Vaccination in Republic of Macedonia: Standards and Actual Trends • INSTITUTE FOR PUBLIC HEALTH OF THE REPUBLIC OF MACEDONIA • MINISTRY OF HEALTH OF THE REPUBLIC OF MACEDONIA • DOCTOR’S CHAMBER OF MACEDONIA Prepared by: Department for Control and Prevention of Communicable Diseases, Institute for Public Health of the Republic of Macedonia Presented by: Prof. Dr. Koco Cakalaroski, president of the Doctor's Chamber of Macedonia

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Vaccination in Republic of Macedonia:
Standards and Actual Trends
• INSTITUTE FOR PUBLIC HEALTH OF THE REPUBLIC OF MACEDONIA• MINISTRY OF HEALTH OF THE REPUBLIC OF MACEDONIA• DOCTOR’S CHAMBER OF MACEDONIA
Prepared by: Department for Control and Prevention of
Communicable Diseases, Institute for Public Health of the Republic of Macedonia
Presented by: Prof. Dr. Koco Cakalaroski, president
of the Doctor's Chamber of Macedonia

Vaccination and Communicable Diseases
• Vaccines are one of the greatestachievements in the history of medicineand public health, and vaccination is one ofthe most cost-effective health investments!!!
• Vaccination is a proven tool for controllingand eliminating life-threateningcommunicable diseases!!!
Legislation on Vaccination in R. Macedonia
• Law on Protection of Population against Communicable Diseases (Official Gazette of RM No. 66/2004)
• Regulations for immunoprophylaxis, chemoprophylaxis, people subject to these measures, means of realization and keeping records and documentation (Official Gazette of RM No. 65/2010)
• Compulsory Immunization Program for the population in the Republic of Macedonia and National Annual Public Health Program in the Republic of Macedonia (annually, Off. Gazette of RM)

Compulsory Vaccination in R. Macedonia
Compulsory vaccination in RM has two periods: • first campaign period until 1960 and • second continuous period since 1960.
Continuous compulsory immunization in Macedonia is implemented against:1. Tuberculosis (introduced in 1948) 2. Diphtheria (introduced in 1951) 3. Tetanus (introduced in 1951) 4. Pertussis (introduced in 1960) 5. Poliomyelitis (introduced in 1961) 6. Morbilli (introduced in 1972) 7. Parotitis epidemica (introduced in 1982) 8. Rubella (introduced in 1982) 9. Hepatitis B (since October 2004)
10. Haemophilus influenzae type B (since September 2008) 11. Human Papillomavirus (since October 2009)
Implementation of Compulsory Vaccination
of the Population in the Republic of Macedonia in 2013

VACCINATION SCHEDULE IN 2013Age of people subject to compulsory vaccination
Disease against the vaccine is administered
Vaccination Revaccination
up to 24 hours of birth, 1 and 6 months Hepatitis B (3 doses) Vaccination
up to 12 months Tuberculosis (without testing) (1 dose) Vaccination
2, 3 and 5 months
Infections with Haemophilusinfluenzae type B (Hib) (3 doses)Diphtheria, Tetanus, Pertussis (3 doses)
vaccinationVaccination
2, 3 and a half and 5 months Poliomyelitis (3 doses three-type oral vaccine) Vaccination
12 months Morbilli, Rubella, Parotitis epidemica (1 dose) Vaccination
18 months
Infections with Haemophilusinfluenzae type B (Hib) (1 dose)Diphtheria, Tetanus, Pertussis(1 dose) Poliomyelitis (1 dose)
I revaccinationI revaccinationI revaccination
4 years Diphtheria, Tetanus, Pertussis(1 dose) II revaccination
6 years (I grade) Morbilli, Rubella, Parotitis epidemica (1 dose) I revaccination
7 years (II grade) Poliomyelitis (1 dose)Diphtheria, Tetanus (1 dose)
II revaccinationIII revaccination
12 years, 2 and 6 months after the first dose (VII grade)
Infections with HumanPapillomavirus (HPV) (only girls) (3 doses)
Vaccination
14 years (final year of primary school)
Poliomyelitis (1 dose)Diphtheria, Tetanus (1 dose)
III revaccinationIV revaccination
18 years (final year of secondary school) Tetanus (1 dose) V revaccination

Primary Vaccination in Macedonia in 2013
TYPE OF VACCINE COVERAGE
DTP vaccine 98,1%
OPV vaccine 97,9%
Vaccine against Haemophilus
influenzae type B 97,1%
Vaccine against Hepatitis B 96,5%
MRP vaccine 96,1%
HPV vaccine 40,1%

Revaccination in Macedonia in 2013
Type of revaccination Order Coverage
Vaccine against Haemophilus
influenzae type B 96,2%
DTP vaccine
I 97,6%II 96,4%III 95,7%IV 97,3%V 97,8%
OPV vaccine I 97,3%
II 95,0%III 97,2%
MRP vaccine 96,2%

Vaccination and Revaccination Coverage of the Population
in Macedonia inTen-year Period from
2004 – 2013

DTP Vaccination and Revaccination Coverage in R. Macedonia, 2004-2013
80,0
85,0
90,0
95,0
100,0
Cov
erag
e %
Year
Di Te Per вакц.
Di Te Per I ревак.
Di Te Per II ревакц.
Di Te III, IV ревакц.
Те V ревак.
DTP, vacc.
DTP, I revacc.
DTP, II revacc.
DT, III, IV revacc.
T, V revacc.

MRP Vaccination and MRP Revaccination Coverage in R. Macedonia, 2004-2013
90,0
95,0
100,0
Cov
erag
e %
Year
MMR вакц.
MMR I ревакц.
MMR, vacc.
MMR, I revacc.

OPV Vaccination and Revaccination Coverage in R. Macedonia, 2004-2013
90,0
95,0
100,0
Cov
erag
e %
Year
OPV вакц.
OPV I,II,III ревакц.
OPV, vacc.
OPV, I, II, III revacc.

Vaccination Coverage against Hepatitis B and Hib in R. Macedonia, 2005-2013
40
50
60
70
80
90
100
Cov
erag
e %
Year
Хепатитис Б*
ХиБ**
ХиБ ревакцинација
* vaccination against Hepatitis B of all newborns has been initiated since 2004
** vaccination against diseases caused by Haemophilus influenzae type B has been initiated since 2008
Hepatitis B*
Hib**
Hib revaccination

Vaccine-preventable Diseases in the Republic of Macedonia –
Before and After the Introduction of the Vaccination

Diphteria• The last recorded death was in 1972• The last recorded case of disease was in 1976
27 28 15 5 3 0,2
366
486
375
27 30
100
200
300
400
500
600
просечен број умрени
просечен број заболени
Average number of deaths/affected in period 1947-1976
Vaccination introduced in 1951
Average number of deaths
Average number of affected
22
13
41 1 1 1 1 1 1
48
37
127 5
2 41 1 2 1 1 2
0
10
20
30
40
50
просечен број умрени
просечен број на заболени
Vaccination introduced in 1951
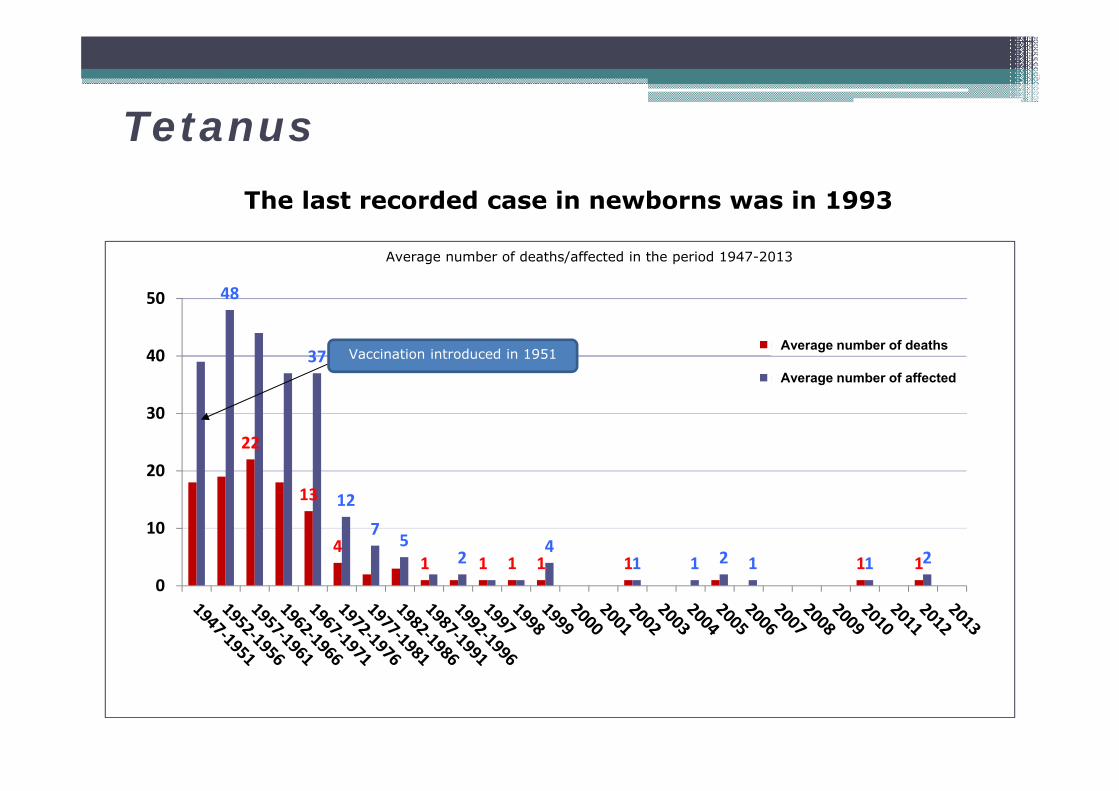
Average number of deaths/affected in the period 1947-2013
TetanusThe last recorded case in newborns was in 1993
Average number of deaths
Average number of affected

Pertussis
The last recorded epidemic was in 1987
3583
1413
403217
125 50
190
500
1000
1500
2000
2500
3000
3500
4000
Average number of affected in period 1956-2000
Просечен број на заболени
Vaccination introduced in 1960
54
1
7 7 7
2
6
9
1
0
2
4
6
8
10
12
14
16
Number of pertussis cases, 2001-2013
Број на заболени
Average number of affected
Number of affected

PertussisThe last recorded death was in 2001
22,4
3,81 0,4 0,6 0,6 0,4 0 0,2 1
0
5
10
15
20
25
Average number of deaths in period 1956-2001
Просечен број на умрени
Vaccination introduced in
1960
Average number of deaths

PoliomyelitisThe last case of disease was recorded in 1987
As a member of the European Region, in June 2002 the Republic of Macedonia achieved certification of poliomyelitis eradication by WHO.
1959 431960 1501961 181962 71963 91964 11965 51966 811967 501968 101969 111970 251971 101972 319731974 21975 619761977 901978 31979198019811982 81983 41984 119851986 31987 1
57
40
21
43
150
187 9
15
81
50
10 11
25
103 2
6
90
38 4 1 3 1
0
20
40
60
80
100
120
140
160
broj
zabo
leni
1956 1958 1960 1962 1964 1966 1968 1970 1972 1974 1976 1978 1980 1982 1984 1986
godi na
ДЕТСКА ПАРАЛИЗА ВО Р. МАКЕДОНИЈА 1956-1986
OPV vaccination introduced in 1961
Poliomyelitis in R.Macedonia, 1956-1986
Nu
mb
er o
f ca
ses
Year

Morbidity and changes in the Immunization schedule against measles and rubella, in period 1967-1997
Morbilli / Rubella
0
100
200
300
400
500
600
МB
/100
.000
Morbilli
Rubella
1972, M-vaccine
1983, MRP vaccine
1987, M-revaccinationR-revaccination
1997, MRP revaccination

Morbilli / Rubella
0,89 1,32 0,25
10,6
34,1
0,3 0,20,02,04,06,08,0
10,012,014,016,018,020,022,024,026,028,030,032,034,036,0
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
MB
/1
00
,00
0
МБ/100.000Рубеола
Morbidity from measles and rubella, in period 1998-2013
The last epidemic of morbilli was in 2010-2011, with 908 affected people in total
- 90.0% (n = 796) of patients with proven vaccination statuswere unvaccinated or with unknown vaccination status
- Most of the affected were in the age group above 20 years (n = 380)
MorbilliRubella

Parotitis epidemica
8436
5161
1016
4321
35860
5865
10920
0
2000
4000
6000
8000
10000
12000
Number of parotitis epidemica cases, 1967-2013
Број на заболени1983 МРП вакцина на 13 месеци
1997 МРП ревакцина на 7г
The last epidemic was in 2008-2009, with over 15,000 affected people
Number of affected1983, MRP vaccination at 13 months
1997, MRP revaccination at 7 years

Epidemics of parotitis epidemica,2008-2009
• Most affected is the group born in 1991-1995, whichaccounts for 51.8% of the recorded cases in total
• The age grouping of patients and the outbreak of theepidemic was probably due to omissions in vaccination inthe corresponding period
• There is a negative correlation between the number of affected people by year of birth and vaccination coverage(r = -0,84, p <0,01)

Vaccination Coverage in Period 1983-2007 and Distribution of Cases in 2009, Per Year of Birth
814
1238
922
697
538
30
35
40
45
50
55
60
65
70
75
80
85
90
95
100
0
100
200
300
400
500
600
700
800
900
1000
1100
1200
130019
78-
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Vac
cin
atio
n c
over
age
%
Nu
mb
er o
f p
arot
itis
epid
emic
aca
ses
Year of birth
Број на заболени
% Опфат со МР(П) вакцина
% Опфат со МР(П) ревакцина
Number of affected
% MR(P) vaccination coverage
% MR(P) revaccination coverage

Conclusion• Primary vaccination against diphtheria, tetanus and whooping cough
continuously has maintained high coverage over 95% in the last decade, with an exception of three years – when it was between 90 and 95%.
• Vaccination and revaccination with OPV vaccine against poliomyelitis wasimplemented in the country with high coverage over 95% in the previous tenyears, with an exception of four years when primary-vaccination coverage wasbetween 90% and 95%.
• Vaccination and revaccination coverage against morbilli, rubella and parotitisepidemica (MRP vaccine) was high - over 95% in the past ten-year period, with an exception in 2006 and 2008, when the range was between 90 and 95%.
• Since the introduction of compulsory vaccination against hepatitis B for all newborns in 2004, this vaccination coverage has ranged from 90.4% (2010) to the highest 98.1% in 2012.
• Vaccination against infections with Haemophilus influenzae type B (Hib) wasinitiated in 2008, primary vaccination and revaccination coverage remainedunder 90% by 2010, after which it increased above the recommended 95%.
• Only the last introduced vaccine in the regular Immunization schedule in 2009 - HPV vaccine has coverage under the recommended 95%.

Conclusion
• Drastic reduction in the number of affected and deaths from vaccine-preventable diseases is evident as a result of the vaccination effects.
• The last recorded case of diphtheria – in 1976, and of poliomyelitis – in 1987.
• In the past ten-year period there were 7 recorded cases of tetanus in total, 3 of which ended with death.
• There were individual cases of whooping cough reported, with mostcases in the previous ten years recorded in 2012 (n = 9). The last death was reported in 2001.
• There has been a steady decline in the morbidity from morbilli and rubella since 1998, with an exception in 2008 and 2010-2011 when there were two outbreaks of morbilli.
• There has been a continuing decline in the number of parotitisepidemica cases since 1997, except in 2008-2009 when there was epidemic of parotitis epidemica.

Challenges
• Continuous maintenance of the coverage over 95% with vaccination and revaccination in each separate territory ("micro" - "macro" area) around the country
- Continuous and active searching for unrecorded, unvaccinated and under-vaccinated individuals, with a special emphasis on hard-to-reach populations (Roma population, migrants, etc.), finding and vaccinating these individuals to complete their vaccination status
• Promotion and strengthening the system of supervision over vaccine-preventable diseases.

• Introduction of polyvalent vaccines for successful implementation of continuous immunization, providing an opportunity for introduction of new vaccines in the Immunization schedule
• Implementation of standardized immunological studies to control the immunity status of the vaccinated people, determining the level of collectiveimmunity, i.e. assessment of the vulnerability to vaccine-preventable diseases in the population.
• Unification (universality) of the system of planning, implementing, recording and supervising the immunization, i.e. introduction of single software with database on immunization.
Challenges

Challenges
• Intensive campaign by all relevant factors in the healthcare system related to the vaccination, which would limit and reduce the effect of emerging anti-vaccine lobby groups that threaten to compromise the regular vaccination.
- In urban areas, especially in the capital, there is a strong influence by anti-vaccine campaign, already reflected in the reduction of vaccination coverage,especially MRP vaccination coverage.
Related Documents

![THE FORMER YUGOSLAV REPUBLIC OF MACEDONIA ...Macedonia. Migration Flows in Modern Macedonia. Skopje. 14 Malgorzata Markiewicz [2006]: Migration and Remittances in Macedonia. Center](https://static.cupdf.com/doc/110x72/5fa5020ac1ba4c3ab23aefc2/the-former-yugoslav-republic-of-macedonia-macedonia-migration-flows-in-modern.jpg)