UVEA Rounds Crissa Marie A. Gay-ya, MD April 27, 2009

UVEA Rounds Crissa Marie A. Gay-ya, MD April 27, 2009.
Dec 30, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

UVEA Rounds
Crissa Marie A. Gay-ya, MDApril 27, 2009

Case
• A.D.
• 38/M
• Seaman
• Right eye pain

HPI
• Recurrent uveitis – 2001, right eye– 2003, left eye– 2005, left eye– 2007, right eye
– Intra-ocular steroids– Prednisolone acetate eye drops, 2 drops 4 x a day

5 days PTC eye pain, right
(+) redness, tearing, and
blurring of vision, right
ER consult
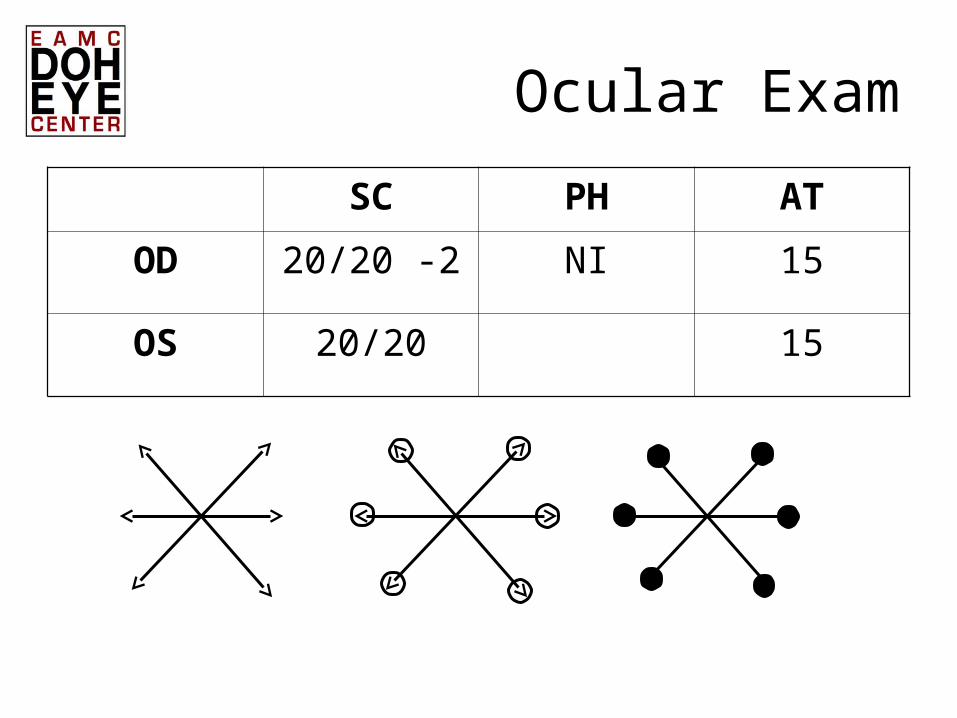
Ocular Exam
SC PH AT
OD 20/20 -2 NI 15
OS 20/20 15


AC deepAC deep

• Fundoscopy:– OD:
• (+) ROR, CM, DDB, CDR 0.3, AVR 2:3, (-) h/e
– OS:• (+) ROR, CM, DDB, CDR 0.3, AVR 2:3, (-) h/e

ER Diagnosis and Plan
• Anterior uveitis, right
• Ibuprofen 400mg BID
• Tobramycin 1gtt QID, OD
• Tropicamide 1gtt TID, OD
• Refer to Uvea Clinic
Uvea Clinic
• Slight improvement of eye pain
• Past Medical History– No hypertension or DM– With scoliosis (?)– With hemorrhoids
• Family History– No heredofamilial disease
Review of Systems
• No fever, no loss of appetite
• No headache, no tinnitus
• No difficulty of breathing, no cough
• No chest pain, no palpitations
• With changes in bowel movement
• No changes in urination, no genital ulcers
• With back pains, no joint pains
• No easy bruising
• No polydypsia, polyphagia, polyuria
• No loss of consiousness, no seizures

Ocular Exam
SC PH AT
OD 20/40 20/20 20
OS 20/32 20
No RAPD(+) Gross Color Perception

Shallowing of ACShallowing of AC

• Fundoscopy:– OD:
• (+) ROR, CM, DDB, CDR 0.3, AVR 2:3, (-) h/e
– OS:• (+) ROR, CM, DDB, CDR 0.3, AVR 2:3, (-) h/e

Salient Features
• 38/M• Recurrent uveitis, both eyes• Eye pain, redness, BOV, • Conjunctivits, iritis, posterior synechiae• Shallowing of AC• Back pain • No joint pains• No genitourinary symptoms

Uvea Diagnosis and Plan
• t/c Ankylosing Spondylitis• Meds:
– Prednisolone acetate 1gtt q 1, OD– Methylprednisolone 40mg/ml, transeptal, OD
• Labs:– RF– ANA– HLA B-27– Sacroiliac x-ray– CXR– PPR– ESR– CBC with platelet

Sadly, the patient was lost to follow-up.
HLA-B27-Associated Anterior Uveitis with Systemic Disease
• Ankylosing spondylitis• Reitier’s syndrome• Inflammatory bowel disease• Psoriatic arthritis• Post-infectious arhtritis

• Incidence
• Role of HLA-B27
• Ocular and Systemic manifestations
• Treatment

Ankylosing Spondylitis: Incidence
• 2.5 to 3 Male: 1 Female
• Females have milder disease
• 96% have (+) HLA-B27
• Only 1.3% of all HLA-B27-positive patients develop the disease
Ankylosing Spondylitis: HLA-B27
• No clear association
• Infection with gram negative bacteria
• Theories on HLA-B27:1. Receptor for infectious agent
2. Cross-react with foreign antigens
3. Marker for immune response gene

Ankylosing Spondylitis: Ocular Manifestations
• 25%
• Bilateral in 80%, but rarely simultaneous
• Recurrence
• Iritis
• Conjunctivitis

• Symptoms occur 1-2 days before clinical signs
• Anterior chamber reaction– Blurring of vision– Fibrin clot– Posterior synechiae

• Sacroilitis
•
Ankylosing Spondylitis: Systemic Manifestations
• Uveitis does not correlate with the severity of the spondylitis
• Aortic insufficiency
• Cardiomegaly
• Conduction defects

• If the disease is recognized and treated early, spinal deformity can be prevented
• Physical therapy
• NSAIDs
Ankylosing Spondylitis: Treatment

Ankylosing Spondylitis
Patient
Male predominance √
HLA-B27 ?
Bilateral √
Recurrence √
Iritis, conjuntivitis √
Symptoms √
Sacroilitis +/-

Reiter’s Syndrome

Reiter’s Syndrome:Incidence
• Most common cause of inflammatory oligoarthropathy in young males
Reiter’s Syndrome:HLA-B27
• 1% with non-specific urethritis – Chlamydia trachomatis– Ureaplasma urealyticum
• 2% dysentery– Shigella, Salmonella, Yersinia– Treatment does not alter the development or
course of the syndrome
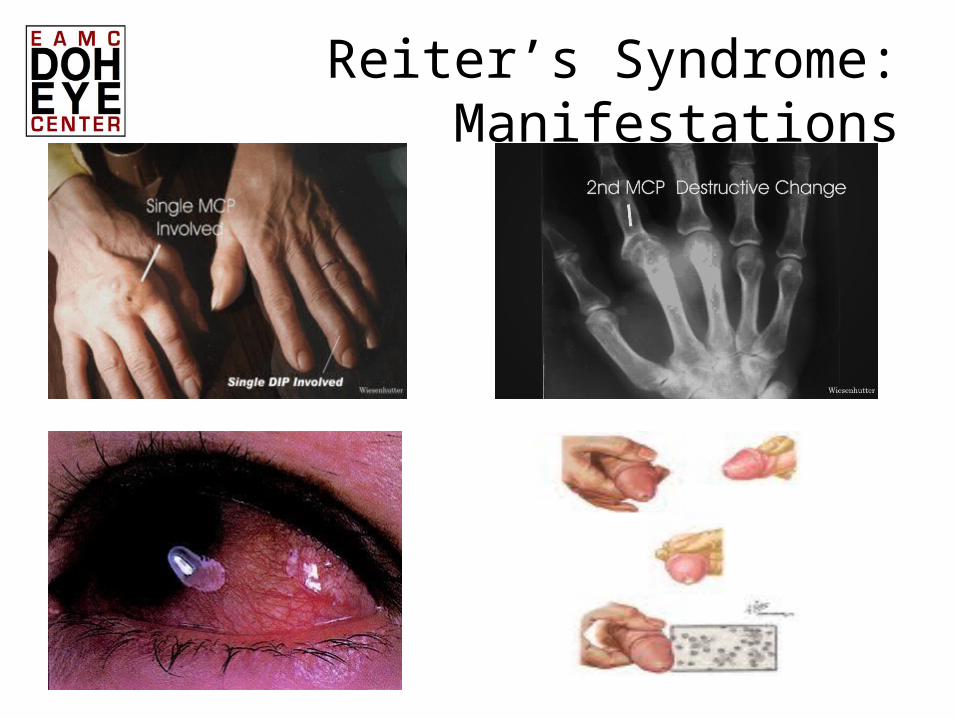
Reiter’s Syndrome:Manifestations


Reiter’s Syndrome:Ocular Manifestations
• Conjunctivitis– Mucoid discharge
• Keratitis– Multifocal punctate subepithelial and stromal
infiltrates
• Iritis– Mild, non-granulomatous
Reiter’s Syndrome:Treatment
• Ocular– Topical corticosterooids– Mydriatic agents
• Joint involvement– NSAIDs– Immunosuppresive therapy
Uveitis and spondyloarthritis: prevalence and relationship with
joint diseaseFaculdade Evangélica de Medicina do
Paraná, and Hospital Universitário Evangélico de Curitiba, Curitiba, PR,
Brazil. [email protected]

• PURPOSE: To study uveitis prevalence in the local population with spondyloarthritis and its temporal relationship with joint complaints.
• METHODS: We reviewed seventy-seven charts of spondyloarthropathy patients from the rheumatology clinic of the "Hospital Universitário Evangélico de Curitiba" for spondyloarthritis class, patients' sex and age, occurrence of uveitis and its location and relationship between the first episode of uveitis and initial joint complaints.

• RESULTS: Uveitis was found in 12 of 77 patients (15.6%) which was anterior in 83.3% of the cases, without preference for spondyloarthropathy class (p=0.72) and patients' sex (p=0.74). In patients with reactive arthritis, the mean time between uveitis appearance and joint complaints was 4.04 months and in ankylosing spondylitis 73 months (p=0.009).
• CONCLUSION: Spondyloarthropathy patients have uveitis that is anterior in most of the cases and that appears earlier in reactive arthritis than in ankylosing spondylitis

Ophthalmological involvement in rheumatic disease]
Spitalul Clinic de Urgente Oftalmologice, Bucuresti.

• PURPOSE: The main objective of this study was to identify the prevalence of ocular manifestations in rheumatic patients admitted in a specialized clinic.

• METHODS: Information regarding rheumatic and ocular diseases was extracted from medical records system available in "Dr. I. Cantacuzino" Clinical Hospital from Bucharest. The prevalence of ocular involvement reported passively by rheumatologists (retrospective descriptive study of 375 different cases of rheumatic patients) was compared with the literature data.

• RESULTS: There were 45 cases of ocular manifestations. Keratoconjunctivitis sicca was noted in 16 patients with rheumatoid arthritis, two patients with systemic lupus erythematosus and one patient with scleroderma. Anterior uveitis was found in seven patients with ankylosing spondylitis, one patient with reactive arthritis, two patients with psoriatic arthritis and one patient with LES. Conjunctivitis was present in two patients with reactive arthritis. In LES ocular involvement also included four cases of retinal vasculitis. Complications clearly related to steroid therapy were nine cases of cataracts. One case with typical "bull's eye" maculopathy due to Hydroxychloroquine treatment was detected.

• CONCLUSIONS: The main conclusion of our study is that the rheumatic patients need to be referred to an ophthalmologist for the diagnosis and the optimal treatment of ocular involvement.

Thank you.
Good morning.

Related Documents











