PHARMACOEPIDEMILOGY AND DRUG SAFETY, VOL 4: 2 1 3-224 (1 995) ORIGINAL REPORT UTILIZATION PATTERNS OF SUBSIDIZED AND NONSUBSIDIZED REIMBURSABLE PEPTIC ULCER MEDICATION IN BELGIUM R. H. VANDER STICHELE MD' AND H. PETRI MD, PhD'.' 'Institute of Pharmacoepidemiology of Belgium (IPhEB), Brussels, Belgium; 'Department of Epidemiology, Rijksuniversiteit Limburg, Maastricht, The Netherlands SUMMARY Study objective - To provide an exploratory description of a dynamic population of Belgian patients treated with reimbursable peptic ulcer medications (ATC Class A20B) and to estimate the annual number @revalence) of patients treated with reimbursable peptic ulcer medications per lo00 inhabitants in Belgium in 1991. Setting - Community pharmacies in Belgium, a country with lo7 inhabitants, where reimbursement of attack therapy (3 months) and maintenance therapy (9 months) is only possible after endoscopic or radiologic confirmation of ulcer or severe esophagitis. Design - Cross-sectional two month registration study of consecutive recipients of reimbursable peptic ulcer medication in a convenience sample of 31 volunteer community pharmacists (a 0.50/0 sample of Belgian community pharmacies). Methods - Data from a simple, self-administered (with assistance from the pharmacist) questionnaire of two pages were used to classify patients in one of four patterns of therapy (attack therapy, relapse therapy, maintenance therapy for 9 months, maintenance therapy longer than 9 months) and to deter- mine the average consumption of qedication packages within each pattern. The number of patients using reimbursable peptic ulcer medication over one year was estimated from these observational data and from the annual sales volume with a theoretical model. Results - The questionnaire was completed by 432 of 481 elegible patients (an 89.9% response rate) in 27 participating pharmacies. Ninety-two per cent of the patients had requested or had obtained reimbursement; 74% had at least one EDG in the past 12 months (113 combined with at least one X-ray). Only nine patients of the small subgroup of 34 patients without reimbursement had undergone diagnostic examinations. Discussion - The study of complex utilization patterns with a simplified model provides a rough estimation of the annual number of medication users. Conclusions - In Belgium, a country with strict reimbursement control, mainly based on EGD per- formed by medical specialists, the annual prevalence of patients using reimbursable peptic ulcer medica- tion is estimated at 30.5 patients/1000 inhabitants/ year. In this country, there is a high utilization of EGD, a high rate of 9 months maintenance therapy and some evidence for channelling of omeprazole. Further longitudinal follow up and comparison with different reimbursement systems in other countries is needed to evaluate the cost-effectiveness and the impact of different regulatory approaches to reimbur- sement regulation on medication utilization. KEY WORDS - histamine H2 receptor blockaders; omeprazole; peptic ulcer; drug costs; endoscopy; cross sectimal study; prevalence; reimbursement system; channelling; Belgium Addressee for Correspondence: Dr R. Vander Stichele, Institute of Pharmacoepidemiology of Belgium (IPhEB), Archimedesstraat, 11, 1040 Brussel, Belgium. CCC 1053-8569/95/040213-12 0 1995 by John Wiley & Sons, Ltd. Received 29 May 1994 Accepted 19 August 1994

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PHARMACOEPIDEMILOGY AND DRUG SAFETY, VOL 4: 2 1 3-224 (1 995)
ORIGINAL REPORT
UTILIZATION PATTERNS OF SUBSIDIZED AND NONSUBSIDIZED REIMBURSABLE
PEPTIC ULCER MEDICATION IN BELGIUM
R. H. VANDER STICHELE MD' AND H. PETRI MD, PhD'.' 'Institute of Pharmacoepidemiology of Belgium (IPhEB), Brussels, Belgium; 'Department of Epidemiology,
Rijksuniversiteit Limburg, Maastricht, The Netherlands
SUMMARY
Study objective - To provide an exploratory description of a dynamic population of Belgian patients treated with reimbursable peptic ulcer medications (ATC Class A20B) and to estimate the annual number @revalence) of patients treated with reimbursable peptic ulcer medications per lo00 inhabitants in Belgium in 1991. Setting - Community pharmacies in Belgium, a country with lo7 inhabitants, where reimbursement of attack therapy (3 months) and maintenance therapy (9 months) is only possible after endoscopic or radiologic confirmation of ulcer or severe esophagitis. Design - Cross-sectional two month registration study of consecutive recipients of reimbursable peptic ulcer medication in a convenience sample of 31 volunteer community pharmacists (a 0.50/0 sample of Belgian community pharmacies). Methods - Data from a simple, self-administered (with assistance from the pharmacist) questionnaire of two pages were used to classify patients in one of four patterns of therapy (attack therapy, relapse therapy, maintenance therapy for 9 months, maintenance therapy longer than 9 months) and to deter- mine the average consumption of qedication packages within each pattern. The number of patients using reimbursable peptic ulcer medication over one year was estimated from these observational data and from the annual sales volume with a theoretical model. Results - The questionnaire was completed by 432 of 481 elegible patients (an 89.9% response rate) in 27 participating pharmacies. Ninety-two per cent of the patients had requested or had obtained reimbursement; 74% had at least one EDG in the past 12 months (113 combined with at least one X-ray). Only nine patients of the small subgroup of 34 patients without reimbursement had undergone diagnostic examinations. Discussion - The study of complex utilization patterns with a simplified model provides a rough estimation of the annual number of medication users. Conclusions - In Belgium, a country with strict reimbursement control, mainly based on EGD per- formed by medical specialists, the annual prevalence of patients using reimbursable peptic ulcer medica- tion is estimated at 30.5 patients/1000 inhabitants/ year. In this country, there is a high utilization of EGD, a high rate of 9 months maintenance therapy and some evidence for channelling of omeprazole. Further longitudinal follow up and comparison with different reimbursement systems in other countries is needed to evaluate the cost-effectiveness and the impact of different regulatory approaches to reimbur- sement regulation on medication utilization.
KEY WORDS - histamine H2 receptor blockaders; omeprazole; peptic ulcer; drug costs; endoscopy; cross sectimal study; prevalence; reimbursement system; channelling; Belgium
Addressee for Correspondence: Dr R. Vander Stichele, Institute of Pharmacoepidemiology of Belgium (IPhEB), Archimedesstraat, 11, 1040 Brussel, Belgium.
CCC 1053-8569/95/040213-12 0 1995 by John Wiley & Sons, Ltd.
Received 29 May 1994 Accepted 19 August 1994

214 R. H. VANDER STICHELE AND H. PETRI
INTRODUCTION
Therapy of peptic ulcer disease (PUD) and related conditions has clearly changed since the nineteen- seventies.'.2 New therapeutic classes like H2 anta- gonists, mucosa protectors and more recently ome- prazole were introduced. The therapeutic value of these drugs for acute symptom relief and preven- tion of relapse in PUD is widely acknowledged, but there is considerable debate about their use in wider indications.' Health economic studies indi- cate that these agents bring about a major reduction of indirect cost (largely due to a decrease of work absenteeism and of hospitalization for uncompli- cated duodenal ulcer), while direct medical costs tended to increase throughout the past two decades (because of rising drug budgets and a surge in diag- nostic procedures like Esophago-gastro-duodeno- scopy (EGD)).'32,4 Most economic observers agree that overall the introduction of peptic ulcer medica- tion was a cost-effective evol~t ion.~- '~ Mortality from PUD stabilizes in most Western countries around two PUD deaths/100,000 inhabitants/ year."
Important issues in the evaluation of the cost- effectiveness of anti-ulcer therapy are the relative prices of different agents, the duration of treatment in acute attack or chronic maintenance therapy and the o timal dosage of these expensive medica- tions.' Most of the economic studies have been performed with cimetidine 800mg daily during 8 weeks attack treatment and cimetidine 400mg daily during 3 year maintenance therapy. The economic value of newer medications (in most cases more expensive) is more difficult to ascertain.
According to medical textbooks, the prevalence of peptic ulcer is 18 patients/1000 inhabitantdyear, a figure based on data from the US National Health Interview In Norway and India, point prevalence of PUD was studied in two recent studies with more sophisticated epidimiological methods, yielding high percenta es up to 47 current PUD patients/l000 inhabitants!?l6 which probably cannot be generalized to other regions of the world. Data from family practice registration studies in the Netherlands indicate a figure of five (well estab- lished) PUD patients/1000 insured/year.I7 The annual incidence of new cases of PUD is estimated between one and two new cases/1000 inhabitants/ year1*-" and the lifetime PUD prevalence is between 62 and 100/1000 male inhabitants and 27 to 40/1000 female inhabitant^.".^^
The prevalence of its common symptom - dys-
pepsia - is at least 380 dyspepsia patients/1000 inhabitants/year,2' although the prevalence of a more restricted definition of non-ulcer-dyspepsia - involving the notions of epigastric pain, chroni- city of the complaint for 1 to 3 months - is prob- ably near the peptic ulcer prevalence.22 The life time prevalence for dyspepsia is over 600/1000 inhabi- tant~.*'**~
The efficacy of potent peptic ulcer medications in non-ulcer - dyspepsia remains subject to dis- p ~ t e . ' ~ Health insurers emphasize that potent and expensive anti-ulcer medication should not be used for simple dyspepsia, gastritis or pyrosis unrelated to reflux esophagitis. Spreading of medication utili- zation to unauthorized indications is considered to be a major threat to the health care budget and rationality of medical care.6 Insurers feel that re- strictions are needed to balance the marketing power of pharmaceutical companies.
We could not find in the literature estimates of the annual prevalence of users of peptic ulcer medi- cations. There are data on annual sales volume, expressed in number of prescriptions, prices or Defined Daily Doses and balanced against inhabi- tants or i n s ~ r e d . ~ . ' ~ . ' ~ ~ ~ ~ - ' ~ Commercial marketing research organizations or national drug data centres probably have statistical data on medi- cation consumption in most Western countries. In the medical literature only limited data have been published: in the Netherlands, 48 prescriptions of H2-antagonists/1000 inhabitantdyear were sold in 1 987,26 in different American states consumption ranges between 65 and 162 anti-secretory drugs pre- scriptions/l 000 inhabitants! year in 1989.27 In Bel- gium, a country with 10 million inhabitants, 125 packages of reimbursable peptic ulcer medications/ 1000 inhabitantdyear were sold in 1991.28
Different regulatory approaches to reimburse- ment have been adopted in developed countries in an attempt to control the public medication budget for peptic ulcer disease. Their influence on medica- tion costs has not been studied exten~ively.~~-'' In Great Britain and the Netherlands, there are no restrictions by formal diagnostic requirements or by limiting therapeutic strategies of prescribing general practitioners and specialists, as insurers rely on the quality of training, continuing edu- cation, quality control and medical audit; the short- term therapeutic trial with potent medications of ulcer-like complaints is allowed and reimbursed. In Denmark, H2-antagonists have changed status from prescription-only to over-the-counter medi- cine (always at the full expense of the patient). In
0 1995 by John Wiley & Sons, Ltd PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 4 213-224 (1995)

REIMBURSABLE PEPTIC ULCER MEDICATION 215
0 1995 by John Wiley & Sons, Ltd PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 4: 213-224 (1995)
Australia and in Belgium, formal (endoscopic or radiologic) proof of peptic ulcer disease is a pre- requisite for reimbursement of peptic ulcer medica- tions; furthermore, therapy strategies are limited by formal regulation of duration and dosage of acute attack and chronic maintenance therapy. In the 1980s until 1993 in Belgium, the reimbursement of anti-ulcer drugs was restricted to narrow indica- tions, requiring substantiation by endoscopy or X- ray examination; acute full dosage attack therapy was possible for 3 months after formal diagnosis, followed by 9 months of maintenance therapy at simple request, renewable for another year after reevaluation.
The aim of this study was to estimate the preva- lence of users of reimbursable peptic ulcer medica- tion in Belgium in 1991 and to describe their medication utilization and diagnostic history.
MATERIAL AND METHODS
From the urban areas and adjoining rural areas of the towns of Ghent, Antwerp, Charleroi and Liege in Belgium (a West European country with 10 million inhabitants) 3 1 community pharmacists were invited to participate in a registration study from October 1 to November 30, 1991. Twenty seven pharmacists (a 0.5% convenience sample out of the 5200 Belgian community pharmacies) agreed to assist patients in completing an anonymous questionnaire of two pages. The pharmacists requested participation from consecutive sample of all patients attending the pharmacy to fill a pre- scription for reimbursable peptic ulcer medication (cimetidine, ranitidine, famotidine, nizatidine, omeprazole) and mucosa protectors (sulfacrate, bismuth subcitrate) (Class A02B in the interna- tional Anatomical Therapeutic and Chemical clas- sification (ATC)32).
Data were collected on sex and age of respon- dent, gastric complaints at the time of the survey, prescribed anti-ulcer medication, whether reimbur- sement was requested or obtained, referral history and previous diagnostic procedures. Patients were asked for the number of packages of peptic ulcer medication consumed in the past 12 months and to classify themselves in one of four stages of ther- apy (attack therapy no longer than 3 months; patients on relapse attack therapy following an ear- lier episode of attack therapy in the last 12 months; patients in maintenance therapy for no longer then
9 months; patients in maintenance therapy for more than 9 months).
Medication packages for ulcer therapy in Bel- gium are designed for 4 weeks of therapy. For the sake of simplicity and because patient recall of medication utilization lacks precision,33 in this pharmacy-based study the number of dispensed packages was equated to the number of months under treatment. Because the majority of Belgian patients on chronic medication attends the phar- macy for refill every one to two months, a regis- tration period of two months (October 1 till November 30, 1991) was considered sufficient to catch all current relapse and chronic medication users and a sufficient number of patients in the acute stage of therapy.
To calculate the prevalence of medication users over one year, the following method has been used in previous
S = P x C where S = Annual sales of medication in packages, P = the total number of patients treated with
medication during one year (to be calculated), C = the average consumption in packagedpatient
over one year (to be empirically determined in a sample survey).
This simple approach is effective for chronic dis- eases like diabetes where most patients have a uniform pattern of utilization and where the popu- lation of diabetes patients in a country is stable over time with a stable incidence of new cases, in equilibrium with a stable mortality rate. In the case of peptic ulcer the situation is more complicated and one has to take into account different patterns of utilization, each with a different average con- sumption. For a disease with complex utilization patterns, six steps are involved in the procedure to determine the prevalence of medication users from observational data stemming from a short observational period:
1 ) To adopt a scheme of relevant patterns of utilization In this study, a scheme of four patterns of therapy has been used.
Pattern I. Patients on 3 months attack therapy, only once in the current year.
Pattern 11. Patients on relapse attack therapy fol- lowing an earlier episode of attack therapy in the

216 R. H. VANDER STICHELE AND H. PETRI
same year (For the sake of simplicity, consumption of users in relapse was schematised to a three month period of attack therapy, followed by three medica- tion-free months, followed by three months relapse therapy).
Pattern 111. Patients in maintenance therapy for no longer than 9 months, following 3 months of attack therapy.
Pattern IV. Patients in maintenance therapy for more than 9 months (all patients having consumed 12 or more packages in the past 12 months).
2 ) To gather observational data on the distribution of treatment stage and average medication consumption In this study we used data from a two month obser- vational cohort of patients attending the pharmacy and filling in a questionnaire.
3) To extrapolate the pattern distribution to the one year cohort Patients observed in the stage of attack therapy will branch later into different patterns; they can be cured and not further treated, they may relapse within the same year or they may be put on main- tenance therapy by their physician. The outcome of the acute attack disease stage is not observable in short observational periods. Outcome can, how- ever, be inferred from the observed distribution of patients over the different stages of therapy at the moment of cross-sectional observation; if many patients are on chronic or relapse therapy, it is almost certain that many of the patients in acute therapy at that moment will evolve later to the chro- nic or the relapse pattern.
To extrapolate from observational data on stages of therapy in a two-month observational cohort to a distribution of patterns of therapy in the one- year prevalence cohort, a model is needed (see Fig. 1). In this model, it is assumed that each month, within each utilization pattern, there is a fixed number of new patients, forming a monthly inci- dence group (potential seasonal variations in the inflow of new patients are neglected, here). How many of these monthly incidence groups are observed within the two month observation period is directly related to the length of the cycle of therapy in each pattern.
In pattern I (only three months attack therapy),
there are 14 monthly incidence groups of NI patients within one year, consuming together 36 x NI packages; four of these 14 groups are observ- able within the two-month observational period, in which they consume 9 x N , packages; the ratio between one-year and two-month consumption is (36/14)/(9/4) = 1.1.
In pattern I1 (three months attack therapy, fol- lowed by a relapse after three months), there are 20 groups of NII patients, consuming together 75 x N,, packages; eight of these 20 groups are observ- able within the 2 months of observation - four in the stage of relapse therapy, in which they con- sume 21 x NII packages) and four in the stage of acute therapy; the ratio between one-year and two- month consumption is (75/20)/(21/4) = 0.71.
In pattern I11 (3 months attack therapy followed by 9 months maintenance therapy), there are 23 groups of NIII patients, consuming 144 X NIII pack- ages; 13 of these 23 groups are observable within the two months observational period - nine in the stage of maintenance therapy, in which they consume 79 X NIIr packages and four in the stage of acute therapy; the ratio between one year and two-month consumption is (144/23)/(79/9) = 0.71.
For pattern IV (maintenance therapy longer than one year), it is assumed that all NIv patients are observable within the two-month observational period and that their comsumption over the past year is 12 x NIv packages; the ratio here is 1.
The extrapolation from distribution of stages to distribution of patterns in the two month observa- tional period proceeds as follows: let w,x,y,z be the observed percentage ( w + x + y + z = 100) ofeach of four stages of therapy (to be determined empiri- cally by a survey) and a,b,c,d be the extrapolated percentage (a + b + c + d = 100) of each of four pat- terns of utilization in the two month observational period. In the observational period x per cent of the patients were observed in the stage of relapse therapy. In order to sustain the dynamics of this distribution, an equal number of patients from the acute stage must evolve to relapse. Hence, the dis- tribution of pattern I1 in the two month observatio- nal period is x + x per cent points. To sustain the number of patients observed in maintenance therapy not longer than 9 months, 4/9 of the number observed must evolve from start phase to maintenance therapy (the model in Fig. 1 indicates four monthly incidence groups starting up for nine in maintenance therapy). For the pattern of main- tenance therapy longer than 9 months, no adjust- ment is made in this model.
0 1995 by John Wiley & Sons, Ltd PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 4: 213-224 (1995)
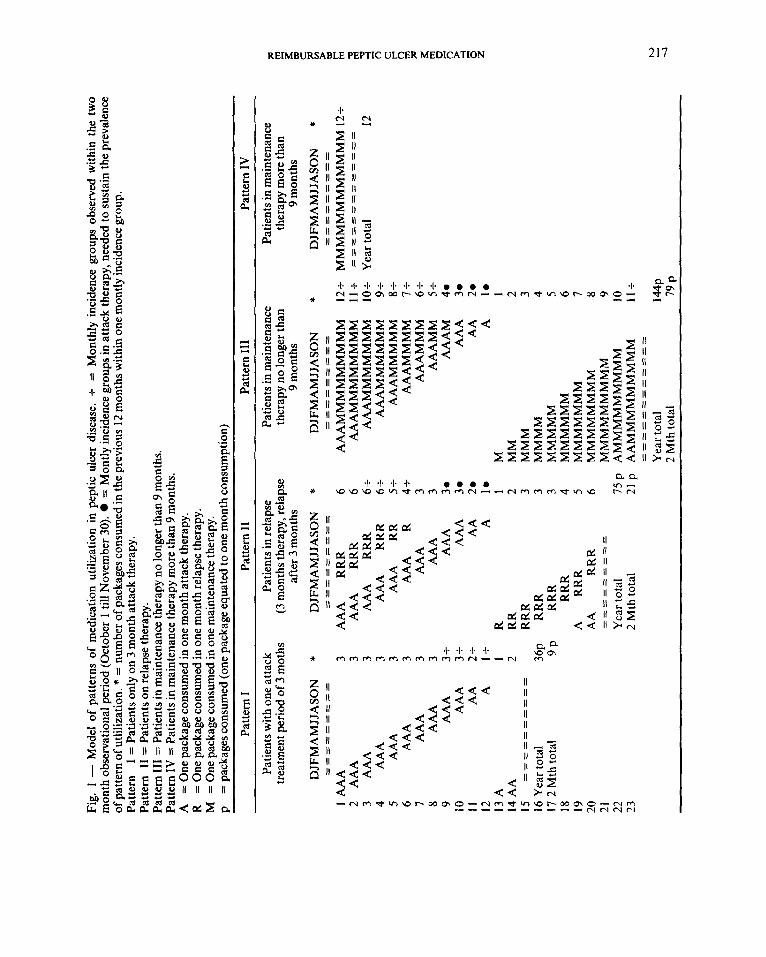
Fig.
1 - M
odel
of
patte
rns
of m
edic
atio
n ut
iliza
tion
in p
eptic
ulc
er d
isea
se. +
= M
onth
ly i
ncid
ence
gro
ups
obse
rved
with
in t
he t
wo
mon
th o
bser
vatio
nal
perio
d (O
ctob
er 1
till
Nov
embe
r 30
). =
Mon
tly in
cide
nce g
roup
s in
atta
ck th
erap
y, n
eede
d to
sust
ain
the
prev
alen
ce
of p
atte
rn o
f utli
lizat
ion.
* =
num
ber o
f pac
kage
s con
sum
ed in
the
prev
ious
12 m
onth
s with
in o
ne m
ontly
inci
denc
e gr
oup.
Pa
ttern
I
= P
atie
nts o
nly
on 3
mon
th a
ttack
ther
apy.
Pa
ttern
I1
= P
atie
nts o
n re
laps
e th
erap
y.
Patte
rn 1
11 =
Pat
ient
s in
mai
nten
ance
ther
apy
no lo
nger
than
9 m
onth
s.
Patte
rn I
V =
Pat
ient
s in
mai
nten
ance
ther
apy
mor
e th
an 9
mon
ths.
A
=
One
pac
kage
con
sum
ed in
one
mon
th a
ttack
ther
apy.
R
= O
ne p
acka
ge c
onsu
med
in o
ne m
onth
rela
pse
ther
apy.
M
=
One
pac
kage
con
sum
ed in
one
mai
nten
ance
ther
apy.
p
= p
acka
ges c
onsu
med
(one
pac
kage
equ
ated
to o
ne m
onth
con
sum
ptio
n)
Patte
rn I
Patie
nts
with
one
atta
ck
treat
men
t per
iod
of 3
mot
hs
DJF
MA
MJJ
ASO
N
----
-----
----
----
- 1
AA
A
2 A
AA
3
AA
A
4 A
AA
5
AA
A
6 A
AA
7
AA
A
8 A
AA
9
AA
A
10
AA
A
I1
AA
12
A
13
A
14 A
A
15
==
==
==
==
==
16
Yea
r tot
al
17 2
Mth
tota
l 18
19
20
21
22
23
* 3 3 3 3 3 3 3 3 3t
3t
2t
It
1 2 36P 9P
Patte
rn I
1 Pa
ttern
Ill
Pa
ttern
IV
ther
apy
no lo
nger
than
Pa
tient
s in
rela
pse
Patie
nts i
n m
aint
enan
ce
Patie
nts i
n m
aint
enan
ce
P
DJF
MA
MJJ
ASO
N
* D
JFM
AM
JJA
SON
*
DJF
MA
MJJ
ASO
N
* 6 c
AA
A
RRR
6 A
AA
MM
MM
MM
MM
M
12s
MM
MM
MM
MM
MM
MM
12+
G 8
AA
A
RRR
6s
A
AA
MM
MM
MM
M
lo+
Y
ear t
otal
12
=!
AA
A
RRR
6s
A
AA
MM
MM
MM
9+
0 5 m 3:
AA
A
3 A
AA
MM
5t
m
(3 m
onth
s th
erap
y, r
elap
se
ther
apy
mor
e th
an
afte
r 3 m
onth
s 9
mon
ths
9 m
onth
s C
----
--- -
- ------- --
-I-------
- - -
- - - - - -
----- --
--
-----c---
-8
AA
AM
MM
MM
MM
M
11 +
=
= =
= =
= =
= =
= =
= =
A
AA
RRR
6
0
P
AA
A
RR
5s
AA
AM
MM
MM
8s
AA
A
R 4s
AA
AM
MM
M
I+
AA
A
3 A
AA
MM
M
6+
AA
A
30
AA
AM
4a
8
AA
A
30
AA
A
3. z
AA
20
z z
AA
20
A
10
A
la
R
1M
1
RR
2 M
M
2 RR
R 3
MM
M
3 RR
R 3
MM
MM
4
RRR
3 M
MM
MM
5
RRR
4 MMMMMM
6 A
RR
R 5
MM
MM
MM
M
I A
A
RRR
6 M
MM
MM
MM
M
8 M
MM
MM
MM
MM
9
Yea
r tot
al
75 p
A
MM
MM
MM
MM
M
lo
2 M
th to
tal
21 p
A
AM
MM
MM
MM
MM
11
+
_ - - - - - - - -
----
--_
--
------------
-_
----------
f! 4
Yea
r tot
al
2 M
th to
tal
79 P

218 R. H. VANDER STICHELE AND H. PETRI
Hence, we can infer that derive the size of this cohort from the annual sales data a = w - x - ~~(419))
b = x + x (2) I I
d = z (4) IV IV IV
(1)
c = y+b(4/9) ) (3) S = c l p * D * C
The extrapolation from the distribution of pat- terns in the two month observational cohort to the distribution of patterns in the one-year cohort pro- ceeds as follows: Let A,& C, D be the extrapolated percentage ( A + B + C + D = 100) of patterns in the one year cohort. From the model, we can derive what fraction of the one year cohort within each pattern is observed during the two month observa- tional period.
Hence, we derive that a relates to A as 4/14; b to B as 8120; c to C as 13/23; d to D as 1/1.
From the equations
1 0 0 = a + b + c + d ( 5 )
(6 ) (7)
a/A = 4/14; b/B = 8/20; c/C = 13/23 and d/D = 111 100 = A + B + C + D
and the equations 1 to 4 A , B, C, D can be calculated, when ru,x,y,z is known.
4 ) To extrapolate the average consumption to the one year cohort
Above we have given the ratio for each pattern between theoretical consumption of packages within the two months observational period and within one year. With this ratio we can multiply the observed average consumption in the study sample, to infer the package consumption over a year for each treatment pattern. This procedure corrects for consumption differences between observed data and theoretical consumption, attributable to patient (non-)compliance.
5 ) To obtain national sales data We received data on the sales of reimbursable pep- tic ulcer medication in 1991 (1,250,300 packages sold in community pharmacies, with or without reimbursement), by the courtesy of SmithKline Beecham, Belgium.
where S = annual sales of medications in packages P = the total number of patients treated with
medication during one year (to be calcu- lated)
D =the frequency of the pattern of utiliza- tion (to be inferred from observational data)
C = the average consumption in packages in one year for each pattern (to be inferred from observational data)
The monthly incidence of new cases (within the current year) can be calculated by dividing the prevalence of pattern I by 14; of pattern I1 by 20; of pattern I11 by 23 (see Fig. 1); the incidence of pattern IV was neglected in our model (to estimate it, a division by at least 60 is necessary).
RESULTS
A total of 481 patients, filling a prescription for reimbursable anti-ulcer medication, were invited to cooperate by 27 pharmacists; 432 patients (89.9 per cent) completed the questionnaire. Of the 432 patients 253 had an additional contact in the two- month observational period but were not asked to complete the questionnaire again.
Patient characteristics
Of the respondents 57 per cent were male and 43 per cent female. Twenty per cent of the patients were between 18 and 39 years old, 39 per cent between 40 and 59 years and 20 per cent 60 years or older. When asked for the location of their ail- ment, 80 per cent of the patients indicated that they were treated for a gastric or duodenal ulcer, 19 per cent for a lesion of the esophagus, 1 per cent did not now.
Symptomatology At the time of the survey, 65 per cent of the patients said to suffer from heartburn, 63 per cent of epigas- tric pain, 50 per cent of difficulty to digest, 37 per
6 ) To calculate the prevalence over one year Once the relative distribution of each treatment pattern and their average package consumption in the yearly prevalence cohort is known, we can
0 1995 by John Wiley & Sons, Ltd
cent of nausea, with of course substantial overlap between these complaints.
PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 4: 2 13-224 (1995)
REIMBURSABLE PEPTIC ULCER MEDICATION
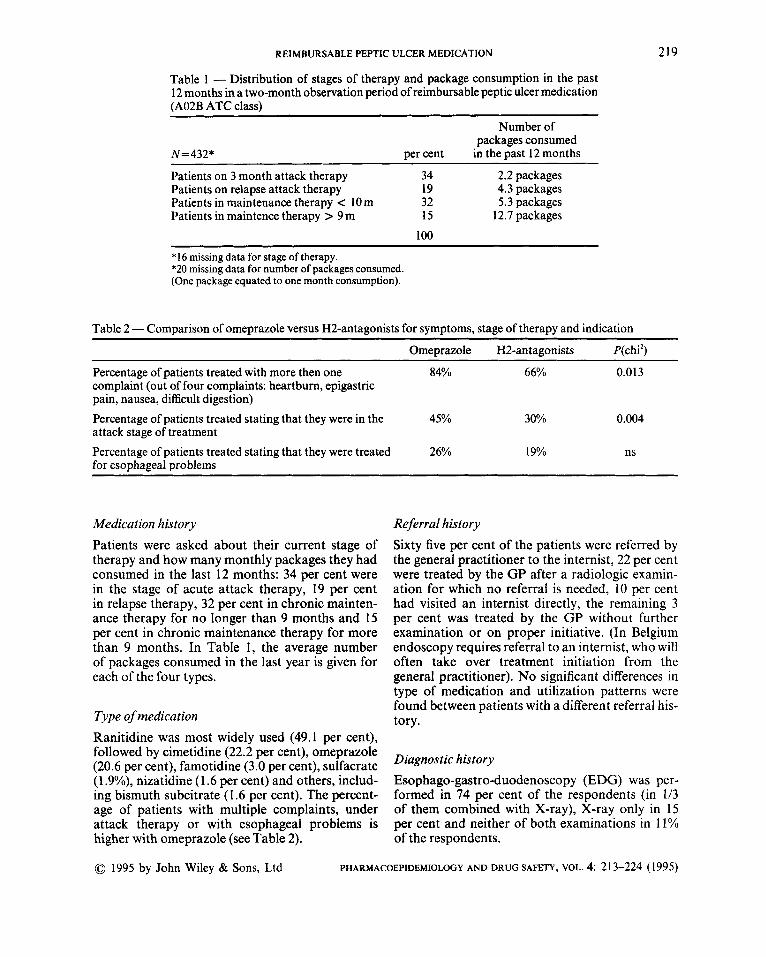
Table 1 - Distribution of stages of therapy and package consumption in the past 12 months in a two-month observation period of reimbursable peptic ulcer medication (A02B ATC class)
219
~~
Number of packages consumed
N=432* per cent in the past 12 months
Patients on 3 month attack therapy 34 2.2 packages Patients on relapse attack therapy 19 4.3 packages Patients in maintenance therapy c 10m 32 5.3 packages Patients in maintence therapy > 9 m 15 12.7 packages
100 ~~~~
*16 missing data for stage of therapy. *20 missing data for number of packages consumed. (One package equated to one month consumption).
Table 2 - Comparison of omeprazole versus H2-antagonists for symptoms, stage of therapy and indication Omeprazole HZantagonists P(chi2)
Percentage of patients treated with more then one 84% 66% 0.013 complaint (out of four complaints: heartburn, epigastric pain, nausea, difficult digestion) Percentage of patients treated stating that they were in the 45% 30% 0.004 attack stage of treatment Percentage of patients treated stating that they were treated 26% 19% ns for esophageal problems
Medication history Patients were asked about their current stage of therapy and how many monthly packages they had consumed in the last 12 months: 34 per cent were in the stage of acute attack therapy, 19 per cent in relapse therapy, 32 per cent in chronic mainten- ance therapy for no longer than 9 months and 15 per cent in chronic maintenance therapy for more than 9 months. In Table 1, the average number of packages consumed in the last year is given for each of the four types.
Type of medication Ranitidine was most widely used (49.1 per cent), followed by cimetidine (22.2 per cent), omeprazole (20.6 per cent), famotidine (3.0 per cent), sulfacrate (1.9%), nizatidine (1.6 per cent) and others, includ- ing bismuth subcitrate (1.6 per cent). The percent- age of patients with multiple complaints, under attack therapy or with esophageal problems is higher with omeprazole (see Table 2).
Referral history Sixty five per cent of the patients were referred by the general practitioner to the internist, 22 per cent were treated by the G P after a radiologic examin- ation for which no referral is needed, 10 per cent had visited an internist directly, the remaining 3 per cent was treated by the GP without further examination or on proper initiative. (In Belgium endoscopy requires referral to an internist, who will often take over treatment initiation from the general practitioner). No significant differences in type of medication and utilization patterns were found between patients with a different referral his- tory.
Diagnostic history Esophago-gastro-duodenoscopy (EDG) was per- formed in 74 per cent of the respondents (in 113 of them combined with X-ray), X-ray only in 15 per cent and neither of both examinations in 11% of the respondents.
0 1995 by John Wiley & Sons, Ltd PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 4: 2 13-224 (1 995)
220 R. H. VANDER STICHELE AND H. PETRI
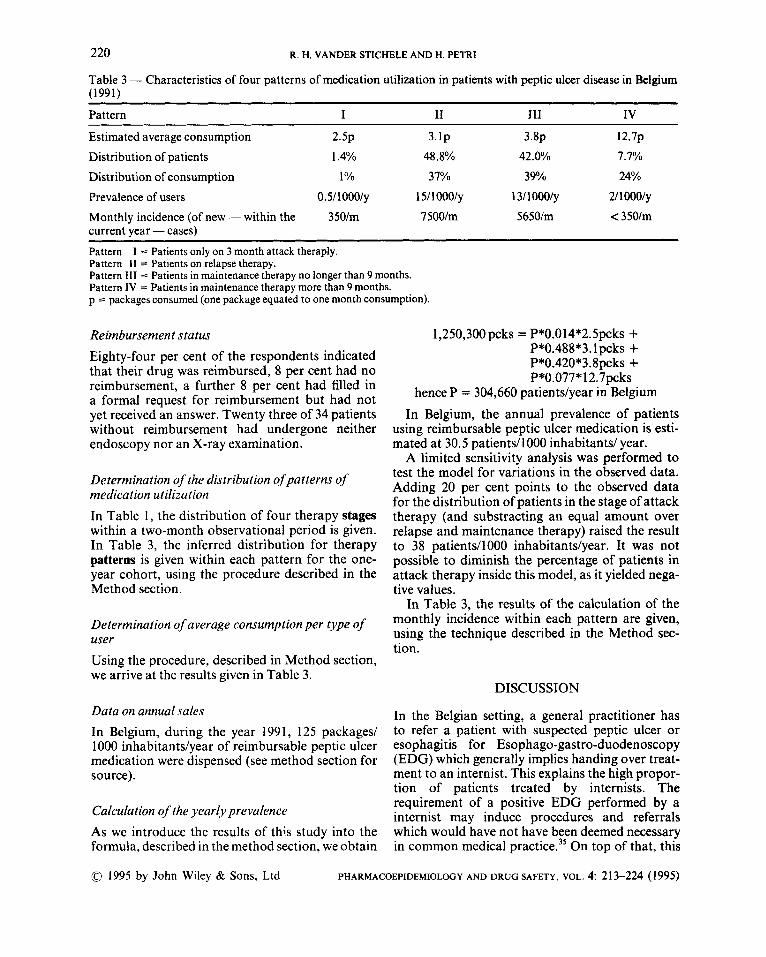
Table 3 - Characteristics of four patterns of medication utilization in patients with peptic ulcer disease in Belgium (1991)
~~~~~~ ~ ~ ~~
Pattern I I1 111 IV
Estimated average consumption 2 . 5 ~ 3.lp 3 . 8 ~ 1 2 . 7 ~
Distribution of patients 1.4% 48.8% 42.0% 7.7%
Distribution of consumption 1 O h 37% 39% 24%
Prevalence of users 0.5/100O/y 15/10oo/y 1 31 1 ooo/y 21 1 Oooiy Monthly incidence (of new - within the 35Olm 7 500im 5650im < 350lm current year - cases) Pattern Pattern I1 = Patients on relapse therapy. Pattern I11 = Patients in maintenance therapy no longer than 9 months. Pattern IV = Patients in maintenance therapy more than 9 months. p = packages consumed (one package equated to one month consumption).
I = Patients only on 3 month attack theraply.
Reimbursement staius Eighty-four per cent of the respondents indicated that their drug was reimbursed, 8 per cent had no reimbursement, a further 8 per cent had filled in a formal request for reimbursement but had not yet received an answer. Twenty three of 34 patients without reimbursement had undergone neither endoscopy nor an X-ray examination.
Determination of the distribuiion of patterns of medication utilization In Table 1, the distribution of four therapy stages within a two-month observational period is given. In Table 3, the inferred distribution for therapy patterns is given within each pattern for the one- year cohort, using the procedure described in the Method section.
Determination of average consumption per type of user Using the procedure, described in Method section, we arrive at the results given in Table 3.
Data on annual sales In Belgium, during the year 1991, 125 packages/ 1000 inhabitantdyear of reimbursable peptic ulcer medication were dispensed (see method section for source).
Calculation of the yearly prevalence As we introduce the results of this study into the formula, described in the method section, we obtain
1,250,300 pcks = P*0.014*2.5pcks + P*0.488*3.lpcks + P*0.420X3.8pcks + P*0.077*12.7pcks
hence P = 304,660 patientdyear in Belgium In Belgium, the annual prevalence of patients
using reimbursable peptic ulcer medication is esti- mated at 30.5 patients/1000 inhabitants/ year.
A limited sensitivity analysis was performed to test the model for variations in the observed data. Adding 20 per cent points to the observed data for the distribution of patients in the stage of attack therapy (and substracting an equal amount over relapse and maintenance therapy) raised the result to 38 patients/1000 inhabitantdyear. It was not possible to diminish the percentage of patients in attack therapy inside this model, as it yielded nega- tive values.
In Table 3, the results of the calculation of the monthly incidence within each pattern are given, using the technique described in the Method sec- tion.
DISCUSSION
In the Belgian setting, a general practitioner has to refer a patient with suspected peptic ulcer or esophagitis for Esophago-gastro-duodenoscopy (EDG) which generally implies handing over treat- ment to an internist. This explains the high propor- tion of patients treated by internists. The requirement of a positive EDG performed by a internist may induce procedures and referrals which would have not have been deemed necessary in common medical pra~tice.~’ On top of that, this
0 1995 by John Wiley & Sons, Ltd PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 4: 2 13-224 (1995)

study has shown that in Belgium prescription behaviour of the GPs closely mimics prescription of specialists in this therapeutic area, even when the general practitioner initiates the treatment. In other countries differences in approach are
and alternative approaches such as trial therapy with low dose cimetidine are Maybe, the request for diagnostic evidence and subsequent referral to the specialist enhance the impact of the specialist on the GP prescription behaviour. The motive for requesting diagnostic evidence of the presence of a anatomical lesion really is the prevention of use for non-approved indications. There is considerable debate on the discriminatory power of EDG, especially as dys- peptic patients (and even asymptomatic patients) very often present objective endoscopic alte- r a t i o n ~ . ~ ~
A small subgroup of patients consuming reim- bursable peptic ulcer medications without being subsidised was detected in this study. These patients were less likely to have undergone endos- copy or X-ray than persons who received reim- bursement. Although patients were not asked why they paid for the medication themselves, one reason might have been dislike of endoscopy, felt as an unpleasant procedure by a substantial minority of patients.* An hypothesis worth studying might be that fright of diagnostic procedures is capable of withholding patients from proper treatment or legi- timate reimbursement.
Patients using omeprazole were more likely to present multiple complaints, to be treated for attack therapy. This significant association is indi- cative for the occurrence of ‘channelling’ pheno- mena, where new drugs in the phase of market introduction are selected for more serious cases.
In the medical literature, two attempts appeared to interpret drug consumption data in the li ht of estimates of annual disease prevalen~e,’’~ but using a restricted definition of PUD and of inci- dence, with data from selected populations. Since no data on annual PUD prevalence in Belgium are available, we will not attempt qualitative apprecia- tion of medication consumption or prescription in Belgium. Moreover, there is considerable weakness in our procedure to estimate the annual prevalence of reimbursable peptic ulcer medication; the em- pirical data stem from a small sample of participat- ing pharmacies; the observational period was short with the possibility of incomplete catchment; dosage differences between esophageal disease and gastric or duodenal disease were neglected; data
stem from non-objective interview with a number of missing data; the dispensing of one medication package was equated with one month consump- tion; the model with four medication utilization patterns is probably a simplification, as some pat- terns are further dividable into more complex pat- terns; a certain degree of seasonal variation might
However, this approach is valid as a rough estimation of the prevalence per year of users of medication with complex patterns of utilization in a restricted geographical area, in countries where there are no data collecting networks of computer- ized pharmacies.
As much as 74 per cent of the patients observed in this study had undergone at least one EGD in the past year. A transposition of this percentage to the annual prevalence group would mean 24 EDGsAOOO inhabitantdyear in Belgium in 199 1, compared to 13 EDGs/1000 inhabitantdyear in Sweden, 198736 and seven EDGs/1000 inhabitants/ year in Leicester, England in 1986.39 With this amount of diagnostic activity, one must take into account the morbidity (estimated at 0.14 to 0.2 per cent), the mortality (0.014 to 0.065 per cent) and the cost of this procedure(3.600 BEF/EDG; 1 US$ = 35 BEF) in any attempt to balance its cost- effectiveness.* It is beyond doubt that the mere volume of this procedure has shaped, in Belgium as in other countries, the professional evolution of gastroenteroI~gy.~~*~
In this survey we found that a large fraction of the patients were on maintenance therapy. In Bel- gium, once reimbursement for acute attack treat- ment is obtained, most physicians seem to orient their patients to maintenance therapy as no formal reevaluation is requested in the transition. Regula- tory authorities in Belgium have chosen for expen- sive specialist performed diagnostic control. One probably unintended result is that this system seems to have favoured the initiation of expensive main- tenance therapy (cimetidine 400 mg 969 BEF/ month;ranitidine 150 mg 1074 BEF/month; ome- prazole 20mg 2.850 BEF/month) and in conse- quence a further growth of direct medical cost.
If one accepts maintenance therapy of one, two and perhaps three years to be cost-effective, as most observers did at the time of this survey, than this unintended effect might balance the cost of tight therapeutic control.26 Since 1993, however, Belgian regulations have become even tighter, with require- ment of repeated EGD after six months therapy and inhibition of long term maintenance therapy. One wonders if this escalation of control will
REIMBURSABLE PEPTIC ULCER MEDICATION 22 1
0 1995 by John Wiley & Sons, Ltd PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 4 213-224 (1995)

222 R. H. VANDER STICHELE AND H. PETRI
remain cost-effective, if it ever was. In order to con- tain costs of drug prescribing alternative approaches are possible e.g. audit of prescribing or educational programmes.4548 The results of this study could also provide a baseline to evaluate the impact of new physiopathological insights on pep- tic ulcer disease with the possibility of short term curative antibiotic treatment, in case of infection by Helicobacter pylori.
This study showed that it is possible to coHect information from patients via pharmacies, not only about medication utilization, but about other medi- cal aspects as well. A more precise estimation of prevalence can be reached using larger samples of computerized pharmacies where comprehensive data on timing of drug dispensing to individual patients are collected.
CONCLUSION
In Belgium, a country with strict reimbursement control, mainly based on EGD performed by medi- cal specialists, the annual prevalence of patients using reimbursable peptic ulcer medication is esti- mated at 30.5 patients/1000 inhabitantdyear. In this country, there is a high utilization of EGD, a high rate of 9 months maintenance therapy and some evidence for channelling of omeprazole. Further longitudinal follow up and comparison with different reimbursement systems in other countries is needed to evaluate the cost-effective- ness and the impact of different regulatory approaches to reimbursement regulation on medi- cation utilization.
ACKNOWLEDGEMENTS
This study was granted by the National Pharmacist Association of Belgium. The study was monitored by the contract research organization Health Care Research. The authors wish to thank participating pharmacists Bracke, D’Hondt, Haelvoet, Halet, Parmentier, Spiers, Storme, Verplancken, Bellet, Bogaerts, Gossein, Marchal, Moyard, Ureel, Vaniekaut, Broeckx, De Beenhouwer, Detroch, Desbuquoit, Keyenberg, Naegels, Willaert, Detrait, Gottschalk, Hustinx, Lemaire, Mouchette, Paques, Quittin, Streber and Wery.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
REFERENCES
Kurata, J. H. and Corboy, E. D. Current peptic ulcer time trends. An epidemiologic profile. Journal of Cli- nical Gastroenterology 1988; 10: 259-268. Bloom, B. S., Fox, N. A. and Jacobs, J. Patterns of care and expenditure, by California Medicaid for peptic ulcer and other acid-related diseases. Journal of Clinical Pharmacology 1989; 11: 615-620. Colin-Jones, D. G. Management of dyspepsia: report of a working party. Lancet 1988; i 576579. Bulthuis, R. and Laing, W. A. Cost-effectiveness of cimetidine. Lancet 1982; ii: 828-829. Fox, N., Morton, R. E. and Jacobs, J. The cost- effectiveness of maintenance therapy for duodenal ulceration with an H2-antagonist. Alimentary Phar- macology and Therapeutics 1988; 2: 297-309. Jensen, D. M. Economic assessment of peptic ulcer disease treatments. Scandinavian Journal of Gas- troenterology 1988; 23(S146): 214-224. Sonnenberg, A. Costs of medical and surgical treat- ment of duodenal ulcer. Gastroenterology 1989; 96:
Pym, B., Sandstad, J., Seville, P., et al. Cost-effec- tiveness of cimetidine maintenance therapy in chro- nic gastric and duodenal ulcer. Gastroenterology 1990; 99: 27-35. Jonsson, B., Carlsson, P. The effects of cimetidine on the cost of ulcer disease in Sweden. Social Science and Medicine 199 1; 33: 275-282. BIoom, B. S. Costs, benefits and unintended gas- trointestinal side effects of pharmaceutical therapy. Pharmaco-Economics 1992; 1: 175-181. La Vecchia, C., Lucchini, F., Negri, E., Reggi, V. and Levi F. The impact of therapeutic improvements in reducing peptic ulcer mortality in Europe. Interna- tional Journal of Epidemiology 1993; 22: 96-106. Ashton, T. Cost-effectiveness of alternative medica- tions in the treatment of duodenal ulcer. Scandina- vian Journal of Gastroenterology 1991; 26 82-88. Sleisenger, M. H. and Fordtran, J. S. (Eds). Internal Medicine. Saunders, Philadephia, 1989. Wyngaarden, J. B. H., Smith, L. H. and Bennett, J. C. (Eds) Cecil Textbook of Medicine 19th edn. Saunders, Philadelphia, 1992. Bernersen, B., Johnsen, R., Straume, B., Burhol, P. G., Jenssen, T. G. and Stakkevold, P. A. Towards a true prevalence of peptic ulcer: the Ssrreisa gas- trointestinal disorder study. Gut 1990; 31: 989-992. Khuroo, M. S., Mahajan, R., Zargar, S. A., Javid, G. and Munshi, S. Prevalence of peptic ulcer in India: an endoscopic and epidemiological study in urban Kashmir. Gut 1989; 30: 930-934. Haayer, F. M. Van der Werf, G. T., Wieringa, N. F. and Wesseling H. Use of cimetidine: parallels and discrepancies between the views of drug regulatory agencies and practicing physicians. European Journal of Clinical Pharmacology 1983; 25: 601-607.
1445-1452.
0 1995 by John Wiley & Sons, Ltd PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 4 213-224 (1995)
REIMBURSABLE PEPTIC ULCER MEDICATION 223
18. Stein, J. H. (Ed.) Internal Medicine 3rd edn. Little, Brown and Company, Boston, 1990.
19. Bonnevie 0. The incidence of gastric ulcer in Copen- hagen County. Gastroenterology 1975; 10: 23 1-239.
20. Johnsen, R., Straume, B., Fauorde, 0. H. and Bur- hol, P. G. Changing incidence of peptic ulcer - facts or artefacts? A cohort study from Tromso. Journal of Epidemiology and Community Health 1992; 46: 433-436.
21. Jones, R. Dyspeptic symptoms in the community.
22. Talley, N. J., Phillips, S. F. Non-ulcer dyspepsia: potential causes and pathophysiology. Annals of Internal Medicine 1988; 108: 865-879.
23. Tibblin, G. Introduction to the epidemiology of dys- pepsia. Scandinavian Journal of Gastrolenferology
24. Brownlee, H. J. Jr, Delaney, R. A. and Hancock, J. B. Abuse of cimetidine in outpatient practice. New England Journal of Medicine 1983; 308: 1226.
25. Mnrller, H., Nissen, A. and Mosbech, J. Use of cime- tidine and other peptic ulcer drugs in Denmark 1977- 1990 with analysis of the risk of gastric cancer among cimetidine users. Gut 1992; 33: 1166-1 169.
26. Zijlstra, I. F., Gribnau, F. W. J., Haaijer-Ruskamp, et al., Tussen wens en werkelijkheid. Geneesmidde- len bij peptische aandoeningen in de huisartsprak- tijk. Huisarts en Wetenschap. 1991; 34: 158-165 (Dutch).
27. Anonymous. Peptic ulcer medication usage. United States. 1989. Statistical Bulletin of the Metropolitan Insurance Companies 1990; 71: 1&17.
28. Personal Communication, SmithKline Beecham, Belgium.
29. Goulston, K. J., Dent, 0. F., Mant, A., Logan, J. and Ngu, M. Use of H2-receptor antagonists in patients with dyspepsia and heartburn: a cost com- parison. Medical Journal of Australia 1991; 155: 20- 26.
30. Bytzer, P. and Hansen, J. M. Schaffaliltzky de Muck- adell OB. [Over-the-counter availability of ulcer drugs. Study of changes in the drug use pattern and the pressure on diagnostic measures]. Ugeskr Laeger 1991; 153: 1405-1410 (Danish).
3 1. Lennholm, B. [The Danish trial with non-prescrip- tion drugs against stomach ulcer evaluated. An inter- nationally unique drug reform caused a stagnant sale of drugs against stomach ulcer]. Lakartidningen 1991; 88: 150-152 (Danish).
32. WHO Collaborating Centre for Drug Statistics Methodology. ATC Index. Oslo, 1990.
33. Van Den Brandt, P. A,, Petri, H., Dorant, E., Gold- bohm, R. A. and Van de Crommert, s. Comparison of questionnaire information and pharmacy data on drug use. Pharmaceutisch Weekblad (Scientific Edi- tion) 1991; 13: 91-96.
34. Walckiers, D., Van der Veken, J., Papoz, L. and Stroobant, A. Prevalence of drug-treated diabetes mellitus in Belgium. Results of a study with the col-
Gut 1989; 30: 893-898.
1985; 2O(S~ppl 109): 29-33.
laboration of a network of pharmacies. European Journal of Clinical Pharmacology 1992; 42: 6 13-6 19.
35. Jonsson B. Cost-effectiveness of endoscopy in the evaluation of dyspepsia. In: Policy Making in Health Care: Changing Goals and New Tools, Jonsson, B., Rutten, F. and Vang, J. (Eds.) Linkoping Collabor- ating Centre, Linkoping, 1991.
36. Warndorff, D. K., Knottnerus, J. A., Huijnen, L. G. J. and Starmans R. How well do general practi- tioners manage dyspepsia? Journal of the Royal Col- lege of General Practitioners 1989; 39: 499-502.
37. Johannessen, T., Kristensen, P., Petersen, H., et a/. The symptomatic effect of 1 -day treatment periods with cimetidine in dyspepsia. Combined results from randomized, controlled, single-subject trials. Scandi- navian Journal of Gastroenterology 1991; 26: 974- 980.
38. Williams, B., Luckas, M., Ellingham, J. H. M., Dain, A. and Wicks, A. C. B. Do young patients with dys- pepsia need investigation? Lancet 1988; ii: 1349- 1351.
39. Kahn, K. L. and Greenfield, S. The efficacy of endos- copy in the evaluation of dyspepsia. A review of the literature and development of a sound strategy. Jour- nal of Clinical Gastroenterology 1986; 8: 346-358.
40. Johnsen, R., Bernersen, B., Straume, B., Ferrde, 0. H., Bostad, L. and Burhol, P. G. Prevalences of endoscopic and histological findings in subjects with and without dyspepsia. British Medical Journal 1991 ;
41. Van Adrichem, J. A. M., van Kessel, J. F. E. and Tjoeng, M. M. H2-remmers: wie zit ermee in zijn maag. Medisch Contact. 1988; 45: 1391-1 394 (Dutch).
42. Braverman, D. Z., Morali, G. A., Patz, J. K. and Jacobsohn, W. Z . Is duodenal ulcer a seasonal dis- ease? A retrospective endoscopic study of 3105 patients. American Journal of Gastroenterology 1992;
43. Smith, J. L. Physicians’ assistants doing endoscopy? editorial. American Journal of Gastroenterology 1992; 87: 937-938.
44. Overholt, B. F. Presidential address 1984. Gastroin- testinal endoscopy in the 1980s: cost, challenge, and change. Gastrointestinal Endoscopy 1984; 30: 325- 328.
45. Lipowski, E. E., Bauwens, S. F. and Collins, T. M. An examination of histamine-2 receptor antagonist use by medicaid recipients in Wisconsin long-term care facilities. Journal of American Geriatric Society
46. Gurwitz, J. H., Noonan, J. P. and Soumerai, S. B. Reducing the use of H2-receptor antagonists in the long-term care setting. Journal of American Geriatric Society 1992; 40: 359-364.
47. Mead, R. A. and McGhan, W. F. Use of histamine,-
302: 749-752.
87: 1591-1593
1988; 36: 531-536.
0 1995 by John Wiley & Sons, Ltd PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 4: 213-224 (1 995)

224 R. H. VANDER STICHELE AND H. PETRI
receptor blocking agents and sucralfate in a health maintenance organization following continued clini- cal pharmacist interventions. DICP, 1988; 22: 4 6 6 469.
48. Raisch, D. W., Bootman, J. L., Larson, L. N. and McGhan, W. F. Improving anti-ulcer agent prescrib- ing in a health maintenance organization. American Journal of Hospital Pharmacy 1990; 47: 1766-1173.
0 1995 by John Wiley & Sons, Ltd PHARMACOEPIDEMIOLOGY AND DRUG SAFETY, VOL. 4: 2 13-224 (1 995)
Related Documents