The anxious patient Royal Free & UCL Medical School Psychiatry Lectures 2010-2011 Dr Theodore Bargiotas ST5 in General Adult Psychiatry-Oxford 21.2.2011

Anxious Patient Amended 21.2.2011
Oct 24, 2014
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
The anxious patientRoyal Free & UCL Medical School
Psychiatry Lectures 2010-2011
Dr Theodore BargiotasST5 in General Adult Psychiatry-Oxford
21.2.2011
Learning Objectives
1. Symptoms anxious patients may presentwithwith
2. From symptoms to diagnosis
3. Anxiety disorders
4. Treatments
Outline
• Lecture ~1 hour
• Cases and case discussion 25 minutes
• Questions• Questions
• End
Anxiety and Anxiety disorders
What is anxiety?
• Anxiety is a normal response to a threat ordanger
• Abnormal when severity is out ofproportion to the threat or danger, or whenit outlasts them
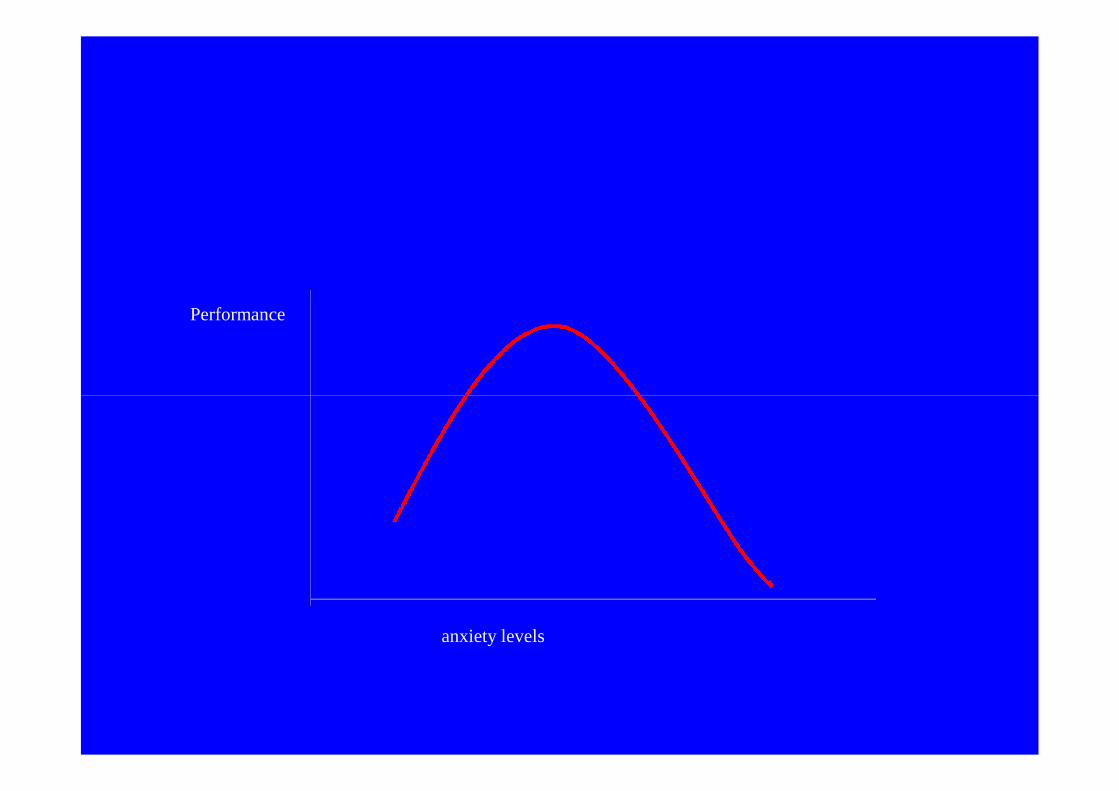
Performance
anxiety levels
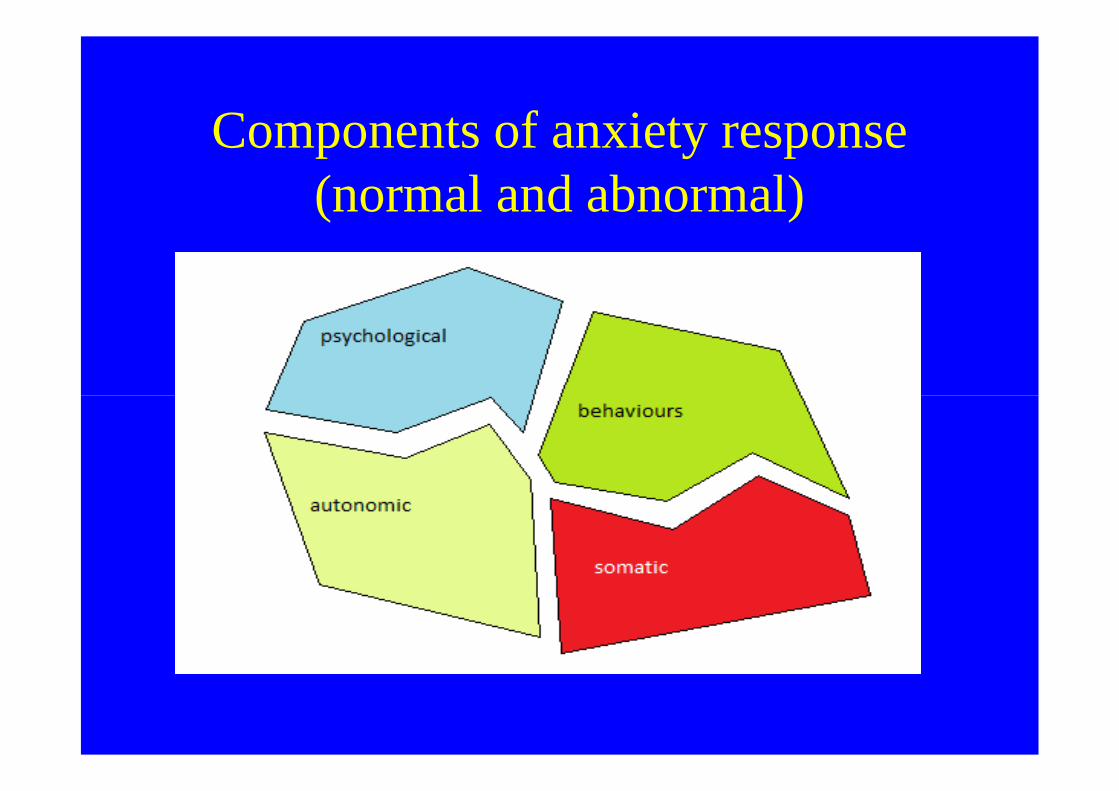
Components of anxiety response(normal and abnormal)
Components of anxiety response(normal and abnormal)
• Psychological: restlessness, narrowing ofattention, worrying thoughts, increasedattention, worrying thoughts, increasedalertness
• Somatic: muscle tension, increased respiration• Autonomic: heart rate, sweating, dry mouth,
urge to urinate or defecate• Behaviours: Avoidance of danger, safety
behaviours

What are the anxiety disorders?
• Abnormal states in which the most strikingfeatures are physical and mentalsymptoms of anxietysymptoms of anxiety
• In the absence of organic brain disease oranother psychiatric disorder
Anxiety disorders as a group
• Very common
• Used to call them neuroses
• Link with stress apparent in most of them• Link with stress apparent in most of them
• Mixtures of symptoms of anxiety
• Frequent co-morbidities with other mentaldisorders
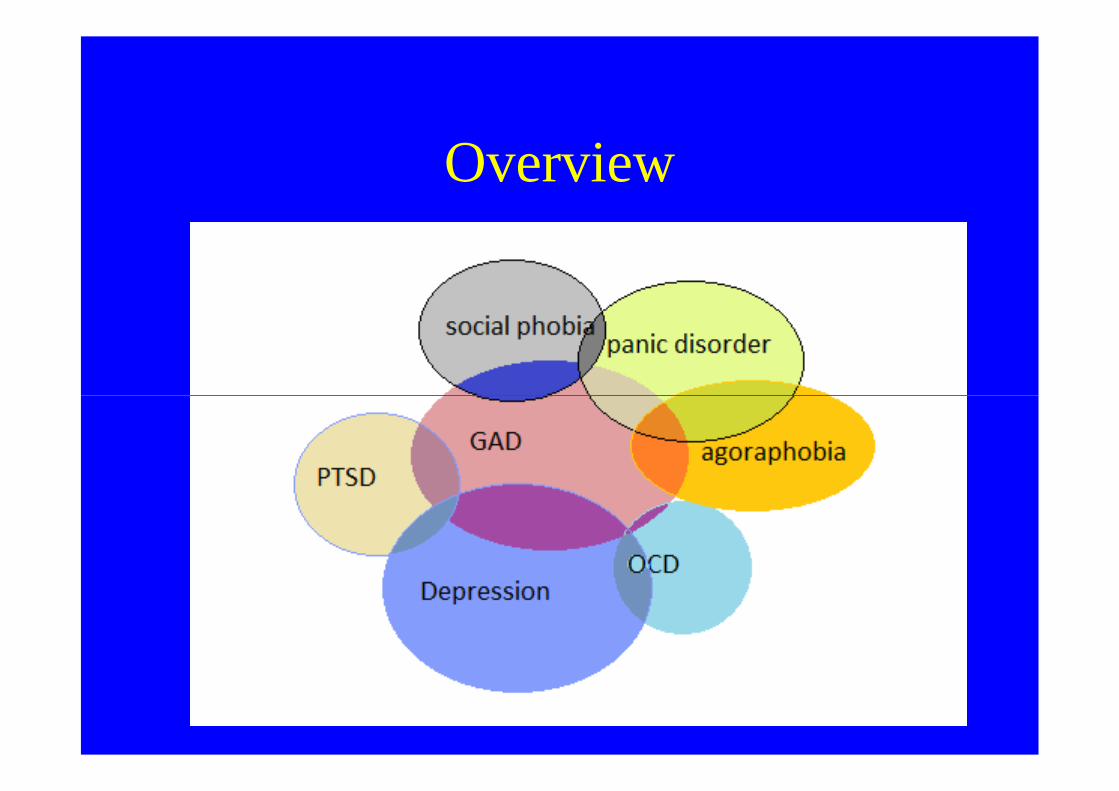
Overview
Historic info
• In the past: together with other mood disorders-depression
• Freud first suggested separate entity of anxiety
=>anxiety neurosis (psychological symptoms of anxiety) and=>anxiety neurosis (psychological symptoms of anxiety) and
=>anxiety hysteria (conversion and phobias)
• Panic disorder only introduced in the 1980s
• Conversion now separate, with somatoform disorders
Aetiology of anxiety disorders
• Evolutionary basis of fears of animals etc
• All share a modest genetic predisposition• All share a modest genetic predisposition
• Monozygotic>Dizygotic, more present infirst degree relatives
Aetiology of GAD
• Stressors+personality predisposed by geneticfactors and environmental influences in early life
• Life events: >4 in the year before• Life events: >4 in the year beforeFinlay - Jones and Brown 1981
• Genetic studies: monozygotic>dizygoticFamily studies: > in 1st degree relatives
• Early experiences: Brown and Harris 1993• Cognitive-Behavioural: conditioning theories-
cognitive schemas
Possible Neurobiologicalmechanisms
• The noradrenergic nervous system
• The HPA axis
• The amygdala and the bed nucleus of the• The amygdala and the bed nucleus of thestria terminalis
• The septohippocampal system (behaviouralinhibition system)
• The serotonergic system
• The benzodiazepine-γ-aminobutyric system
Aetiology of anxiety disorders (cont)
• Psychoanalytic theories: realistic anxiety, neuroticanxiety, moral anxiety (stemming from ego, id, superegorespectively)
• Freud: Castration anxiety: failure to overcome rivalry withfatherfather
• Experience of unmodified anxiety due to failure ofdefence mechanisms.
• Importance of Separation and loss early in life: normallyovercome by secure attachment (Bowlby 1969). If this isnot the case the individual predisposed to experienceanxiety later in life whenever
.
*learning theory –conditionedresponse (2 stage)* Evolutionary response that is nowout of placeout of place
Clinical presentation
• What symptoms do you expect an anxiouspatient to have?
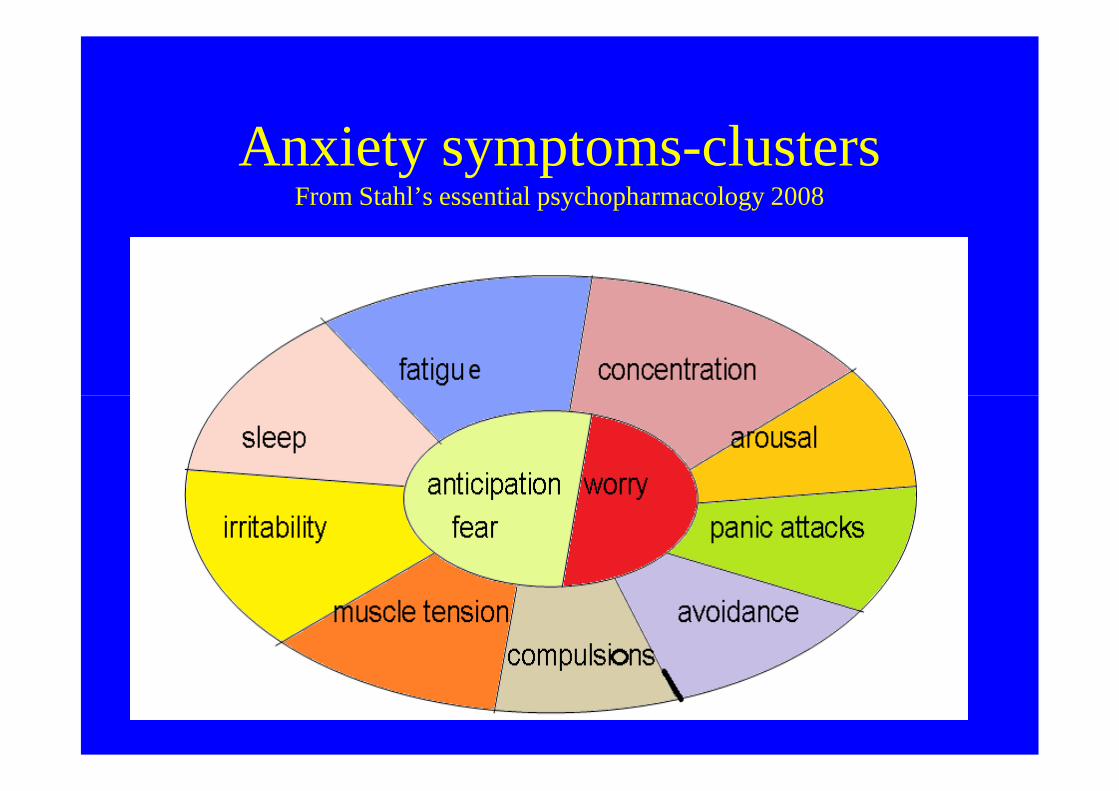
Anxiety symptoms-clustersFrom Stahl’s essential psychopharmacology 2008
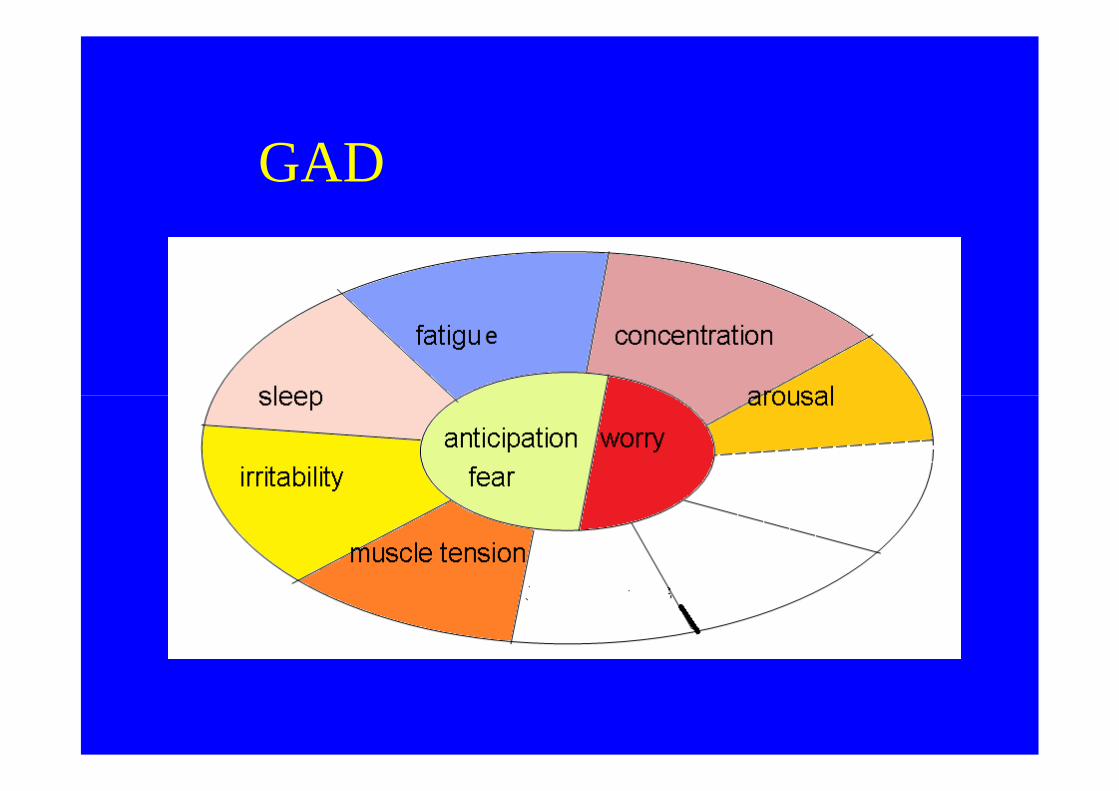
GAD
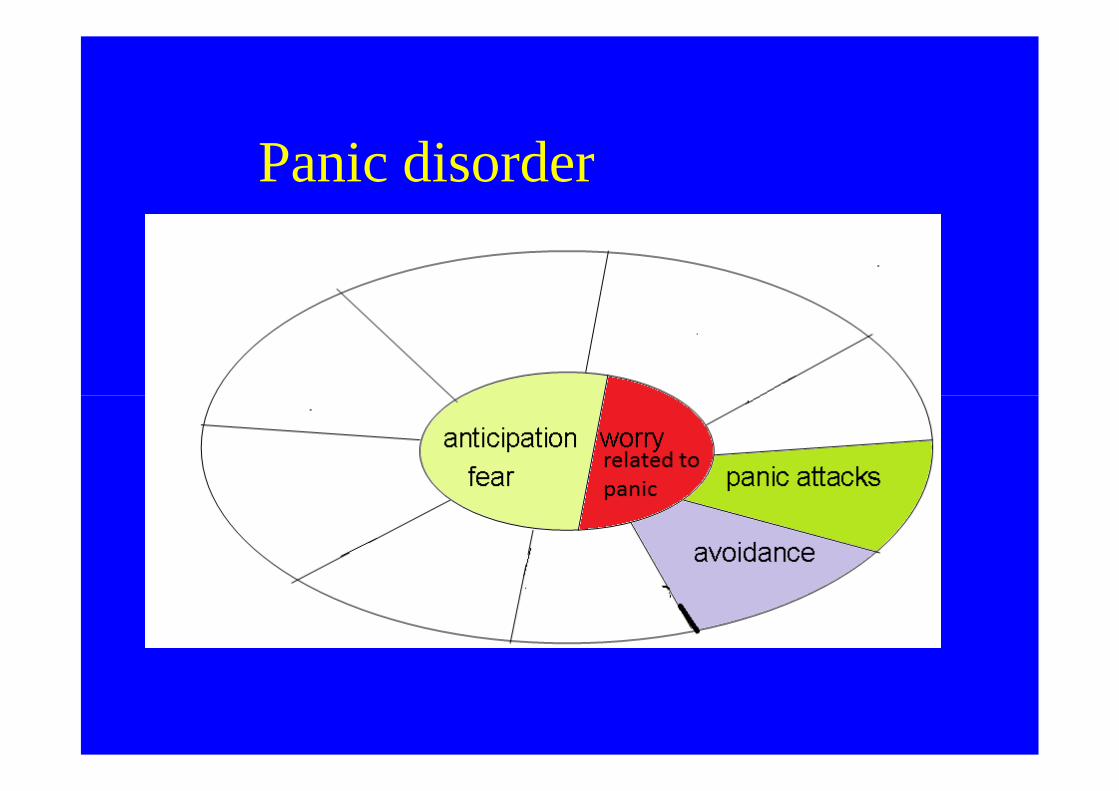
Panic disorder
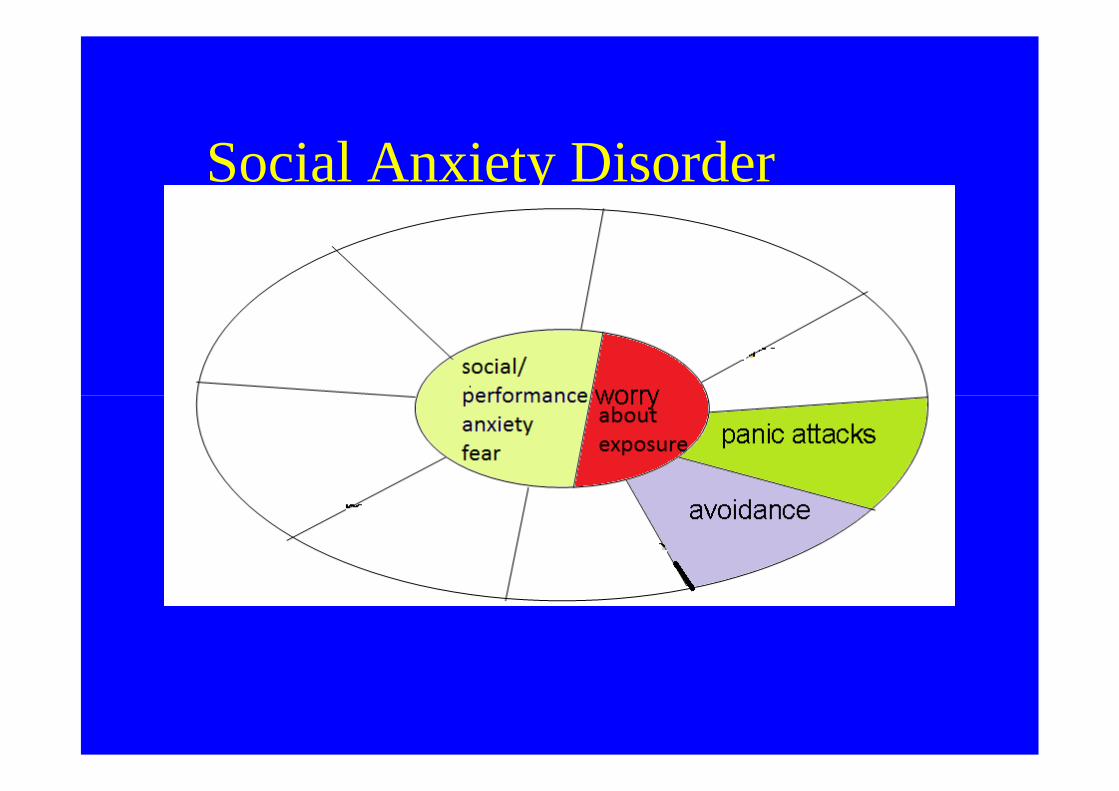
Social Anxiety Disorder
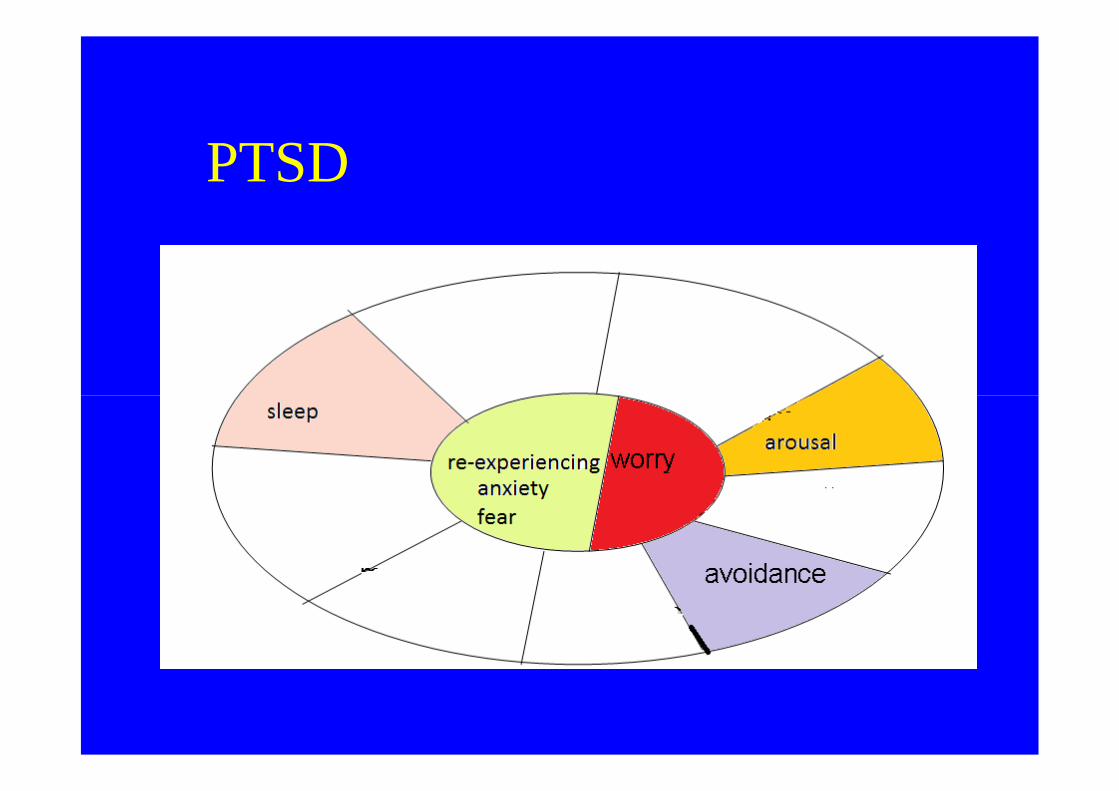
PTSD
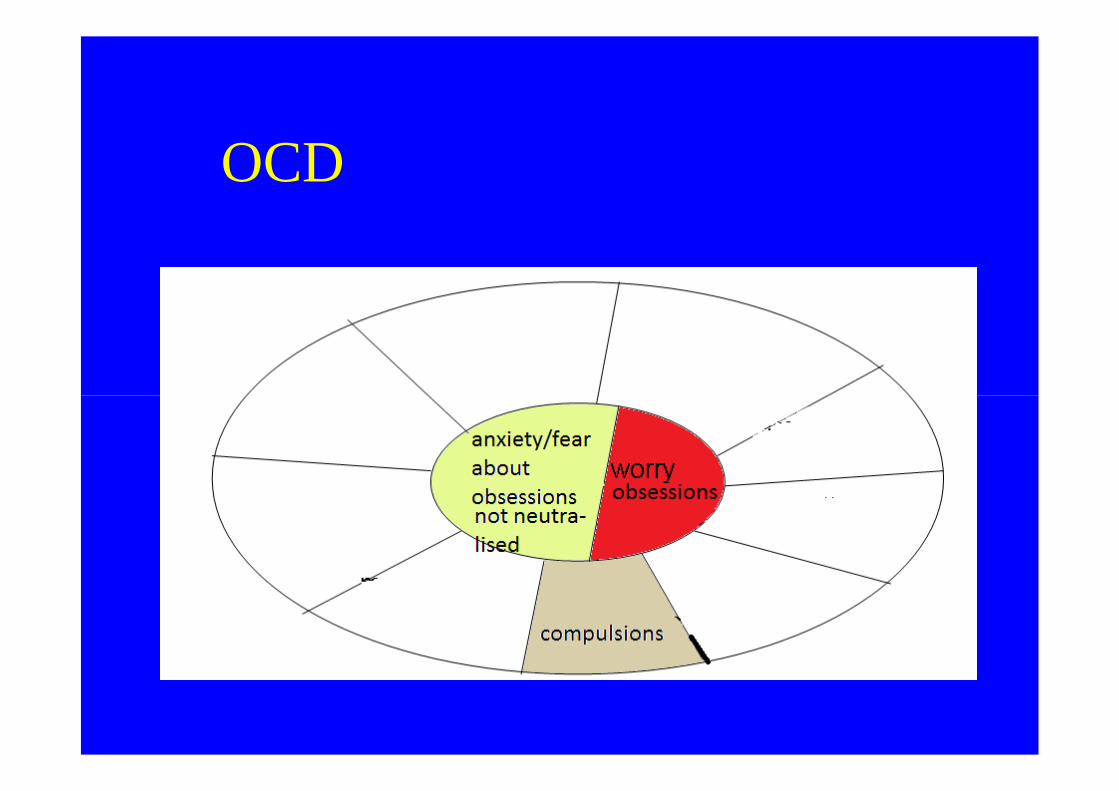
OCD
Groups of anxiety symptoms
a) Psychological arousal
b) Autonomic overactivity
c) Muscle tensionc) Muscle tension
d) Hyperventilation
e) Sleep disturbances
f) Other features
a. Psychological arousal
• Fearful anticipation
• Irritability
• Sensitivity to noise• Sensitivity to noise
• Restlessness
• Poor concentration
• Worrying thoughts
=>Fear of losing control, going crazy or passing out
=>Fear of dying
b. Autonomic arousal
GI:
• Dry mouth
• Difficulty swallowing• Difficulty swallowing
• Epigastric discomfort
• Excessive wind
• Frequent or loose motions
b. Autonomic arousal (cont)
Respiratory
• Sense of constriction in the chest
• Difficulty inhaling• Difficulty inhaling
CV
• Palpitations
• Discomfort in the chest
• Awareness of missed heartbeats
b. Autonomic arousal (cont)
Genitourinary
• Frequent urge to pass urine
• Failure of erection• Failure of erection
• Menstrual discomfort
• Amenorrhoea
Other
Sweating
Cold extremities
c. Muscle tension
• Tremor
• Headache
• Aching muscles (usually shoulders and back)• Aching muscles (usually shoulders and back)
• Inability to relax
d. Hyperventilation
• Dizziness
• Tingling sensation
• Feeling of breathlessness
Sleep disturbance
• Insomnia (initial most common)
• Nightmares and Night terrors• Nightmares and Night terrors
Sweating
Cold extremities
Derealisation, depersonalisation
Generalised anxietydisorderdisorder
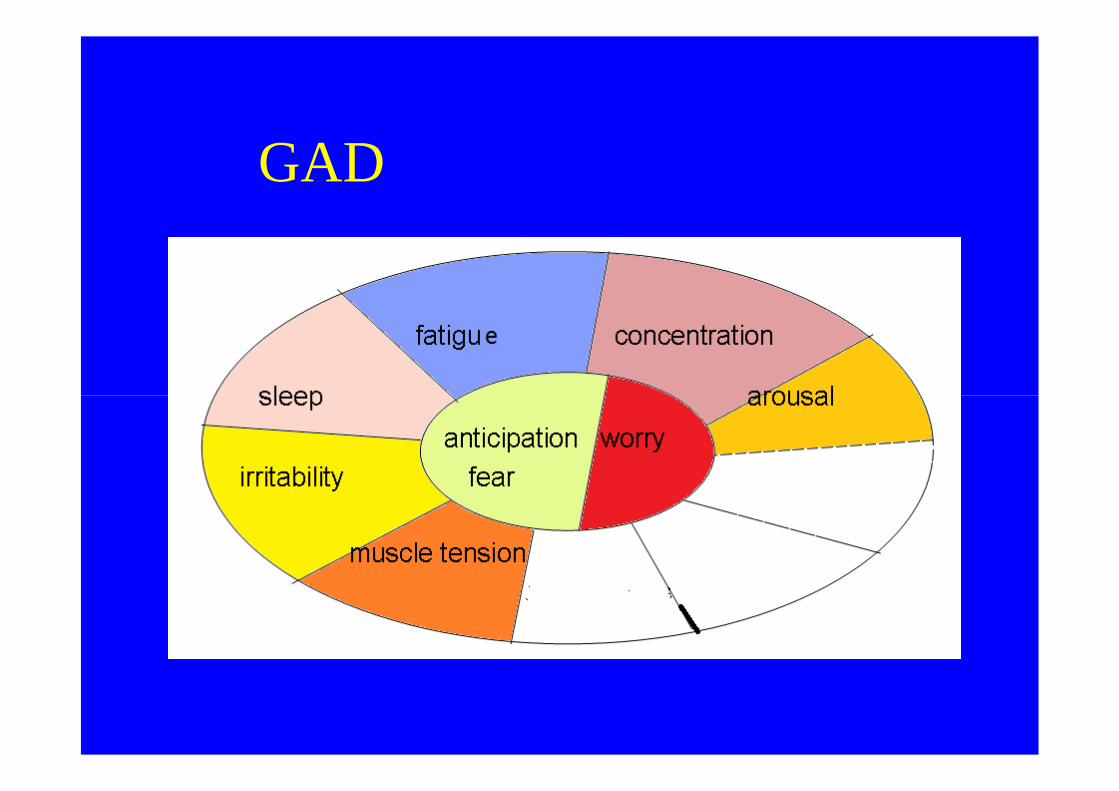
GAD
Generalised anxiety disorder
• Anxiety is generalized and persistent but notrestricted to or even strongly predominant in anyparticular situation (free floating).
• Variable but persistent nervousness and• Variable but persistent nervousness andsometimes fears that patient will become ill orhave an accident
• NB symptoms different in children: autonomicarousal often less prominent
Generalised anxiety disorderEpidemiology
• Variable 2.4-6.6%
• Risk factors
• females, people under 30• females, people under 30
• Genetic basis 41% monozygotic twins vs4% dizygotic
Generalised anxiety disorderdiagnosis
• For at least 6 months prominent tension, worryand feelings of apprehension about everydayevents and problems
• at least four symptoms of anxiety - one must be• at least four symptoms of anxiety - one must beautonomic arousal but the list of others isexpanded
• Disorder does not meet criteria for panic disorder/phobic anxiety disorder/ OCD/ hypochondriacal
disorder
DD
• Onset of scz or dementia
• Substance abuse to self medicate
• Endocrinological illness: thyrotoxicosis,• Endocrinological illness: thyrotoxicosis,phaeochromocytoma, hypoglycemia, orsecondary to physical illness
• Major stresses, eg life at risk (drug trade)
• Physical illness
Generalised anxiety disorderdiagnosis
Exclusion clauses:
• Not due to physical illness
• organic mental illness• organic mental illness
• substance misuse or withdrawal
Generalised anxiety disorderHelping patients understand
– Stress or worry have many physical and mentaleffects, and may be responsible for many oftheir symptoms.
– Symptoms are likely to be at their worst at– Symptoms are likely to be at their worst attimes of personal stress.
– Aim to help the patient to reduce his or hersymptoms.
– These problems are not due to weakness orlaziness: patients are trying to cope.
– Regular structured visits can be helpful.

Treatment-relaxation groups
Generalised anxiety disorderTreatment
– Explain to patients
– If tension-related symptoms: relaxation methods to relieve physicalsymptoms.
– Reduction in caffeine intake and a balanced diet– Reduction in caffeine intake and a balanced diet
– problem-solving
– Supportive psychotherapy
– Encourage self-help books, tapes and/or leaflets
– Discuss ways to challenge negative thoughts or exaggeratedworries => CBT
Generalised anxiety disorderMedication
• Second-line treatment• Significant anxiety or persistence despite other
measuresImmediate-short termImmediate-short term• Benzodiazepines medication may be used for no
longer than two-three weeks.• Avoid short-acting benzodiazepines except for
sleep• Beta-blockers:helpful for peripheral autonomic
symptoms such as tremor, palpitations.
GAD-medication
Long term
• Antidepressant drugs: SSRIs, venlafaxine,imipramine, clomipramine, may be helpful.imipramine, clomipramine, may be helpful.
• Buspirone
• Alpha2-δ ligands-voltage-gated calcium channels: Gabapentine, Pregabaline
Panic disorder
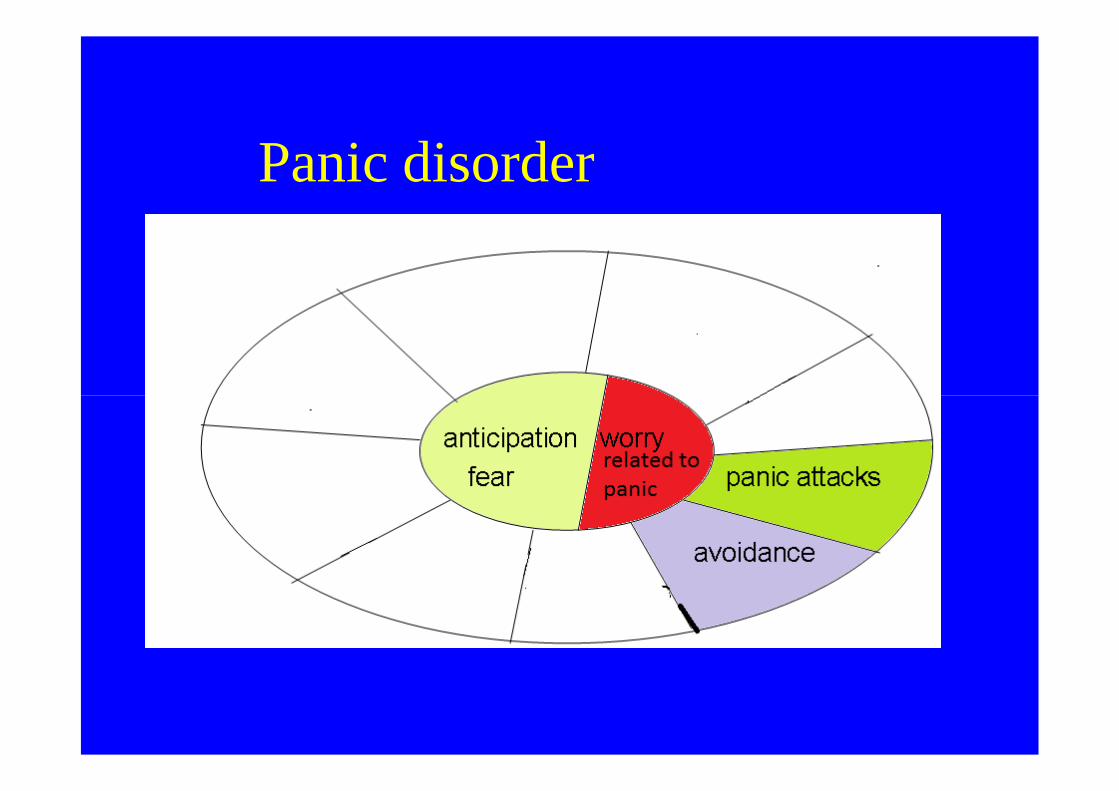
Panic disorder
Panic disorder
• Recurrent attacks of severe anxiety notrestricted to any particular situation.
• They are therefore unpredictable• They are therefore unpredictable
• Symptoms of anxiety
• Do not diagnose panic disorder ifdepression is present when they start.
Panic Disorder Epidemiology
• Rates vary 0.13 rural Taiwan - 2.2% newZealand
• Higher rates in women• Higher rates in women
• lowest rates in older people but patternsdiffer in different countries
Panic Attack
= all of the following
– Discrete episode of intense fear or discomfort
– starts abruptly– starts abruptly
– reaches a maximum within a few minutes andlasts some minutes
– at least four symptoms of anxiety - one must bea symptom of autonomic arousal
Panic Disorder Diagnosis
Exclusion clause:
• Not secondary to physical illness or othermental illnessmental illness
• Moderate - four panic attacks in a month
• Severe - four panic attacks a week for amonth
Panic DisorderDifferential Diagnosis
• Physical illness
• Prescribed drugs• Prescribed drugs
• Depression
• Phobia
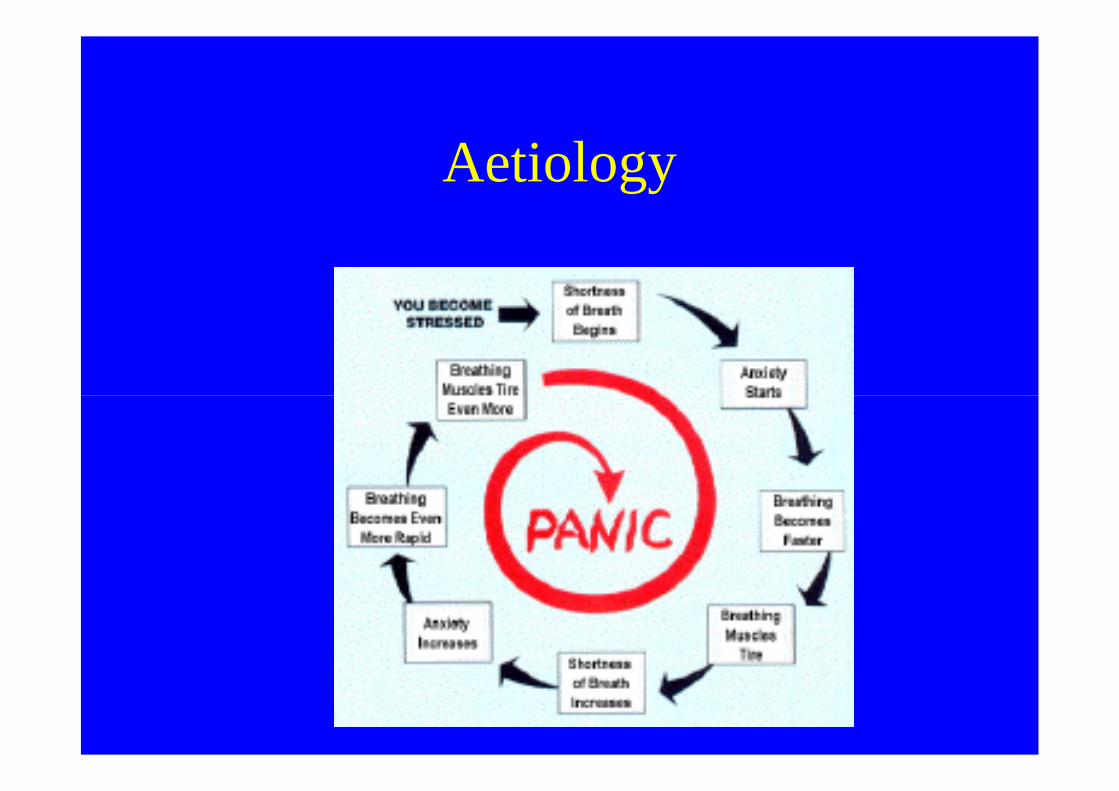
Aetiology
Panic Disorder Treatment
• Explain to the patient
– treatable
– Catastrophic misinterpretation of normal– Catastrophic misinterpretation of normalsensations is the key
– mental and physical symptoms reinforce eachother
– Safety behaviours consolidate thoughts
Panic DisorderTreatment
• CBT: thoughts, experiments, stoppingsafety behaviours
Panic Disorder Treatment
• Do not move out of situation
• Do not use alcohol
• Do monitor caffeine intake• Do monitor caffeine intake
• Do read self help books
Panic DisorderTreatment : Medication
• Consider SSRI if initial CBT fails
• Note that symptoms can become worse• Note that symptoms can become worsebefore they become better
• Avoid benzodiazepines

Phobic anxiety disorders
Phobic anxiety disorders
• Agoraphobia
• Social phobia• Social phobia
• Specific phobias
Phobic anxiety disorders-general
• Patients avoid or restrict activities because of fear of specific objects-situations=>anticipatory anxiety develops
• If severe, social implications.• If severe, social implications.
• Sometimes physical symptoms (eg palpitations, shortness of breath or‘asthma’). Questioning will reveal specific fears.
• Focus moves to individual symptoms/secondary fears(dying, losing control or going mad)
agoraphobia
Agoraphobia
• Phobias related to distance fromhome, crowding and confinement.
• Anxious thoughts about fainting andlosing controllosing control
• Panic frequently present
• Avoidance is prominent
• Little anxiety if the patient completelyavoids situation
Agoraphobia Epidemiology
• Female>male
• Starts early-middle twenties, another peakin mid thirties-(18-35)in mid thirties-(18-35)
• Rates vary
– 2-4% year prevalence
– 6-10% life prevalence
Agoraphobia Epidemiology
• increased life events prior to onset
Agoraphobia Diagnosis
• Presentation: after panic attack, orduring exploration of symptoms ofanxiety
• Fear in or avoidance of at least 2 of• Fear in or avoidance of at least 2 of– crowds, / public places, / travelling
alone, / travelling away from home
• At least two symptoms of anxiety(one must be of autonomic arousal)
• Most likely starts with a panic attack
• Prognosis
course is fluctuating, if lasts 1 yr thenunchanged at 5 yrs without treatmentunchanged at 5 yrs without treatment
Social phobia
Social Anxiety Disorder
Social Phobia• Fear of scrutiny of others => avoidance of
social situations
• low self esteem and fear of criticism
• May present as blushing, and tremor,urgency of micturition - patient maypresent these secondary symptoms as theirprimary problem.
• May develop panic attacks
Social Phobia Epidemiology
• Low in rural Taiwan 0.4% high in NewZealand 3.9%
• Risk factors highest rates in those who are18-29, less educated, single and lowersocio-economic class
Social Phobia Epidemiologyand DD
* onset usually gradual from late puberty (17-30).
* gender males = females
* overlap with social dysfunction (social skillsdeficit, avoidant personality disorder). Socialdeficit, avoidant personality disorder). Socialphobia limited to specific situations, whereasin social dysfunction there is a more generalsocial skills deficit
Social Phobia Diagnosis
• At least two symptoms of anxiety arepresent in the feared situation, they musthave been present since the onset of thehave been present since the onset of theproblem and occur with at least one of
– blushing or shaking
– fear of vomiting
– urgency and fear of micturition or defecation
• Depression
• Alcoholism
• Increased distress-may be undetected for• Increased distress-may be undetected fordecades
Specific phobias
Specific phobias
• Phobias restricted to highly specificsituations
– animal type - insects, dogs
– natural forces - eg storms and water
– blood, injections, injury type
– situational elevators, tunnels
– other
Specific phobias Epidemiology
• Common – 7-15%
• Often start in childhood(aged 2-4)(aged 2-4)

Specific Phobias Diagnosis
• Must be present
– marked fear of a specific object or situation notincluded in agoraphobia or social phobiaincluded in agoraphobia or social phobia
– marked avoidance of the object/ situation
Specific Phobias Diagnosis
1. Symptoms of anxiety in feared situation
2. Significant emotional distress caused bythe symptoms or the avoidancethe symptoms or the avoidance
3. Symptoms restricted to feared situations
4. Individual recognizes that these areexcessive or unreasonable
Differential diagnoses andtreatmenttreatment
Phobic anxiety disordersDifferential diagnoses
• Depression
• Panic disorder• Panic disorder
• Organic illness
• Secondary to other mental illness such as apsychotic illness
Phobic anxiety disordersEssential information for patient
• phobias can be treated
• avoidance makes fears grow• avoidance makes fears grow
• following simple steps can diminish fear
• TOPs groups and “Living with Fear” workfor most people
Phobic anxiety disordersTreatment
• Most people do well with CBT and do not needmeds
• Alcohol=>no good solution
• Antidepressants: if depression or persistent givenif depression present
• Social phobia may be helped by SSRIs, MAOIs
• B-blockers decrease physical symptoms inperformance anxiety
Obsessive compulsivedisorderdisorder
OCD
Obsessive compulsive disorder
• Recurrent obsessional thoughts and/orcompulsive acts.
• Obsessional thoughts• Obsessional thoughts
– ideas, images or impulses
– enter patient’s mind again and again
– usually distressing
– patient often tries to resist them
– recognized as own thoughts
Obsessive compulsive disorder
• Compulsion
– stereotyped behaviours
– repeated again and again– repeated again and again
– not inherently enjoyable or useful
– function to prevent some objectively unlikelyevent (harm to or by patient)
– usually recognized as pointless
– patient attempts to resist
– resistance causes anxiety
Obsessive compulsive disorder
• Obsession/ compulsion most days for 2 wks
Obsessive compulsive disorder
• Distress or interference with the patient’sfunctioning e.g. wasting excessive amountif timeif time
• Most common exclusion cause is symptomsdue to other psychiatric illness egdepression, SCZ
Obsessive compulsive disorderPsychiatric clinic population
• Obsessions and compulsions 69%
• Obsessions only 25%
• Compulsions only 6%• Compulsions only 6%
Obsessive compulsive disorderTypes of rituals
• · Cleaning 51%
• · Repeating 40%• · Repeating 40%
• · Checking 38%
• · Orderliness 9%
Obsessive compulsive disorder
• Prevalence
• Epidemiologic Catchment Area study in• Epidemiologic Catchment Area study inUSA (sample size 18,500): one monthprevalence rate 1.3% m=f
Obsessive compulsive disorderepidemiology
• Onset usually insidious in early 20s (malesearlier than females but equal incidence),with excess of life events in year prior towith excess of life events in year prior toonset.
• Fewer are married, those seeking treatmenthave slightly raised intelligence and socialclass 92% 10-40 years. Mean age 22.Mean age at presentation 34.
Obsessive compulsive disorder
• OC symptoms also in depression (20%-25%), in schizophrenia and dementia.
• 12% past history of anorexia• 12% past history of anorexia
• Gilles de la Tourette syndrome,parkinsonism, encephalitis lethargica, headtrauma and basal ganglia lesions.
Treatment
• CBT: challenging compulsions, belief incatastrophe, relapse prevention
• Serotoninergic antidepressants
• Atypical antipsychotic augmentation
• Psychosurgery(!) in extreme cases!
Mixed anxiety and depression
Mixed anxiety and depressivedisorder
• Symptoms of anxiety and depression areboth present
• Neither is clear predominant and neithertype of symptoms justifies a separate
• Neither is clear predominant and neithertype of symptoms justifies a separatediagnosis
• if both depression and anxiety are severeenough to satisfy individual criteria thendiagnose both
Mixed anxiety and depression
– Patient may present with one or morephysical symptoms (eg various pains,poor sleep and fatigue), accompanied bya variety of anxiety and depressivea variety of anxiety and depressivesymptoms,
– present for more than six months. Thesepatients may be well known to theirdoctors, and have often been treated by avariety of psychotropic agents over theyears.
Mixed anxiety and depression
• Treatment use methods above for treatmentof anxiety Medication
– simplify medication use as little as possible– simplify medication use as little as possible
– only continue or start antidepressant if it isshown to work in individual
– SSRIs, tricyclics, MAOI
Overview of medication for anxietysymptoms-disorders
Medication
• Antidepressants
• Beta-blockers
• A-δ ligands (pragabaline-gabapentin)• A-δ ligands (pragabaline-gabapentin)
• Benzodiazepines
• Buspirone
• Antihistamines
• Sleeping tablets
• Antipsychotics (small doses)
• Mainly serotonergic for OCD, panic
• Both noradrenergic and serotonergic forGAD, anxiety and depressionGAD, anxiety and depression
• Β-blockers for peripheral symptoms of autonomic arousal
Diagnostic rubric
Diagnosing anxiety disorders
• Anxiety
– A. Feeling tense or anxious?
– B. Worrying a lot about things?
Diagnosing anxiety disorders
1.Symptoms of arousal and anxiety?
Diagnosing anxiety disorders
2. Experienced intense or sudden fear unexpectedlyor for no apparent reason?
Fear of dying Fear of losing control
Pounding heart SweatingPounding heart Sweating
Trembling/shaking Nausea
Chest pains/ breathing difficulty
Feeling dizzy / lightheaded or faint
Numbness/ tingling sensations
Feelings of unreality
Diagnosing anxiety disorders
3.Experiences fear/anxiety when:
• leaving familiar places
• travelling alone, eg train, car, plane• travelling alone, eg train, car, plane
• crowds confined places/public places
Diagnosing anxiety disorders
4. Experienced fear/anxiety when
speaking in front of others
• social events• social events
• eating in front of others
• worry a lot about what others think or self-conscious?
Diagnosing anxiety disorders
• Summing up
• Positive to A, B and 1, recurring regularly,negative to 2, 3 and 4 Indication of Generalizedanxietyanxiety
• Positive to 1 and 2: indication of panic disorder
• Positive to 2 and 3: indication of agoraphobia
• Positive to 3 and 4: indication of social phobia
Cases
Case 1CASE VIGNETTE 1Francis is a M.W.M. and presents with extraordinary concern about the safety of his wifeand young daughter. He rarely leaves them alone when away (e.g., at work) hetelephones home every hour. He has lost one job because of this, and his wife hasthreatened to leave him if he does not seek psychiatric help. Six months ago, thesymptoms, which have been present for years, became worse after his wife had a seriousautomobile accident.
Francis describes recurrent, unbidden thoughts in which dangerous events befall hisfamily and he is not there to save them. He knows the thoughts are “silly” and they comefamily and he is not there to save them. He knows the thoughts are “silly” and they comefrom his own mind rather than any real danger, but he cannot resist contacting his wife ordaughter in some way to be certain they are safe. His wife has arranged to lift thetelephone receiver briefly, then hang up, which is usually sufficient to allay his fears foran hour or so.
There is no history of significant medical illness or Substance Abuse. The clientcompleted 2 years of college and has a responsible job. He performs well, and is notparticularly perfectionistic, overly conscientious (except with regard to his family’ssafety), rigid, or preoccupied with details.
• OCD
Case 2• George, 21 yo male. Lives with parents. Self employed as sound and studio
specialist.
• Presents with intense and recurrent worries about the possibility of vomiting.He was last sick more than 7 years ago when ill from a tummy virus, however,he avoids all meat except chicken, and other food like fish, eggs and anythingunhealthy, for fear of vomiting. He also avoids getting close to people whohave any virus, to avoid a tummy bug. Occasionally he becomes so caught upin his worry and rumination that he has panic attacks.in his worry and rumination that he has panic attacks.
• When he was 8 a classmate vomited all over him, which made him feelhumiliated in class. At the age of 14 he had a tummy virus and since then hisfear of being sick has been with him continually. Its intensity fluctuates.Became much worse since a trip to Spain two years ago. He does not tend toworry about anything else.
• He doesn’t drink alcohol, and smokes 2-3 joints of cannabis a week, which“relaxes his thoughts”. No other medical history
• Emetophobia
Helen is a 35 year old M.B.F. who for the past 6 months, has had increasing anxiety andoccasional panic attacks. Although the anxiety and panic were initially not associatedwith any particular situation they are now associated with her work as a personneldirector for a large corporation. When she goes to work she often (sometimes more thanonce a week) has sudden attacks of nausea, perspiring, a feeling of unreality andimpending doom, and trembling. These symptoms become quite intense within a fewminutes and last less than half an hour. Helen dreads the episodes, which are souncomfortable that she occasionally prevents them by staying home rather than going tothe office.
She has noticed that the episodes, which initially came randomly and unexpectedly, haverecently become more specifically associated with certain responsibilities, such as boardmeetings and presentations to her superiors. Helen denies any discomfort from themeetings and presentations themselves, saying that she enjoys her position, handles itwell, and feels very comfortable as a member of the management team. She is notaffected in ordinary social situations or while working with people in other settings. Theclient has never had other psychiatric symptoms, enjoys a normal family life, and is ingood health. She takes no medications, has a low caffeine intake, and denies drug oralcohol abuse. Physical examination, with thyroid tests and echocardiogram, is normal.
• Panic disorder
Case 1
• 30 yrs male
• Mother dead - withdrawal from social life
• Not going out alone• Not going out alone
• Tense in social situations, fears scrutiny
• Continually on edge – panic attacks
• Drinking
• Now depressed
Case 2
• 35
• Worried that her sweat smelled terrible
• Ideas of reference• Ideas of reference
• Avoidance of social situations because shethinks she smells
• Believed neighbours talking about her
• Baths and changes clothes 4 times a day
Case 3
• 30
• Fear he might abuse or kill his 8 yr old daughter
• Resists but cannot stop thoughts• Resists but cannot stop thoughts
• Reassurance does not help
• Avoids being left alone with her
• Depressed – quit his job
• Asks to be in a locked ward
Case 4
• 30 yr old woman
• Poor sleep, can’t concentrate, restless
• Changed jobs, separated from husband• Changed jobs, separated from husband
• Raped
• Poor sleep and nightmares about the event
• Hyper-vigilant
• Increased startle, misidentification, suicidal
Case 5
• 45 years old
• Intense bouts of anxiety andhyperventilation lastinghyperventilation lasting
• Avoidance of supermarkets and theatres
• Carrying mobile phone for help
• Wanted to be accompanied where she went
References
• Gelder, Harrison, Cowen Shorter Oxford Textbookof Psychiatry, 5th edition
• Gelder, Andreasen, Lopez-Ibor, Geddes
• New Oxford textbook of Psychiatry 2nd ed 2009
• Apu Chakraborty: notes from lecture on anxietydisorders 2006
Thank you
end
Related Documents