RapiddeclineinrenalfuncKon• OliguricoranuricAKI
• CausedbyprecipitaKonofdrugs• Sulfonamides,methotrexate,acyclovir,others• Needle-likecrystalsseeninleukocytesonurinalysis
• PrevenKon:pre-treatmenthydraKon,maintenanceofhighurinaryvolume,alkalinizaKonofurine
PostrenalAKI• Extra-renalurinarytractobstrucKon• BHP• Tumors• AnKcholinergicagents
• Nephrolithiasis• MedicaKonswhichcontributetoformaKonofkidneystones:triamterene,indinavir,sulfadiazine,others
Vancomycin-inducedAKI• Nephrotoxicityassociatedwithvancomycinisalong-standing,yethighlydebatedadverseeffect
• KnownasMississippimudin1950sduetobrowncolorofearlyformulaKons(70%pure)• IncreasedincidenceofadversedrugreacKons• In1985purityincreasedto95%
• FrequencyofnephrotoxicityduetovancomycinmonotherapyfollowingpurificaKonwasconsideredinfrequentat5-7%
• Mechanismofinjury• Vancomycinisnotmetabolized;excretedunchangedintheurineviaglomerularfiltraKon
• DecreasedGFRfromanycausewillresultinincreasedvancomycinconcentraKons
• VancomycinhasoxidaKveeffectsoncellsoftheproximalrenaltubuleandcausesrenaltubularischemia
Elyasietal.Vancomycin-inducednephrotoxicity:mechanism,incidence,riskfactorsandspecialpopulaKons:Aliteraturereview.EurJClinPharmacol2012;68:1243-1255.

9/28/18
21
Vancomycin-inducedAKI• Guideline-drivenmoreintensevancomycindosingwithgoaltroughsbetween15-20hasbeenassociatedwithincreasingreportsofvancomycin-inducedAKI
• Ratesreportedas5-43%inarecentmeta-analysisof15studies(1996-2012)–dependentonpopulaKon
• OR=2.67fornephrotoxicityfortroughs≥15vstroughs<15• Highestrateswithtroughs>20
• OR=3.3forpaKentsreceivingconcomitantnephrotoxins• Timeofonset:onaverage4-17daysayeriniKaKon• Upto75%ofcasesresolvedwithin≤7days• Short-termdialysisrequiredin3%ofpts• Nonereportedtorequirelong-termdialysis
VanHal,SJetal.SystemicReviewandMeta-AnalysisofVancomycin-InducedNephrotoxicityAssociatedwithDosingSchedulesthatMaintainTroughsbetween15and20mg/L.AnKmicrobialAgentsandChemotherapy.2013;57(2):734-744.
Vancomycin-inducedAKI
• Nephrotoxicityriskcorrelateswithtroughs>15andduraKonoftreatment>7-14days
• Otherriskfactors:doses≥4gm/day,weight>100kg,criKcallyillinICU,concomitantnephrotoxicdrugs,preexisKngCKD
• Concomitantnephrotoxinscanincreaseincidenceofvancomycin-inducedAKIbyupto35%• Tobramycin,vasopressors,IVcontrastmedia,amphotericinB,loopdiureKcs,somecephalosporinsandPCNs
• Althoughvancomycin-inducednephrotoxicityisusuallyreversible,itisassociatedwithpooreroutcomes• Nephrotoxicityisassociatedwithincreasedoverallmortality,prolongedhospitalandICUlengthsofstay
Vancomycin-inducedAKI• Avoidtotaldailydoses>4grams• AvoidduraKonoftherapy>7days• OrdernasalMRSAswabforpaKentsadmiledwithMDROpneumoniaandD/CMRSA-coverageifnegaKve• 95-98%negaKvepredicKvevalue
• Limitexposuretoconcomitantnephrotoxins• MonitorrenalfuncKonverycarefully• BothurinaryoutputandSCr
• ConsideralternaKveanK-MRSAagentsforpaKentswithriskfactorsfornephrotoxicityrequiringprolongedtreatmentwithvancomycin
• ObtainathoroughallergyhistoryinpaKentsclaimingallergytopenicillininordertoavoidunnecessaryvancomycinprescribing
• TreatpaKentswithMSSAinfecKonswithnafcillinorcefazolinovervancomycin(decreasedmortalityovervanco)

9/28/18
22
Vancomycin+Piperacillin/TazobactamAKI
• PackageinsertforPiperacillin/Tazobactamlistsincidenceofnephrotoxicityat<1%
• RecentretrospecKvecohortstudycomparing99ptsonvancomycinalonewith92ptsoncombotherapyobservednephrotoxicityin8.1%and16.3%ofpts,respecKvely(p=0.041)
• ConsideralternaKvestopiperacillin/tazobactam(e.g..cefepime)foranKpseudomalcoverageinpaKentsalreadyonvancomycin
BurgessLD,etal.ComparisonoftheIncidenceofVancomycin-InducedNephrotoxicityinHospitalizedPaKentswithandwithoutConcomitantPiperacillin-Tazobactam.Pharmacotherapy2014;34(7):670-676.
80y/ofemaleadmittedduetoincreasedconfusion• Admissiondiagnosis:uremicencephalopathysecondarytoAKI• VS:T36.6,BP161/79,P67,RR14• Labs:wbc7,800,Hgb8.5/Hct27,platelets384,glucose170,Na135,K5.9,Cl105,Bicarb22,BUN28,SCr2.0,eGFR24,CRP16
• HomemedicaKons:lisinopril20mgdaily,vancomycin1.5gmIVevery24hrs(heldx3days),aspirin81mgpoBID…
• UA:SG1.011,protein30mg/dL,rbc>182/hpf,wbc71/hpf,glucose(-)
• SCrondischarge:2.3(maxwhilehospitalized2.6)
• WhatisthestageofherAKI?• WhatistheunderlyingcauseofherAKI?
HelpPreventDI-AKI• AvoiduseofmedicaKonsassociatedwithAKIinpaKentswithriskfactors
• Avoidconcurrentuseofagentswhichaffectrenalhemodynamics• Avoidover-diuresis• Consideronce-dailydosingofaminoglycosides• Avoidconcomitantexposuretonephrotoxins• CounselpaKentsaboutrisksofvolumedepleKonandaneedtomaintainadequatefluidintake
• PreferenKaluseofnon-ionic,iso-osmolarcontrastagents• LimitduraKonoftherapywithmedicaKonsassociatedwithAKI• Maintainadequatefluidstatus• Startatlowestdoses(medicaKonswithhemodynamiceffects)• PreferenKaluseoflipid-basedproducts
Tisdaleetal.Drug-inducedDiseases,2ndediKon.

9/28/18
23
NINJAProject• NINJA:NephrotoxicInjuryNegatedbyJust-in-TimeAcKon• ProspecKvequality-improvementprojectuKlizingEHRscreeninganddecisionsupportprocessatCincinnaKChildren’sHospitalMedicalCenter
• PopulaKon:• ChildrenathighriskforDI-AKIadmiledtonon-criKcalcareunits• PediatricpaKentsreceivingaminoglycosidesfor≥3daysor≥3nephrotoxinssimultaneously
• IntervenKon:• PharmacistsrecommendeddailySCrmonitoringinexposedpaKents
• AKIwasdefinedbymodifiedcriteriaof≥25%decreaseinesKmatedcreaKnineclearance
GoldsteinSLetal.ElectronicHealthRecordIdenKficaKonofNephrotoxinExposureandAssociatedAcuteKidneyInjury.Pediatrics2013;132:e756-e767.
NINJAResults
• Inthefirstyear,AKIoccurredin25%ofexposedpaKents• In3years,EHR-driven,pharmacy-lednoKficaKonprocessresultedin38%decreaseintherateof3nephrotoxicmedicaKonexposureand64%decreaseinAKIrates
GoldsteinSLetal.ElectronicHealthRecordIdenKficaKonofNephrotoxinExposureandAssociatedAcuteKidneyInjury.Pediatrics2013;132:e756-e767.
HealthyPeople2020• Oneofthegoalsfor2020focusesondecreasingtheburdenofChronicKidneyDisease(CKD)
• ObjecKve#3forCKDgoalfocusesonAKIfollow-up• PaKentshospitalizedforAKIshouldbeevaluated6monthsayerdischargetomonitorkidneyfuncKonandpreventordelayonsetofCKD• PerKDIGOguidelines,allptswhoexperienceAKIshouldhavetheirkidneyfuncKonre-evaluated3monthsayerAKItoidenKfyneworworseningCKD
www.healthypeople.gov

9/28/18
24
NewNomenclature• TradiKonaltaxonomyofAKIbasedonanatomiclocaKons(pre,intra,andpost-renal)isoverlysimplisKc
• NewspecificAKIsyndromes:• Hepatorenal• Cardiorenal• Nephrotoxic• Sepsis-associated
KellumJA.WhyarepaKentssKllgeznganddyingfromacutekidneyinjury?CurrOpinCritCare
2016;22:513-519.
References• Barton-PaiAandMason,DL.AcuteKidneyInjury.In:Tisdaleetal.Drug-InducedDiseases,2ndEdiKon.2010;853-871.
• Tisdaleetal.Drug-InducedDiseases:PrevenKon,DetecKon,andManagement.2ndEdiKon.
• KIDGOAKIWorkgroup.KDIGOClinicalPracKceGuidelineforAcuteKidneyInjury.KidneyIntSuppl.2012;2(1):1-138.
• MoorePK,HsuRK,andLiuKD.ManagementofAcuteKidneyInjury:CoreCurriculum2018.AmJKidneyDis.72(1):136-148.
• BellomoR,KellumJA,andRoncoC.AcuteKidneyInjury.Lancet2012;380:756-66.
• GoldsteinSL.MedicaKon-inducedacutekidneyinjury.CurrOpinCritCare2016;22:542-545.
• GoldsteinSLetal.ElectronicHealthRecordIdenKficaKonofNephrotoxinExposureandAssociatedAcuteKidneyInjury.Pediatrics2013;132:e756-e767.
• WatkinsSCandShawAD.FluidresuscitaKonforacutekidneyinjury:anemptypromise.CurrOpinCritCare2016;22:527-532.
• RahmanM,ShadF,andSmithMC.AcuteKidneyInjury:AGuidetoDiagnosisandManagement.AmFamPhysician.2012;86(7):631-639.
AcuteKidneyInjury:Drug-InducedUnlessProvenOtherwiseElizaBorzadek,BSN,PharmD,BCPSAdvancedClinicalPharmacistEasternIdahoRegionalMedicalCentereliza@borzadek.com208.339.0604