www.hospicefundamentals.com Hospice Fundamentals Subscriber Webinar March 2017 © 2017 Hospice Fundamentals All Rights Reserved 1 The Clinicians Connection to Documentation: Using the PPS, FAST , BMI, MAC and NYHA March 2017 Subscriber Webinar What We’ll Cover • Common scaling and measurement tools • Importance of tools in supporting eligibility • Effective use • Common challenges Assessment Tools Tools provide a data point or points that, used in context with the whole person, help to make a determination of eligibility. It is important to assess the data points over time. The purpose of an assessment scale is reduce subjectivity and increasing objectivity Importance of Tools Communicates patient symptoms and functional status Supports effective care planning Determine if care plan is effective Revise care plan to meet current needs Anticipate future needs Foundational to eligibility determination

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

www.hospicefundamentals.com Hospice Fundamentals Subscriber WebinarMarch 2017
© 2017 Hospice FundamentalsAll Rights Reserved 1
The Clinicians Connection to Documentation: Using the PPS, FAST, BMI, MAC and NYHA
March 2017 Subscriber Webinar
What We’ll Cover
• Common scaling and measurement tools
• Importance of tools in supporting eligibility
• Effective use
• Common challenges
Assessment Tools
Tools provide a data point or points that, used in context with the whole person, help to make a determination of eligibility.
It is important to assess the data points over time.
The purpose of an assessment scale is reduce subjectivity and increasing objectivity
Importance of Tools
Communicates patient symptoms and functional status
Supports effective care planningDetermine if care plan is effective
Revise care plan to meet current needs
Anticipate future needs
Foundational to eligibility determination

www.hospicefundamentals.com Hospice Fundamentals Subscriber WebinarMarch 2017
© 2017 Hospice FundamentalsAll Rights Reserved 2
Data Points
Data points are just that, points of data
The more the accuracy and consistency of data points, the clearer the picture of the patient
Put them together to paint your patient’s picture
Medicare Coverage RequirementsMedicare wants to know what they are paying for
They review hospice records and decide whether to pay or not (or take money back)
Report card
A get paid in full
C partial payment
F free care provided
It’s the evidence
Top Denial Reasons
It all means the same thing: the documentation does not tell the reviewer the story of why the patient has a prognosis of 6 months or less
Palmetto GBA Not Hospice Appropriate
CGS Six‐month terminal prognosis not supported
NGSAccording to Medicare hospice requirements, the information provided does not support a terminal prognosis of six months or less
Common Problems 1. Using wrong tool(s) for patient or diagnosis or not using it at all2. Inconsistencies among clinicians
– Scoring – Usage – some do, some don’t– Documentation placement (especially with EMRs)
3. Clicking templates without actual data4. Not identifying scores that don’t make sense or are in conflict
with others5. Scoring without reference to context6. No baseline measurements

www.hospicefundamentals.com Hospice Fundamentals Subscriber WebinarMarch 2017
© 2017 Hospice FundamentalsAll Rights Reserved 3
Assessment Tools - Today’s Focus
• Functional performance measurement tools– Palliative Performance Scale (PPS)– Functional Assessment Staging (FAST) (measures
both cognition and function)– New York Heart Association Classification (NYHA)
• Nutritional status measurement tools– Weight scales– Body Mass Index (BMI)– Mid Arm Circumference (MAC)
Effective Use of Tools Requires Decision Making
1. Determination of which tools will be used (for which patients and when)
2. Defining how tool data will be incorporated into documentation system so it goes in the same place in the same way for trending and retrieval
3. How tool data will connect to care planning and delivery of care
4. On‐going education needs5. Monitoring and auditing plans
Using Functional
Measurement Tools
The PPS & FAST
• Excellent tools for monitoring, quantifying and documenting the functional performance and decline in hospice patients
• Documents a dementia patient’s current cognitive abilities– How they manifest in the patient’s functional abilities– Predict and document disease progression

www.hospicefundamentals.com Hospice Fundamentals Subscriber WebinarMarch 2017
© 2017 Hospice FundamentalsAll Rights Reserved 4
Probability of Death within Six Months
PPS 30 40 50 >60
Cancer 98.3% 95.5% 92.8% 89.1%
Cardiovasculardisease
89.8% 74.2% 65.3% 51.8%
Dementia 73.6% 54.9% 51.4% 36.6%
Pulmonary disease 92.4% 79.9% 71.6% 63.8%
Stroke 67.4% 48.4% 39.4% 32.6%
Harris, et alCan Hospices Predict which Patients Will Die within Six Months?Journal of Palliative Medicine; Vol 17, Number 8, 2014
Palliative Performance Scale (PPS)• Designed to measure functional performance and progressive
decline in palliative care patients– Ambulation
– Activity
– Evidence of disease
– Self care
– Intake
– Level of consciousness
• Designed to measure what a person is capable of doing, not what they choose to do
% Ability toAmbulate
Activity and Evidence of Disease Self-Care Intake Level of Conscious.
100 Full Normal activity, no evidence of disease Full Normal Full
90 Full Normal activity, some evidence of disease Full Normal Full
80 Full Normal activity with effort, some evidence of disease
Full Normal or reduced Full
70 Reduced Unable to do normal work, some evidence of disease
Full Normal or reduced Full
60 Reduced Unable to do hobby or housework, Evidence of significant disease
Occasional assist necessary Normal or reduced Full or confusion
50 Mainly sit/lie Unable to do any work, extensive disease Considerable assistance required
Normal or reduced Full or confusion
40 Mainly in bed Unable to do any work, extensive disease Mainly assistance Normal or reduced Full, drowsy, or confusion
30 Totally bed bound
Unable to do any work, extensive disease Total care Normal or reduced Full, drowsy, or confusion
20 Totally bed bound
Unable to do any work, extensive disease Total care Minimal sips Full, drowsy, or confusion
10 Totally bed bound
Unable to do any work, extensive disease Total care Mouth care only Drowsy or coma
0 Death - - - -
Palliative Performance Scale
15Copyright © 2001 Victoria Hospice Society
FAST (Functional Assessment Staging)• 16‐item scale designed to parallel the progressive activity
limitations associated with Alzheimer’s Disease• A 7‐step staging system, to determine hospice eligibility which
identifies progressive steps and sub‐steps of functional decline• Designed for Alzheimer’s Disease
• Little information on other dementias• Problems of “non‐ordinate” patients
• Stage 7 identifies the threshold of activity limitation that would support a six‐month prognosis– To qualify under Alzheimer's Disease the patient should have a FAST
of 7 along with secondary conditions

www.hospicefundamentals.com Hospice Fundamentals Subscriber WebinarMarch 2017
© 2017 Hospice FundamentalsAll Rights Reserved 5
Keys to ScoringThe scoring must be done sequentially:
– Its not the lowest score for which the patient qualifies, it’s the lowest uninterrupted score
Unable to ambulate without assistance
– This means personal assistance, someone holding them up so they can walk ‐ It is not: walker, cane, standby assist
Verbal communication
– Ability to speak limited to approximately a half a dozen intelligible different words or fewer, in the course of an average day or in the course of an intensive interview
Deficits are a result of the dementing process
– Walking limitation can not be from osteoarthritis or other non related disease processes
Case Study
Patient with Alzheimer's living in a SNF– Unable to ambulate safely without assistance, but tries and falls
frequently
– Cannot hold his balance on the edge of the bed
– No longer smiles.
– Frequently tells staff things like “don’t touch that”, “leave me alone”, “this isn’t my house”, “I want ice cream”
– Is incontinent of bowel and bladder
– Needs assistance to dress, bathe and toilet
– What’s the FAST?
New York Heart Association Functional Classification
NYHA Classification
©2017 All Rights Reserved R&C Healthcare Solutions
NYHA Functional Classification
• Provides a simple way of classifying the extent of heart failure
• Places patients in 1 of 4 categories based on– How much they are limited during physical activity
– Limitations / symptoms are in regards to normal breathing
– Varying degrees in shortness of breath and / or angina pain

www.hospicefundamentals.com Hospice Fundamentals Subscriber WebinarMarch 2017
© 2017 Hospice FundamentalsAll Rights Reserved 6
End Stage Heart Disease-Prognostication
NYHA Class
1 Year Mortality
I 5-10%
II-III 10-15%
IV 30-40%
Fast Facts and Concepts #143Gary M Reisfield, MD & George R Wilson, MD
New York Heart Association Functional Classification
Class I
Mild No limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, or dyspnea (shortness of breath) or angina
Class II
Mild Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in fatigue, palpitation, or dyspnea or angina
Class III
Moderate Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes fatigue, palpitation, or dyspnea, or angina
Class IV
Severe Unable to carry out any physical activity without discomfort. Symptoms of cardiac insufficiency or the angina syndrome may be present even at rest. If any physical activity is undertaken, discomfort is increased
The Criteria Committee of the New York Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels. 9th ed. Boston, Mass: Little, Brown & Co; 1994:253-256.
Mr. Smith
78 year old admitted with ASHD. Depressed and anxious because of disease. Wife states his function has declined lately. His medical records show he has CHF, COPD, HTN, anemia, and a history of TIA’s. Echocardiogram of 4 months ago notes an EF of 25%. His hemoglobin is 10.3
Mr. Smith denies any real complaints. States “I don’t have the same energy as I used to, probably should quit smoking”. He does admit to having some chest pain with exertion.
His wife states he gets short of breath just walking around the house but not at rest. He has oxygen but doesn’t like to use it. He is much less active compared to a three months ago when he was fully ambulatory with only occasional dyspnea and chest pain.
Mr. Smith’s Assessment
• Medications include Lisinopril, Nitroglycerin prn, Lasix 40 mg. daily, Albuterol prn, Atrovent and aspirin.
• Assessment shows that he gets around the house some, but spends a lot of time sitting in a chair. He needs assistance bathing, but otherwise can do his own ADLs. However, states he is very fatigued afterwards. His appetite is fair and has lost 10 lbs. (6% of his body weight) in the past 3 months. He states he is too tired to eat and nothing tastes good. His wife is worried because he doesn’t eat and use to be a big eater.
• He has 2 – 3+ edema to his lower extremities. Lungs sounds have coarse rales with expiratory wheezes. O2 sat on RA is 88%.
• What is his NYHA Classification?
www.hospicefundamentals.com Hospice Fundamentals Subscriber WebinarMarch 2017
© 2017 Hospice FundamentalsAll Rights Reserved 7
% Ability toAmbulate
Activity and Evidence of Disease
Self-Care Intake Level of Conscious.
100 Full Normal activity, no evidence of disease Full Normal Full
90 Full Normal activity, some evidence of disease Full Normal Full
80 Full Normal activity with effort, some evidence of disease
Full Normal or reduced
Full
70 Reduced Unable to do normal work, some evidence of disease
Full Normal or reduced
Full
60 Reduced Unable to do hobby or housework, Evidence of significant disease
Occasional assist necessary
Normal or reduced
Full or confusion
50 Mainly sit/lie
Unable to do any work, extensive disease Considerable assistance required
Normal or reduced
Full or confusion
40 Mainly in bed
Unable to do any work, extensive disease Mainly assistance Normal or reduced
Full, drowsy, or confusion
30 Totally bed bound
Unable to do any work, extensive disease Total care Normal or reduced
Full, drowsy, or confusion
20 Totally bed bound
Unable to do any work, extensive disease Total care Minimal sips Full, drowsy, or confusion
10 Totally bed bound
Unable to do any work, extensive disease Total care Mouth care only Drowsy or coma
0 Death - - - -
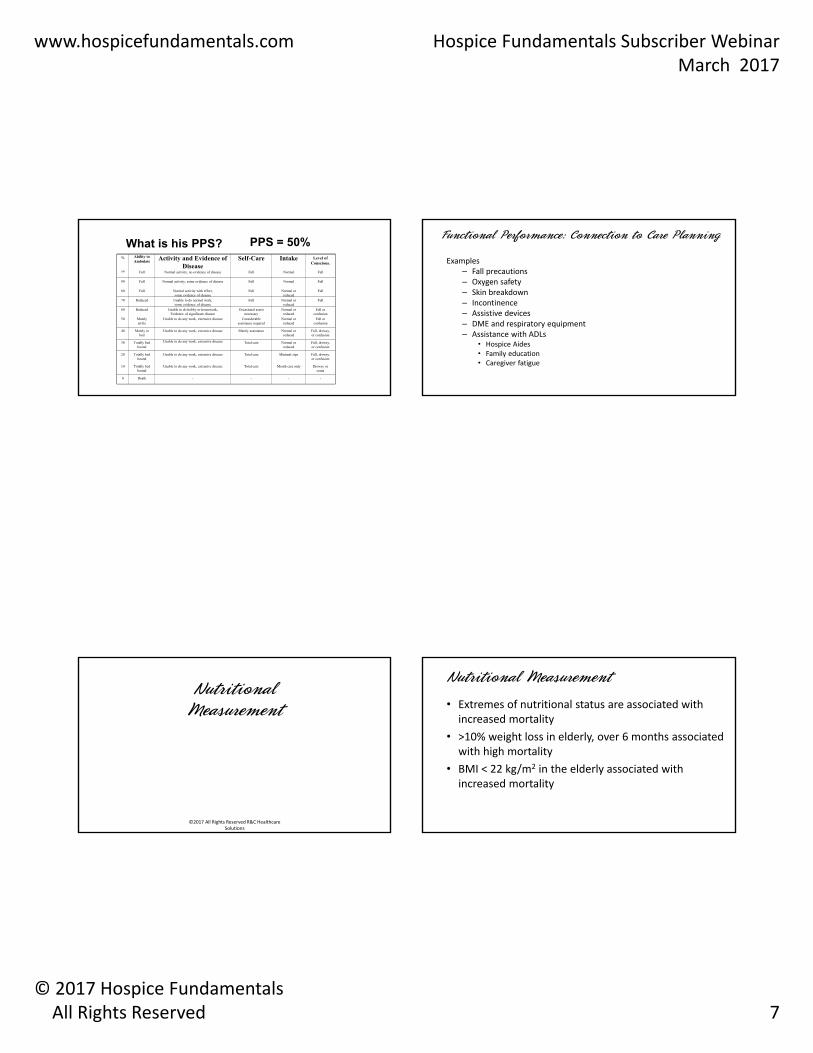
What is his PPS? PPS = 50% Functional Performance: Connection to Care Planning
Examples– Fall precautions– Oxygen safety– Skin breakdown– Incontinence– Assistive devices– DME and respiratory equipment– Assistance with ADLs
• Hospice Aides• Family education• Caregiver fatigue
Nutritional Measurement
©2017 All Rights Reserved R&C Healthcare Solutions
Nutritional Measurement
• Extremes of nutritional status are associated with increased mortality
• >10% weight loss in elderly, over 6 months associated with high mortality
• BMI < 22 kg/m2 in the elderly associated with increased mortality

www.hospicefundamentals.com Hospice Fundamentals Subscriber WebinarMarch 2017
© 2017 Hospice FundamentalsAll Rights Reserved 8
Weights
• Admission
– Accurate actual weight (not reported)
– For NF patients, if weights fluctuate find out why and then get an accurate admission weight
– Obtain weight from 6 months ago (if available)
– Obtain MAC for baseline future need• Ongoing
– Accurate actual weight (not reported)
– For NF patients, don’t accept wide discrepancies • Take into account impact of fluid retention
BMI
• Measure of body fat based on height and weight that applies to adult men and women
• Underweight ‐ BMI is less than 18.5
• Accurate actual weight (not what is reported)
• Maximum adult height (reported)
• Half arm‐span • Multiply the half arm span measurement by 2
Nutritional Assessment-MAC• Provides an indication of skeletal muscle mass, bone and
subcutaneous fat
• Used for patients who cannot be weighed
• Key point is consistency in measurement– Standard method
– Centimeters
• Obtain a MAC on every patient at admission
Nutrition: Connection to Care Planning
• Examples
– Weight loss• Nutritional assessments
– Calorie consumption
– Diet
• Family and caregiver education food intake and end of life
– Weight gain• Fluid retention: heart failure, chronic lung disease, kidney disease, liver
disease, cancer, medications
– Physical assessment

www.hospicefundamentals.com Hospice Fundamentals Subscriber WebinarMarch 2017
© 2017 Hospice FundamentalsAll Rights Reserved 9
Where Are the Opportunities for Improvement?
• Frequency of measurements
• Which arm
• Consistency
Mid Upper Arm Circumference (MAC)
Date cms
2/15/2017 16.4
2/1/2017 16.9
1/23/2017 17.7
1/16/2017 16.8
1/11/2017 17.5
Could This Be Improved?
Date Weight MAC O2 sats FAST
9/9/2016 22.0 cm LA 98% 7c
10/7/2016 18.0 cm LA 94% Ra 7b
11/15/2016 19.5 cm LA 97% 7b
12/15/2016 123 19.5 cm LA 96% Ra 7c
1/24/2017 125 19.5 cm LA 92% 7c
2/21/2017 129 20.0 cm LA 92% 7c
Audit Tool Example

www.hospicefundamentals.com Hospice Fundamentals Subscriber WebinarMarch 2017
© 2017 Hospice FundamentalsAll Rights Reserved 10
Actions of The Prudent HospiceDetermine which tools will be used (and for which type of patients and when)
Define how tool data will be incorporated into documentation system so it goes in the same place in the same way for trending and retrieval
Understand how the trending ability of your EMR
Use the power of your documentation system
Teach staff how tools connect to care and care planning
Educate and then educate some more
Implement effective auditing and use the results to develop and implement improvement activities
References
• BMI App
– IPhone: http://apps.usa.gov/bmi‐app.shtml
– Droid: http://www.freewarelovers.com/android/app/bmi‐calculator
• https://www.victoriahospice.org
• Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels. 9th ed. Boston, Mass: Little, Brown & Co; 1994:253‐256The Criteria Committee of the New York .
• Reisberg, B. Functional Assessment Staging (FAST). Psychopharmacology Bulletin, 1988; 24:653‐659.
To Contact UsSusan Balfour919‐491‐0699
Roseanne Berry480‐650‐5604
Charlene Ross602‐740‐0783
[email protected] information enclosed was current at the time it was presented. This presentation is intended to serve as a tool to assist providers and is not intended to grant rights or impose obligations.
Although every reasonable effort has been made to assure the accuracy of the information within these pages, the ultimate responsibility for the correct submission of claims and response to any remittance advice lies with the provider of services.
Hospice Fundamentals September 2017 Subscriber Webinar Handout
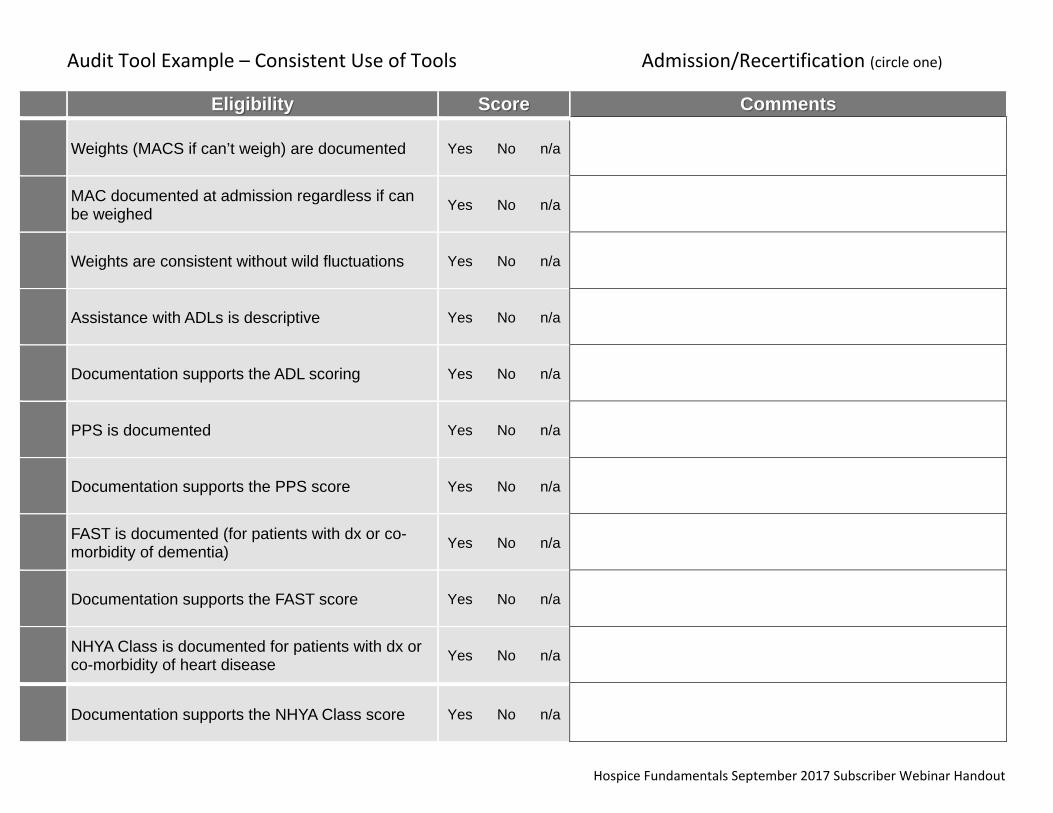
Audit Tool Example – Consistent Use of Tools Admission/Recertification (circle one)
Eligibility Score Comments
Weights (MACS if can’t weigh) are documented Yes No n/a
MAC documented at admission regardless if can be weighed Yes No n/a
Weights are consistent without wild fluctuations Yes No n/a
Assistance with ADLs is descriptive Yes No n/a
Documentation supports the ADL scoring Yes No n/a
PPS is documented Yes No n/a
Documentation supports the PPS score Yes No n/a
FAST is documented (for patients with dx or co-morbidity of dementia) Yes No n/a
Documentation supports the FAST score Yes No n/a
NHYA Class is documented for patients with dx or co-morbidity of heart disease Yes No n/a
Documentation supports the NHYA Class score Yes No n/a

8/22/2012
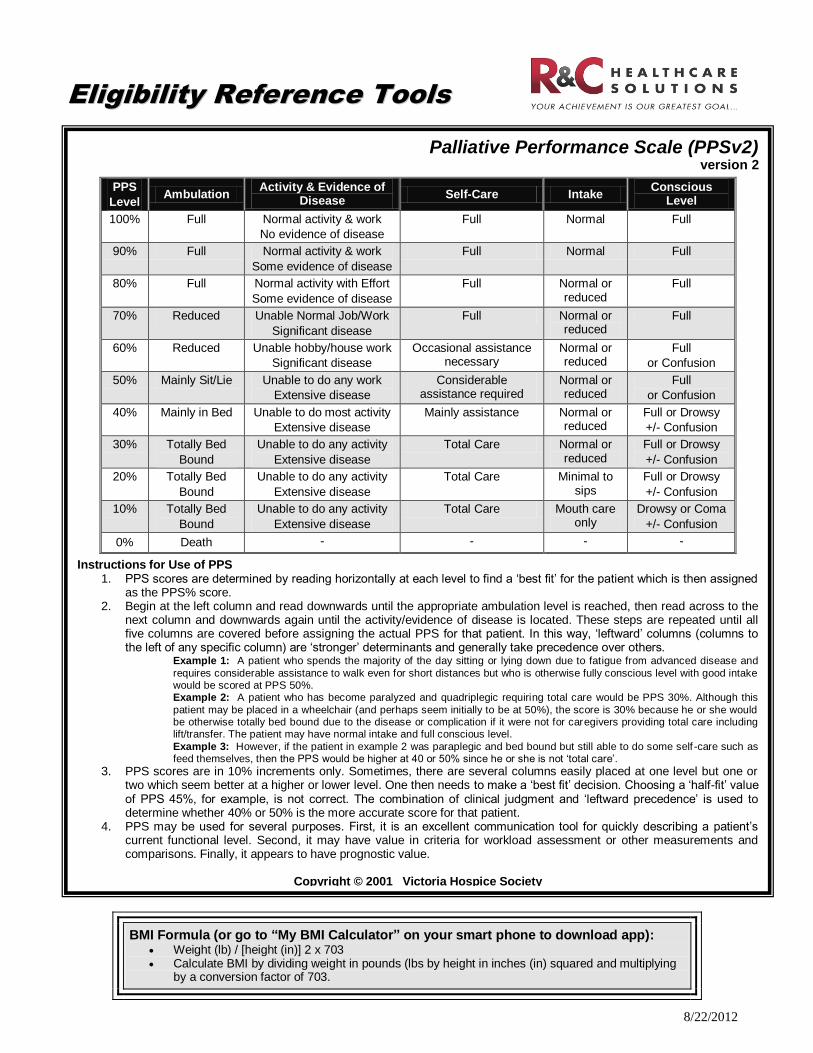
BMI Formula (or go to “My BMI Calculator” on your smart phone to download app): Weight (lb) / [height (in)] 2 x 703 Calculate BMI by dividing weight in pounds (lbs by height in inches (in) squared and multiplying
by a conversion factor of 703.
EElliiggiibbiilliittyy RReeffeerreennccee TToooollss
Palliative Performance Scale (PPSv2) version 2
PPS
Level Ambulation
Activity & Evidence of Disease
Self-Care Intake Conscious
Level
100% Full Normal activity & work
No evidence of disease
Full Normal Full
90% Full Normal activity & work
Some evidence of disease
Full Normal Full
80% Full Normal activity with Effort
Some evidence of disease
Full Normal or reduced
Full
70% Reduced Unable Normal Job/Work
Significant disease
Full Normal or reduced
Full
60% Reduced Unable hobby/house work
Significant disease
Occasional assistance necessary
Normal or reduced
Full
or Confusion
50% Mainly Sit/Lie Unable to do any work
Extensive disease
Considerable assistance required
Normal or reduced
Full
or Confusion
40% Mainly in Bed Unable to do most activity
Extensive disease
Mainly assistance Normal or reduced
Full or Drowsy
+/- Confusion
30% Totally Bed
Bound
Unable to do any activity
Extensive disease
Total Care Normal or reduced
Full or Drowsy
+/- Confusion
20% Totally Bed
Bound
Unable to do any activity
Extensive disease
Total Care Minimal to sips
Full or Drowsy
+/- Confusion
10% Totally Bed
Bound
Unable to do any activity
Extensive disease
Total Care Mouth care only
Drowsy or Coma
+/- Confusion
0% Death - - - -
Instructions for Use of PPS 1. PPS scores are determined by reading horizontally at each level to find a ‘best fit’ for the patient which is then assigned
as the PPS% score. 2. Begin at the left column and read downwards until the appropriate ambulation level is reached, then read across to the
next column and downwards again until the activity/evidence of disease is located. These steps are repeated until all five columns are covered before assigning the actual PPS for that patient. In this way, ‘leftward’ columns (columns to the left of any specific column) are ‘stronger’ determinants and generally take precedence over others.
Example 1: A patient who spends the majority of the day sitting or lying down due to fatigue from advanced disease and
requires considerable assistance to walk even for short distances but who is otherwise fully conscious level with good intake would be scored at PPS 50%. Example 2: A patient who has become paralyzed and quadriplegic requiring total care would be PPS 30%. Although this
patient may be placed in a wheelchair (and perhaps seem initially to be at 50%), the score is 30% because he or she would be otherwise totally bed bound due to the disease or complication if it were not for caregivers providing total care including lift/transfer. The patient may have normal intake and full conscious level.
Example 3: However, if the patient in example 2 was paraplegic and bed bound but still able to do some self -care such as feed themselves, then the PPS would be higher at 40 or 50% since he or she is not ‘total care’.
3. PPS scores are in 10% increments only. Sometimes, there are several columns easily placed at one level but one or two which seem better at a higher or lower level. One then needs to make a ‘best fit’ decision. Choosing a ‘half-fit’ value of PPS 45%, for example, is not correct. The combination of clinical judgment and ‘leftward precedence’ is used to determine whether 40% or 50% is the more accurate score for that patient.
4. PPS may be used for several purposes. First, it is an excellent communication tool for quickly describing a patient’s current functional level. Second, it may have value in criteria for workload assessment or other measurements and comparisons. Finally, it appears to have prognostic value.
Copyright © 2001 Victoria Hospice Society

8/22/2012
New York Heart Association Classification
Class I
(Mild) No limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, or dyspnea (shortness of breath).
Class II
(Mild) Slight limitation of physical activity. Comfortable at rest, but ordinary physical activity results in fatigue, palpitation, or dyspnea.
Class III
(Moderate) Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes fatigue, palpitation, or dyspnea.
Class IV
(Severe) Unable to carry out any physical activity without discomfort. Symptoms of cardiac insufficiency at rest. If any physical activity is undertaken, discomfort is increased.
www.RCHealthcareSolutions.com
Mid Arm Circumference (MAC)
1. Ask the pt to bend their non-dominant arm at the elbow at a right angle with the palm up.
2. Measure the distance between the acromial surface of the scapula (bony protrusion surface of upper shoulder) and the olecranon process of the elbow (bony point of the elbow) on the back of the arm.
3. Mark the mid-point between the two with the pen.
4. Ask the pt to let the arm hang loosely by his/her side.
5. Position the tape at the mid-point on the upper arm and tighten snugly. Pull the tape just snugly enough around the arm to ensure contact with the medial side of the arm and elsewhere. Make sure that the tape is not too tight that it causes dimpling or pinching of the skin. Keep the tape perpendicular to the shaft of the upper arm.
6. Measure again. Check to see if the 2 measurements are within 0.4 cm of each other. If they are not, take two more measurements and record the mean of all four
7. Record measurement to nearest millimeter and document which arm.
Functional Assessment Staging (FAST) Check highest consecutive level of disability: 1. No difficulty either subjectively or objectively. 2. Complains of forgetting location of objects. Subjective work difficulties. 3. Decreased job functioning evident to co-workers. Difficulty in traveling to new locations. Decreased organizational
capacity.* 4. Decreased ability to perform complex tasks, e.g., planning dinner for guests, handling personal finances (such as
forgetting to pay bills), difficulty marketing, etc. 5. Requires assistance in choosing proper clothing to wear for the day, season, or occasion, e.g., patient may wear the
same clothing repeatedly unless supervised.* 6.
A) Improperly putting on clothes without assistance or cueing (e.g., may put street clothes on over night clothes, or put shoes on wrong feet, or have difficulty buttoning clothing) occasionally or more frequently over the past weeks.*
B) Unable to bathe properly (e.g., difficulty adjusting the bath-water temperature) occasionally or more frequently or the past weeks.*
C) Inability to handle mechanics of toileting (e.g., forgets to flush the toilet, does not wipe properly or properly dispose of toilet tissue) occasionally or more frequently over the past weeks.*
D) Urinary incontinence (occasionally or more frequently over the past weeks).* E) Fecal incontinence (occasionally or more frequently over the past weeks).*
7. A) Ability to speak limited to approximately a half a dozen intelligible different words or fewer, in the course of an
average day or in the course of an intensive interview. B) Speech ability is limited to the use of a single intelligible word in an average day or in the course of an intensive
interview (the person may repeat the word over and over). C) Ambulatory ability is lost (cannot walk without personal assistance). D) Cannot sit up without assistance (e.g., the individual will fall over if there are not lateral rests [arms] on the chair). E) Loss of ability to smile. F) Loss of ability to hold head up independently.
* Scored primarily on the basis of information obtained from acknowledgeable informant and/or category. Reisberg, B. Functional assessment staging (FAST). Psychopharmacology Bulletin, 1988; 24:653-659.
R&C Healthcare Solutions August 2016
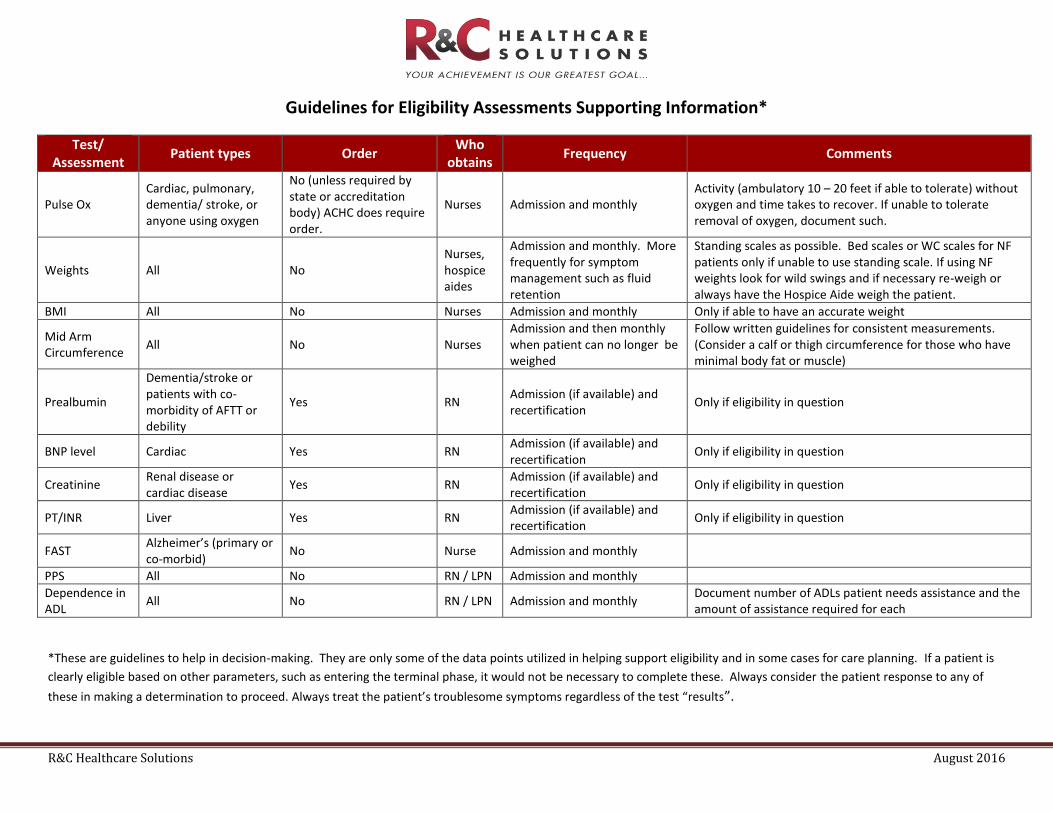
Guidelines for Eligibility Assessments Supporting Information*
Test/ Assessment
Patient types Order Who
obtains Frequency Comments
Pulse Ox Cardiac, pulmonary, dementia/ stroke, or anyone using oxygen
No (unless required by state or accreditation body) ACHC does require order.
Nurses Admission and monthly Activity (ambulatory 10 – 20 feet if able to tolerate) without oxygen and time takes to recover. If unable to tolerate removal of oxygen, document such.
Weights All No Nurses, hospice aides
Admission and monthly. More frequently for symptom management such as fluid retention
Standing scales as possible. Bed scales or WC scales for NF patients only if unable to use standing scale. If using NF weights look for wild swings and if necessary re-weigh or always have the Hospice Aide weigh the patient.
BMI All No Nurses Admission and monthly Only if able to have an accurate weight
Mid Arm Circumference
All No Nurses Admission and then monthly when patient can no longer be weighed
Follow written guidelines for consistent measurements. (Consider a calf or thigh circumference for those who have minimal body fat or muscle)
Prealbumin
Dementia/stroke or patients with co-morbidity of AFTT or debility
Yes RN Admission (if available) and recertification
Only if eligibility in question
BNP level Cardiac Yes RN Admission (if available) and recertification
Only if eligibility in question
Creatinine Renal disease or cardiac disease
Yes RN Admission (if available) and recertification
Only if eligibility in question
PT/INR Liver Yes RN Admission (if available) and recertification
Only if eligibility in question
FAST Alzheimer’s (primary or co-morbid)
No Nurse Admission and monthly
PPS All No RN / LPN Admission and monthly
Dependence in ADL
All No RN / LPN Admission and monthly Document number of ADLs patient needs assistance and the amount of assistance required for each
*These are guidelines to help in decision-making. They are only some of the data points utilized in helping support eligibility and in some cases for care planning. If a patient is
clearly eligible based on other parameters, such as entering the terminal phase, it would not be necessary to complete these. Always consider the patient response to any of
these in making a determination to proceed. Always treat the patient’s troublesome symptoms regardless of the test “results”.
Related Documents





![4000 Essential English Words - Internet Archive · 2016. 11. 17. · anxious [gerj/cjas] adj. When a person is anxious, they worry that something bad will happen.-»She was anxious](https://static.cupdf.com/doc/110x72/60b31605db2bec2604179ede/4000-essential-english-words-internet-archive-2016-11-17-anxious-gerjcjas.jpg)



