REGULAR ARTICLE Variable responsiveness to clopidogrel and aspirin among patients with acute coronary syndrome as assessed by platelet function tests Boris Shenkman a,1 , Shlomi Matetzky b,1 , Paul Fefer b , Hanoch Hod b , Yulia Einav c , Aharon Lubetsky a , David Varon d , Naphtali Savion e, ⁎ a Amalia Biron Research Institute of Thrombosis and Hemostasis, Israel b Heart Institute, Sheba Medical Center, Tel-Hashomer, Israel c Quantitative Biology Unit, Faculty of Sciences, Holon Institute of Technology, Holon, Israel d Coagulation Unit, Hadassah Hebrew University Medical Center, Jerusalem, Israel e Goldschleger Eye Research Institute, Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel Received 19 June 2007; received in revised form 1 October 2007; accepted 22 October 2007 Available online 26 December 2007 Abstract Unresponsiveness to clopidogrel or aspirin has been reported in patients with acute coronary syndrome (ACS). Platelet aggregometry (PA) and the Impact-R [Cone and Plate(let) Analyzer (CPA) technology, measuring whole blood platelet adhesion under flow conditions] were compared in detecting laboratory unresponsiveness to clopidogrel and aspirin among ACS patients. Platelet-rich plasma (PRP) samples were evaluated in 404 patients by PA using adenosine diphosphate (ADP) and arachidonic acid (AA) and whole blood samples by the Impact-R ADP- and AA-response tests. The first cohort (n =114) was assayed by PA on days 1 and 4 of the onset of ACS. A patient with relative decrease of ≤ 10% in ADP- induced maximal platelet aggregation after clopidogrel treatment was defined as laboratory non-responding (NR) patient to clopidogrel. This relative value correlated well with an absolute value of ADP-induced aggregation ≥ 70%. A patient with an absolute value of AA-induced maximal aggregation ≥ 60% was defined as laboratory KEYWORDS Acute coronary syndrome; Platelets; Clopidogrel; Aspirin; Platelet aggregometer; Impact-R Abbreviations: ACS, acute coronary syndrome; PA, platelet aggregometry; CPA, Cone and Plate(let) Analyzer; PRP, platelet-rich plasma; ADP, adenosine diphosphate; AA, arachidonic acid; NR, non-responding; ROC, receiver operating characteristic; SC, surface coverage; PCI, percutaneous coronary intervention; VASP, vasodilator-stimulated phosphoprotein; PPP, platelet-poor plasma; PBS, phosphate-buffered saline; AUC, area under the curve; SD., standard deviation ⁎ Corresponding author. Goldschleger Eye Research Institute, Sheba Medical Center, Tel Hashomer 52621, Israel. Tel.: +972 3 5302954; fax: +972 3 5351577. E-mail address: [email protected] (N. Savion). 1 B. Shenkman and S. Matetzky contributed equally to this study. intl.elsevierhealth.com/journals/thre 0049-3848/$ - see front matter © 2007 Elsevier Ltd. All rights reserved. doi:10.1016/j.thromres.2007.10.018 Thrombosis Research (2008) 122, 336–345

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

intl.elsevierhealth.com/journals/thre
Thrombosis Research (2008) 122, 336–345
REGULAR ARTICLE
Variable responsiveness to clopidogrel and aspirinamong patients with acute coronary syndrome asassessed by platelet function tests
Boris Shenkman a,1, Shlomi Matetzky b,1, Paul Fefer b, Hanoch Hod b,Yulia Einav c, Aharon Lubetsky a, David Varon d, Naphtali Savion e,⁎
a Amalia Biron Research Institute of Thrombosis and Hemostasis, Israelb Heart Institute, Sheba Medical Center, Tel-Hashomer, Israelc Quantitative Biology Unit, Faculty of Sciences, Holon Institute of Technology, Holon, Israeld Coagulation Unit, Hadassah Hebrew University Medical Center, Jerusalem, Israele Goldschleger Eye Research Institute, Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel
Received 19 June 2007; received in revised form 1 October 2007; accepted 22 October 2007Available online 26 December 2007
Abbreviations: ACS, acute coronarplasma; ADP, adenosine diphosphate;coverage; PCI, percutaneous coronaryphosphate-buffered saline; AUC, area⁎ Corresponding author. Goldschleger
fax: +972 3 5351577.E-mail address: [email protected]
1 B. Shenkman and S. Matetzky contr
0049-3848/$ - see front matter © 200doi:10.1016/j.thromres.2007.10.018
Abstract
Unresponsiveness to clopidogrel or aspirin has been reported in patients with acutecoronary syndrome (ACS). Platelet aggregometry (PA) and the Impact-R [Cone andPlate(let) Analyzer (CPA) technology, measuring whole blood platelet adhesion underflow conditions] were compared in detecting laboratory unresponsiveness toclopidogrel and aspirin among ACS patients.Platelet-rich plasma (PRP) samples were evaluated in 404 patients by PA usingadenosine diphosphate (ADP) and arachidonic acid (AA) and whole blood samples bythe Impact-R ADP- and AA-response tests. The first cohort (n=114) was assayed by PAon days 1 and 4 of the onset of ACS. A patient with relative decrease of ≤10% in ADP-induced maximal platelet aggregation after clopidogrel treatment was defined aslaboratory non-responding (NR) patient to clopidogrel. This relative value correlatedwell with an absolute value of ADP-induced aggregation ≥70%. A patient with anabsolute value of AA-induced maximal aggregation ≥60% was defined as laboratory
KEYWORDSAcute coronarysyndrome;Platelets;Clopidogrel;Aspirin;Platelet aggregometer;Impact-R
y syndrome; PA, platelet aggregometry; CPA, Cone and Plate(let) Analyzer; PRP, platelet-richAA, arachidonic acid; NR, non-responding; ROC, receiver operating characteristic; SC, surfaceintervention; VASP, vasodilator-stimulated phosphoprotein; PPP, platelet-poor plasma; PBS,
under the curve; SD., standard deviationEye Research Institute, Sheba Medical Center, Tel Hashomer 52621, Israel. Tel.: +972 3 5302954;
c.il (N. Savion).ibuted equally to this study.
7 Elsevier Ltd. All rights reserved.

337Response to clopidogrel and aspirin in ACS patients
NR patient to aspirin. The second cohort (n=290) was tested on day 4 by both systemsand results analyzed by receiver operating characteristic curve. The following cut-offvalues of the Impact-R surface coverage were obtained: ≤2.8% and ≤3.4% forclopidogrel and aspirin NR patients, respectively. The incidence of NR patients toclopidogrel and aspirin, according to the two methods was 27% and 22%, respectively.Impact-R compared to PA in detecting clopidogrel and aspirin NR patients revealed: 79%and 82% agreement, 71% and 73% sensitivity, 83% and 86% specificity, respectively. Inconclusion, the Impact-R and PA results demonstrated high degree of similarity.© 2007 Elsevier Ltd. All rights reserved.
Figure 1 Impact-R [cone and plate(let) analyzer (CPA)]protocol. Whole blood (130 μL) is placed in a polystyrene welland subjected to flow (1800 s−1 for 2min) using a rotating cone.The well is washed and stained with the May–Gruenwald stain.Platelet adhesion (surface coverage, %) is evaluated by animage analysis system connected to the Impact-R device.
Introduction
Treatment with clopidogrel and aspirin has become apart of the standard anti-platelet therapy ofpatients with acute coronary syndrome (ACS) andof patients undergoing percutaneous coronary inter-vention (PCI) [1–3]. However, their response to theanti-platelet drugs is not uniform and some are non-responding (NR) to a specific drug [4–7]. Generally,the term NR patient is used when the drug does notfulfill its pharmacological target, i.e., inability toinhibit platelet response to the correspondingagonist. In preliminary small-scale studies, bothlaboratory aspirin and clopidogrel unresponsivenesswere associated with increased risk of recurrentatherothrombotic events and thrombotic complica-tions after coronary intervention [4,8]. A recentmeta-analysis study indicates a correlation oflaboratory defined “aspirin resistance”with a higherrisk of recurrent cardiovascular events [9]. Thedefinition of NR patients is not standardized, despitethe clinical significance of this phenomenon.
The laboratory methods used to define NRpatients to anti-platelet drugs may include plateletaggregation (PA) [10,11], PFA-100 measuring theocclusion time of a membrane pore coated withcollagen and platelet agonists under flow condition[12,13], Ultegra—VerifyNow measuring platelet-induced agglutination of fibrinogen-coated beads(13), measuring clopidogrel effect on ADP-inducedreduction of cyclic AMP or cyclic AMP-dependentphosphorylation of vasodilator-stimulated phospho-protein (VASP) [14–16], and detecting the effect ofthe drug on platelet activation markers measuredby flow cytometry [10,11,17–19]. Comparativestudies using different methods to establish drugNR patients showed non-sufficient agreementbetween different methods. A comparative studythat detected the incidence of aspirin NR patientsby PA, PFA-100 and Ultegra—VerifyNow in patientswho had a stroke found poor agreement betweenthe tests and very few NR patients were determinedby all three tests [13]. In another study, theinhibition of platelet aggregation in clopidogrel-treated healthy volunteers correlated with phos-
phorylation of VASP measured by enzyme immu-noassay and flow cytometry but did not correlatewith either P-selectin expression or PFA-100 closuretime [12]. Furthermore, a moderate positive corre-lation was found between the results of PA and
338 B. Shenkman et al.
activation-dependent receptor expression as assessedby flow cytometry after clopidogrel was adminis-tered [11]. As a result, the reported incidence ofclopidogrel and aspirin NR patients varied from 5% to60% [4,6,11,13,20,21].
Recently, we used the Impact-R device, whichmeasured platelet adhesion in whole blood underdefined flow condition (1800 s−1), to evaluate,in vitro, the response to aspirin and 2-Methylthioa-denosine 5'-monophosphate triethylammonium salt(2MeSAMP), a P2Y12 inhibitor [22]. In the presentstudy, two methods were applied and compared, PAand the Impact-R, to detect NR patients to clopido-grel and aspirin among ACS patients undergoing PCI.
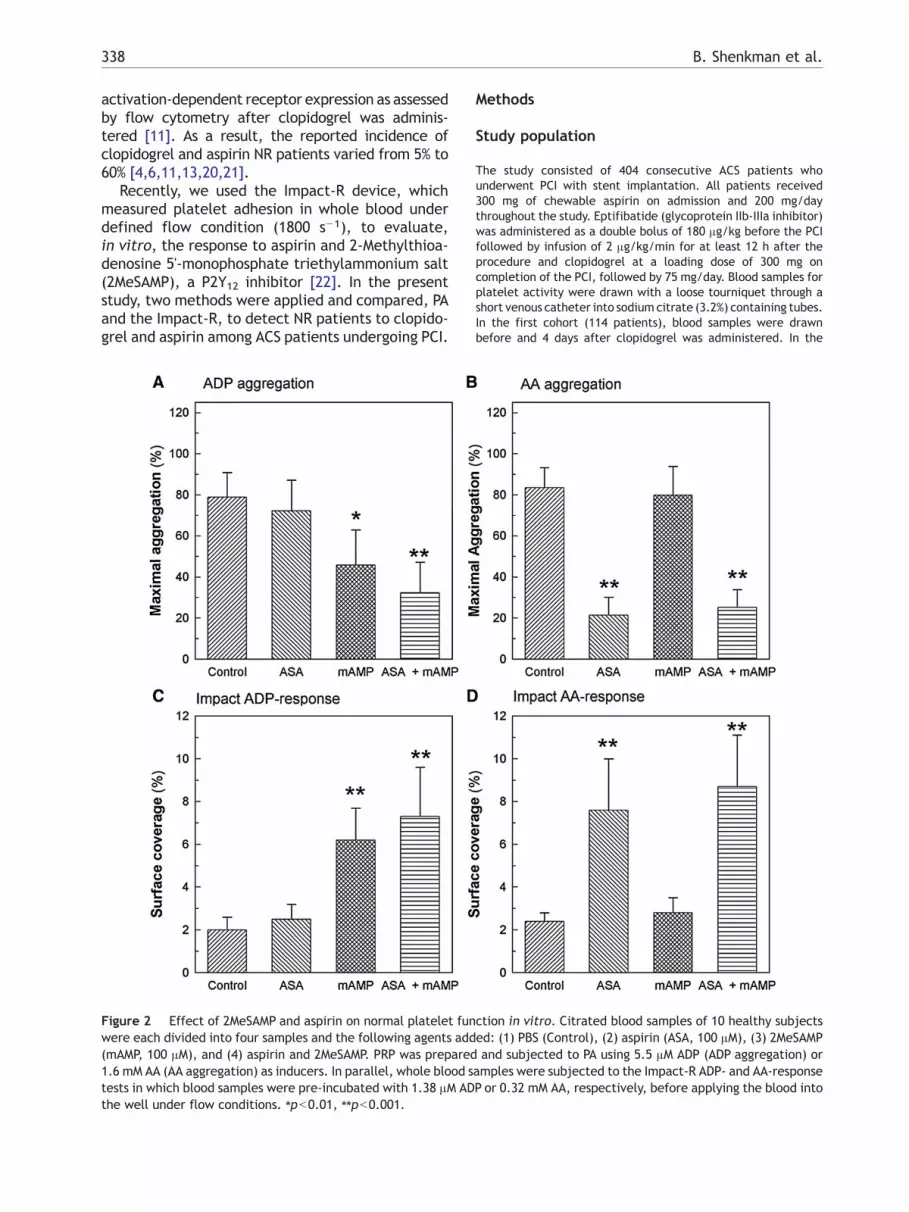
Figure 2 Effect of 2MeSAMP and aspirin on normal platelet funwere each divided into four samples and the following agents add(mAMP, 100 μM), and (4) aspirin and 2MeSAMP. PRP was prepared1.6 mM AA (AA aggregation) as inducers. In parallel, whole blood stests in which blood samples were pre-incubated with 1.38 μM ADthe well under flow conditions. ⁎pb0.01, ⁎⁎pb0.001.
Methods
Study population
The study consisted of 404 consecutive ACS patients whounderwent PCI with stent implantation. All patients received300 mg of chewable aspirin on admission and 200 mg/daythroughout the study. Eptifibatide (glycoprotein IIb-IIIa inhibitor)was administered as a double bolus of 180 μg/kg before the PCIfollowed by infusion of 2 μg/kg/min for at least 12 h after theprocedure and clopidogrel at a loading dose of 300 mg oncompletion of the PCI, followed by 75 mg/day. Blood samples forplatelet activity were drawn with a loose tourniquet through ashort venous catheter into sodium citrate (3.2%) containing tubes.In the first cohort (114 patients), blood samples were drawnbefore and 4 days after clopidogrel was administered. In the
ction in vitro. Citrated blood samples of 10 healthy subjectsed: (1) PBS (Control), (2) aspirin (ASA, 100 μM), (3) 2MeSAMPand subjected to PA using 5.5 μM ADP (ADP aggregation) or
amples were subjected to the Impact-R ADP- and AA-responseP or 0.32 mM AA, respectively, before applying the blood into

Figure 3 ADP- and AA-induced platelet aggregation.Platelet aggregation was assayed in normal subjects (n=36)and ACS patients (cohort 1, n=114) on day 1 (under aspirin)and day 4 after hospitalization (under both aspirin andclopidogrel). Maximal aggregation is presented.
339Response to clopidogrel and aspirin in ACS patients
second cohort (290 patients), blood samples were assayed once,4 days after initial clopidogrel treatment. Normal volunteers(n=36) age- and gender-matched to the patients (from 40 to66 years old), who did not receive any anti-platelet drug at least10 days prior to blood collection, served as a control group.
Turbidimetric platelet aggregometry
Blood samples were centrifuged (140 g for 12 min) and the upperfraction was collected as the platelet-rich plasma (PRP). Theremaining blood was centrifuged again (1660 g for 12 min) toobtain platelet-poor plasma (PPP). The platelet count wasmeasured in PRP and adjusted to 2–2.5×108/ml with PPP.Platelet aggregation was evaluated by a turbidimetric PACKS-4aggregometer (Helena Laboratories, Beaumont, Texas) usingadenosine diphosphate (ADP, 5.5 μM) and arachidonic acid (AA,1.6 mM) as platelet agonists.
Impact-R test
The Impact-R device (DiaMed, Cresier, Switzerland) is based onthe cone and plate(let) analyzer (CPA) technology [23–25].Briefly, the whole blood sample (130 μl) is placed in a polystyrenewell and subjected to flow (1800 s−1 for 2 min) using a rotatingcone (Fig. 1). The well is washed and stained with the May–Gruenwald stain. Platelet deposition is evaluated by the Impact-R image analysis system. Platelet adhesion, surface coverage(SC,%) of adherent platelet particles including single plateletsand aggregates, is measured.
ADP- and AA-response tests: Pre-incubation of whole bloodwith ADP or AA at sub-optimal concentrations (1.38 μM and0.32 mM, respectively) for 1 min under gentle mixing (10 RPM)prior to the Impact-R test leads to platelet activation and micro-aggregates formation in the tube resulting in reduced plateletadhesion as reflected by reduced SC [26]. The reduction isattenuated in samples from patients treated by and respondingwell to the appropriate anti-platelet drug, clopidogrel or aspirin,while full reduction is observed with platelets from NR patients.
Treatment of normal platelet by aspirinand 2MeSAMP
Citrated blood samples of 10 healthy volunteers were treated withphosphate-buffered saline (PBS); aspirin (100 μM); 2MeSAMP(100 μM; Sigma, St. Louis, MO); or aspirin and 2MeSAMP. PRP wasprepared and platelet aggregation tests were performed using5.5 μM ADP or 1.6 mM AA as agonists. Additionally, whole bloodsampleswere subjected to the Impact-RADP- andAA-response tests.
Statistical analysis
Impact-R ADP-response test results were log-transformed toaccount for its skewed distribution. Pearson correlation was usedto determine the correlation between the results of aggregationinduced by ADP and the results of the Impact-R ADP-responsetest. The distribution of AA-induced aggregation was bimodal;therefore, the PA results were analyzed as a categorial variablewith two groups: maximal aggregation b60% and N60%. Mann–Whitney non-parametric test for independent samples was usedto study the relation between the PA results and the Impact-Rresults. ROC curve analysis was used to identify the Impact-R cut-off values (% SC) according to the defined PA cut-off values of≥70% and ≥60% for ADP- and AA-induced aggregation, respec-tively, and to determine the sensitivity and specificity of the
Impact-R for detecting clopidogrel and aspirin NR patients. Thenon-parametric estimate of area under the curve (AUC) wascalculated according to the Wilcoxon rank-sum test as a summarymeasure of Impact-R diagnostic accuracy to the determination ofdrug NR. The mean±SD was presented for normally distributedvariables and median (25th percentile–75th percentile) waspresented for non-normally distributed variables. pb0.05 wasconsidered statistically significant.
Results
Effect of aspirin and 2MeSAMP on normal plateletfunction in vitro
ADP-induced platelet aggregationPre-treatment of PRP with 2MeSAMP reduced maximal aggrega-tion (45.8±17.1% vs. 78.9±11.9%; pb0.01) that was furtherreduced by addition of aspirin (32.3±15.0%; pb0.001) (Fig. 2A).Pre-treatment with aspirin alone did not influence the ADP-induced maximal aggregation (72.2±15.0%; pN0.05).

340 B. Shenkman et al.
AA-induced platelet aggregationPre-treatment of PRP with aspirin reduced maximal aggregation(21.4±8.7% vs. 83.5±9.8%; pb0.001) that was unaffected byaddition of 2MeSAMP (25.3±8.5%) (Fig. 2B). Pre-treatment with2MeSAMP alone did not affect maximal aggregation in response toAA (79.8±14.0%; pN0.05).
Impact-R ADP-response testPre-treatment of blood with 2MeSAMP increased SC (6.2±1.5% vs.2.0±0.6%; pb0.001) that was further increased by addition ofaspirin (7.3±2.3%) (Fig. 2C). Pre-treatment with aspirin alone didnot influence the ADP-response SC (2.5±0.7%; pN0.05).
Impact-R AA-response testPre-treatment of blood with aspirin increased SC (7.6±2.4% vs.2.4±0.4%; pb0.001) that was unaffected by addition of 2MeSAMP(7.3±2.3%) (Fig. 2D). Pre-treatment with 2MeS-AMP alone did notinfluence the AA-response SC (2.5±0.7%; pN0.05).
Patients' response to clopidogrel and aspirin
Patients of the first cohort (n=114) were tested twice by PA:after taking aspirin (day 1), and under both clopidogrel andaspirin treatment (day 4). As a control, the blood of 36 normalsubjects who did not receive anti-platelet drugs was assayed. Atday 1, the ADP-induced maximal aggregation of ACS patients wassimilar to normal subjects (80.0±8.3% vs. 80.7±11.5%) (Fig. 3),but was significantly lower under clopidogrel treatment (day 4)(55.0±22.4%, pb0.01). AA-induced maximal aggregation wassignificantly lower at day 1 compared to normal subjects'reflecting aspirin effect, and remained at a similar level at day4 (55.0±24.0% and 43.4±31.3% vs. 87.5±8.8%, pb0.01).
Cut-off values of ADP- and AA-inducedmaximal aggregation for detection of NR patientsto anti-platelet drugs
The difference in percentage of ADP-induced maximal aggrega-tion in cohort 1 between days 1 and 4, i.e., before and under
Figure 4 Regression analysis between post-clopidogrel ADP-indADP-induced maximal aggregation. Significant correlation betweeof ≤10% correlates to maximal aggregation of ≥70% at post-clop
clopidogrel treatment, correlated well with maximal aggregationat day 4 (Fig. 4). Based on this correlation and the cut-off valuefor clopidogrel laboratory NR patients as a change in maximalaggregation ≤10% accepted by others [21,27], a cut-off value ofmaximal aggregation ≥70% at day 4 was established. This newcut-off value allowed the evaluation of clopidogrel NR patientson the basis of a single assay of a clopidogrel-treated patient.
Establishment of a cut-off value for aspirin laboratory NRpatients based on a difference in AA-maximal aggregation betweenpre- and post-aspirin treatment could not be carried out sincemostof the patients were already taking aspirin before admission to thehospital. Therefore, the cut-off value for aspirin NR patients wasestablished based on the results of the normal (untreated)volunteers [22]. The extent of AA aggregation in the cohort wasbimodal distributed. The AA-induced maximal aggregation was87.5±8.8%. Therefore, the AA-induced maximal aggregation≥60%, representing mean minus three standard deviations of thisvalue, was considered as a cut-off value for aspirin NR patients.
Correlation between Impact-R ADP- andAA-response test and ADP- and AA-induced PA
Due to the skewed distribution of the Impact-R ADP-response testresults were log transformed. Pearson correlation was used todetermine the correlation between Impact-R and PA results (Fig.5A). Linear regression analysis revealed R2=0.39 (pb0.001).Since the distribution of AA-induced aggregation is bimodal, thePA results were analyzed as a categorical variable with twogroups: maximal aggregation b60% and ≥60% (Fig. 5B). Mann–Whitney non-parametric test for independent samples was usedto study the relation between the results of the PA and theImpact-R. In the AA-response test, the Impact-R results (% SC)corresponding to the two PA groups were: [median (25thpercentile-75th percentile)] 5.7(4.3–7.0) and 2.9(2.1–3.5),respectively (pb0.001).
Determination of Impact-R cut-off values for NRpatients by ROC analysis
The ADP- and AA-induced aggregation and the Impact-R ADP- andAA-response tests of cohort 2 were subjected to ROC curve
uced maximal aggregation and clopidogrel-induced change inn these parameters is presented and a change in aggregationidogrel treatment.

Figure 5 Correlation between Impact-R and PA results.(A) Impact-R ADP-response test and ADP-induced PA. Data ofImpact-R ADP-response test were log-transformed to accountfor their skewed distribution. Pearson correlation was used todetermine correlation between ADP-response test (% SC) andADP-induced PA (% maximal aggregation) after clopidogreltreatment. Linear regression and 95% confidence intervalare shown. The linear regression revealed R2=0.39, pb0.001.(B) Impact-R AA-response test and AA-induced PA. Distribu-tion of the AA-induced PA was bimodal. Thus, this measurewas analyzed as a categorical variable with two groups: b60%and ≥60%. Box-plot distribution of surface coverage in thetwo groups of maximal aggregation is shown. Each box-plotrepresents different percentiles (from bottom to top: 0, 25th,50th, 75th, 100). The 50th percentile represents the median;the mean is represented by a star. Mann–Whitney non-parametric test for independent samples was used to studythe relation between Impact-R and PA results in determina-tion of the responsiveness to aspirin. pb0.001.
341Response to clopidogrel and aspirin in ACS patients
analysis. The ROC analysis was used to evaluate the sensitivityand specificity of all possible Impact-R thresholds for detectingaspirin and clopidogrel responsiveness using PA cut-offs of b60%and b70% maximal aggregation for AA- and ADP-inducedaggregation, respectively (Fig. 6). The non-parametric estimateof area under curve (AUC), according to the Wilcoxon rank-sumtest, was calculated as a summary measure of Impact-R
diagnostic accuracy to responsiveness to the drugs. The valuesof AUC were 0.867 (clopidogrel) and 0.871 (aspirin). The optimalSC cut-off values of the Impact-R ADP- and AA-response test of≤2.8% and ≤3.4%, respectively, were chosen. Table 1 shows thesensitivity, specificity and positive and negative predictive valueparameters found for the Impact-R versus the PA tests forclopidogrel and aspirin NR patients.
Agreement between PA and Impact-R tests inevaluating the laboratory response to clopidogreland aspirin
Based on the established cut-off values of the response toclopidogrel and aspirin, the results obtained from cohort 2 weredivided into four boxes (Fig. 7). Boxes A and D representresponding and NR patients, respectively according to bothmethods used. Boxes B and C represent patients withoutagreement between the two methods. Table 2 summarizes theresults showing the percentage and number of patients in eachgroup. The summarized agreement (responding plus NR patients)between PA and Impact-R was 79% and 82% for clopidogrel andaspirin response, respectively. According to both methods, 33% ofpatients were defined as NR to clopidogrel, 30% NR to aspirin, and18% NR to both drugs.
Discussion
In patients with cardiovascular diseases, no or poorresponse to clopidogrel and aspirin, as detected bylaboratory methods, may be an important clinicalentity that could predict recurrent atherothrombo-tic events. Recently, we reported an increased riskof vascular re-occlusion among clopidogrel NRpatients with acute coronary syndrome as testedby ADP-induced platelet aggregation [8]. Similarly,others have shown a higher incidence of stentthrombosis among NR patients treated by clopido-grel and/or aspirin [28–31]. In a meta-analysis,patients identified as having “laboratory aspirinresistance” were more likely to have “clinical resis-tance” to aspirin due to their higher risk of recur-rent cardiovascular events compared with patientsidentified as “laboratory aspirin sensitive” (oddsratio of all outcomes was 3.8) [9]. However, thelaboratory entity of responding versus NR patientsto anti-platelet drugs is poorly standardized. More-over, several unresolved questions arise from thegrowing literature regarding NR patients to clopido-grel and aspirin.
The first problem is the insufficient agreementbetween different platelet function tests used toobserve the determination of NR patients toclopidogrel and aspirin [12,13]. In the presentstudy, laboratory criteria were established withthe use of the PA and Impact-R devices. For thispurpose, Impact-R ADP- and AA-response tests wereused in which the modulation of whole bloodplatelet adhesion under flow by sub-optimal dosesof ADPor AA, respectively, was tested in vitro. When

Figure 6 Receiver operating characteristic (ROC) analysis. Evaluation of sensitivity and specificity of all possible Impact-Rthresholds for detecting clopidogrel (A) and aspirin (B) responsiveness (using ADP-induced aggregation b70% and AA-inducedaggregation b60% as the criterion standard, respectively). Results obtained from cohort 2 patients were included. The non-parametric estimate of area under curve (AUC) was calculated according to the Wilcoxon rank-sum test. The AUC was 0.867(clopidogrel) and 0.871 (aspirin). Optimal cut-off values of SC ≤2.8% and ≤3.4% were found for Impact-R ADP- and AA-responsetests, respectively.
Table 1 Parameters of Impact-R versus PA tests in thedetermination of clopidogrel and aspirin response
Clopidogrel (%) Aspirin (%)
Cut-off value ≤2.8 ≤3.4Sensitivity 71 73Specificity 83 86Positive predict value 72 70Negative predict value 83 88
Values derived from data presented in Fig. 6.
342 B. Shenkman et al.
patients respondedwell to the appropriate drug, theaddition of the corresponding agonist to the bloodsample attenuated the reduction of platelet adhe-sion by the agonist while full reduction was recordedin NR patients. Using the PA results as a “goldstandard”, the results of this study demonstrate thefollowing degree of sensitivity (71% and 73%),specificity (83% and 86%), positive (72% and 70%)and negative (83% and 88%) predictive values for theImpact-R ADP- and AA-response tests in detectingclopidogrel and aspirin NR patient, respectively. Theagreement between the two tests was 79% and 82%in NR patients, respectively.
The second problem is the need for selectivedetection of clopidogrel and aspirin NR patients inindividuals receiving these drugs. The results of thecurrent study suggest that the cross-relationshipbetween the biochemical effects of 2MeSAMP, thep2Y12 inhibitor and aspirin on platelet activity waseither negligible (minimal decrease in the responseto ADP in aspirin-treated blood) or absent (no changein AA effect in 2MeSAMP-treated blood), at leastin vitro. This is in compliance with a previous
study in which high concentrations of ADP inducedfull platelet aggregation independent of thrombox-ane A2 production [6]. Furthermore, ADP does notinduce thromboxane A2 production in human plate-lets [32].
These observations should be confirmed in ACSNR patients, where unresponsiveness to each drugmay represent a state of high thrombo-inflamma-tory response. These responses may include tran-sient “by-passing” signaling pathways that could beinhibited by the addition of another drug, thus
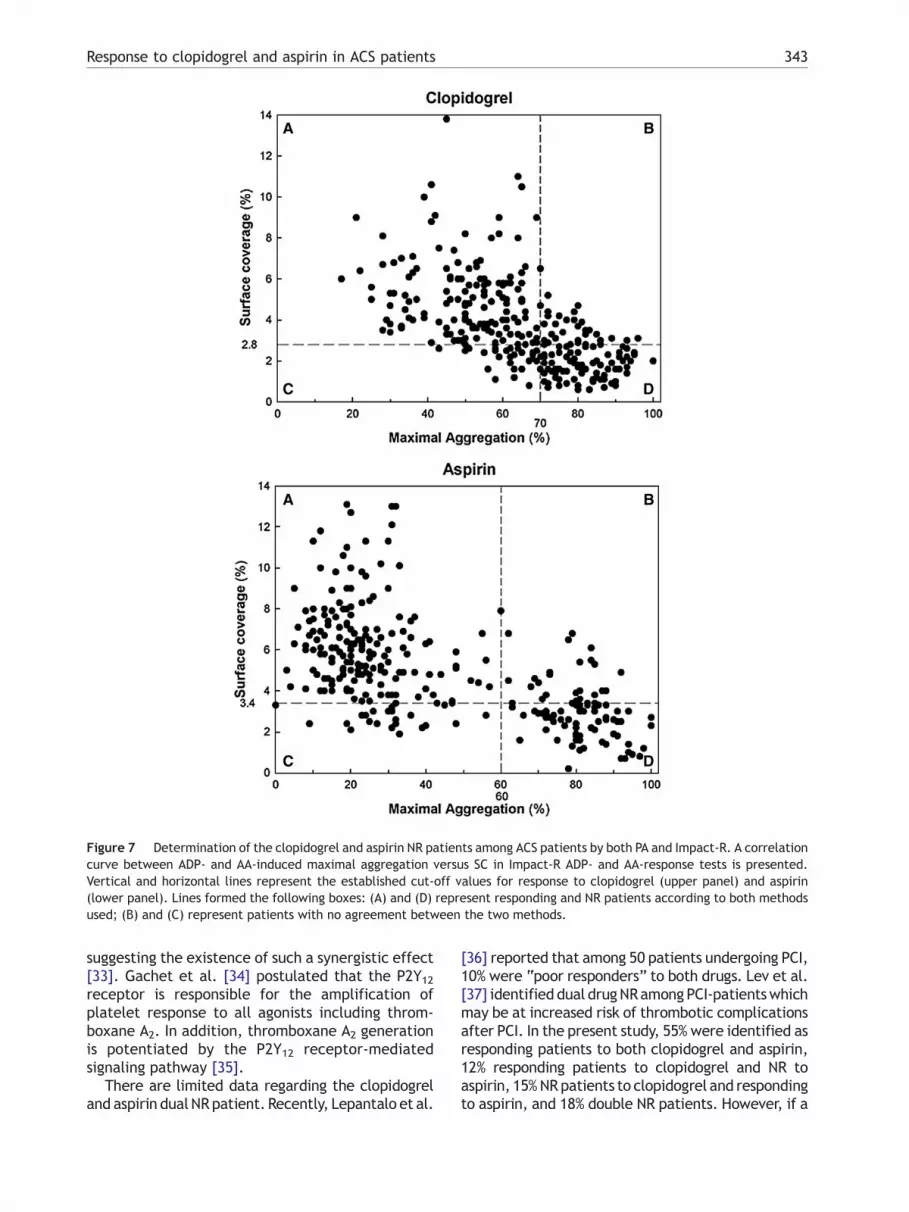
Figure 7 Determination of the clopidogrel and aspirin NR patients among ACS patients by both PA and Impact-R. A correlationcurve between ADP- and AA-induced maximal aggregation versus SC in Impact-R ADP- and AA-response tests is presented.Vertical and horizontal lines represent the established cut-off values for response to clopidogrel (upper panel) and aspirin(lower panel). Lines formed the following boxes: (A) and (D) represent responding and NR patients according to both methodsused; (B) and (C) represent patients with no agreement between the two methods.
343Response to clopidogrel and aspirin in ACS patients
suggesting the existence of such a synergistic effect[33]. Gachet et al. [34] postulated that the P2Y12receptor is responsible for the amplification ofplatelet response to all agonists including throm-boxane A2. In addition, thromboxane A2 generationis potentiated by the P2Y12 receptor-mediatedsignaling pathway [35].
There are limited data regarding the clopidogreland aspirin dual NRpatient. Recently, Lepantalo et al.
[36] reported that among 50 patients undergoing PCI,10% were “poor responders” to both drugs. Lev et al.[37] identified dual drugNRamong PCI-patientswhichmay be at increased risk of thrombotic complicationsafter PCI. In the present study, 55% were identified asresponding patients to both clopidogrel and aspirin,12% responding patients to clopidogrel and NR toaspirin, 15%NRpatients to clopidogrel and respondingto aspirin, and 18% double NR patients. However, if a

Table 2 Agreement between PA and Impact-R test
The degree of response and non-response (NR) to clopidogrel(A) and aspirin (B) was determined by the Impact-R and PA in290 patients of cohort 2 and the data is presented as % andabsolute numbers (in parenthesis) of patients in each group.The values presented in the table are derived from the datapresented in Fig. 7.
344 B. Shenkman et al.
patient is NR for one drug, the odds ratio of being NRfor the two drugs was 5.
The third problem is whether the determinationof a drug NR patient needs two assays: before andunder drug therapy, or can it be established on thebasis of one under-treatment assay. Despite the factthat the first approach was thought to be mandatoryor at least of significant importance [6,38], there aredisadvantages: the absolute level of platelet reac-tivity is not considered, and unsuitable for patientswho are chronically treated with a drug, and forpatients urgently treated on admission to thehospital. Recent studies suggest that testing drugresponse by one under-treatment assay may be abetter parameter to predict thrombotic risk than thedifference between the pre- and under-treatmentassays [3,39]. In the present study, the delta-residual aggregation as≤10% change in ADP-inducedaggregation accepted by others [5,21,37], was usedas an initial point, which correlated well to the valueof absolute aggregation when testing patients underclopidogrel treatment according to linear regressionanalysis. This allowed a cut-off value for the secondparameter to be established. Thus, a clopidogrel NRpatient was defined as having maximal ADP-inducedaggregation ≥70% after clopidogrel loading, whichwas used to determine NR patients among the 290ACS patients. However, this approachwas unsuitablefor detection of NR to aspirin, since both the first andsecond assays were performed under treatment withaspirin. Therefore, the AA-induced aggregation,≥60%, was defined as a cut-off level of aspirin NR,based on the level of AA-induced aggregation innormal subjects.
To check the degree of correlation between PAand Impact-R results, different approaches were
taken for ADP- and AA-related tests. Due to theskewed distribution of the Impact-R ADP-responsetest, the Pearson correlation was used to determinethe correlation between PA and Impact-R. However,due to the bimodal distribution of response to AA inPA, this parameter was analyzed as a categoricalvariable with two groups: b60% and ≥60% maximalaggregation.
Application of the established cut-off values forplatelet aggregation and the results of the AA- andADP-response tests of cohort 2 to ROC analysisprovided the following optimal cut-off parametersfor NR patients in the Impact-R tests: SC ≤3.4%(aspirin) and ≤2.8% (clopidogrel).
In conclusion, a correlation between Impact-Rand routine PA was found in the detection of NRpatients to clopidogrel and aspirin in the group ofacute coronary syndrome patients.
Acknowledgement
The authors thank S. Kotev-Emeth for technicalassistance. The study was partially supported byDiaMed (Cresier, Switzerland).
Disclosure: D. Varon and N. Savion are thefounders of the Company developing the Impact-Rtechnology.
References
[1] Mehta SR, Yusuf S, Peters RJG, Bertrand ME, Lewis BS,Natarjan MK, et al. Effects of pretreatment with clopidogreland aspirin followed by long-term therapy in patientsundergoing percutaneous coronary intervention: the PCI-CURE study. Lancet 2001;358:527–33.
[2] Steinhubl SR, Berger PB, Mann 3rd JT, Fry ET, DeLago A,Wilmer C, et al. CREDO investigators. Clopidogrel for thereduction of events during observation. Early and sustaineddual oral antiplatelet therapy following percutaneouscoronary intervention: a randomized controlled trial.JAMA 2002;288:2411–20.
[3] Cuisset T, Frere C, Quilici J, Barbou F, Morange PE, HovasseT, et al. High post-treatment platelet reactivity identifiedlow-responders to dual antiplatelet therapy at increasedrisk of recurrent cardiovascular events after stenting foracute coronary syndrome. J Thromb Haemost 2006;4:542–9.
[4] Gum PA, Kottke-Marchant K, Welsh PA, White J, Topol EJ. Aprospective, blinded determination of the natural history ofaspirin resistance among stable patients with cardiovascu-lar disease. J Am Coll Cardiol 2003;41:961–5.
[5] Gurbel PA, Bliden KP, Hiatt BL, O'Connor CM. Clopidogrel forcoronary stenting: response variability, drug resistance, andthe effect of pretreatment platelet reactivity. Circulation2003;107:2908–13.
[6] Cattaneo M. Aspirin and clopidogrel: efficacy, safety, andthe issue of drug resistance. Arterioscler Thromb Vasc Biol2004;24:1980–7.
[7] Sanderson S, Emery J, Baglin T, Kinmonth AL. Narrativereview: aspirin resistance and its clinical implication. AnnIntern Med 2005;142:370–80.
345Response to clopidogrel and aspirin in ACS patients
[8] Matetzky S, Shenkman B, Guetta V, Shechter M, Bienart R,Goldenberg I, et al. Clopidogrel resistance is associatedwith increased risk of recurrent atherothrombotic events inpatients with acute myocardial infarction. Circulation2004;109:3171–5.
[9] Snoep JD, Hovens MMC, Eikenboom JCJ, van der Bom JG,Huisman MV. Association of laboratory defined aspirinresistance with a higher risk of recurrent cardiovascularevents. Arch Intern Med 2007;167:1593–9.
[10] Gurbel PA, Kevin PB. Durability of platelet inhibition byclopidogrel. Am J Cardiol 2003;91:1123–5.
[11] Serebruany VL, Steinhubl SR, Berger PB, Malinin AI, BhattDL, Topol EJ. Variability in platelet responsiveness toclopidogrel among 544 individuals. J Am Coll Cardiol2005;45:246–51.
[12] Geiger J, Teichmann L, Grossmann R, Aktas B, SteigerwaldU, Walter U, et al. Monitoring of clopidogrel action:comparison of methods. Clin Chem 2005;51:957–65.
[13] Harrison P, Segal H, Balsbery K, Furtado C, Silber L, RothwellPM. Screening for aspirin responsiveness after transientischaemic attack and stroke. Comparison of 2-point-of-care-platelet function tests with optical aggregometry.Stroke 2005;36:1001–5.
[14] Mills DC, Puri R,HuCJ,Minniti C, GranaG, FreedmanMD, et al.Clopidogrel inhibits the binding of ADP analogues to thereceptor mediating inhibition of platelet adenylate cyclase.Arterioscler Thromb 1992;12:430–6.
[15] Barragan P, Bouvier JL, Roquebert PO, Nacaluso G,Commeau P, Cornet B, et al. Resistance to thienopyridines:clinical detection of coronary stent thrombosis by monitor-ing of vasodilator-stimulated phosphoprotein phosphoryla-tion. Catheter Cardiovasc Interv 2003;59:295–302.
[16] Aleil B, Ravanat C, Cazenave JP, Rochoux G, Heitz, GachetC. Flow cytometric analysis of intraplatelet VASP phosphor-ylation for the detection of clopidogrel resistance inpatients with ischemic cardiovascular diseases. J ThrombHaemost 2005;3:85–92.
[17] Jaremo P, Lindahl TL, Fransson SG, Richter A. Individualvariations of platelet inhibition after loading doses ofclopidogrel. J Intern Med 2002;252:233–8.
[18] Seyfarth HJ, Koksch M, Roethig C, Rother T, Neugebauer A,Klein N, et al. Effect of 300- and 450-mg clopidogrel loadingdoses on membrane and soluble P-selectin in patientsundergoing coronary stent implantation. Am Heart J2002;143:118–23.
[19] Quinn MJ, Bhatt DL, Zidar F, Vivekananthan D, Chew DP, EllisSG, et al. Effect of clopidogrel pretreatment on inflamma-tory marker expression in patients undergoing percutaneouscoronary intervention. Am J Cardiol 2004;93:679–84.
[20] Eikelboom JW, Hankey CJ. Failure of aspirin to preventatherothrombosis: potential mechanisms and implicationsfor clinical practice. Am J Cardiovasc Drugs 2004;4:57–67.
[21] Lau WC, Gurbel PA, Watkins PB, Neer CJ, Hopp AS, CarvilleDG, et al. Contribution of hepatic cytochrome P450 3A4metabolic activity to the phenomenon of clopidogrelresistance. Circulation 2004;109:166–71.
[22] Spectre G, Brill A, Gural A, Shenkman B, Touretsky N,Mosseri E, et al. A new point-of-care method for monitoringanti-platelet therapy: application of the cone and plate(let)analyzer. Platelets 2005;16:293–9.
[23] Varon D, Dardik R, Shenkman B, Kotev-Emeth S, Farzame N,Tamarin I, et al. A new method for quantitative analysis ofwhole blood platelet interaction with extracellular matrixunder flow conditions. Thromb Res 1997;85:283–94.
[24] Varon D, Lashevski I, Brenner B, Beyar R, Lanir N, Tamarin I,et al. Cone and plate(let) analyzer: monitoring glycoproteinIIb/IIIa antagonists and von Willebrand disease replacementtherapy by testing platelet deposition under flow condi-tions. Am Heart J 1998;135:S187–93.
[25] Shenkman B, Savion N, Dardik R, Tamarin I, Varon D. Testingof platelet deposition on polystyrene surface under flowconditions by the cone and plate(let) analyzer: role ofplatelet activation, fibrinogen and von Willebrand factor.Thromb Res 2000;99:353–3561.
[26] Savion N, Shenkman B, Tamarin I, Dardik R, Frojmovic M,Varon D. Transient adhesion refractoriness of circulatingplatelets under shear stress: the role of partial activationand microaggregate formation by suboptimal ADP concen-tration. Br J Haematol 2001;112:1055–61.
[27] Gurbel PA, Bilden KP, Hayes KM, Yoho JA, Herzog WR, TantryUS. The relation of dosing to clopidogrel responsiveness andthe incidence of high post-treatment platelet aggregationin patients undergoing coronary stenting. J Am Coll Cardiol2005;45:1392–6.
[28] Sane DC, McKee SA, Malinin AI, Serebruany VL. Frequency ofaspirin resistance in patients with congestive heart failuretreated with antecedent aspirin. Am J Cardiol 2002;90:893–5.
[29] Eikelboom JW, Hankey GJ. Aspirin resistance: a newindependent predictor of vascular events? J Am Coll Cardiol2003;41:966–8.
[30] Yilmaz MB, Balbay Y, Caldir V, Ayaz S, Guray Y, Guray U, et al.Late saphenous vein graft occlusion in patients withcoronary bypass: possible role of aspirin resistance.Thromb Res 2005;115:25–9.
[31] Galvani M. High postclopidogrel platelet reactivity in non-ST-elevation acute coronary syndrome treated with stent-ing: a clue for adverse prognosis? J Thromb Haemost2006;4:536–8.
[32] Cattaneo M, Gachet C, Cazenave JP, Packham MA. Adeno-sine diphosphate (ADP) does not induce thromboxane A2generation in human platelets. Blood 2002;99:3668–9.
[33] Abdelrahman N, Brill A, Touretsky N, Mosseri E, Mosseri M,Varon D. High rate of aspirin resistance among patientsundergoing per-cutaneous intervention for unstable anginais associated with clinical outcome. Blood 2004;104:515a(Abstract, 46th Annual Meeting of ASH).
[34] Gachet C. The platelet P2 receptors as molecular targets forold and new antiplatelet drugs. Pharmacol Ther 2005;108:180–92.
[35] Shankar H, Kahner B, Kunapuli SP. G-protein dependentplatelet signaling-perspectives for therapy. Curr DrugTargets 2006;7:1253–63.
[36] Lepantalo A, Virtanen KS, Heikkila J, Wartiovaara U, LassilaR. Limited early antiplatelet effect of 300 mg clopidogrel inpatients with aspirin therapy undergoing percutaneouscoronary interventions. Eur Heart J 2004;25:476–83.
[37] Lev EI, Patel RT, Maresh KJ, Guthikonda S, Granada J, DeLaoT, et al. Aspirin and clopidogrel drug response in patientsundergoing percutaneous coronary intervention. J Am CollCardiol 2006;47:27–33.
[38] Nguyen TA, Diodati JG, Pharand C. Resistance to clopido-grel: a review of the evidence. J Am Coll Cardiol 2005;45:1157–64.
[39] Samara WM, Bliden KP, Tantry US, Gurbel PA. The differencebetween clopidogrel responsiveness and posttreatmentplatelet reactivity. Thromb Res 2005;115:89–94.
Related Documents











