Vascular disrupting action of electroporation and electrochemotherapy with bleomycin in murine sarcoma G Sersa * ,1 , T Jarm 2 , T Kotnik 2 , A Coer 3 , M Podkrajsek 1 , M Sentjurc 4 , D Miklavcic 2 , M Kadivec 1 , S Kranjc 1 , A Secerov 1 and M Cemazar 1 1 Institute of Oncology Ljubljana, Zaloska 2, SI-1000 Ljubljana, Slovenia; 2 Faculty of Electrical Engineering, University of Ljubljana, Trzaska 25, SI-1000 Ljubljana, Slovenia; 3 Faculty of Medicine, University of Ljubljana, Korytkova 2, SI-1000 Ljubljana, Slovenia; 4 Institute Jozef Stefan, Jamova 39, SI-1000 Ljubljana, Slovenia Electrochemotherapy has a direct cytotoxic effect on tumour cells, and presumably, a vascular disrupting effect. In this study, on the basis of the prediction of the mathematical model, histological evaluation and physiological measurements of the tumours were carried out to confirm that electroporation and electrochemotherapy of tumours have a vascular disrupting action. In the study, SA-1 solid subcutaneous sarcoma tumours in A/J mice were treated by bleomycin (BLM) given intravenously (1 mg kg 1 ), application of electric pulses (8 pulses, 1040 V, 100 ms, 1 Hz) or a combination of both – electrochemotherapy. The vascular effect was determined by laser Doppler flowmetry, power Doppler ultrasonographic imaging and Patent blue staining. The extent of tumour hypoxia was determined immunohistochemically by hypoxia marker pimonidazole and partial pressure of oxygen (pO 2 ) in tumours by electron paramagnetic resonance oximetry. Electrochemotherapy with BLM induced good antitumour effect with 22 days, tumour growth delay and 38% tumour cures. The application of electric pulses to the tumours induced instant but transient tumour blood flow reduction (for 70%) that was recovered in 24 h. During this tumour blood flow reduction, we determined an increase in hypoxic tumour area for up to 30%, which was also reflected in reduced tumour oxygenation (for 70%). According to the described mathematical model, endothelial cells lining in tumour blood vessels are exposed to a B40% higher electric field than the surrounding tumour cells, and therefore easily electroporated, allowing access of high BLM concentration to the cytosol. Consequently, electrochemotherapy has, besides the immediate vascular disrupting action, also a delayed one (after 24 h), as a consequence of endothelial cell swelling and apoptosis demonstrated by extensive tumour necrosis, tumour hypoxia, prolonged reduction of tumour blood flow and significant tumour growth delay, and tumour cures. Our results demonstrate that in addition to the well-established direct cytotoxic effect on tumour cells, electrochemotherapy also has an indirect vascular disrupting action resulting altogether in extensive tumour cell necrosis leading to complete regression of tumours. British Journal of Cancer (2008) 98, 388 – 398. doi:10.1038/sj.bjc.6604168 www.bjcancer.com Published online 8 January 2008 & 2008 Cancer Research UK Keywords: vascular disruption; electrochemotherapy; electroporation; bleomycin In vivo electroporation has found its place as a drug delivery system for chemotherapeutics, that is electrochemotherapy, and is currently under intensive investigation for delivery of therapeutic genes to normal tissues and tumours, that is gene electrotransfer (Neumann et al, 1982; Cemazar et al, 2006; Heller and Heller, 2006; Mir, 2006). Bleomycin (BLM) and cisplatin proved to be effective in electrochemotherapy for treatment of various tumours in mice, rats, cats, dogs and horses (Sersa et al, 2006b). In a clinical setting, several studies predominantly on patients with malignant mela- noma, basal cell carcinoma, head and neck tumours, and others have proved antitumour effectiveness of electrochemotherapy by long-lasting local tumour control (Heller et al, 1999; Marty et al, 2006; Sersa, 2006a). The predominant underlying mechanism of electrochemo- therapy is electroporation of cells in the tissues, which facilitates access of poorly permeant and nonpermeant molecules, including cytotoxic drugs such as BLM and cisplatin, into the cells (Mir, 2006). In addition to electroporation of tumour cells, electric pulses were found to modify blood flow in normal tissues and in tumours (Ramirez et al, 1998; Sersa et al, 1998, 1999b; Engstrom et al, 2001; Gehl et al, 2002). This phenomenon was well documented by different techniques demonstrating reduced blood flow and oxygenation in the tumours (Sersa et al, 1999b, 2002). In addition, we demonstrated that electroporation of adherent endothelial monolayer induced disruption of actin filaments and microtubule network cytoskeleton as well as loss of cell – cell contact junctions, which altogether increased endothelial mono- layer permeability (Kanthou et al, 2006). This suggests that in addition to the direct effect of electric pulses applied to the tumour, there may also be an indirect effect on tumour via the effect of electric pulses on tumour blood vessels (vascular Revised 26 November 2007; accepted 27 November 2007; published online 8 January 2008 *Correspondence: Professor G Sersa; E-mail: [email protected] British Journal of Cancer (2008) 98, 388 – 398 & 2008 Cancer Research UK All rights reserved 0007 – 0920/08 $30.00 www.bjcancer.com Translational Therapeutics

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Vascular disrupting action of electroporation andelectrochemotherapy with bleomycin in murine sarcoma
G Sersa*,1, T Jarm2, T Kotnik2, A Coer3, M Podkrajsek1, M Sentjurc4, D Miklavcic2, M Kadivec1, S Kranjc1,A Secerov1 and M Cemazar1
1Institute of Oncology Ljubljana, Zaloska 2, SI-1000 Ljubljana, Slovenia; 2Faculty of Electrical Engineering, University of Ljubljana, Trzaska 25, SI-1000Ljubljana, Slovenia; 3Faculty of Medicine, University of Ljubljana, Korytkova 2, SI-1000 Ljubljana, Slovenia; 4Institute Jozef Stefan, Jamova 39, SI-1000Ljubljana, Slovenia
Electrochemotherapy has a direct cytotoxic effect on tumour cells, and presumably, a vascular disrupting effect. In this study, on thebasis of the prediction of the mathematical model, histological evaluation and physiological measurements of the tumours werecarried out to confirm that electroporation and electrochemotherapy of tumours have a vascular disrupting action. In the study, SA-1solid subcutaneous sarcoma tumours in A/J mice were treated by bleomycin (BLM) given intravenously (1 mg kg�1), application ofelectric pulses (8 pulses, 1040 V, 100ms, 1 Hz) or a combination of both – electrochemotherapy. The vascular effect was determinedby laser Doppler flowmetry, power Doppler ultrasonographic imaging and Patent blue staining. The extent of tumour hypoxia wasdetermined immunohistochemically by hypoxia marker pimonidazole and partial pressure of oxygen (pO2) in tumours by electronparamagnetic resonance oximetry. Electrochemotherapy with BLM induced good antitumour effect with 22 days, tumour growthdelay and 38% tumour cures. The application of electric pulses to the tumours induced instant but transient tumour blood flowreduction (for 70%) that was recovered in 24 h. During this tumour blood flow reduction, we determined an increase in hypoxictumour area for up to 30%, which was also reflected in reduced tumour oxygenation (for 70%). According to the describedmathematical model, endothelial cells lining in tumour blood vessels are exposed to a B40% higher electric field than the surroundingtumour cells, and therefore easily electroporated, allowing access of high BLM concentration to the cytosol. Consequently,electrochemotherapy has, besides the immediate vascular disrupting action, also a delayed one (after 24 h), as a consequence ofendothelial cell swelling and apoptosis demonstrated by extensive tumour necrosis, tumour hypoxia, prolonged reduction of tumourblood flow and significant tumour growth delay, and tumour cures. Our results demonstrate that in addition to the well-establisheddirect cytotoxic effect on tumour cells, electrochemotherapy also has an indirect vascular disrupting action resulting altogether inextensive tumour cell necrosis leading to complete regression of tumours.British Journal of Cancer (2008) 98, 388–398. doi:10.1038/sj.bjc.6604168 www.bjcancer.comPublished online 8 January 2008& 2008 Cancer Research UK
Keywords: vascular disruption; electrochemotherapy; electroporation; bleomycin
����������������������������������������������������������������
In vivo electroporation has found its place as a drug deliverysystem for chemotherapeutics, that is electrochemotherapy, and iscurrently under intensive investigation for delivery of therapeuticgenes to normal tissues and tumours, that is gene electrotransfer(Neumann et al, 1982; Cemazar et al, 2006; Heller and Heller, 2006;Mir, 2006). Bleomycin (BLM) and cisplatin proved to be effectivein electrochemotherapy for treatment of various tumours in mice,rats, cats, dogs and horses (Sersa et al, 2006b). In a clinical setting,several studies predominantly on patients with malignant mela-noma, basal cell carcinoma, head and neck tumours, and othershave proved antitumour effectiveness of electrochemotherapy bylong-lasting local tumour control (Heller et al, 1999; Marty et al,2006; Sersa, 2006a).
The predominant underlying mechanism of electrochemo-therapy is electroporation of cells in the tissues, which facilitatesaccess of poorly permeant and nonpermeant molecules, includingcytotoxic drugs such as BLM and cisplatin, into the cells (Mir,2006). In addition to electroporation of tumour cells, electricpulses were found to modify blood flow in normal tissues and intumours (Ramirez et al, 1998; Sersa et al, 1998, 1999b; Engstromet al, 2001; Gehl et al, 2002). This phenomenon was welldocumented by different techniques demonstrating reduced bloodflow and oxygenation in the tumours (Sersa et al, 1999b, 2002). Inaddition, we demonstrated that electroporation of adherentendothelial monolayer induced disruption of actin filaments andmicrotubule network cytoskeleton as well as loss of cell–cellcontact junctions, which altogether increased endothelial mono-layer permeability (Kanthou et al, 2006). This suggests that inaddition to the direct effect of electric pulses applied to thetumour, there may also be an indirect effect on tumour via theeffect of electric pulses on tumour blood vessels (vascular
Revised 26 November 2007; accepted 27 November 2007; publishedonline 8 January 2008
*Correspondence: Professor G Sersa; E-mail: [email protected]
British Journal of Cancer (2008) 98, 388 – 398
& 2008 Cancer Research UK All rights reserved 0007 – 0920/08 $30.00
www.bjcancer.com
Tra
nsla
tion
al
Th
era
peu
tics

disrupting effect). Furthermore, we have previously demonstratedthat electrochemotherapy with either BLM or cisplatin also has atumour blood flow modifying effect (Sersa et al, 1999a, 2002). Inaddition, we showed that cultured endothelial cells are verysusceptible to electrochemotherapy with BLM and to the sameextent as tumour cells in the case of electrochemotherapy withcisplatin (Cemazar et al, 2001). Therefore, by electroporation ofendothelial cells in tumour blood vessels, these may also becomesusceptible to chemotherapeutics, leading to endothelial cell death,vessel occlusion and abrogated tumour blood flow, thus inducing acascade of cell death in the surroundings of the occluded bloodvessel. If so, then electrochemotherapy is also currently a memberof the intensively investigated vascular disrupting therapies thatcause a rapid and selective shutdown of established tumourvasculature and can lead to secondary tumour cell death (Tozeret al, 2001, 2005; Siemann et al, 2005).
In this study, we present a mathematical model of electric fielddistribution in tumour blood vessels, predicting vascular disrup-ting action of electrochemotherapy. The prediction of the model issupported by the data demonstrating reduced tumour blood flowafter electroporation and electrochemotherapy with BLM as wellas pronounced tumour hypoxia, reduced tumour oxygenation,endothelial cells swelling and apoptosis, and extensive tumour cellnecrosis. The study demonstrates that in addition to the directeffect on tumour cells, electrochemotherapy also has a vasculardisrupting effect.
MATERIALS AND METHODS
Mice and tumours
Murine fibrosarcoma SA-1 (The Jackson Laboratory, Bar Harbor,ME, USA) cells were used in the experiments. A/J mice of bothsexes, purchased from the Institute of Pathology, Faculty ofMedicine, University of Ljubljana, Slovenia, were used for thisstudy. They were kept at a constant room temperature (221C) witha natural day/night light cycle in a conventional animal colonywith food and water ad libitum. Before the experiments, the micewere subjected to an adaptation period of at least 10 days. Themice were 10–14 weeks old at the beginning of the experiments,weighing 20–25 g.
Tumour cells were obtained from the ascitic form of thetumours in mice. Solid subcutaneous tumours, located dorso-laterally in mice, were initiated by an injection of 5� 105 SA-1 cellsin 0.1 ml 0.9% NaCl solution. Six to 8 days after implantation,when tumours reached approximately 40 mm3 in volume, the micewere randomly divided into experimental groups. The study wasapproved by the Ministry of Agriculture, Forestry and Food of theRepublic of Slovenia (No. 323-02-237/01) in compliance with theGuide for the Care and Use of Laboratory Animals (NationalInstitutes of Health, Bethesda, MD, USA).
Electrochemotherapy
Bleomycin (Heinrich Mack Nachf., Illertissen, Germany) at a doseof 1 mg kg�1 (B20 mg per mouse) was injected intravenously.Injection volume was 7.5 ml per kg body weight. Eight square waveelectric pulses in two sets of four pulses, in two mutuallyperpendicular directions of 1040 V (at voltage to distance ratio1300 V cm�1) and with a pulse duration of 100 ms and repetitionfrequency of 1 Hz, were delivered by two flat, parallel stainless-steel electrodes 8 mm apart (two stainless-steel strips: length15 mm, width 7 mm, with rounded corners), which were placedpercutaneously at the opposite margins of the tumour. Goodcontact between the electrodes and the skin was assured by meansof a conductive gel. Electric pulses were generated by a JouanGHT 1287 electroporator (Jouan, Saint Herblain, France). In the
electrochemotherapy protocol, the mice were treated with electricpulses 3 min after BLM injection. All treatments except in the caseof electron paramagnetic resonance (EPR) oximetry, laser Dopplermeasurements and power Doppler ultrasonographic imaging (seebelow), were performed without anaesthesia and were welltolerated by the animals.
Tumour growth was followed by measuring three mutuallyorthogonal tumour diameters (e1, e2 and e3) with a Vernier calliperthree times per week. Tumour volumes were calculated accordingto the formula for the volume of an ellipsoid, V¼ pe1e2e3� 6�1.The AM (arithmetic mean) of tumour volumes and s.e. werecalculated for each experimental group. Tumour doubling timewas determined for each individual tumour from the growthcurves. Tumour growth delay was calculated for each individualtumour by subtracting the doubling time of each tumour from themean doubling time of the control group and then averaged foreach experimental group. Animals that were tumour free for 100days were declared cured.
Histology
At different time points after treatment with BLM, the applicationof electric pulses and electrochemotherapy of tumour’s morpho-logical changes, extent of tumour necrosis and the area withhypoxia marker pimonidazole adduct staining were determined.Tumour cell and blood vessels morphology as well as the extent oftumour necrosis were estimated on haematoxylin and eosin-stained slides. For necrotic tumour area analysis, the slides of threetumours per group were examined by two co-authors blinded totherapy status. The area of tumour necrosis was determined in awhole mount tumour section through the largest tumour diameterand expressed as a percentage of necrosis in relation to the wholetumour cross-section area. If the difference between two observerswere greater than 10%, a consensus was achieved.
The hypoxia marker pimonidazole (Hypoxyprobet-1, NaturalPharmacia International Inc., Belmont, MA, USA) (60 mg kg�1 in0.2 ml PBS) was injected intraperitoneally. Tumours (3– 9 pergroup) were excised 90 min thereafter, fixed in 10% bufferedneutral formalin, embedded in paraffin, cut at three different levelsthroughout the tumour and stained for pimonidazole according tothe manufacturer’s instructions. Briefly, the sections were depar-affinised with xylene and rehydrated in ethanol. Sections wereexposed to 3% H2O2 in methanol for 5 min to quench endogenousperoxidase activity. Antigen retrieval was achieved by incubatingtissue sections with 0.01% pronase for 25 min at 401C. Sectionswere then incubated with 1 : 50 dilution of monoclonal anti-pimonidazole antibody (Natural Pharmacia International Inc.)for 40 min at room temperature. This step was followed bybiotin-conjugated rabbit anti-mouse secondary antibody andperoxidase-conjugated avidin–biotin complex (Dako, Glostrup,Denmark). Finally, sections were incubated with 3,30-diamino-benzidine peroxidase substrate and stained with haematoxylin. Theslide in which primary antibody was omitted served as a negativecontrol. The mean percentage of area positive for pimonidazoleadducts was determined by the image-based analysis system LUCIA(Nikon, Tokyo, Japan). The results of the percentages of necrotictumour area and the percentages of pimonidazole-positive areawere presented as AM and s.e. for each experimental group.
Mathematical model of electric field distribution in andaround a blood vessel
The lumen of a tumour blood vessel was modelled as a cylinderwith a diameter of 15 and 8 mm and an electric conductivity of0.75 S m�1 for larger tumour vessels and 0.6 S m�1 for tumourcapillaries, which is the electric conductivity of the blood serum(Hirsch et al, 1950, Tozer et al, 2001). The wall of the blood vesselwas modelled as a layer with a thickness of 1 mm and the tumour
Electroporation and electrochemotherapy
G Sersa et al
389
British Journal of Cancer (2008) 98(2), 388 – 398& 2008 Cancer Research UK
Tra
nsl
ati
on
al
Th
era
peu
tics

tissue as a homogeneous material surrounding the vessel wall.Both regions were assigned an electric conductivity of 0.3 S m�1,which is an average value of reported bulk electric conductivitiesof soft tissues (including epithelial and tumour tissues) that rangefrom 0.1 to 0.5 S m�1 (Geddes and Barker, 1967; Duck, 1990;Gabriel et al, 1996). The distribution of the electric potential wasderived analytically by solving the Laplace equation in cylindricalcoordinates with the boundary conditions of homogeneity of theelectric field far from the vessel, boundedness and continuity of theelectric potential, and continuity of the electric current density(Kotnik et al, 1997; Kotnik and Miklavcic, 2000). The distributionof the electric field was then determined by calculating the gradientof the electric potential.
Power Doppler ultrasonographic imaging
The gross tumour perfusion changes after application of electricpulses, BLM and electrochemotherapy to the tumours wereevaluated by power Doppler ultrasonographic imaging. Beforeand after (at 3 min, 35 min and 48 h) different therapies, grey-scaleultrasound (US) of tumours was performed. The longest and theshortest diameter of tumour and the longest diameter of anechogenic central part (necrosis) were measured. After baseline,US scan evaluation power Doppler US was performed at each timepoint to check vascularisation. Before microbubble contrast agent(Sono Vue, Bracco, Milan, Italy) injection, the persistence of theimage display on the US machine was set to zero, the signal gainwas registered below the noise threshold, and one focus waspositioned below the level of the lesion. SonoVue is a sulphurhexafluoride-filled microbubble contrast agent that is licensed foruse in abdominal and vascular imaging in most Europeancountries. This agent has a strong nonlinear harmonic responsewhen it is insonated with low acoustic power. The safety andeffectiveness of this agent in vascular and parenchymal diagnosticapplications have been proved in preliminary experimental andclinical investigations (Delorme and Krix, 2006).
SonoVue (5 mg ml�1) was mixed with a solution of sodiumchloride 0.9% w v�1 solution to form a dispersion containingmillions of tiny bubbles of sulphur hexafluoride gas. The solutionwas injected intravenously (0.2 ml) in mice by using a 27-gaugeneedle. After 5– 10 s, we observed strong peripheral enhancement,and central necrosis was better depicted as on baseline US image.If contrast enhancement was considered inadequate by the on-siteexaminator after the first bolus injection, the mouse receivedan additional microbubble contrast agent bolus (0.2 ml). Wemonitored contrast enhancement for at least 5 min after injection.During the measurements, the mice were anaesthetised in the sameway as for EPR oximetry measurements. All US examinations wereperformed by one experienced radiologist on a US machine (AplioHU 80; Toshiba, Otawara, Japan) with a 12 MHz, 38-mm longlinear transducer. The scanning plane was selected for optimalvisualisation of enhancement. Dynamic US data were stored in theUS unit until the signal enhancement had completely diminished,usually within 5 min. Static images were obtained before and every15 s after injection of the contrast agent. The whole examinationwas stored on a CD for further analysis.
Laser Doppler flowmetry
Relative blood perfusion was monitored using an OxyFlo2000Laser Doppler flowmeter and OxyData data acquisition unit(Oxford Optronix Ltd, Oxford, UK). The signals were sampledand stored at a frequency of 100 Hz. The theory and applicationsof laser Doppler flowmetry (LDF) are well known (Shepherd andOberg, 1990); briefly, LDF measures the spread of the wavelengthsof photons emitted by a coherent laser source when the photonsscatter on moving red blood cells in capillaries. The distribution of
photon wavelengths is used for calculation of relative micro-circulation in tissue.
For skin measurements, LDF can be used entirely noninvasively.In our study, we, however, used thin invasive probes (diameter200mm) to assess the perfusion inside the tumour (Jarm et al,2002). To minimise discomfort of the mice and to keep them asmotionless as possible during 1 h continuous monitoring, the micewere anaesthetised using isoflurane (flurane-isoflurane; AbbottLabs, Berkshire, UK). Isoflurane was delivered to the mice via aminiature face mask in a mixture of oxygen and nitrous oxide(flow of each 0.6 l min�1) at 3.0 and 1.8% concentrations,respectively, for induction and maintenance of anaesthesia.Although anaesthetised, the mice were kept on an automaticallyregulated heating pad to prevent hypothermia. Rectal temperaturewas kept as close as possible to 371C with variations of up to0.51C during single measurements and with the contact surfacetemperature of the heating pad always below 391C.
Approximately 4 min after the induction of anaesthesia, the dataacquisition was started and a probe inserted in the tumour. Theprobe was inserted through a small superficial incision in theskin, pushed a few millimetres into the tumour and then slightlywithdrawn to minimise the pressure of the tip of the probe on thesurrounding tissue. After approximately 30 min, either BLM orphysiological saline was injected intravenously. Exactly 3 min afterthe injection, the electrodes were attached to the tumour and theelectric pulses delivered. The electrodes were then removed andthe blood flow signal recording continued for at least 1 hafterwards. In the control and BLM groups, the electrodes weremanipulated in the same way as in the groups treated by electricpulses or electrochemotherapy, except that no electric pulses wereapplied. Special care was taken throughout the measurements tominimise all movements of the probes and the mouse to keep themovement artefacts in recorded signals as small as possible.
After the measurement, the raw laser Doppler signals were firstfiltered using a special custom-made digital filter to removemovement artefacts caused mostly by respiration of the mice (seeFigure 5A as an example), thus resulting in a smoothed anddownsampled (1 Hz) version of the raw signal, which representedthe actual baseline blood flow level. We defined the moment 1 secbefore the application of the first electric pulse (3 min afterinjection) as time zero (see Figure 5B). From the filtered signal,average blood flow values at distinct predefined time momentsbefore, at and after the treatment were calculated. In general, thesetime moments were spaced at intervals of 5 min except aroundtime zero, where they were distributed more densely to track rapidchanges in baseline blood flow levels occurring after the treatment.Average blood flow values were calculated from filtered signalsegments of 20 s length cantered at the aforementioned timemoments. As the last step, all average blood flow values werenormalised with respect to the average blood flow level measured5 min before time zero (pretreatment value at �5 min in Figure 5Band C). Thus, the blood flow level in each tumour was expressed asa percentage of the pretreatment blood flow level. These relativevalues were then used to present the final results and to evaluatethe effects of different treatments on tumour blood flow.
Assessment of tumour perfusion by Patent blue staining
Patent blue (Byk Gulden, Krenzlingen, Switzerland) was used toestimate tumour perfusion. Patent blue (1.25%) diluted in 0.2 ml0.9% NaCl was injected at different time points after treatment intothe tail vein of animals with tumours from the control, electricpulses, BLM and electrochemotherapy groups. After the dye wasdistributed evenly through the tissue (1 min), animals were killedand the tumours carefully excised. The excised tumours wereremoved from the skin, cut in half along their largest diameter andphotographed. The images were evaluated using Image J software.The stained area of tumour cross-section was used as an indicator
Electroporation and electrochemotherapy
G Sersa et al
390
British Journal of Cancer (2008) 98(2), 388 – 398 & 2008 Cancer Research UK
Tra
nsla
tion
al
Th
era
peu
tics

of tumour perfusion. In the study comparing Patent blue stainingand the pharmacological method measuring the relative tumourblood flow, a good correlation (r¼ 0.962) was found between bothmethods (Sersa et al, 1999a, b).
Electron paramagnetic resonance oximetry
Electron paramagnetic resonance (EPR) oximetry was used toevaluate changes in the partial pressure of oxygen (pO2) intumours and subcutaneous tissue on the contralateral side beforeand after treatment of tumours with electric pulses, BLM andelectrochemotherapy. Electron paramagnetic resonance oximetryis a non-invasive method (after insertion of the paramagneticprobe), which allows monitoring of pO2 repeatedly at the samepoint in the tissue over long periods of time (O’Hara et al, 2001;Sersa et al, 2002). For this purpose, a paramagnetic probe, a char(B0.5 mm3, with particle size of approximately 10 mm) fromBubinga tree (a kind gift of EPR Center for Viable System,Dartmouth College of Medicine, Hanover, NH, USA), which issensitive to oxygen, was implanted into the tumour centre andperiphery (tumour volume approximately 40 mm3) and in thesubcutis 1 day before the treatments. Its EPR spectral linewidthwas measured at different time points up to 2 days after thetreatment. The char implantation with a sterile needle did notprovoke bleeding. In the presence of oxygen, the linewidth of theEPR lines is broadened; the extent of broadening depends on pO2
(Swartz et al, 1993; Swartz and Clarkson, 1998). The pO2 in theregion in contact with the probe was measured.
The measurements were performed on a Varian E-9 EPRspectrometer with a custom-made low-frequency microwavebridge operating at 1.1 GHz and an extended loop resonator(11 mm in diameter), both designed by Professor T Walczak(Dartmouth College of Medicine, Hanover, NH, USA). Typicalspectrometer settings were modulation frequency, 100 kHz;modulation amplitude not more than one-third of the peak-to-peak linewidth, and scan range, 2 mT. The linewidth of the EPRspectra reflects the pO2, which was determined from an existingcalibration curve (Krzic et al, 2001).
For EPR oximetry, animals were anaesthetised with a mixture ofDomitor (1.0 mg per kg body weight; Pfizer GmbH, Karlsruhe,Germany) and 10% ketamine (75.0 mg per kg body weight; Veyx-Pharma GmbH, Schwarzenborn, Germany) administered intra-peritoneally. During anaesthesia, body temperature was kept atphysiological values by a regulated heating pad on which the micewere placed (Guymar T/pump; Linton Instruments, Norfolk, UK).
Statistical analysis
Significance tests were carried out on the data groups usinganalysis of variance followed by the Bonferroni t-test for individualpairwise comparisons, with values of Po0.05 considered assignificant. The SigmaStat statistical software was used forstatistical analysis (SPSS Inc., Chicago, IL, USA).
RESULTS
Antitumour effect of electrochemotherapy
Electrochemotherapy with BLM was very effective in treatmentof subcutaneous SA-1 tumours, resulting in substantial tumourgrowth delay and high percentage of tumour cures, compared tountreated tumours and tumours treated with BLM or applicationof electric pulses alone (Table 1).
Tumour histology after electrochemotherapy
Electrochemotherapy with BLM had, as already mentioned,significant antitumour effect on tumour growth. We specificallyobserved significant increase in extent in tumour necrosis reachingB50% at 48 h after the treatment (Po0.05 compared to othertreatment groups). The necrotic areas were found mostly in thecentre of the tumours and consisted of cells with eosinophiliccytoplasm and pycnotic nuclei. In some cells, acute cellularswelling and nuclear disappearance with cell ghosts were alsofound. Central necrosis was surrounded by a thin viable tumourrim that led to regrowth after 8 –10 days in those tumours thatwere not cured (Figure 1). The extent of tumour necrosis in thetumours treated with BLM only was the same as in the untreatedtumours, confirming the data on tumour growth. The applicationof electric pulses alone increased the extent of necrosis in thetumours, but only transiently, returning to the normal valueswithin 48 h after treatment. This small but significant increase(Po0.05) in the extent of tumour necrosis up to 24 h after thetreatment confirmed the previous observation that the applicationof electric pulses alone to the tumours induced a small butinsignificant retardation in tumour growth (tumour growthdelay¼ 0.6 days, P40.05).
Table 1 Tumour growth after electrochemotherapy with bleomycin
Group NTumour doubling time
(days; AM±s.e.)P-value compared to tumour
doubling time of controlTumour growth delay
(days; AM±s.e.)Cures n
(%)
Control 16 1.2±0.06 0Bleomycina 16 1.2±0.04 NS 0.0 0Electric pulsesb 16 1.8±0.02 NS 0.6±0.02 0Electrochemotherapyc 16 23.7±4.6 Po0.05 22.5±4.6 6 (38)
NS¼ nonsignificant. aBleomycin injected intravenously (1 mg kg�1). bApplication of electric pulses to the tumour (8 pulses, 1040 V, 100 ms, 1 Hz). cElectrochemotherapy:application of electric pulses to the tumour 3 min after intravenous injection of bleomycin.
60ControlBleomycinElectric pulsesElectrochemotherapy
50
40
30
20
10
00 10 20 30
Time after theraphy (h)
% o
f nec
rosi
s
40 50
Figure 1 Time course of changes in tumour necrosis in untreatedcontrol tumours, and after treatment of tumours with bleomycin,application of electric pulses or electrochemotherapy. Symbols indicateAM (arithmetic mean)±s.e. of at least three mice per point.
Electroporation and electrochemotherapy
G Sersa et al
391
British Journal of Cancer (2008) 98(2), 388 – 398& 2008 Cancer Research UK
Tra
nsl
ati
on
al
Th
era
peu
tics

Tumour slides were also examined for blood vessels changes.Changes in the endothelial cell shape were observed 1 h after theapplication of electric pulses. Endothelial cells were rounded upand swollen and the lumen of blood vessels was narrowed(Figure 2A). After electrochemotherapy, the same morphologicalchanges were found. At later times after electrochemotherapy (8 h),in some vessels endothelial cells with apoptotic morphologicalcharacteristics were found (Figure 2B). Furthermore, blood vesselswere stacked with erythrocytes and extravasation of erythrocyteswas also observed (Figure 2B). Apoptotic endothelial cells were notobserved in tumours treated with electric pulses alone, BLM aloneor in the control group.
Mathematical model of electric field distribution in andaround a blood vessel
The local distortion of the electric field in the vicinity of a bloodvessel is illustrated in the two plots in Figure 3, for a thin capillary
of 8 mm diameter (Figure 3A) and for a thicker tumour vessel of15mm diameter (Figure 3B). Denoting by E the local field and by E0
the homogeneous field far from the vessel, the plots show the ratioE/E0 along the cross-section passing through the centre of thevessel (line a) for the vessel perpendicular to the field directionand for the vessel tilted by 301 and 601 with respect to the fielddirection. As the plots show, the electric field in the tissue at thevery edge of the lumen, that is in the endothelium of the bloodvessel, can exceed the homogeneous value by as much as 42% inthe extreme case (the larger vessel, perpendicular orientation) andby 10– 30% in typical cases, represented by different orientationsof the vessels. This is the consequence of the significantly higherconductivity of the blood with respect to the surrounding tissue(see Materials and methods), due to which the electric current islocally concentrated in the vicinity and inside the blood vessel. Inthe blood, the electric field is only 60– 90% of the homogeneousfield in the tissue, which reflects the fact that the electric field is theratio between the current density and the conductivity and that the
50 �m 50 �m
A B
Figure 2 (A) Rounding up of tumour blood vessels endothelial cells 1 h after electric pulses increases vascular resistance to blood flow (arrows).(B) Apoptotic-like endothelial cells occur in tumours 8 h after electrochemotherapy (arrows).
1.50 E/E0
1.25
1.00
0.75
0.50
0.25
30 20 10 0 10
Blood withreducedserum content(0.60 S m–1)
Endothelium (0.3 S m–1)
Blood (0.75 S m–1)
Endothelium (0.3 S m–1)
Tumour tissue (0.3 S m–1)
Tumour tissue (0.3 S m–1)
20 30 �m
1.50 E/E0
1.25
1.00
0.75
0.50
0.25
30 20 10 0 10 20 30 �m
E0 E0
a a
Figure 3 The electric field strength in a capillary of 8mm diameter (A), a vessel of 15mm diameter (B) and in the endothelial and tumour tissuesurrounding them. The plot shows the ratio between the local electric field (E) along the line a and the external field to which the tissue is exposed (E0), forthree different orientations of the vessel with respect to the field (901 – solid, 601 – dashed, 301 – dotted). The conductivities of the tissues and the bloodare taken from the literature (Hirsch et al, 1950; Duck 1990; Gabriel et al, 1996). In the capillary, a somewhat lower serum content (and thereforeconductivity) is assumed due to the erythrocytes filling most of the volume in the thin passages.
Electroporation and electrochemotherapy
G Sersa et al
392
British Journal of Cancer (2008) 98(2), 388 – 398 & 2008 Cancer Research UK
Tra
nsla
tion
al
Th
era
peu
tics
conductivity of blood is considerably higher than the conductivityof the surrounding tissue. Consequently, the model predicts thatendothelial cells lining the blood vessels are exposed to up to 40%higher electric field than the surrounding tumour cells.
Tumour blood flow changes induced by application ofelectric pulses and electrochemotherapy
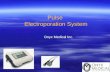
We have already demonstrated in previous studies that electricpulses and electrochemotherapy significantly reduce the bloodflow of the treated tumours (Sersa et al, 1999a, b). In this study, weused two new approaches to further evaluate this effect. We usedpower Doppler ultrasonographic imaging to assess the grosstumour blood flow changes and LDF to monitor local micro-vascular blood flow in the tissue. The application of eight electricpulses to the tumours reduced the blood flow of the tumoursimmediately after their application. Power Doppler ultrasono-graphic imaging showed immediate abrogation of blood flow inthe vessels supplying the tumour, with restoration of blood flowwithin 48 h after application of electric pulses alone (Figure 4).The same time course of the effect was observed after elec-trochemotherapy of the tumours. However, at 48 h after electro-chemotherapy, a reduced tumour blood flow was still observedafter electrochemotherapy, contrary to electric pulses alone. Bloodflow in tumours in the control group and in tumours treated withBLM only did not change during the observation period.
We were further able to follow the exact profile of micro-circulatory changes by means of LDF after application of electricpulses to the tumours or electrochemotherapy in a small volumeof tumour tissue. Figure 5A shows a highly reproducible exampleof an extremely rapid decline in microcirculatory perfusion, which
starts as soon as the first pulse is delivered and continues until themaximum reduction is obtained, which can occur as soon as 10 safter application of the first pulse. This figure also demonstratesvarious movement artefacts present in raw laser Doppler signal(owing to respiration, electrode manipulation and delivery ofelectric pulses) and thus the need for filtering of such a signalbefore any signal analysis.
Figure 5B and C show average changes in perfusion of tumoursin the four experimental groups. The rapid and abrupt initialdecrease in perfusion of tumours after application of electricpulses and electrochemotherapy-treated tumours was followed bya gradual but only partial reperfusion of the tumours. This partialreperfusion peaked approximately 10–15 min after delivery ofelectric pulses and did not continue afterwards. On the contrary,the injection of BLM or physiological saline (control) produced nosignificant changes during the observation period. The fourexperimental groups started to differ significantly as soon as 30 safter application of electric pulses and remained significantlydifferent until the end of observation (Po0.001 for all timeinstants after time zero in Figure 5B). The differences were highlysignificant (Po0.001) between control and BLM alone comparedto the group of tumours that was exposed to electric pulses or theelectrochemotherapy group. Differences between the groups beforeand at time zero in Figure 5B were not statistically significant(P40.05). It was also interesting to note that the two groupsinvolving the use of BLM (BLM alone and electrochemotherapy)developed higher blood flow levels after treatment than thecorresponding two groups without BLM (control and applicationof electric pulses, respectively), which can be observed inFigure 5B. However, even though this difference was consistent,it was not statistically significant (P40.05).
Before
Ele
ctro
chem
othe
rapy
Ele
ctric
pul
ses
Ble
omyc
inC
ontr
ol
3 min after 35 min after 48 h after
AA
A
A
A
AA
A
A
AA
A
B
B
B
B
B
B
B
B
B
B
Figure 4 Representative power Doppler ultrasonographic images of tumours (delineated with white lines A and B) treated by bleomycin, electric pulsesor electrochemotherapy at various time points post-treatment.
Electroporation and electrochemotherapy
G Sersa et al
393
British Journal of Cancer (2008) 98(2), 388 – 398& 2008 Cancer Research UK
Tra
nsl
ati
on
al
Th
era
peu
tics

Tumour perfusion changes were also measured by Patent bluestaining of the tumours with similar vascular effects as observedwith other methods of measurement (Figure 6). An immediatereduction was observed in tumour perfusion after application ofelectric pulses and electrochemotherapy with reduction of tumourperfusion to 10% of the value in control tumours. Approximately0.5 h later, the tumours started to reperfuse in both groups; in thetumours treated by electrochemotherapy, the reperfusion levelled
at B1 h after the treatment and stayed at B20% up to 48 h afterthe treatment, whereas the tumours treated with application ofelectric pulses continued to reperfuse and reached normal valuesbetween 24 and 48 h.
Tumour hypoxia induced by application of electric pulsesand electrochemotherapy
Blood flow measurements showed that there is an immediatereduction of tumour blood flow after the application of electricpulses and electrochemotherapy. Owing to the effect of appliedelectric pulses on the vascular supply of the tumours, the extent ofhypoxic regions in the tumours as a consequence of reducedtumour blood flow was determined.
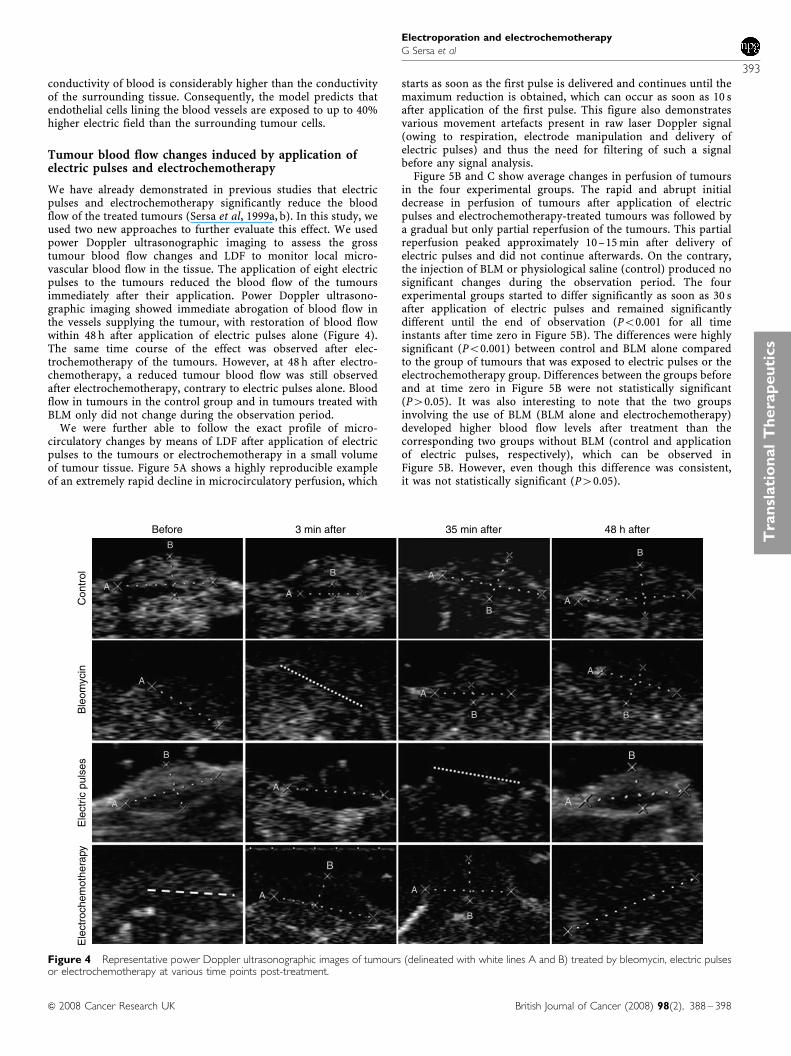
Tumour sections were immunohistochemically stained forprotein adduct of reductively activated pimonidazole. Positivestaining was found in the cytoplasm of tumour cells and somepositive nuclei of tumour cells were also determined. Aspimonidazole is known to be preferentially bound by hypoxictumour cells, the detection of pimonidazole adducts usingmonoclonal antibodies can serve as a method for measuringtumour hypoxia. In most control tumours, discrete foci ofpimonidazole positivity were found. In BLM-treated tumours, arim of positive cells was found mainly around the necrotic area. Inelectric pulses and in the electrochemotherapy-treated group oftumours, reticular staining patterns were observed at somedistance from blood vessels, with some diffuse pimonidazole-positive area. In some slides from the electrochemotherapy-treatedgroup of tumours, the endothelial cells of blood vessels were alsopositive. The tumour cells around these pimonidazole-labelledvessels did not show pimonidazole immunoreactivity (Figure 7).
The percentage of pimonidazole-positive tumour areas in viabletumour tissue was determined and the results are presented inFigure 8. Both in the group of tumours treated with electric pulsesand in those treated with electrochemotherapy, the onset oftumour hypoxia was instant, reaching its peak at 2 h and lasting upto 8 h after treatment. After the application of electric pulses, therecovery to the pretreatment level lasted 14 h, whereas the recoveryto pretreatment level after electrochemotherapy lasted 24 h. From24 to 48 h after treatment, the level of tumour hypoxia was thesame in all experimental groups.
Tissue oxygenation changes induced by application ofelectric pulses and electrochemotherapy
Partial pressure of oxygen was measured in animals treated withBLM and with the application of electric pulses to the tumours andelectrochemotherapy, using EPR oximetry. In the same animals,
2500
RawFiltered
8 EP pulses
Respiration movement artefacts
Blo
od fl
ow (
BP
U)
Rel
ativ
e bl
ood
flow
(%
)R
elat
ive
bloo
d flo
w (
%)
2000
1500
1000
500
0
0
140
120
100
80
60
40
20
0
20
40
60
80
100
120
140
–20
–15
–10 –5
–10 0
0
4321
15
0 5 10
30 45 60
Time after electric pulses (s)
Time after electric pulses (min)
Time after electric pulses (min)
Control (n=13)Bleomycin (n=17)Electric pulses (n=14)Electrochemotherapy (n=13)
10 20
Figure 5 Blood flow changes after different treatments assessed bymeans of laser Doppler flowmetry. (A) Rapid decrease in blood flowimmediately after application of electric pulses (EP). Movement artefactcaused by the pulses, manipulation of the electrodes (spikes just before andafter pulses) and respiration (before and after electroporation) can beobserved in the raw signal along with the filtered signal. (B) Average bloodflow values before and after treatment expressed as a percentage of thepretreatment blood flow (mean values with s.e. bars are shown). After timezero, the differences between the groups were statistically highly significant(Po0.001). (C) A close-up from (B): (1) pretreatment level at �5 min; (2)moment of injection at �3 min; (3) �1.5 min; (4) time zero. Relatively largescatter (nonsignificant) of values at time zero was of transient nature andwas a result of movement artefacts caused by manipulation of theelectrodes. Note different time scale.
1009080706050403020100
0 10 20 30 40 50
Time after therapy (h)
% o
f sta
ined
tum
our
area
Control Bleomycin Electric pulses Electrochemotherapy
Figure 6 Time course of changes in tumour perfusion in untreatedtumours, and after treatment of tumours with bleomycin, application ofelectric pulses or electrochemotherapy. Symbols indicate AM (arithmeticmean)±s.e. of at least three mice per point.
Electroporation and electrochemotherapy
G Sersa et al
394
British Journal of Cancer (2008) 98(2), 388 – 398 & 2008 Cancer Research UK
Tra
nsla
tion
al
Th
era
peu
tics
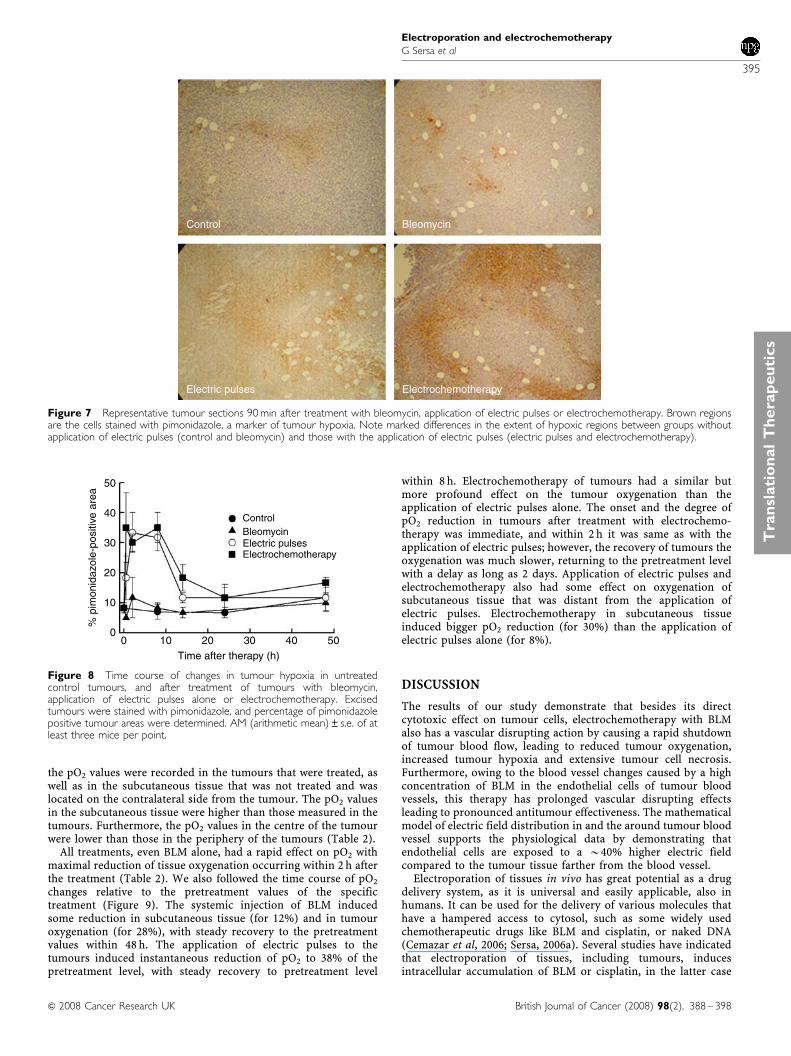
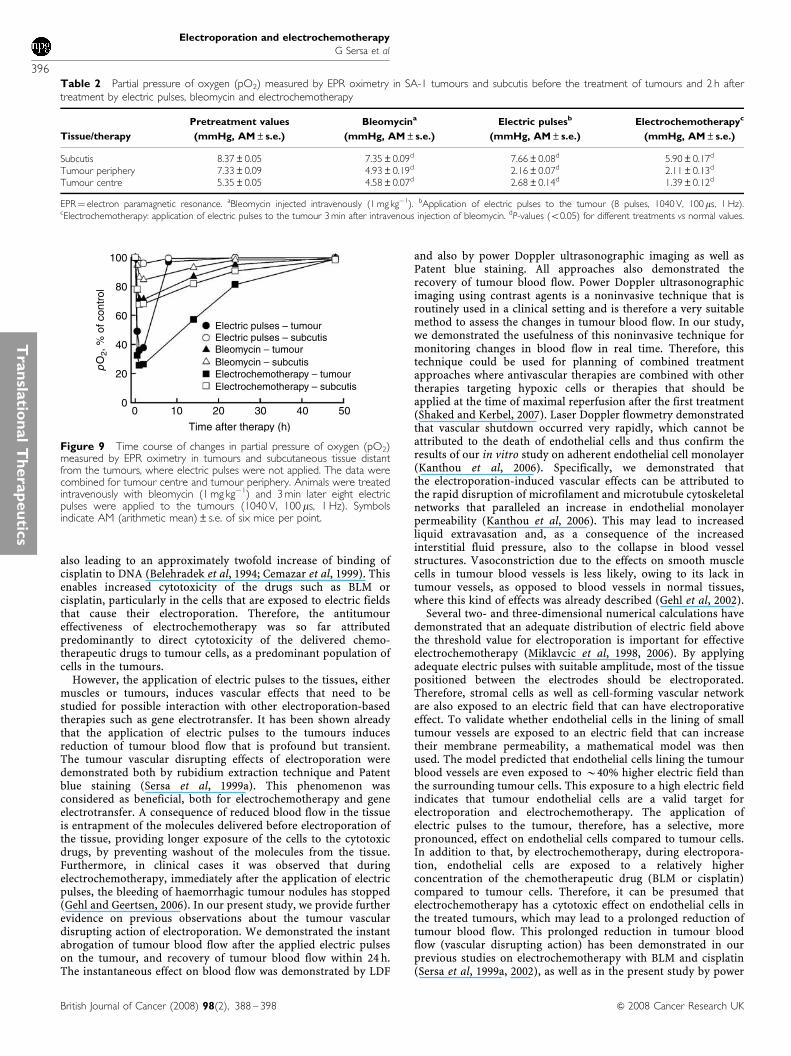
the pO2 values were recorded in the tumours that were treated, aswell as in the subcutaneous tissue that was not treated and waslocated on the contralateral side from the tumour. The pO2 valuesin the subcutaneous tissue were higher than those measured in thetumours. Furthermore, the pO2 values in the centre of the tumourwere lower than those in the periphery of the tumours (Table 2).
All treatments, even BLM alone, had a rapid effect on pO2 withmaximal reduction of tissue oxygenation occurring within 2 h afterthe treatment (Table 2). We also followed the time course of pO2
changes relative to the pretreatment values of the specifictreatment (Figure 9). The systemic injection of BLM inducedsome reduction in subcutaneous tissue (for 12%) and in tumouroxygenation (for 28%), with steady recovery to the pretreatmentvalues within 48 h. The application of electric pulses to thetumours induced instantaneous reduction of pO2 to 38% of thepretreatment level, with steady recovery to pretreatment level
within 8 h. Electrochemotherapy of tumours had a similar butmore profound effect on the tumour oxygenation than theapplication of electric pulses alone. The onset and the degree ofpO2 reduction in tumours after treatment with electrochemo-therapy was immediate, and within 2 h it was same as with theapplication of electric pulses; however, the recovery of tumours theoxygenation was much slower, returning to the pretreatment levelwith a delay as long as 2 days. Application of electric pulses andelectrochemotherapy also had some effect on oxygenation ofsubcutaneous tissue that was distant from the application ofelectric pulses. Electrochemotherapy in subcutaneous tissueinduced bigger pO2 reduction (for 30%) than the application ofelectric pulses alone (for 8%).
DISCUSSION
The results of our study demonstrate that besides its directcytotoxic effect on tumour cells, electrochemotherapy with BLMalso has a vascular disrupting action by causing a rapid shutdownof tumour blood flow, leading to reduced tumour oxygenation,increased tumour hypoxia and extensive tumour cell necrosis.Furthermore, owing to the blood vessel changes caused by a highconcentration of BLM in the endothelial cells of tumour bloodvessels, this therapy has prolonged vascular disrupting effectsleading to pronounced antitumour effectiveness. The mathematicalmodel of electric field distribution in and the around tumour bloodvessel supports the physiological data by demonstrating thatendothelial cells are exposed to a B40% higher electric fieldcompared to the tumour tissue farther from the blood vessel.
Electroporation of tissues in vivo has great potential as a drugdelivery system, as it is universal and easily applicable, also inhumans. It can be used for the delivery of various molecules thathave a hampered access to cytosol, such as some widely usedchemotherapeutic drugs like BLM and cisplatin, or naked DNA(Cemazar et al, 2006; Sersa, 2006a). Several studies have indicatedthat electroporation of tissues, including tumours, inducesintracellular accumulation of BLM or cisplatin, in the latter case
Control Bleomycin
Electric pulses Electrochemotherapy
Figure 7 Representative tumour sections 90 min after treatment with bleomycin, application of electric pulses or electrochemotherapy. Brown regionsare the cells stained with pimonidazole, a marker of tumour hypoxia. Note marked differences in the extent of hypoxic regions between groups withoutapplication of electric pulses (control and bleomycin) and those with the application of electric pulses (electric pulses and electrochemotherapy).
0
% p
imon
idaz
ole-
posi
tive
area
50
40
30
20
10
010 20 30 40 50
Time after therapy (h)
Control Bleomycin Electric pulses Electrochemotherapy
Figure 8 Time course of changes in tumour hypoxia in untreatedcontrol tumours, and after treatment of tumours with bleomycin,application of electric pulses alone or electrochemotherapy. Excisedtumours were stained with pimonidazole, and percentage of pimonidazolepositive tumour areas were determined. AM (arithmetic mean)±s.e. of atleast three mice per point.
Electroporation and electrochemotherapy
G Sersa et al
395
British Journal of Cancer (2008) 98(2), 388 – 398& 2008 Cancer Research UK
Tra
nsl
ati
on
al
Th
era
peu
tics
also leading to an approximately twofold increase of binding ofcisplatin to DNA (Belehradek et al, 1994; Cemazar et al, 1999). Thisenables increased cytotoxicity of the drugs such as BLM orcisplatin, particularly in the cells that are exposed to electric fieldsthat cause their electroporation. Therefore, the antitumoureffectiveness of electrochemotherapy was so far attributedpredominantly to direct cytotoxicity of the delivered chemo-therapeutic drugs to tumour cells, as a predominant population ofcells in the tumours.
However, the application of electric pulses to the tissues, eithermuscles or tumours, induces vascular effects that need to bestudied for possible interaction with other electroporation-basedtherapies such as gene electrotransfer. It has been shown alreadythat the application of electric pulses to the tumours inducesreduction of tumour blood flow that is profound but transient.The tumour vascular disrupting effects of electroporation weredemonstrated both by rubidium extraction technique and Patentblue staining (Sersa et al, 1999a). This phenomenon wasconsidered as beneficial, both for electrochemotherapy and geneelectrotransfer. A consequence of reduced blood flow in the tissueis entrapment of the molecules delivered before electroporation ofthe tissue, providing longer exposure of the cells to the cytotoxicdrugs, by preventing washout of the molecules from the tissue.Furthermore, in clinical cases it was observed that duringelectrochemotherapy, immediately after the application of electricpulses, the bleeding of haemorrhagic tumour nodules has stopped(Gehl and Geertsen, 2006). In our present study, we provide furtherevidence on previous observations about the tumour vasculardisrupting action of electroporation. We demonstrated the instantabrogation of tumour blood flow after the applied electric pulseson the tumour, and recovery of tumour blood flow within 24 h.The instantaneous effect on blood flow was demonstrated by LDF
and also by power Doppler ultrasonographic imaging as well asPatent blue staining. All approaches also demonstrated therecovery of tumour blood flow. Power Doppler ultrasonographicimaging using contrast agents is a noninvasive technique that isroutinely used in a clinical setting and is therefore a very suitablemethod to assess the changes in tumour blood flow. In our study,we demonstrated the usefulness of this noninvasive technique formonitoring changes in blood flow in real time. Therefore, thistechnique could be used for planning of combined treatmentapproaches where antivascular therapies are combined with othertherapies targeting hypoxic cells or therapies that should beapplied at the time of maximal reperfusion after the first treatment(Shaked and Kerbel, 2007). Laser Doppler flowmetry demonstratedthat vascular shutdown occurred very rapidly, which cannot beattributed to the death of endothelial cells and thus confirm theresults of our in vitro study on adherent endothelial cell monolayer(Kanthou et al, 2006). Specifically, we demonstrated thatthe electroporation-induced vascular effects can be attributed tothe rapid disruption of microfilament and microtubule cytoskeletalnetworks that paralleled an increase in endothelial monolayerpermeability (Kanthou et al, 2006). This may lead to increasedliquid extravasation and, as a consequence of the increasedinterstitial fluid pressure, also to the collapse in blood vesselstructures. Vasoconstriction due to the effects on smooth musclecells in tumour blood vessels is less likely, owing to its lack intumour vessels, as opposed to blood vessels in normal tissues,where this kind of effects was already described (Gehl et al, 2002).
Several two- and three-dimensional numerical calculations havedemonstrated that an adequate distribution of electric field abovethe threshold value for electroporation is important for effectiveelectrochemotherapy (Miklavcic et al, 1998, 2006). By applyingadequate electric pulses with suitable amplitude, most of the tissuepositioned between the electrodes should be electroporated.Therefore, stromal cells as well as cell-forming vascular networkare also exposed to an electric field that can have electroporativeeffect. To validate whether endothelial cells in the lining of smalltumour vessels are exposed to an electric field that can increasetheir membrane permeability, a mathematical model was thenused. The model predicted that endothelial cells lining the tumourblood vessels are even exposed to B40% higher electric field thanthe surrounding tumour cells. This exposure to a high electric fieldindicates that tumour endothelial cells are a valid target forelectroporation and electrochemotherapy. The application ofelectric pulses to the tumour, therefore, has a selective, morepronounced, effect on endothelial cells compared to tumour cells.In addition to that, by electrochemotherapy, during electropora-tion, endothelial cells are exposed to a relatively higherconcentration of the chemotherapeutic drug (BLM or cisplatin)compared to tumour cells. Therefore, it can be presumed thatelectrochemotherapy has a cytotoxic effect on endothelial cells inthe treated tumours, which may lead to a prolonged reduction oftumour blood flow. This prolonged reduction in tumour bloodflow (vascular disrupting action) has been demonstrated in ourprevious studies on electrochemotherapy with BLM and cisplatin(Sersa et al, 1999a, 2002), as well as in the present study by power
Bleomycin – tumour Bleomycin – subcutis
Electric pulses – tumourElectric pulses – subcutis
Electrochemotherapy – tumourElectrochemotherapy – subcutis
00
20
40
60
80
100
10 20 30 40 50
Time after therapy (h)
pO
2, %
of c
ontr
ol
Figure 9 Time course of changes in partial pressure of oxygen (pO2)measured by EPR oximetry in tumours and subcutaneous tissue distantfrom the tumours, where electric pulses were not applied. The data werecombined for tumour centre and tumour periphery. Animals were treatedintravenously with bleomycin (1 mg kg�1) and 3 min later eight electricpulses were applied to the tumours (1040 V, 100 ms, 1 Hz). Symbolsindicate AM (arithmetic mean)±s.e. of six mice per point.
Table 2 Partial pressure of oxygen (pO2) measured by EPR oximetry in SA-1 tumours and subcutis before the treatment of tumours and 2 h aftertreatment by electric pulses, bleomycin and electrochemotherapy
Pretreatment values Bleomycina Electric pulsesb Electrochemotherapyc
Tissue/therapy (mmHg, AM±s.e.) (mmHg, AM±s.e.) (mmHg, AM±s.e.) (mmHg, AM±s.e.)
Subcutis 8.37±0.05 7.35±0.09d 7.66±0.08d 5.90±0.17d
Tumour periphery 7.33±0.09 4.93±0.19d 2.16±0.07d 2.11±0.13d
Tumour centre 5.35±0.05 4.58±0.07d 2.68±0.14d 1.39±0.12d
EPR¼ electron paramagnetic resonance. aBleomycin injected intravenously (1 mg kg�1). bApplication of electric pulses to the tumour (8 pulses, 1040 V, 100ms, 1 Hz).cElectrochemotherapy: application of electric pulses to the tumour 3 min after intravenous injection of bleomycin. dP-values (o0.05) for different treatments vs normal values.
Electroporation and electrochemotherapy
G Sersa et al
396
British Journal of Cancer (2008) 98(2), 388 – 398 & 2008 Cancer Research UK
Tra
nsla
tion
al
Th
era
peu
tics

Doppler US imaging and Patent blue staining. The measurement ofhypoxia in tumours and partial pressure of oxygen do not entirelyfollow the measurement of reduction of blood flow. The reductionof partial pressure of oxygen was instantaneous but with quickrecovery to the pretreatment level within 8 h after application ofelectric pulses or 48 h after electrochemotherapy of the tumours.These results on tissue oxygenation correlated well with theobserved percentage of the pimonidazole-positive area, but notwith the reduction of tumour blood flow as demonstrated bypower Doppler ultrasonography and Patent blue staining. Wedemonstrated that the pimonidazole-positive area increased to35% within 1 h after treatment, with recovery to control valueswithin 12 h after application of electric pulses, whereas tumourblood flow did not recover during the observation period. Thereason for that can be that the percentage of pimonidazole-positivearea did not increase after electrochemotherapy because in theviable area that remained after therapy, blood flow was restoredand the pimonidazole-positive areas were not evaluated in thenecrotic areas. Another reason for lower pimonidazole-positiveareas can also be ascribed to the fact that the pimonidazole uptakeinto tumour tissue could be prevented if some parts of the tumoursare not perfused at all (owing to the normal fluctuation of tumourblood flow), and this could result in falsely negative areas, despitebeing hypoxic owing to the treatment. Furthermore, the dis-crepancy between the oxygenation measurements obtained by EPRoximetry and blood flow reduction measured by power Dopplersonography and Patent blue technique could be due to thedifferences in the sample volume of the techniques. Specifically,with power Doppler sonography, the whole tumour is assessed,whereas with EPR oximetry, pO2 is measured only in the region incontact with the probe that comprises only B0.5 mm3. As theprobes were inserted mainly in the periphery of the tumours,which is part of the tumour that recovers after the treatment withvascular disruption agents, quicker the restoration of partialoxygen pressure compared to tumour blood flow could result fromthe differences in measurement between the techniques. Never-theless, the results of partial pressure of oxygen indicated thatrestoration of oxygen supply in the region of interest afterelectrochemotherapy is much slower than after electroporationonly. This may indicate that many cells undergo cell death, whichmay take up to 24 h. Furthermore, histological analysis of thetumours indicated that the extent of tumour necrosis afterelectroporation of tumours paralleled the extent of tumournecrosis after electrochemotherapy up to 24 h after treatmentand that only thereafter is there an increase in the extent of tumournecrosis by electrochemotherapy. This may indicate, on a dualeffect, the immediate vascular disrupting action of electroporation(increase in vascular permeability due to the disruption ofendothelial cytoskeleton and endothelial cell swelling) and delayedeffect due to the exposure of these cells to a high concentration ofBLM causing endothelial cell death as observed in histologicalspecimens. The first phenomenon is present up to 8–12 h afterelectroporation of the tissue and is due to disruption of endothelialcell lining in tumour vessels leading to some extent of tumour celldeath present up to 24 h, but with quick recovery withoutsignificant antitumour effect. The second phenomenon is due toendothelial cell death caused by electrochemotherapy that inaddition to the vascular disrupting action of electroporationinduces a prolonged shutdown of tumour blood flow andconsequently a cascade of tumour cell death in the surroundingtissue that becomes evident at longer times after therapy. Furthersupport for this second phenomenon is the observation thatpredominantly central tumour necrosis after electrochemotherapywas observed, which is characteristic for vascular disruptingagents.
Electroporation compared to other vascular disrupting agentssuch as CA-4-P and DMXAA, which have specific effects ontumour blood vessels as opposed to normal blood vessels, is not
specific and selectivity is achieved by the local application ofelectric pulses to the tumours. The vascular disrupting effectsof vascular disrupting agents on tumour endothelial cells involvethe rapid reorganisation of the actin cytoskeleton, which ismediated by the disruption of the tubulin cytoskeleton for CA-4-P, but not DMXAA (Tozer et al, 2005). The signalling pathwaysassociated with CA-4-P and their effects on vascular permeabilityinvolve the activation of small GTPase Rho and Rho kinase(Kanthou and Tozer, 2002). The activation of Rho proteinsnecessitates their translocation and association with membranecomponents (Bokoch et al, 1994). In the case of electroporation,actin as well as microtubule cytoskeleton is disrupted as aconsequence of the applied electric field; however, disruption byelectroporation appears to uncouple Rho and inactivate Rhokinases. It is likely that electroporation inactivates Rho bypreventing its association with the cell membrane (Kanthouet al, 2006).
Electroporation, similar to vascular disrupting agents, induces avery rapid and significant reduction in tumour blood flow, whichcan be detected already within a minute after the application of thetreatment. The proposed mechanism for rapid tumour vascularshutdown after treatment with CA-4-P or DMXAA involves thedisruption of the cytoskeleton of endothelial cells, leading to cellshape changes and an increase in the permeability of the cellmonolayer. This would increase vascular resistance to blood flow.Apoptosis of endothelial cells might also contribute to vascularshutdown. Other contributing factors are platelet activation andserotonin release leading to active vasoconstriction. The proteinleakage due to the increased tumour vascular permeability wouldlead to oedema and an increase in tumour interstitial pressurefurther leading to vascular collapse. In addition, as the blood flowslows down, red cells stack up causing an increase in viscousresistance and slowing the blood flow by positive mechanisms. Theconsequence of this is the appearance of central necrosis with aviable peripheral rim of tumour cells, leading to rapid repopula-tion of tumours and the consequent failure to achieve significanttumour growth delay (Tozer et al, 2005). Major vascular disruptingagents that have been tested in clinical phase I studies includeCA-4-P, DMXAA, ZD6126, AVE8062 and ABT-751 (Hinnen andEskens, 2007; Patterson and Rustin, 2007). The combination ofvascular disrupting agents with other treatment modalities, such asradiotherapy or chemotherapy, leads to increased antitumoureffect of these combined treatments (Tozer et al, 2005; Pattersonand Rustin, 2007). In the case of electrochemotherapy, electro-poration is combined with chemotherapy. This treatment in asingle application thus combines the immediate vascular disrup-ting action of electroporation with delayed endothelial cell deathcaused presumably by a high chemotherapeutic drug concentra-tion in the cytosol of endothelial cells. Both these effects, inaddition to direct tumour cell killing by electrochemotherapy,contribute to the high antitumour effectiveness of electrochemo-therapy.
In conclusion, in this study, we provide evidence thatelectrochemotherapy, in addition to direct cytotoxic effect ontumour cells, has a vascular disrupting action. The vasculardisrupting action is dual, namely the effect of application ofelectric pulses to the tumours that induce a rapid shutdown oftumour blood flow that recovers within 24 h and the continuationof the vascular disrupting effect of electrochemotherapy, pre-dominantly through its cytotoxic effect on endothelial cells.
ACKNOWLEDGEMENTS
The authors acknowledge the financial support of the state budgetby the Slovenian Research Agency (project nos. P3-0003, P2-0249,J2-2222 and J3-7044).
Electroporation and electrochemotherapy
G Sersa et al
397
British Journal of Cancer (2008) 98(2), 388 – 398& 2008 Cancer Research UK
Tra
nsl
ati
on
al
Th
era
peu
tics
REFERENCES
Belehradek Jr J, Orlowski S, Ramirez LH, Pron G, Poddevin B, Mir LM(1994) Electropermeabilization of cells and tissues assessed by thequantitative and qualitative electroloading of bleomycin. Biocim BiophysActa 1190: 155 – 163
Bokoch GM, Bohl BP, Chuang TH (1994) Guanine nucleotide exchangeregulates membrane translocation of Rac/Fho GTP-binding proteins.J Biol Chem 269: 31674 – 31679
Cemazar M, Golzio M, Sersa G, Rols MP, Teissie J (2006) Electrically-assisted nucleic acids delivery to tissues in vivo: where do we stand?Curr Pharm Des 12: 3817 – 3825
Cemazar M, Miklavcic D, Scancar J, Dolzan V, Golouh R, Sersa G (1999)Increased platinum accumulation in SA-1 tumour cells after in vivoelectrochemotherapy with cisplatin. Brit J Cancer 79: 1386 – 1391
Cemazar M, Parkins CS, Holder AL, Chaplin DJ, Tozer GM, Sersa G (2001)Electroporation of human microvascular endothelial cells: evidence foranti-vascular mechanism of electrochemotherapy. Br J Cancer 84:556 – 570
Delorme S, Krix M (2006) Contrast-enhanced ultrasound for examiningtumor biology. Cancer Imaging 6: 148 – 152
Duck FA (1990) Physical Properties of Tissue. New York: Academic PressEngstrom PE, Ivarsson K, Tranberg KG, Stenram U, Salford LG, Persson BR
(2001) Electrically mediated drug delivery for treatment of anadenocarcinoma transplanted into rat liver. Anticancer Res 21(3B):1817 – 1822
Gabriel S, Lau RW, Gabriel C (1996) The dielectric properties of biologicaltissues. II. Measurements in the frequency range 10 Hz – 20 GHz.Phys Med Biol 41: 2251 – 2269
Geddes LA, Barker LE (1967) The specific resistance of biological material –a compendium of data for the biomedical engineer and physiologist.Med Biol Eng 5: 271 – 293
Gehl J, Geertsen PF (2006) Palliation of haemorrhaging and ulceratedcutaneous tumours using electrochemotherapy. Eur J Cancer Suppl 4(11):35 – 37
Gehl J, Skovsgaard T, Mir LM (2002) Vascular reactions to in vivoelectroporation: characterization and consequences for drug and genedelivery. Biochim Biophys Acta 1569: 51 – 58
Heller LC, Heller R (2006) In vivo electroporation for gene therapy.Hum Gene Ther 17: 890 – 897
Heller R, Gilbert R, Jaroszeski MJ (1999) Clinical applications ofelectrochemotherapy. Adv Drug Deliv Rev 35(1): 119 – 129
Hinnen P, Eskens FALM (2007) Vascular disrupting agents in clinicaldevelopment. Brit J Cancer 96: 1159 – 1165
Hirsch FG, Clinton EC, Wood LA, Ballard WC, Horan FE, Wright IS (1950)The electrical conductivity of blood. I. Relationship to erythrocyteconcentration. Blood 5: 1017 – 1035
Jarm T, Sersa G, Miklavcic D (2002) Oxygenation and blood flow in tumorstreated with hydralazine: evaluation with a novel luminescence-basedfiber-optic sensor. Technol Health Care 20: 363 – 380
Kanthou C, Kranjc S, Sersa G, Tozer G, Zupanic A, Cemazar M (2006) Theendothelial cytoskeleton as a target of electroporation based therapies.Mol Cancer Ther 5: 3145 – 3152
Kanthou C, Tozer GM (2002) The vascular disrupting agent combretastatinA-4 phosphate induces reorganisation of the actin cytoskeleton and earlymembrane blebbing in human endothelial cells. Blood 99: 2060 – 2069
Kotnik T, Bobanovic F, Miklavcic D (1997) Sensitivity of transmembranevoltage induced by applied electric fields – a theoretical analysis.Bioelectrochem Bioenerg 43: 285 – 291
Kotnik T, Miklavcic D (2000) Analytical description of transmembranevoltage induced by electric fields on spheroidal cells. Biophys J 79:670 – 679
Krzic M, Sentjurc M, Kristl J (2001) Improved skin oxygenation after benzylnicotinate application in different carriers as measured by EPR oximetry.J Cont Release 70: 203 – 211
Marty M, Sersa G, Garbay JR, Gehl J, Collins CG, Snoj M, Billard V,Geertsen PF, Larkin JO, Miklavcic D (2006) Electrochemotherapy – an
easy, highly effective and safe treatment of cutaneous and subcutaneousmetastases: results of ESOPE (European Standard Operating Proceduresof Electrochemotherapy) study. Eur J Cancer Suppl 4(11): 3 – 13
Miklavcic D, Beravs K, Semrov D, Cemazar M, Demsar F, Sersa G (1998)The importance of electric field distribution for effective in vivoelectroporation of tissues. Biophys J 74: 2152 – 2158
Miklavcic D, Corovic S, Pucihar G, Pavselj N (2006) Importance of tumourcoverage by sufficiently high local electric field for effective electro-chemotherapy. Eur J Cancer Suppl 4(11): 45 – 51
Mir LM (2006) Bases and rationale of the electrochemotherapy. EurJ Cancer Suppl 4(11): 38 – 44
Neumann E, Schaefer-Riddler M, Wang Y, Hofschneider PH (1982) Genetransfer into mouse myeloma cells by electroporation in high electricfields. EMBO J 1: 841 – 845
O’Hara JA, Blumenthal RD, Grinberg OY, Demidenko E, Grinberg S,Wilmot CM, Taylor AM (2001) Response to radioimmunotherapycorrelates with tumor pO2 measured by EPR oximetry in human tumorxenografts. Rad Res 155: 466 – 473
Patterson DM, Rustin GJS (2007) Vascular damaging agents. Clin Oncol 19:443 – 456
Ramirez LH, Orlowski S, An D, Bindoula G, Dzodic R, Ardouin P, Bognel C,Belehradek Jr J, Munck JN, Mir LM (1998) Electrochemotherapy on livertumours in rabbits. Br J Cancer 77(12): 2104 – 2111
Sersa G (2006a) The state-of-the-art of electrochemotherapy before theESOPE study: advantages and clinical uses. Eur J Cancer Suppl 4(11):52 – 59
Sersa G, Beravs K, Cemazar M, Miklavcic D, Demsar F (1998) Contrastenhanced MRI assessment of tumor blood volume after application ofelectric pulses. Electro-Magnetobiol 17: 299 – 306
Sersa G, Cemazar M, Miklavcic D, Chaplin DJ (1999a) Tumor blood flowmodifying effect of electrochemotherapy with bleomycin. Anticancer Res19: 4017 – 4022
Sersa G, Cemazar M, Miklavcic D, Rudolf Z (2006b) Electrochemotherapyof tumours. Radiol Oncol 40: 163 – 174
Sersa G, Cemazar M, Parkins CS, Chaplin DJ (1999b) Tumour bloodflow changes induced by application of electric pulses. Eur J Cancer 35:672 – 677
Sersa G, Krzic M, Sentjurc M, Ivanusa T, Beravs K, Kotnik V, Coer A,Swartz HM, Cemazar M (2002) Reduced blood flow and oxygenation inSA-1 tumours after electrochemotherapy with cisplatin. Br J Cancer 87:1047 – 1054
Shaked Y, Kerbel RS (2007) Antiangiogenic strategies on defense: on thepossibility of blocking rebounds by the tumor vasculature afterchemotherapy. Cancer Res 67: 7055 – 7058
Shepherd AP, Oberg PA (eds). (1990) Laser-Doppler Blood Flowmetry.Kluwer: Dordrecht
Siemann DW, Bibby MC, Dark GG, Dicker AP, Eskens FA, Horsma MR,Marme D, Lorusso PM (2005) Differentiation and definition of vascular-targeted therapies. Clin Cancer Res 11: 416 – 420
Swartz HM, Boyer S, Brown D, Chang K, Gost P, Glockner JF, Hu H, Lin KJ,Moussavi M, Nilges M, Norby SW, Smirnow A, Vahidi N, Walzcak T, WuM, Clarckson RB (1993) The use of EPR for the measurement of theconcentration of oxygen in vivo in tissues under physiologicallypertinent conditions and concentrations. In: Oxygen Transport to TissueXIV, Nemoto M and La Mana C (eds), pp. 221 – 228. New York: PlenumPress
Swartz HM, Clarkson RB (1998) The measurement of oxygen in vivo usingEPR techniques. Phys Med Biol 43: 1957 – 1975
Tozer GM, Kanthou C, Baguley BC (2005) Disrupting tumour blood vessels.Nature Rev Cancer 5: 423 – 435
Tozer GM, Prise VE, Wilson J, Cemazar M, Shan S, Dewhrist MW,Barber PR, Vojnovic B, Chaplin DJ (2001) Mechanisms associated withtumour vascular shut-down induced by combretatstatin A-4 phosphate:Intravital microscopy and measurement of vascular permeability. CancerRes 61: 6413 – 6422
Electroporation and electrochemotherapy
G Sersa et al
398
British Journal of Cancer (2008) 98(2), 388 – 398 & 2008 Cancer Research UK
Tra
nsla
tion
al
Th
era
peu
tics
Related Documents