CLINICAL CHALLENGES PETER SAVINO AND HELEN DANESH-MEYER, EDITORS You’re Too Old for That Vinay A. Shah, MD, 1 Sandeep Randhawa, MD, 1 Thomas Mizen, MD, 4 Andrew G. Lee, MD, 1,2,3 and Rod Foroozan, MD 5 Departments of 1 Ophthalmology, 2 Neurology, and 3 Neurosurgery at the University of Iowa Hospitals and Clinics, Iowa City, Iowa, USA; the 4 H. Stanley Thompson Neuro-ophthalmology Clinic, and Departments of Ophthalmology, Neurology and Neurosurgery, Rush University Medical Center, Chicago, Illinois, USA; and 5 Baylor College of Medicine, Houston, Texas, USA (In keeping with the format of a clinical pathologic conference, the abstract and key words appear at the end of the article.) Case Report. A 72-year-old man presented with visual loss. Eighteen months prior to presentation he complained of mild decreased visual acuity OU. He was seen by an ophthalmologist and diagnosed with cataracts and subsequently underwent cataract sur- gery OD and then OS. Postoperatively, he required surgical repositioning of the intraocular lens OD. He then complained of painless progressive loss of vision OD 1 month after his cataract surgery. The left eye was normal. A retina specialist found no abnormalities. The patient subsequently was referred to a neuro- ophthalmologist in September 2004. Visual acuity was now count fingers OD and 20/30 OS. He could not read the color plates OD and correctly read 14 out of 14 Ishihara color plates OS. The pupils were equal and reactive bilaterally but he had a right relative afferent pupillary defect (RAPD). Ophthalmoscopy showed moderate pallor of the right optic nerve, but the left optic nerve was normal. Kinetic and static perimetry revealed a cecocentral scotoma OD and a normal visual field OS (Fig. 1). The past medical history was significant for hypertension, diabetes, hypercholesterolemia, and coronary artery disease. He had had a gross total resection of a melanoma from his right arm several years prior to presentation without recurrence or metastatic disease. His medications were simvastatin, finasteride, tamsulosin, amantadine, lisinopril, baby aspirin, metformin, clopidogrel, hydrochlorothia- zide, multivitamins, and glucosamine/chondroitin. Social history was negative for alcohol or tobacco use. What is the differential diagnosis? What further testing should be performed at this time? Comments Comments by Rod Foroozan, MD Slowly progressive decreased vision one month after cataract surgery is most suggestive of retinop- athy (cystoid macular edema), especially with a history of a second procedure to reposition the intraocular lens. We are not told if fluorescein angiography or optical coherence tomography (OCT) was performed at the time the patient was 403 Ó 2008 by Elsevier Inc. All rights reserved. 0039-6257/08/$--see front matter doi:10.1016/j.survophthal.2008.04.003 SURVEY OF OPHTHALMOLOGY VOLUME 53 NUMBER 4 JULY–AUGUST 2008

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
CLINICAL CHALLENGESPETER SAVINO AND HELEN DANESH-MEYER, EDITORS
You’re Too Old for ThatVinay A. Shah, MD,1 Sandeep Randhawa, MD,1 Thomas Mizen, MD,4
Andrew G. Lee, MD,1,2,3 and Rod Foroozan, MD5
Departments of 1Ophthalmology, 2Neurology, and 3Neurosurgery at the University of Iowa Hospitals and Clinics,Iowa City, Iowa, USA; the 4H. Stanley Thompson Neuro-ophthalmology Clinic, and Departments of Ophthalmology,Neurology and Neurosurgery, Rush University Medical Center, Chicago, Illinois, USA; and 5Baylor College of Medicine,Houston, Texas, USA
(In keeping with the format of a clinical pathologic conference,the abstract and key words appear at the end of the article.)
SURVEY OF OPHTHALMOLOGY VOLUME 53 � NUMBER 4 � JULY–AUGUST 2008
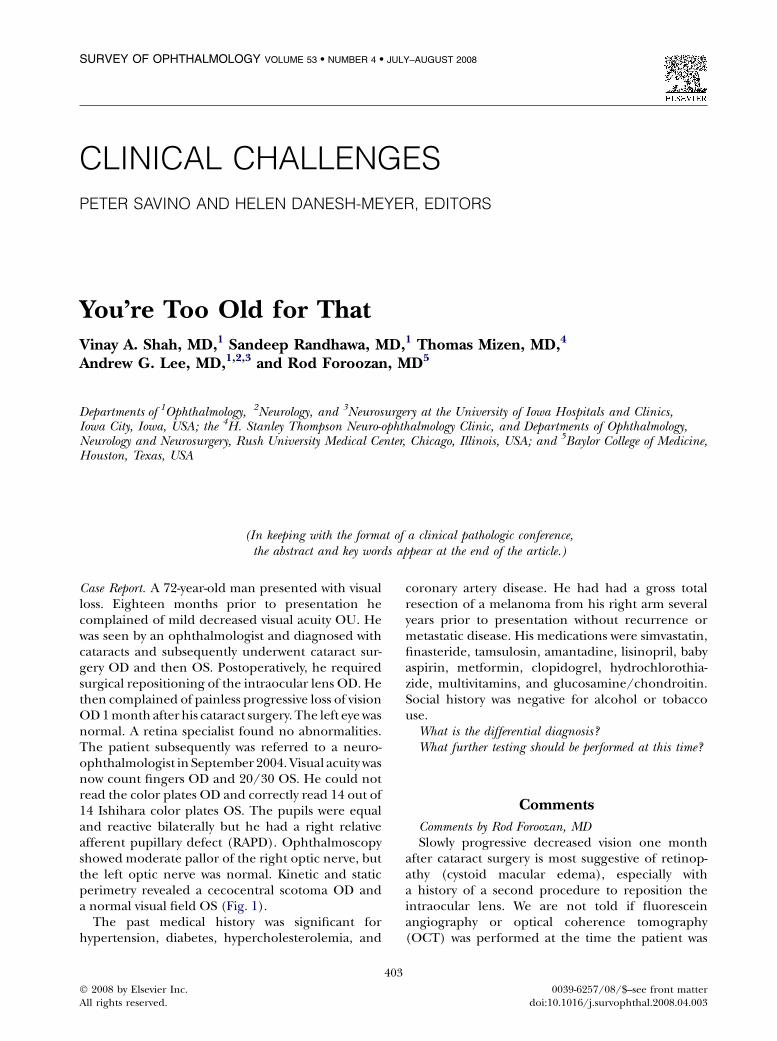
Case Report. A 72-year-old man presented with visualloss. Eighteen months prior to presentation hecomplained of mild decreased visual acuity OU. Hewas seen by an ophthalmologist and diagnosed withcataracts and subsequently underwent cataract sur-gery OD and then OS. Postoperatively, he requiredsurgical repositioning of the intraocular lens OD. Hethen complained of painless progressive loss of visionOD 1 month after his cataract surgery. The left eye wasnormal. A retina specialist found no abnormalities.The patient subsequently was referred to a neuro-ophthalmologist in September 2004. Visual acuity wasnow count fingers OD and 20/30 OS. He could notread the color plates OD and correctly read 14 out of14 Ishihara color plates OS. The pupils were equaland reactive bilaterally but he had a right relativeafferent pupillary defect (RAPD). Ophthalmoscopyshowed moderate pallor of the right optic nerve, butthe left optic nerve was normal. Kinetic and staticperimetry revealed a cecocentral scotoma OD anda normal visual field OS (Fig. 1).
The past medical history was significant forhypertension, diabetes, hypercholesterolemia, and
40
� 2008 by Elsevier Inc.All rights reserved.
coronary artery disease. He had had a gross totalresection of a melanoma from his right arm severalyears prior to presentation without recurrence ormetastatic disease. His medications were simvastatin,finasteride, tamsulosin, amantadine, lisinopril, babyaspirin, metformin, clopidogrel, hydrochlorothia-zide, multivitamins, and glucosamine/chondroitin.Social history was negative for alcohol or tobaccouse.
What is the differential diagnosis?What further testing should be performed at this time?
Comments
Comments by Rod Foroozan, MDSlowly progressive decreased vision one month
after cataract surgery is most suggestive of retinop-athy (cystoid macular edema), especially witha history of a second procedure to reposition theintraocular lens. We are not told if fluoresceinangiography or optical coherence tomography(OCT) was performed at the time the patient was
3
0039-6257/08/$--see front matterdoi:10.1016/j.survophthal.2008.04.003
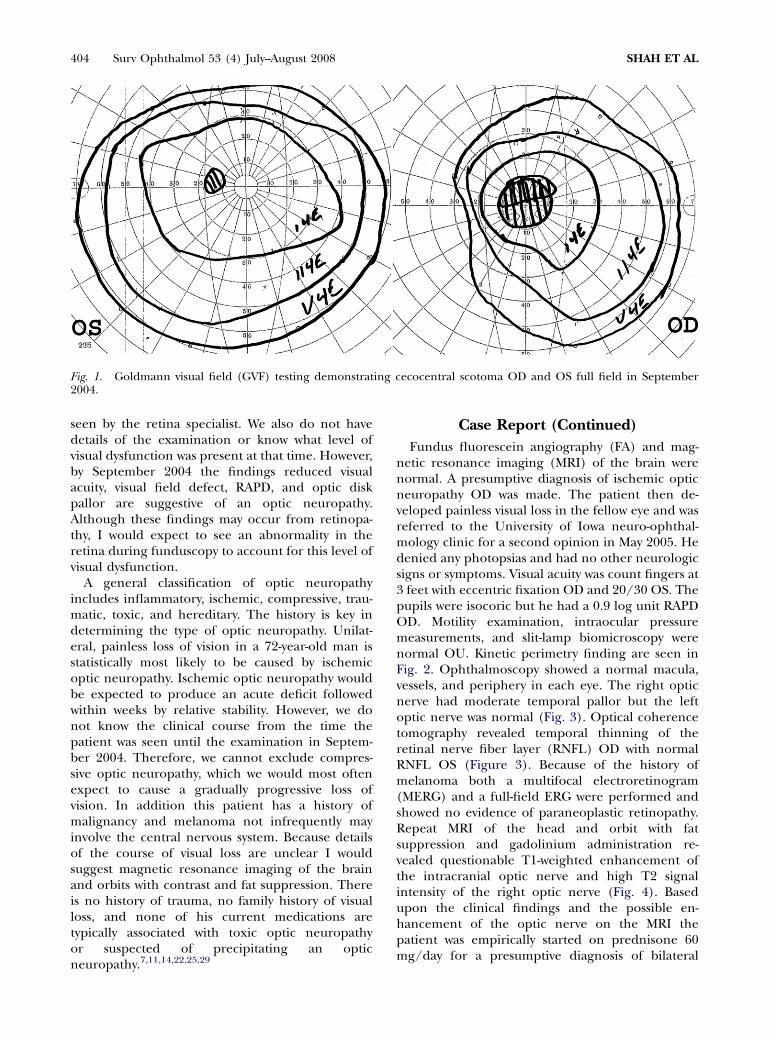
Fig. 1. Goldmann visual field (GVF) testing demonstrating cecocentral scotoma OD and OS full field in September2004.
404 Surv Ophthalmol 53 (4) July--August 2008 SHAH ET AL
seen by the retina specialist. We also do not havedetails of the examination or know what level ofvisual dysfunction was present at that time. However,by September 2004 the findings reduced visualacuity, visual field defect, RAPD, and optic diskpallor are suggestive of an optic neuropathy.Although these findings may occur from retinopa-thy, I would expect to see an abnormality in theretina during funduscopy to account for this level ofvisual dysfunction.
A general classification of optic neuropathyincludes inflammatory, ischemic, compressive, trau-matic, toxic, and hereditary. The history is key indetermining the type of optic neuropathy. Unilat-eral, painless loss of vision in a 72-year-old man isstatistically most likely to be caused by ischemicoptic neuropathy. Ischemic optic neuropathy wouldbe expected to produce an acute deficit followedwithin weeks by relative stability. However, we donot know the clinical course from the time thepatient was seen until the examination in Septem-ber 2004. Therefore, we cannot exclude compres-sive optic neuropathy, which we would most oftenexpect to cause a gradually progressive loss ofvision. In addition this patient has a history ofmalignancy and melanoma not infrequently mayinvolve the central nervous system. Because detailsof the course of visual loss are unclear I wouldsuggest magnetic resonance imaging of the brainand orbits with contrast and fat suppression. Thereis no history of trauma, no family history of visualloss, and none of his current medications aretypically associated with toxic optic neuropathyor suspected of precipitating an opticneuropathy.7,11,14,22,25,29
Case Report (Continued)
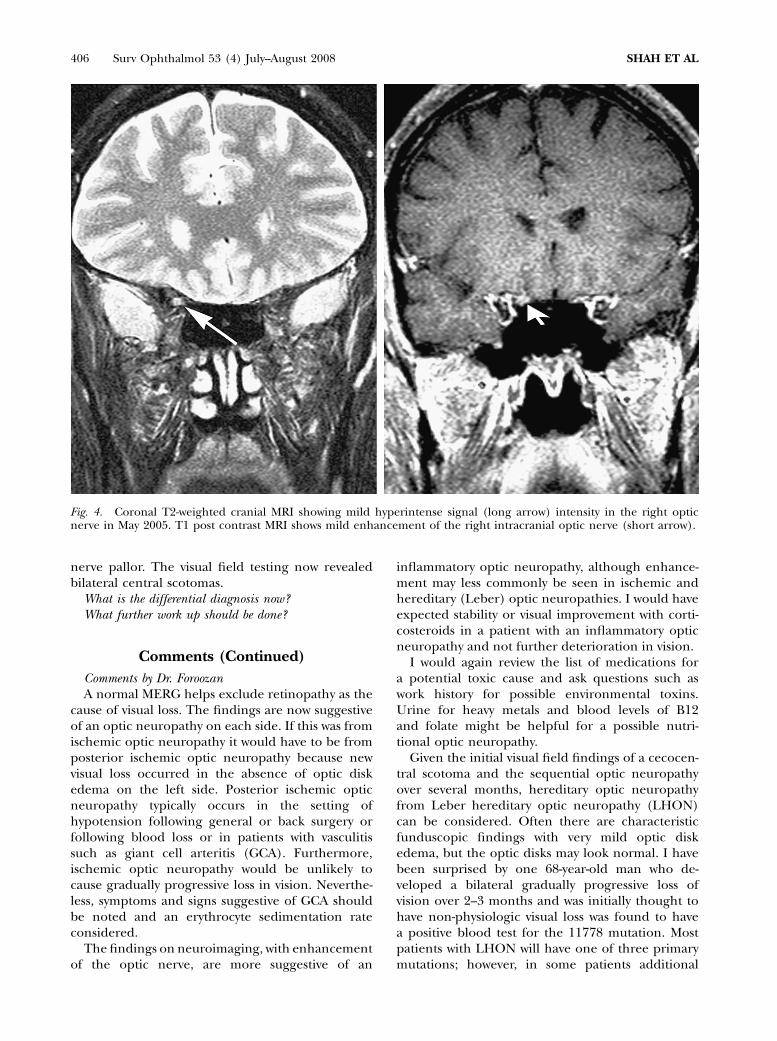
Fundus fluorescein angiography (FA) and mag-netic resonance imaging (MRI) of the brain werenormal. A presumptive diagnosis of ischemic opticneuropathy OD was made. The patient then de-veloped painless visual loss in the fellow eye and wasreferred to the University of Iowa neuro-ophthal-mology clinic for a second opinion in May 2005. Hedenied any photopsias and had no other neurologicsigns or symptoms. Visual acuity was count fingers at3 feet with eccentric fixation OD and 20/30 OS. Thepupils were isocoric but he had a 0.9 log unit RAPDOD. Motility examination, intraocular pressuremeasurements, and slit-lamp biomicroscopy werenormal OU. Kinetic perimetry finding are seen inFig. 2. Ophthalmoscopy showed a normal macula,vessels, and periphery in each eye. The right opticnerve had moderate temporal pallor but the leftoptic nerve was normal (Fig. 3). Optical coherencetomography revealed temporal thinning of theretinal nerve fiber layer (RNFL) OD with normalRNFL OS (Figure 3). Because of the history ofmelanoma both a multifocal electroretinogram(MERG) and a full-field ERG were performed andshowed no evidence of paraneoplastic retinopathy.Repeat MRI of the head and orbit with fatsuppression and gadolinium administration re-vealed questionable T1-weighted enhancement ofthe intracranial optic nerve and high T2 signalintensity of the right optic nerve (Fig. 4). Basedupon the clinical findings and the possible en-hancement of the optic nerve on the MRI thepatient was empirically started on prednisone 60mg/day for a presumptive diagnosis of bilateral
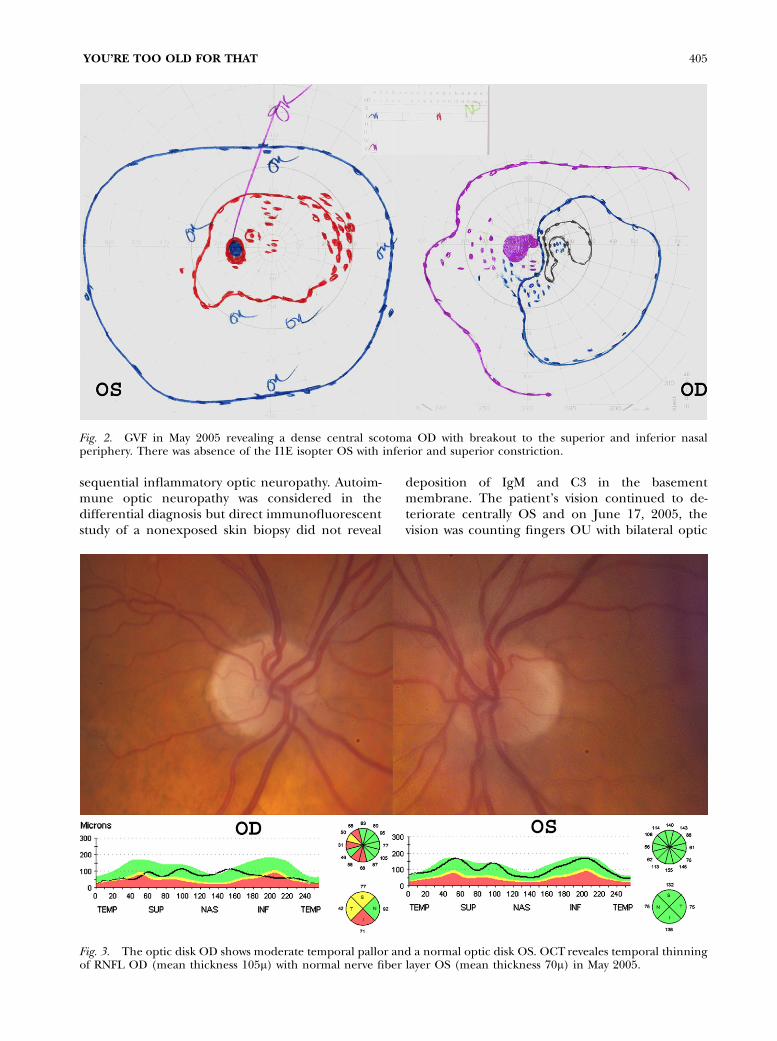
Fig. 2. GVF in May 2005 revealing a dense central scotoma OD with breakout to the superior and inferior nasalperiphery. There was absence of the I1E isopter OS with inferior and superior constriction.
YOU’RE TOO OLD FOR THAT 405
sequential inflammatory optic neuropathy. Autoim-mune optic neuropathy was considered in thedifferential diagnosis but direct immunofluorescentstudy of a nonexposed skin biopsy did not reveal
deposition of IgM and C3 in the basementmembrane. The patient’s vision continued to de-teriorate centrally OS and on June 17, 2005, thevision was counting fingers OU with bilateral optic
Fig. 3. The optic disk OD shows moderate temporal pallor and a normal optic disk OS. OCT reveales temporal thinningof RNFL OD (mean thickness 105m) with normal nerve fiber layer OS (mean thickness 70m) in May 2005.
406 Surv Ophthalmol 53 (4) July--August 2008 SHAH ET AL
Fig. 4. Coronal T2-weighted cranial MRI showing mild hyperintense signal (long arrow) intensity in the right opticnerve in May 2005. T1 post contrast MRI shows mild enhancement of the right intracranial optic nerve (short arrow).
nerve pallor. The visual field testing now revealedbilateral central scotomas.
What is the differential diagnosis now?What further work up should be done?
Comments (Continued)
Comments by Dr. ForoozanA normal MERG helps exclude retinopathy as the
cause of visual loss. The findings are now suggestiveof an optic neuropathy on each side. If this was fromischemic optic neuropathy it would have to be fromposterior ischemic optic neuropathy because newvisual loss occurred in the absence of optic diskedema on the left side. Posterior ischemic opticneuropathy typically occurs in the setting ofhypotension following general or back surgery orfollowing blood loss or in patients with vasculitissuch as giant cell arteritis (GCA). Furthermore,ischemic optic neuropathy would be unlikely tocause gradually progressive loss in vision. Neverthe-less, symptoms and signs suggestive of GCA shouldbe noted and an erythrocyte sedimentation rateconsidered.
The findings on neuroimaging, with enhancementof the optic nerve, are more suggestive of an
inflammatory optic neuropathy, although enhance-ment may less commonly be seen in ischemic andhereditary (Leber) optic neuropathies. I would haveexpected stability or visual improvement with corti-costeroids in a patient with an inflammatory opticneuropathy and not further deterioration in vision.
I would again review the list of medications fora potential toxic cause and ask questions such aswork history for possible environmental toxins.Urine for heavy metals and blood levels of B12and folate might be helpful for a possible nutri-tional optic neuropathy.
Given the initial visual field findings of a cecocen-tral scotoma and the sequential optic neuropathyover several months, hereditary optic neuropathyfrom Leber hereditary optic neuropathy (LHON)can be considered. Often there are characteristicfunduscopic findings with very mild optic diskedema, but the optic disks may look normal. I havebeen surprised by one 68-year-old man who de-veloped a bilateral gradually progressive loss ofvision over 2--3 months and was initially thought tohave non-physiologic visual loss was found to havea positive blood test for the 11778 mutation. Mostpatients with LHON will have one of three primarymutations; however, in some patients additional
YOU’RE TOO OLD FOR THAT 407
blood tests may be necessary to exclude othermutations.
At this point the clinical findings and tempo ofvisual loss are atypical for the most common opticneuropathies. Antibodies for autoimmune opticneuropathy can be ordered through the laboratoryat the University of California, Davis. Although theyield is likely to be low in the absence of othersymptoms, other screening blood tests can beconsidered including: RPR, FTA-Abs, angiotensinconverting enzyme, anti-nuclear antibody (ANA),c-ANCA, p-ANCA. A lumbar puncture with analysisof cerebrospinal fluid may help exclude malignantcells within the cerebrospinal fluid.
Case Report (Continued)
Testing for LHON was sent from the outsideacademic institution and was negative for the threecommon LHON mutations. Because of his priorhistory of melanoma and the mild enhancement ofthe optic nerve on the MRI, his primary carephysicians ordered a positron emission tomography(PET) scan that showed nonspecific decreasedmetabolic activity in the parietal lobes and slightincreased activity in the caudate nuclei, which was ofuncertain significance. There was some increasedmetabolic activity in one lymph node in the left axilla,which appeared to be due to benign lymphadenitis.There was some nonspecific increased activity in thesmall and large intestine but no evidence forsarcoidosis or an underlying neoplastic process.Serum C-reactive protein (CRP), rheumatoid factor(RF), ANA, and complement levels were all negative.Cerebrospinal fluid (CSF) analysis (i.e., CSF protein,cell count, glucose, and cytology) was normal. He was
empirically treated with oral corticosteroids forpresumptive inflammatory optic neuropathy.
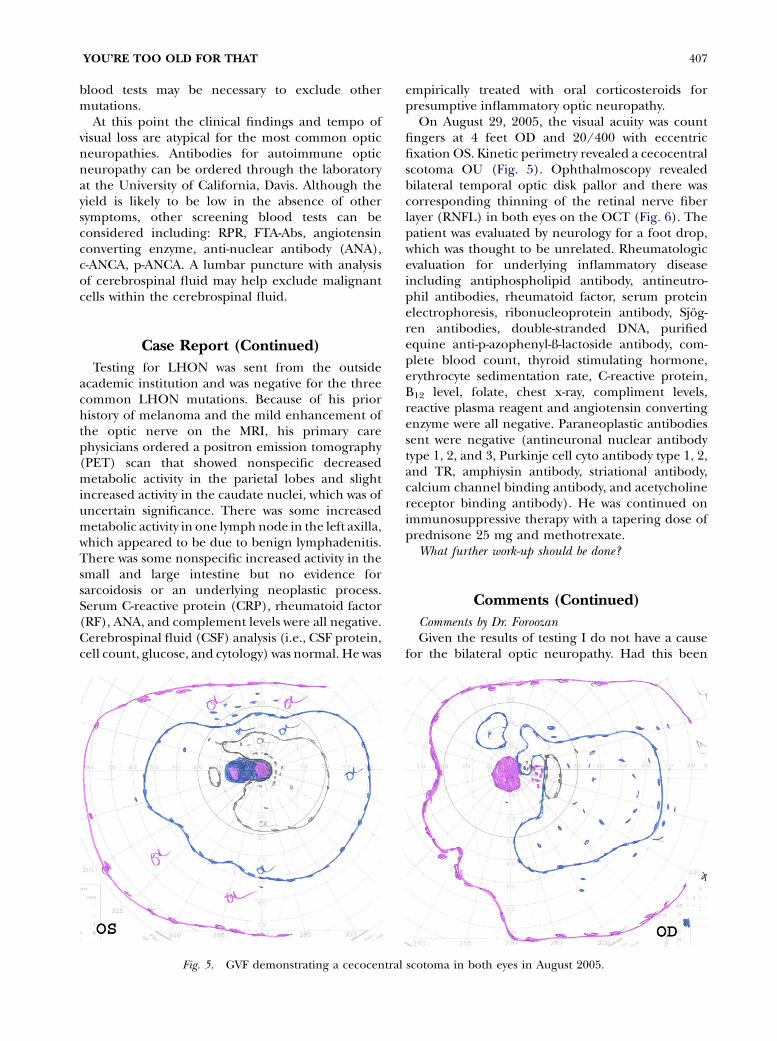
On August 29, 2005, the visual acuity was countfingers at 4 feet OD and 20/400 with eccentricfixation OS. Kinetic perimetry revealed a cecocentralscotoma OU (Fig. 5). Ophthalmoscopy revealedbilateral temporal optic disk pallor and there wascorresponding thinning of the retinal nerve fiberlayer (RNFL) in both eyes on the OCT (Fig. 6). Thepatient was evaluated by neurology for a foot drop,which was thought to be unrelated. Rheumatologicevaluation for underlying inflammatory diseaseincluding antiphospholipid antibody, antineutro-phil antibodies, rheumatoid factor, serum proteinelectrophoresis, ribonucleoprotein antibody, Sjog-ren antibodies, double-stranded DNA, purifiedequine anti-p-azophenyl-ß-lactoside antibody, com-plete blood count, thyroid stimulating hormone,erythrocyte sedimentation rate, C-reactive protein,B12 level, folate, chest x-ray, compliment levels,reactive plasma reagent and angiotensin convertingenzyme were all negative. Paraneoplastic antibodiessent were negative (antineuronal nuclear antibodytype 1, 2, and 3, Purkinje cell cyto antibody type 1, 2,and TR, amphiysin antibody, striational antibody,calcium channel binding antibody, and acetycholinereceptor binding antibody). He was continued onimmunosuppressive therapy with a tapering dose ofprednisone 25 mg and methotrexate.
What further work-up should be done?
Comments (Continued)
Comments by Dr. ForoozanGiven the results of testing I do not have a cause
for the bilateral optic neuropathy. Had this been
Fig. 5. GVF demonstrating a cecocentral scotoma in both eyes in August 2005.
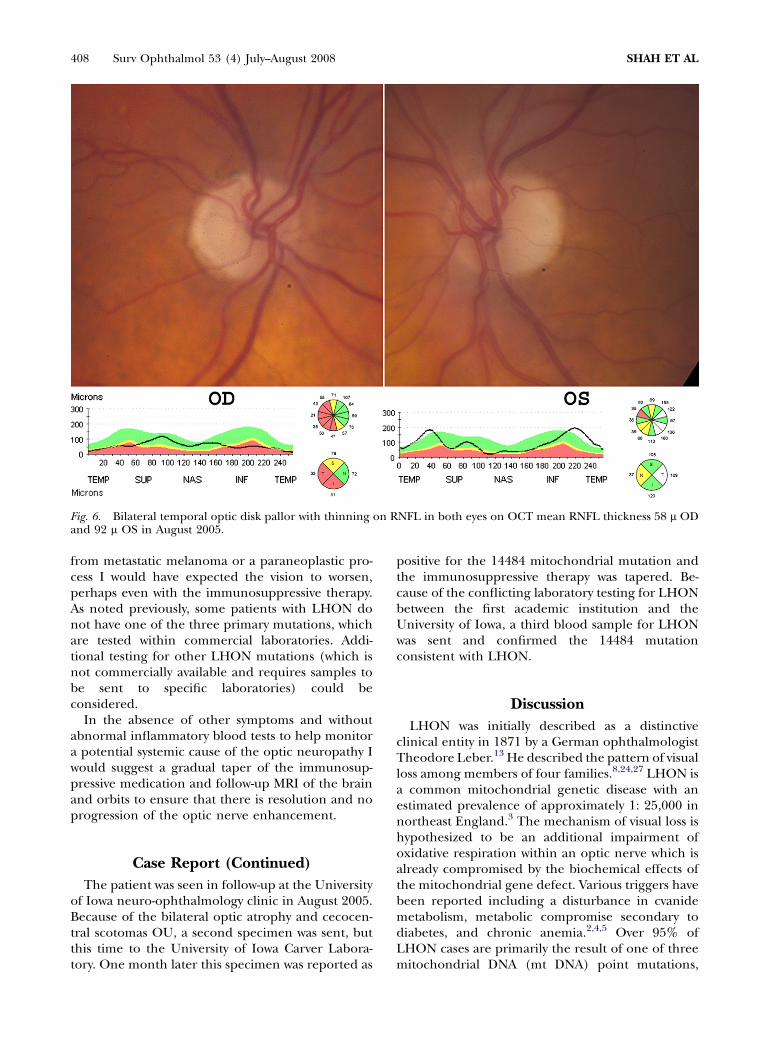
Fig. 6. Bilateral temporal optic disk pallor with thinning on RNFL in both eyes on OCT mean RNFL thickness 58 m ODand 92 m OS in August 2005.
408 Surv Ophthalmol 53 (4) July--August 2008 SHAH ET AL
from metastatic melanoma or a paraneoplastic pro-cess I would have expected the vision to worsen,perhaps even with the immunosuppressive therapy.As noted previously, some patients with LHON donot have one of the three primary mutations, whichare tested within commercial laboratories. Addi-tional testing for other LHON mutations (which isnot commercially available and requires samples tobe sent to specific laboratories) could beconsidered.
In the absence of other symptoms and withoutabnormal inflammatory blood tests to help monitora potential systemic cause of the optic neuropathy Iwould suggest a gradual taper of the immunosup-pressive medication and follow-up MRI of the brainand orbits to ensure that there is resolution and noprogression of the optic nerve enhancement.
Case Report (Continued)
The patient was seen in follow-up at the Universityof Iowa neuro-ophthalmology clinic in August 2005.Because of the bilateral optic atrophy and cecocen-tral scotomas OU, a second specimen was sent, butthis time to the University of Iowa Carver Labora-tory. One month later this specimen was reported as
positive for the 14484 mitochondrial mutation andthe immunosuppressive therapy was tapered. Be-cause of the conflicting laboratory testing for LHONbetween the first academic institution and theUniversity of Iowa, a third blood sample for LHONwas sent and confirmed the 14484 mutationconsistent with LHON.
Discussion
LHON was initially described as a distinctiveclinical entity in 1871 by a German ophthalmologistTheodore Leber.13 He described the pattern of visualloss among members of four families.8,24,27 LHON isa common mitochondrial genetic disease with anestimated prevalence of approximately 1: 25,000 innortheast England.3 The mechanism of visual loss ishypothesized to be an additional impairment ofoxidative respiration within an optic nerve which isalready compromised by the biochemical effects ofthe mitochondrial gene defect. Various triggers havebeen reported including a disturbance in cvanidemetabolism, metabolic compromise secondary todiabetes, and chronic anemia.2,4,5 Over 95% ofLHON cases are primarily the result of one of threemitochondrial DNA (mt DNA) point mutations,
YOU’RE TOO OLD FOR THAT 409
G11778A (50--76% of families), G3460A (7--30%)and T14484C (10--31%).15,16,19
In approximately 70% of affected individualsvisual loss begins in the second or third decade oflife and 95% of patients lose their vision by theirfifth decade of life.16,21 To our knowledge, theoldest reported patient with LHON to date is73 years old and was also reported from ourinstitution.1 This patient had the 11778 mt DNA.Our patient was 72 years old when he started havingvisual loss; however, to our knowledge he is one ofthe oldest patients if not the oldest reported patientwith LHON harboring the 14484 mt DNA. It hasbeen noted that this and other atypical late onsetcases are associated with a poorer prognosis forvisual recovery.
Johns et al described the clinical features of theLHON with the 14484 mutation and compared itsclinic features with the other known mutations.They found that the 14484 mitochondrial DNAmutation may have a better prognosis for visualrecovery.9 In their study of 19 visually symptomaticpatients with 14484 mutations, the average age ofonset was 27 years (range 10 to 56 years). Theclinical presentation of these patients as is similar toother known LHON mutations. However the au-thors found a higher incidence of visual recovery(37%, improved to 20/60 or better) in thesepatients as compared with the 11778 (4%), 3460(28%) and 15257 (28%) mutations.10,26
Although MRI of the brain and orbits is usuallynormal in patients with LHON,18 there have beena few cases with enhancement in the opticnerve.17,20,28 In our patient, cranial MRI showeda mild amount of enhancement on T1 postcontrast and increased optic nerve signal on theT2-weighted imaging that prompted more aggres-sive evaluation for inflammatory and autoimmuneoptic neuropathies. There have been a few neuro-pathological studies of LHON. These consistentlyshow degeneration of the retinal ganglion layer andoptic nerve with axonal loss, occasionally with mildinflammation.6,12,23 This may be the basis of opticnerve enhancement on MRI seen in some cases ofLHON.
This patient had undergone testing for LHONearly in his evaluation that was negative. A repeatLHON test at our institution, however, provedpositive for the 14484 mutation. Variability inlaboratory testing, as with any test can, producefalse positive and false negative results and thiscase emphasizes the importance of clinical corre-lation and repeat testing if necessary in specificsituations.
LHON should be considered in the differentialdiagnosis of any bilateral and sequential optic
neuropathy regardless of age. LHON may presentwith a stuttering course and may show mild opticnerve enhancement on MRI that might be mistakenfor an inflammatory optic neuropathy. Spontaneousimprovement, especially in the 14484 mutation, maybe misinterpreted (as was presumed in our patient)as evidence of steroid responsiveness.
References
1. Ajax ET, Kardon R: Late-onset Leber’s hereditary opticneuropathy. J Neuroophthalmol 18:30--1, 1998
2. Berninger TA, von Meyer L, Siess E, et al: Leber’s hereditaryoptic atrophy: further evidence for a defect of cyanidemetabolism? Br J Ophthalmol 73:314--6, 1989
3. Chinnery PF, Johnson MA, Wardell TM, et al: Theepidemiology of pathogenic mitochondrial DNA mutations.Ann Neurol 48:188--93, 2000
4. DuBois LG, Feldon SE: Evidence for a metabolic trigger forLeber’s hereditary optic neuropathy. A case report. J ClinNeuroophthalmol 12:15--6, 1992
5. Goyal S, Riordan-Eva P, Coakes RL: Late onset of Leber’shereditary optic neuropathy precipitated by anaemia. Eye18:1017--8, 2004
6. Howell N: Human mitochondrial diseases: answeringquestions and questioning answers. Int Rev Cytol 186:49--116, 1999
7. Hwang JM, Park HW: Carbon monoxide poisoning as anepigenetic factor for Leber’s hereditary optic neuropathy.Korean J Ophthalmol 10:122--3, 1996
8. Imai Y, Moriwaki D: A probable case of cytoplasmicinheritance in man: a critique of Lebers disease. J Genet33:163--7, 1936
9. Johns DR, Heher KL, Miller NR, et al: Leber’s hereditaryoptic neuropathy. Clinical manifestations of the 14484mutation. Arch Ophthalmol 111:495--8, 1993
10. Johns DR, Smith KH, Miller NR: Leber’s hereditary opticneuropathy. Clinical manifestations of the 3460 mutation.Arch Ophthalmol 110:1577--81, 1992
11. Kerrison JB, Miller NR, Hsu F, et al: A case-control study oftobacco and alcohol consumption in Leber hereditary opticneuropathy. Am J Ophthalmol 130:803--12, 2000
12. Kovacs GG, Hoftberger R, Majtenyi K, et al: Neuropathologyof white matter disease in Leber’s hereditary optic neurop-athy. Brain 128:35--41, 2005
13. Leber T: Ueber hereditaere und congenital angelegtesehnervenleiden. Graefes Arch Clin Exp Ophthalmol 17:249--91, 1871
14. Mackey DA, Fingert JH, Luzhansky JZ, et al: Leber’shereditary optic neuropathy triggered by antiretroviraltherapy for human immunodeficiency virus. Eye 17:312--7,2003
15. Mackey DA, Oostra RJ, Rosenberg T, et al: Primarypathogenic mtDNA mutations in multigeneration pedigreeswith Leber hereditary optic neuropathy. Am J Hum Genet59:481--5, 1996
16. Man PY, Turnbull DM, Chinnery PF: Leber hereditary opticneuropathy. J Med Genet 39:162--9, 2002
17. Mashima Y, Oshitari K, Imamura Y, et al: Orbital highresolution magnetic resonance imaging with fast spin echoin the acute stage of Leber’s hereditary optic neuropathy. JNeurol Neurosurg Psychiatry 64:124--7, 1998
18. Newman NJ: Leber’s hereditary optic neuropathy. Newgenetic considerations. Arch Neurol 50:540--8, 1993
19. Nikoskelainen EK, Huoponen K, Juvonen V, et al: Ophthal-mologic findings in Leber hereditary optic neuropathy, withspecial reference to mtDNA mutations. Ophthalmology 103:504--14, 1996
20. Phillips PH, Vaphiades M, Glasier CM, et al: Chiasmalenlargement and optic nerve enhancement on magnetic

410 Surv Ophthalmol 53 (4) July--August 2008 SHAH ET AL
resonance imaging in leber hereditary optic neuropathy.Arch Ophthalmol 121:577--9, 2003
21. Riordan-Eva P, Sanders MD, Govan GG, et al: The clinicalfeatures of Leber’s hereditary optic neuropathy defined bythe presence of a pathogenic mitochondrial DNA mutation.Brain 118:319--37, 1995
22. Rizzo JF: Adenosine triphosphate deficiency: a genre ofoptic neuropathy. Neurology 45:11--6, 1995
23. Saadati HG, Hsu HY, Heller KB, et al: A histopathologic andmorphometric differentiation of nerves in optic nervehypoplasia and Leber hereditary optic neuropathy. ArchOphthalmol 116:911--6, 1998
24. Seedorff T: Leber’s disease. Acta Ophthalmol (Copenh) 46:4--25, 1968
25. Shaikh S, Ta C, Basham AA, et al: Leber hereditary opticneuropathy associated with antiretroviral therapy for humanimmunodeficiency virus infection. Am J Ophthalmol 131:143--5, 2001
26. Stone EM, Newman NJ, Miller NR, et al: Visual recoveryin patients with Leber’s hereditary optic neuropathy and
the 11778 mutation. J Clin Neuroophthalmol 12:10--4,1992
27. Van Senus AHC: Lebers disease in the Netherlands. DocOphthalmol 17:1--162, 1963
28. Vaphiades MS, Newman NJ: Optic nerve enhancementon orbital magnetic resonance imaging in Leber’shereditary optic neuropathy. J Neuroophthalmol 19:238--9, 1999
29. Warner RB, Lee AG: Leber hereditary optic neuropathyassociated with use of ephedra alkaloids. Am J Ophthalmol134:918--20, 2002
The authors reported no proprietary or commercial interest inany product mentioned or concept discussed in this article.
Reprint address: Andrew G. Lee, MD, Department ofOphthalmology, University of Iowa Hospitals and Clinics, 200Hawkins Dr., PFP Iowa City, IA 52242-1091. e-mail: [email protected].
Abstract. Leber hereditary optic neuropathy (LHON) produces a subacute and typically bilateral butsequential optic neuropathy. LHON is a mitochondrial disease and the most common mutations are atpositions 11778, 14484 and 3460. LHON typically presents in young (age 20--40), healthy men but mayoccur in either sex and at any age. We report a case of LHON in a 72-year-old man and we emphasizethe importance of testing for LHON in all cases of unexplained bilateral and sequential opticneuropathy with a ceco-central or central scotoma. (Surv Ophthalmol 53:403--410, 2008. � 2008Elsevier Inc. All rights reserved.)
Key words. central scotoma � Leber hereditary optic neuropathy
Related Documents











