




100,000 Genomes ProjectRare Disease Programme
Dr Richard Scott
Clinical Lead for Rare Disease, Genomics England

Recruitment to 16th June
210 July 2017
• 31,231 rare disease participants
• Average = 490 participants / week
• Mean family size = 2.3

10/07/2017 3310 July 2017
Rare disease programme
• >200 recruitment categories• Covering >3000 Rare Diseases
• Detailed standardised eligibility
• Prior genetic testing in line with current standard practice
• Core clinical data set:• Disease status• Pedigree data• Human Phenotyping Ontology• Clinical test data where relevant
and not captured by HPO• Using established standards
wherever possible

Patient/ family
Phenotypes & Pedigree
DNA
Genome sequence
Annotated VCFs
Tiered variants
Gene Panel
Variant filtering
Annotation Companies
Review
Gene Panels
Clinical assessment
GeCIP(s)
Validation
Outcomes
Reporting tool
Interpretation pipeline
Report QC

Patient/ family
Phenotypes & Pedigree
DNA
Genome sequence
Annotated VCFs
Tiered variants
Gene Panel
Variant filtering
Annotation Companies
Review
Gene Panels
Clinical assessment
GeCIP(s)
Validation
Outcomes
Reporting tool
Interpretation pipeline
Report QC

Patient/ family
Phenotypes & Pedigree
DNA
Genome sequence
Annotated VCFs
Tiered variants
Gene Panel
Variant filtering
Annotation Companies
Review
Gene Panels
Clinical assessment
GeCIP(s)
Validation
Outcomes
Reporting tool
Interpretation pipeline
Report QC
Gene Panels

Pre-interpretation sign-off
710 July 2017
‘PanelAssigner’

PanelApp
https://panelapp.extge.co.uk/crowdsourcing/PanelApp


Patient/ family
Phenotypes & Pedigree
DNA
Genome sequence
Annotated VCFs
Tiered variants
Gene Panel
Variant filtering
Annotation Companies
Review
Clinical assessment
GeCIP(s)
Validation
Outcomes
Reporting tool
Interpretation pipeline
Report QC
Test request

Tiering
1110 July 2017

121210 July 2017
Interpretation at the hospitals
12
1. ‘Tiering’– Automated focused initial analysis set up prior to interpretation– Aims to mirror standard diagnostic analysis– ‘Tier 1 or 2' – variants in 0-5 genes within prescribed panel(s)– Non-penetrance pipeline can be run
2. Broader analysis– CIP software allows hospitals further, bespoke analysis– ‘Tier 3’ – standard GeL pipeline but not restricted to gene panels; 20-100s variants– Other tools, dependent on which CIP system
3. Lab-clinical team curate variants and record outcomes– Curations are saved in the central knowledge base– Record clinical impacts of diagnostic result
Tier 1 Tier 2 Tier 3
Singletons 0.2 0.8 497.1
Duos 0.3 0.5 184.1
Trios 0.3 0.5 29.0
Larger 0.4 0.8 27.4
1310 July 2017
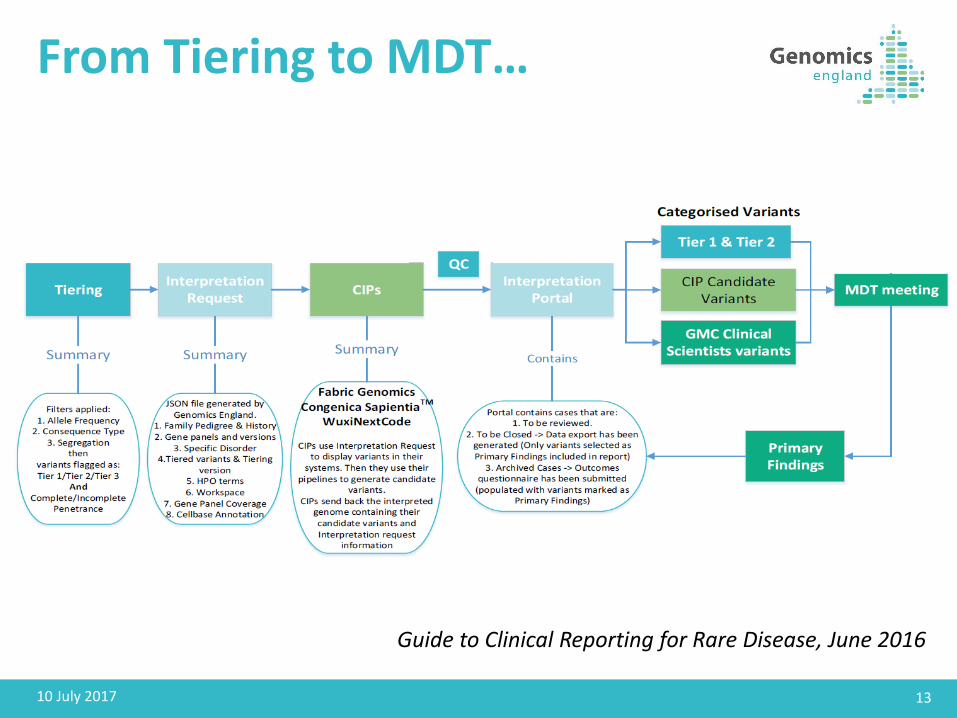
From Tiering to MDT…
Guide to Clinical Reporting for Rare Disease, June 2016

1410 July 2017
From Tiering to MDT…‘Interpretation Request’ and ‘Interpreted Genome’ JSON files
Accessible to NHS GMCs via ‘CIP API’
Guide to Clinical Reporting for Rare Disease, June 2016

1510 July 2017
From Tiering to MDT…Lists pending/open/closed cases
Links to CIP page for familyCollects outcomes
Access to HTML reports (incl coverage) & other files
Guide to Clinical Reporting for Rare Disease, June 2016

Patient/ family
Phenotypes & Pedigree
DNA
Genome sequence
Annotated VCFs
Tiered variants
Gene Panel
Variant filtering
Annotation Companies
Review
Gene Panels
Clinical assessment
GeCIP(s)
Validation
Outcomes
Reporting tool
Semi-automatedInterpretation pipeline
Report QA
Test request
WORKFLOW MANAGER
DATA DISTRIBUTION FRAMEWORK

Return of results to sites
Reports to date (to 19th June)
• 1988 families (4106 genomes) dispatched to CIPs
• 1741 families (3462 genomes) reports sent to GMCs
• 221 families (467 genomes) outcomes questionnaires completed by GMC labs
• Includes >85% of pilot; status summary to sites for remaining in coming week
Upcoming
• Further batch passing through pipeline now >1000 families
• = ALL of the families with HPO data and no other data issues on GRCh37
• Release to CIPs from mid-July
• Results to GMCs from 1-2 weeks after that (i.e. from late July)
Next steps
• Move to GRCh38 reporting (and with it, CNV calls that we expect to use)
• Move away from batches to even out flow
• Looking at mechanisms to allow GMCs greater control re flow
1710 July 2017

A pipeline for diagnostics
• Major focus of the next year will be validation, QA and accreditation
• This will involve analysis of samples already held as part of the programme
• Plus sequencing of additional positive control samples
• Existing pipeline components• New components, eg STR
Validation, QA and accreditation

Summary
• An overview of the project’s approach to reporting in RD
• An introduction to some of the components that are available to NHS GMCs• Including PanelApp, CIP API and Interpretation portal
• Increased automation is beginning to increase the pace at which reports can be returned to sites• Upcoming batch of >1000 main programme families
• Next steps including• Move to build 38
• Focus of experimental activity to validate pipeline
1910 July 2017
Stay in touch
Follow ‘Genomics England’
www.genomicsengland.co.uk
@genomicsengland #genomes100k
Like the ‘Genomics England’ page





























