University of Groningen Oral antidiabetic drugs and cardiac remodeling Yin, Meimei IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2012 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Yin, M. (2012). Oral antidiabetic drugs and cardiac remodeling. [S.l.]: [s.n.]. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 06-07-2020

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

University of Groningen
Oral antidiabetic drugs and cardiac remodelingYin, Meimei
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2012
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Yin, M. (2012). Oral antidiabetic drugs and cardiac remodeling. [S.l.]: [s.n.].
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 06-07-2020

Oral Antidiabetic Drugs and Cardiac Remodeling

Oral antidiabetic drugs and cardiac remodeling
Meirnei Yin

Financial support by University of Groningen, Groningen Institute for Drug Exploration (GUIDE) for publication of this thesis is gratefully acknowledged.
Oral antidiabetic drugs and cardiac remodeling copyright 2012 Meimei Yin
All rights reserved No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, without permission of the author
ISBN: 978-90-367-5364-7 ISBN electronic version: 978-90-367-5362-3
Cover design: Meimei Yin Layout: Meimei Yin Printing: Jpskamp Drukkers B.V., Enschede

,----� ... . ,t� t ...,),.,'.
. �. Stellingen
Behorende bij het proefschrift
, .... i.> Ora antidiabetic drugs and cardiac remodeling
Meimei Yin
I. In addition to hypertrophy, fibrosis, and apoptosis, myocardial metabolism also plays a pivotal role in cardiac remodeling. (This thesis)
2. Comparable to the renin-angiotensin system, the incretin system is not only working systemically but also exerts specific local tissue dependent effects. (This thesis)
3. Diabetes and heart failure are strongly interrelated; they can aggravate and provoke each other. This should be a strong focus for designing relevant new therapeutic strategies. (This thesis)
4. Observational data suggest that metformin and GLP-1 may be beneficial in diabetic patients with cardiovascular disease independent of their effect on glucose metabolism. (This thesis).
5. AMPK acts as a metabolic master switch regulating several intracellular systems including the cellular uptake of glucose, fatty acids oxidation and the biogenesis of glucose transporter 4 (GLUT4), protein synthesis and mitochondria. (This thesis)
6. If you think research is expensive, then try disease. Mary Lasker ( 1900-1994)
7. Success is going from failure to failure without losing enthusiasm. -Winston Churchill
s. ..t�:§'7](, 7JcflWJJJ!ltililii�� The best (man] is like water. Water is good; it benefits all things and does not compete with them. It dwells in [lowly] places that all disdain. This is why it is so near to Tao Lao-tzu (Chinese philosopher, 604 -531 BC).
9. The most important part to get a PhD degree is not to get the title of Doctor, but to develop the skills to be a philosopher.
10. For Dutch people, there is a clear line between work and holiday; but Chinese people are always mixing work and holiday.

--

/ rijk:suniversiteit gron1ngen
Oral antidiabetic drugs and cardiac remodeling
Proefschrift
ter verkrijging van het doctoraat in de
Medische W etenschappen
aan de Rijksuniversiteit Groningen
op gezag van de
Rector Magnificus, dr. E. Sterken,
in het openbaar te verdedigen op
maandag 2 april 2012
om 16.15 uur
door
Meimei Yin
geboren op 26 maart 1981
te Heilongjiang, China
Cl'lltr:.!c U 1\1.:diM h\! M Bibll,nhct.k C Grm11nb::n G

Promotor:
Copromotores:
Beoordelingscommissie:
Prof. dr. W.H. van Gilst
Dr. R.A. de Boer
Dr. H.H.W. Sillje
Prof. dr. M.P. van den Berg
Prof. dr. A.A Voors
Prof. dr. J.H. Kingma

Paranimfen: Anne-Margreet R. de Vries- de Jong
Hongjuan Yu

I

Contents
Chapter 1 General introduction 9
Chapter 2 Variable effects of anti-diabetic drugs in animal models of 19 myocardial ischemia and remodeling: lessons for the cardiologist
Chapter 3 Metformin improves cardiac function in a nondiabetic rat model 51 of post-Ml heart failure
Chapter 4 Early and late effects of the DPP-4 inhibitor 73 vildagliptin in a rat model of post-myocardial infarction heart failure
Chapter 5 The effects of the DPP-4 inhibitor vildagliptin on diabetic 93 cardiomyopathy in Zucker Fatty Diabetic rats
Chapter 6 Diabetes is associated with an increased incidence of 113 non- ischemic heart failure in patients with coronary artery disease
Chapter 7 Summary and future perspectives 125
Nederlandse samenvatting 133
Acknowledgement 141

"

Chapter 1
General introduction
Chapter l
General introduction
Heart failure Heart failure is the common end-stage phase of most cardiac diseases and a leading cause of death in the developed countries. The most common definition of heart failure is "A pathophysiological state in which an abnormality of cardiac function is responsible for the failure of the heart to pump blood at a rate commensurate with the requirement of the metabolizing tissues" 1
• Five-year survival rate of patients is around 50% after a diagnosis of heart failure 2• There is a dramatic increase in the number of persons who will develop heart failure and heart failure-related diagnosis, which has resulted in a heavy burden to the health care expenditure in past decades '· 3.
As said, the etiology of heart failure is diverse, as many cardiac and also noncardiac diseases may ultimately manifest as heart failure. Most common causes for heart failure are coronary artery disease, hypertension, valvular disease, congenital heart disease, diabetes, and arrhythmias, amongst others 4• The initial injury is followed by a maladaptive compensatory response, referred to as cardiac remodeling 5• Different causes of heart failure develop differently, with distinct patterns and time course, as shown in figure I. An important distinction is heart failure with reduced ejection fraction (HFREF) vs. heart failure with preserved ejection fraction (HFPEF). Chief cause for HFREF is myocardial infarction, followed by pronounced remodeling and changing shape of the left ventricle, leading to systolic heart failure. Chief cause for HFPEF is hypertension, with or without diabetes mcllitus. However, it is important to realize that both patients with a myocardial infarction and patients with hypertension with or without diabetes may pass through an HFPEF period into HFREF 6•
The early typical clinical symptoms of heart failure include fatigue and shortness of breath which exacerbates on exertion 1
• However, on longer term, pathophysiology and clinical manifestations of heart failure arc typical for a multisystem disease, since not only the heart is affected, but other organs, including kidneys, lungs, muscle, liver, bone marrow and other organs arc also affected and show pathophysiological changes and damage. The last decades, many new insights into the pathophysiology of heart failure have been made. These possible molecular mechanisms of heart failure involve cardiomyocyte apoptosis, myocardial fibrosis, and dysfunction of myocyte metabolism 5
• 7• 8
. However, the precise pathophysiological mechanisms of heart failure are still incompletely understood.
Although pharmacological interventions attenuate the progression of the disease, mortality still remains high and patients still suffer a poor outcome 9• 10• Therefore, new therapeutic possibilities to improve the clinical outcome are dearly warranted.
10

General introduction
LVEF
45% -. ---------------------------------- ----------------------------- ··· ... _------------------------
·•. SHF
· ... ?
\.: •.... ·· ... o�-----------�--------------Time-
Figure 1 Time course and pattern of development of heart failure primarily caused by myocardial infarction (MI), and of heart failure primarily caused by hypertension (Hl), with or without mellitus (DM)Both patients with an MI and patients with HT may pass through an SHF period. Sanderson J E. Heart, 2007.Reprinted with permission from the Publisher.
Type 2 diabetes mellitus Type 2 diabetes mellitus is by far the most common type of diabetes (type 1 diabetes
mellitus being the other main type). In this thesis, diabetes simply refers to type 2
diabetes mellitus. The prevalence of diabetes is growing rapidly and it is associated
with both lifestyle and genetic factors, such as obesity, sedentary lifestyle, older age,
family history of diabetes 11, especially in western societies, but also in developing
countries 12• The epidemic of diabetes is predicted to be one of the major challenges of
health care in the 21st century.
Diabetes is a metabolic disorder characterized by insulin resistance or defective
insulin secretion. Insulin is synthesized and secreted by the p cells in the islets of
Langerhans, which are the regions of the pancreas that contain its endocrine (i.e.,
hormone-producing) cells. Insulin plays an important role in the regulation of glucose
metabolism. Reduced insulin sensitivity or deficient insulin levels result in a high body
glucose level, which is called hyperglycemia, and on the long term, after a subclinical
phase before the clinical presentation shows, this may turn into diabetes.
The classic symptoms of diabetes are polyuria (frequent urination), polydipsia
(increased thirst), polyphagia (increased hunger), fatigue and weight loss. Diabetes is
often diagnosed as hyperglycemia, and long-term high glucose levels result in chronic
diabetic complications which affect many organs, such as heart, kidney, eyes and
nerves. The most important strategy to treat type 2 diabetes is glycemic control to slow
11
II

Chapter 1
down the development and progression of the clinical complications and improve
outcome. Current therapies include lifestyle intervention through diet changes and
exercise 11• When lifestyle intervention is not sufficient, oral antidiabetic drugs are
recommended. Eventually, insulin treatment is needed.
Diabetes is associated with hyperglycemia, hyperinsulinemia, dyslipidemia, and
an inflammatory state. All of these features affect the organs, and diabetes-associated
end organ damage is the main reason for diabetes-related morbidity and mortality.
Cardiovascular disease, such as hypertension, myocardial infarction or heart failure, is
the most common complication of diabetes, which in fact accounts for 80% of the
mortality in the diabetic population. The Framingham study showed that a high
incidence of congestive heart failure exist in diabetic subjects: a 2.4-fold increase in
diabetic men and a 5-fold increase in diabetic women independent of age, hypertension
and coronary artery disease 13•
I ·a. _g
C: � -� r. ·J C:
Cl.
0
� c:i
8 c:i
� c:i
0 0
0
Normal Low Normal High IFG New OM OM
200 400
__,...J
/
600 800 1000 1200
Days of Follow-up
Figure 2 The proportion of patients with hospitalization for CHF ( chronic heart failure divided into classes of glycemia at baseline. IFG indicates impaired fasting glucose. Held C et al, Circulation, 2007, reprinted with permission of the Publisher.
Heart failure and diabetes Heart failure and diabetes seem to have a close relationship with each other, since 20-
30% of heart failure patients also have diabetes 14• Vice versa, patients with diabetes
have a high likelihood of developing heart failure. As shown in figure 2, patients with
hyperglycemia, insulin resistance and diabetes have much higher incidence to develop
12

General introduction
incident heart failure 15• So, diabetes mellitus is considered as a well-recognized risk
factor for heart failure.
As discussed, the most common connection between diabetes and heart failure is
II atherosclerosis and coronary artery disease 8, which may cause myocardial infarction,
and cause heart failure 16• Diabetes increases the risk for myocardial infarction,
followed by a process of myocardial remodeling, in the end resulting in heart failure.
Interestingly, part of the incident heart failure associated with diabetes is observed in
the absence of cardiovascular disease, myocardial infarction, or other causes, but it
seems that glycometabolic dysregulation per se may cause heart failure by itself. This
entity is called "diabetic cardiomyopathy''. It manifests as cardiac dysfunction in
diabetes patients, which is mainly characterized by myocardial hypertrophy and
diastolic dysfunction (although cardiac dilatation and systolic dysfunction may also
occur), independent of the coexistence of ischemic heart disease or hypertension 17•
However, the link between diabetes and cardiovascular disease is only partially
understood. Multiple mechanisms play a role: sustained hyperglycemia can result in
overload of cellular Ca2+, activation of the renin-angiotensin system, increased
oxidative stress, mitochondrial dysfunction and altered myocardial substrate
metabolism, which is shown as increased lipolysis, impaired myocardial glucose
uptake and utilization and increased fatty acid (FA) oxidation 12•18• As captured in
figure 3, in addition to other causes like ischemic heart disease, hypertension, valvalur
disease, endothelial dysfunction, such diabetes-specific factors may also contribute to
increased L V diastolic stiffness, and result in diastolic dysfunction.
In line with these mechanistic insights, several clinical post-hoc analyses from
large scale trials showed that diabetes is a predictor of a worse prognosis and outcome
of heart failure. The Studies of Left Ventricular Dysfunction (SOL VD) Prevention and
Treatment trials showed that diabetes accelerated the progression of myocardial
dysfunction 19• These findings were confirmed by Das et al. who showed that diabetic
patients had an increased risk of progression to symptomatic heart failure,
hospitalization and death for heart failure compared with patients with L V dysfunction
due to ischemia without diabetes 20• An analysis of the CHARM (Candesartan in Heart
failure: Assessment of Reduction in Mortality and morbidity) program demonstrated
that diabetes was associated with a greater relative risk of cardiovascular death or heart
failure hospitalization in patients with preserved ejection fraction (HFPEF) than in
patients with reduced EF (HFREF) 21• Finally, also in elderly patients with heart failure
(�70 years of age), in whom comorbidity including diabetes is very common; diabetes
is associated with a worse prognosis 22•
Clearly, we have convincing data showing that diabetes as co-morbidity for
heart failure patients is associated with worse outcome. However, we have limited data
13

Chapter 1
as to what diabetes treatment is best for heart failure patients, and if antidiabetic drugs
my improve heart failure outcome.
Diastolic dysfunction and ventricular (LV) stiffness
Hyperglycaemia � and diabetes
Systolic dysfunction and heart faillure: 'final common pathway'
lschaemic heart disease
Hypertension
<lllf-, Valvular heart disease
.. · .. ···
_.,,
···
.. ·· .. . . . \ ·
············�
............ .
Inherited cardiomyopathy
.. · ••• ··small,
.• • • · lntramyocardial .:
.... --� • ..- and large :"
.,.�·· arteries
• • ••• rR�S
cardiomyocyte
Myocardial fibrosis
Myocardial Infarction
Insulin resistance
Myocardial apoptosis
Metabolic factors
Overload of cellular ca2•
lncreasad oxidative stress Mitochondria dysfunction
Figure 3 Overview of interactions between the myocardial and vascular changes present in diabetic hearts and their contribution to diabetic cardiomyopathy and heart failure. Modified from Asghar O et al. Clinical Science (2009) 116, 741-760. Reprinted with permission.
Oral antidiabetic drugs Today, a variety of treatments is available to clinicians to treat patients with type 2
diabetes. In addition to dietary and physical activity interventions, pharmacological
therapies are playing a central role 1 1• There are five classical types of anti-diabetic
drugs: biguanides, sulfonylureas, meglitinides, thiazolidinediones, and a-glucosidase
inhibitors. Novel compom1ds have recently been introduced: the incretin mimetic drugs
(GLP-1 analogues), the dipeptidyl peptidase (DPP-4) inhibitors, the dual peroxisome
proliferator-activated receptors (PPAR) agonists and the amylin mimetic drugs 23•
There are no prospective trials evaluating if antidiabetic drugs affect heart
failure outcome, however, there is data available to give us directions which drugs
should be first choice. The UKPDS (United Kingdom Prospective Diabetes Study)
demonstrated that long-term metformin treatment significantly reduced incidence of
myocardial infarction and diabetes-related mortality in overweight and obese patients,
and meta-analysis have shown that metformin improves clinical outcome and reduces
all-cause mortality compared to other treatments in patients who had both heart failure
and diabetes mellitus 24
' 25
• In experimental studies, metformin also showed beneficial
14

General introduction
effects on cardiac function by the activation of AMPK. Also the relatively novel incretin hormones and DPP-4 inhibitors are reported to play a protective effect on the cardiovascular system. The actions of GLP-1 on cardiovascular system include I] improvement of endothelial function, cardiac function and myocardial glucose uptake 26• From these data, the suggestion may arise that some oral anti-diabetic agents may exert cardioprotective effects.
Aims of this thesis
Aims of this thesis were: 1) In chapter 2, we reviewed the published data on oral antidiabetic drugs in experimental cardiac remodeling and HF; 2) In chapter 3, we evaluated the cardioprotective effects of metformin in post-MI heart failure; 3) In chapter 4, we evaluated the cardioprotective effects of the DPP-4 inhibitor vildagliptin, either as early or as late intervention in post-MI heart failure; 4) In chapter 5, we investigated the protective effects on DPP-4 inhibitor vildagliptin on the early stage of diabetic cardiomyopathy and explore the molecular mechanisms of diabetic cardiomyopathy; 5) In chapter 6, we evaluated the effects diabetes and in subjects at risk for developing heart failure, who underwent coronary artery bypass grafting ( data from the IMAGINE trial), and 6) In chapter 7, we summarized our findings and suggested clues for future research.
15

Chapter I
References
I . Dickstein K, Cohen-Solal A, Filippatos G, McMurray JJ, Ponikowski P, Poole-Wilson PA, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the diagnosis and treatment of acute and chronic heart failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (I IF A) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur J I lea rt Fail 2008;10:933-989.
2. Levy D, Kcnchaiah S, Larson MG, Benjamin EJ, Kupka MJ, I Io KK, ct al. Long-term trends in the incidence of and survival with heart failure. N Engl J Med 2002;347: 1 397-1 402.
3. McMurray JJ, Petric MC, Murdoch DR, Davie AP. Clinical epidemiology of heart failure: public and private health burden. Eur Heart J 1 998; 19 Suppl P:P9- I 6.
4. Fcrdinandy P, Schulz R, Baxter GF. Interaction of cardiovascular risk factors with myocardial ischcmia/rcperfusion injury, preconditioning, and postconditioning. Pharmacol
Rev 2007;59:41 8-458.
5. Fedak PW, Verma S, Weisel RD, Li RK. Cardiac remodeling and failure: from molecules to man (Part I). Cardiovasc Pathol 2005;14: 1 - 1 1 .
6. Sanderson JE. Heart failure with a normal ejection fraction. lleart 2007;93: 1 55- 158.
7. Fedak PW, Verma S, Weisel RD, Li RK. Cardiac remodeling and failure From molecules to man (Part I I). Cardiovasc Pathol 2005;14:49-60.
8. Boudina S, Abel ED. Diabetic cardiomyopathy revisited. Circulation 2007;1 15:32 1 3-3223.
9. Sharpe N, Smith I I, Murphy J, Greaves S, Hart I I, Gamble G. Early prevention of left ventricular dysfunction after myocardial infarction with angiotensin-converting-enzyme inhibition. Lancet 1991 ;337:872-876.
1 0. Khalil ME, Basher AW, Brown EJ,Jr, Alhaddad IA. A remarkable medical story: benefits of angiotensin-convcrting enzyme inhibitors in cardiac patients. J Am Coll Cardiol
200 1 ;37: 1 757- 1 764.
1 1 . Distefano JK , Watanabe RM. Pharmacogenetics of Anti-Diabetes Drugs. Pharmaceuticals
(Basel) 20 I 0;3:26 1 0-2646.
1 2. Falcao-Pires I, Leite-Moreira AF. Diabetic cardiomyopathy: understanding the molecular and cellular basis to progress in diagnosis and treatment. Heart Fail Rev 201 1 ; e-pub ahead of print.
16

General introduction
1 3 . Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol 1 974;34:29-34.
14. Bertoni AG, Hundley WG, Massing MW, Bonds DE, Burke GL, Goff DC,Jr. I leart failure prevalence, incidence, and mortality in the elderly with diabetes. Diabetes Care 2004;27:699-703.
15 . Held C, Gerstein HC, Yusuf S , Zhao F , Hilbrich L, Anderson C , et al. Glucose levels predict hospitalization for congestive heart failure in patients at high cardiovascular risk. Circulation 2007;1 15 : 1 37 1 - 1 375.
1 6. Ashrafian I I, Frenneaux M P, Opie LI I. Metabolic mechanisms in heart failure. Circulation 2007;1 1 6:434-448.
1 7. Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytes to current diagnosis and management strategies. Vase Health Risk Manag 201 0;6:883-903.
1 8. van den Brom CE, Huisman MC, Vlasblom R, Boontje NM, Duijst S, Lubberink M, et al. Altered myocardial substrate metabolism is associated with myocardial dysfunction in early diabetic cardiomyopathy in rats: studies using positron emission tomography. Cardiovasc Diabetol 2009;8:39.
1 9. Dries DL, Sweitzer NK, Drazner Ml-I, Stevenson LW, Gersh BJ. Prognostic impact of diabetes mellitus in patients with heart failure according to the etiology of left ventricular systolic dysfunction. J Am Coll Cardiol 200 I ;38:42 1 -428.
20. Das SR, Drazner Ml-I, Yancy CW, Stevenson LW, Gersh BJ, Dries DL. Effects of diabetes mellitus and ischemic heart disease on the progression from asymptomatic left ventricular dysfunction to symptomatic heart failure: a retrospective analysis from the Studies of Left Ventricular Dysfunction (SOL VD) Prevention trial. Am Heart J 2004;148:883-888.
2 1 . MacDonald MR, Petrie MC, Varyani F , Ostergren J, Michelson EL, Young JB, et al. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in I leart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur Heart J 2008;29: 1 377- 1 385.
22. de Boer RA, Doehner W, van der Horst IC, Anker SD, Babalis D, Roughton M, et al. Influence of diabetes mellitus and hyperglycemia on prognosis in patients �70 years old with heart failure and effects of nebivolol ( data from the Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors with heart failure [SENIORS]). Am J Cardiol 20 1 0;106:78-86.
17

Chapter I
23. Fisman EZ, Tenenbaum A. A cardiologic approach to non-insulin antidiabctic pharmacotherapy in patients with heart disease. Cardiovasc Diabetol 2009;8:38.
24. Bailey CJ, Grant PJ. The UK Prospective Diabetes Study. Lancet 1 998;352: 1 932; author reply 1 934.
25. Eurich DT, McAlister FA, Blackbum DF, Majumdar SR, Tsuyuki RT, Varney J, et al.
Benefits and harms of antidiabetic agents in patients with diabetes and heart failure: systematic review. BMJ 2007;335:497.
26. Jax T. Treatment of patients with diabetes with GLP-1 analo!:,'1.ICS or DPP-4- inhibitors: a hot topic for cardiologists? Clin Res Cardiol 2009;98:75-79.
1 8

Chapter 2
Variable effects of anti-diabetic drugs in animal
models of myocardial ischemia and remodeling:
lessons for the cardiologist
Meimei Yin, Maxi Meissner, Wiek H. van Gilst, Rudolf A. de Boer
University Medical Center Groningen, University of Groningen, Department of Cardiology, Groningen, The Netherlands
Submitted

Chapter 2
Abstract
Diabetes and heart failure are very prevalent and it has been demonstrated that they affect each other mutually. Novel therapies to reduce post-myocardial infarction (Ml) remodeling which subsequently leads to heart failure are urgently needed, especially in diabetic patients. Clinical studies have suggested that some agents, like mctformin, exert a cardiovascular protective role in heart failure patients with diabetes, whereas other oral antidiabetic against may be disadvantageous. Herc, we provide an overview of oral antidiabetic drugs on post-MI animal studies with respect to their cardiospecific effects. The aim of the current paper is to summarize the experimental data of the most commonly subscribed anti-diabetic agents (biguanidcs, sulfonylurcas, thiazolidincdioncs) on diabetes and heart failure and to compare these with the data available for the newer compounds (the incrctin mimetic drugs glucagon-like peptide 1 (GLP-1) and the dipcptidyl peptidase (DPP-4) inhibitors. Metformin has proven effects in ameliorating cardiac remodeling in different models of heart failure. Sulfonylurea derivatives are controversial with respect to their direct effects on the cardiovascular system. G LP- 1 has a potential to play a beneficial effect on cardiovascular system. Thiazolidinediones are beneficial against myocardial ischemia-reperfusion injury but that their effects on post-MI remodeling are less clear, and clinical studies raised concerns with respect to their cardiovascular safety. Altogether, the available experimental evidence indicates that some anti diabetic agents should be preferred over others if cardioprotective effects arc warranted. These experimental clues should be confirmed in clinical trials. Current clinical guidelines, in absence of such clinical trials, neglect experimental and mechanistic data and provide generic recommendations only.
20

Oral antidiabetic drugs in post-MI remodeling
Introduction:
Heart Failure and Diabetes - a reciprocal relation The prevalence of diabetes mellitus is rapidly growing due to lifestyle and the aging population. Cardiovascular complications are the leading cause of diabetes-related morbidity and mortality. First, because diabetes is associated with other cardiovascular risk factors such as hypertension, dyslipidemia, but most importantly because diabetes leads to accelerated atherosclerosis, involving all large arterial beds: carotid, aorta, femoral, and the coronary arteries 1
• Coronary artery disease (CAD) is the leading cause for heart failure 2, either due to sustained ischemia or via myocardial infarction (MI), followed by a process of myocardial remodeling, in the end resulting in heart failure (Figure 1 ).
Insulin resistance
ndothelial ysfunction
l
/ 1 '911!A!"!'b•n•o•rm•a-.!I•
metabolism
1 Diabetic
cardiomyopath
Coronary artery disease
l Myocardial infarction
l Left ventricular remodeling
l Heart failure
Figure 1 Overview of the interaction between diabetes and heart failure
Diabetic patients have a higher risk for developing heart failure, and apart from this, heart failure patients with diabetes have worse prognosis compared to heart failure patients without diabetes, as reported in numerous reports 3-5_ Furthermore, heart failure itself also bears an increased risk for new onset diabetes 6• 7, so that diabetes and heart failure have a reciprocal relation. Despite availability of effective treatments, heart failure remains one of the most common causes of death and health care
2 1

Chapter 2
expenditure. Therefore, novel therapies to reduce (post-Ml) cardiac remodeling and subsequent heart failure are urgently needed, and this need is particularly strong in diabetic patients. Currently, a wide array of oral antidiabctic agents is available which have primarily been evaluated for their glucose lowering capacity. However, recently there have been several reports questioning whether all these agents are safe in patients with risk for or established cardiovascular disease. Some drugs have been fiercely under debate because of safety concerns and increased risk for cardiovascular outcomes, like rosiglitazone 8
• There are no prospective studies comparing the cardioprotective effects between different oral antidiabetic agents. We herein provide an overview of available experimental data of oral antidiabetic agents with respect to their cardiospecific effects, and postulate that these effects could be of help in choosing a therapeutic regimen in diabetic patients with concomitant cardiovascular disease, and specifically heart failure.
Heart Failure and anti-diabetic medication Anti-diabetic medications arc primarily aimed to lower blood glucose levels. There are five classical types of anti-diabetic drugs: biguanides, sulfonylurca derivatives, mcglitinidcs, thiazolidinediones, and a-glucosidase inhibitors. Recently, novel compounds for diabetic treatment have been introduced on the market: the incrctin mimetic drugs (GLP-1 analogues), the dipeptidyl peptidase (DPP-4) inhibitors, the (dual) peroxisome proliferator-activated receptors (PPAR) agonists, and the amylin mimetic drugs 9• All drugs have established glucose lowering effects, and based on experience, tolerability, safety profile and price, they are indicated for type 2 diabetes as described in the guidelines 1 0•
Recent published data from a meta-analysis has suggested that metformin improves clinical outcome and reduces all-cause mortality when compared to other treatments in patients suffering from both heart failure and diabetes 1 1 • 1 2• From these data, the suggestion arises that some oral anti-diabetic agents may exert superior cardioprotection over others. Given the comparable effects on blood glucose that most oral anti-diabetics share, it is unlikely that these differences arc simply explained by better glycemic control. However, mechanistic studies with different oral anti-diabetic agents primarily addressed the glycometabolic mechanisms of these compounds, while direct effects on other organs, including the heart have not been given much emphasis herein.
In the current paper, we focus on the cardiospecific effects of the most commonly subscribed anti-diabetic agents on diabetes and heart failure and to compare these with the data available for the newer compounds.
22

Oral antidiabetic drugs in post-Ml remodeling
Classical medication
Metformin and cardiovascular effects Metformin is the only drug belonging to the biguanides class and is currently utilized as first line anti-diabetic agent in most parts of the world. It decreases blood glucose levels by enhancing insulin sensitivity involving two major mechanisms: first, by an increased peripheral uptake of glucose (mainly skeletal muscles) in the presence of insulin, and second by a decreased hepatic glucose output through suppression of gluconeogenesis while lowering plasma insulin concentrations 1 3. Compared to other anti-diabetic medication, the use of metformin also includes ancillary, nonhypoglycemic effects, such as improving both serum lipid profile and fibrinolytic activity 9• In addition, metformin has been shown to have effects that mimic caloric restriction, i.e. less body weight gain 14, and thus appears to be the drug of choice in obese patients. Clinical observations suggest that metformin might have direct cardioprotective effects independent of its glucose-lowering action: patients with type 2 diabetes treated with metformin had a lower risk of all-cause mortality and myocardial infarction compared to other anti-diabetic medication 1 5• 1 6• Recent experimental data suggest possible mechanisms for metformins' cardioprotective effects, including reduction of myocardial ischemia-reperfusion injury as well as attenuated fibrosis and cardiac remodeling, e.g. in post-MI remodeling.
Metformin limits myocardial ischemia-reperfusion injury (Table 1) Substantial evidence from experimental research demonstrates that metformin is beneficial in protecting the heart from ischemia-reperfusion injury. For example, in an isolated working rat heart model, low dose metformin was found to increase coronary blood flow before ischemia and during reperfusion, which was associated with improved cardiac function 17• Furthermore, another study demonstrated that a single oral dose of metformin (250 mg/kg body weight), administrated 24 hours before coronary occlusion, significantly reduced infarct size in a rat Langendorff-perfused heart. Interestingly, 2 hours after metformin administration an approximately two-fold increase in AMPK-a2 activity was observed 18• AMPK-a2 is a protein necessary for the maintenance of myocardial energy homeostasis during ischemia 1 9• The metformininduced decrease in infarct size in rats was reproduced in a murine myocardial ischemia-reperfusion injury model. In this study, metformin administration (125 µg/kg; intraperitoneal injection) before the ischemic period decreased myocardial reperfusion injury in mice, associated with concomitant activation of AMPK and endothelial nitric oxide synthase ( eNOS) phosphorylation, which both appear to be crucial for limiting infarct size 20• Further evidence for metformins' cardioprotective properties upon
23

Chapter 2
ischcmia stems from a study in both isolated perfused Wistar and diabetic GotoKakizaki rat hearts. Here, coronary perfusion with metformin (50 µmol/L in the pcrfusate during the first 15 minutes of repcrfusion) reduced infarct size through Aktmcdiatcd inhibition of mitochondrial permeability transition pore opening 2 1 . In contrast, the cellular mechanism of cardioprotection by AMPK activation was not confirmed by Bhamra ct al 2 1 • Possible factors accounting for the discrepancies in findings may be related to different dose utilized in this study. An identical, infarct size limiting effect was later confirmed by other studies 22• 23. However, further support for mctformins' effect on reducing infarct-size is evident from a study in type 2 diabetic rats where oral metformin administration (200 mg/kg/day) led to significant reduction of infarct size compared to controls 24
. Altogether, these studies offer insights into the cardioprotective effect of metformin in limiting myocardial ischcmia-rcpcrfusion injury by mechanisms entailing an increased AMPK activity and eNOS phosphorylation, leading to reduced myocardial infarct size and improved cardiac function.
The effect of metformin on post-infarct remodeling and heart failure (Table 1) Importantly, the cardioprotective benefits of metformin are not limited to models of myocardial reperfusion injury but further extend to murine, rat and dog models of postmyocardial infarction where mctformin treatment consistently ameliorated long-term cardiac remodeling. First, in a murine model of permanent left coronary artery occlusion metformin, administered to mice before ischemia and then daily for 4 weeks ( 1 25 µg/kg; i.p. injections), improved 4-week survival from 30 to 44% 25• The underlying factors prolonging survival upon metformin administration appear to be associated with improved cardiac function as treated mice displayed preserved LV dimensions and LV ejection fraction at 4 weeks. In this model AMPK, eNOS phosphorylation and increased peroxisomc proliferator-activated receptor-gamma coactivator (PGC)-1 alpha expression appear to be central players in metformins ' cardioprotcctivc effects. Importantly, AMPK, cNOS and PGC- l alpha are all regulators of cellular energy metabolism.
The metformin-induced improvements in L V ejection fraction were confirmed in rat studies using myocardial infarction after permanent coronary ligation 26• 27
•
Administration of metformin (250mg/kg) during 12 weeks led to significant reductions in infarct size and left ventricular dilatation 26
. Further, metformin treatment for 4 weeks ( IO0mg/kg) significantly improved cardiac function ( increased L V systolic pressure, increased LV ejection fraction and decreased LV end diastolic diameter) 27•
The beneficial effects of metformin in these rat studies were not only associated with the previously observed increases in AMPK and cNOS phosphorylation, but also with
24

Oral antidiabetic drugs in post-MI remodeling
a reduction in plasma insulin which may contribute to the cardioprotective effects of
metformin.
In addition, metformin also reduces myocardial fibrosis by reducing key fibrotic
factors, including transforming growth factor (TGF)-Pl , basic fibroblast growth factor
(bFGF), and tumor necrosis factor (1NF)-alpha levels in the circulation and/or the
myocardium 27• Similarly, anti-fibrotic effects of metformin were also observed in
other experimental heart failure models, including a dog model of rapid pacing 28
and
murine pressure overload models, where a decreased expression of TGF-Pl was
observed 29
•
Additionally, metformin has also been shown to attenuate the development of
diabetic cardiomyopathy in diabetic mice via activation of AMPK 30•
However, in contrast to the earlier observations in post-MI models, metformin
had no effects on cardiac structure and function, and did not activate AMPK, in a
volume-overload-induced heart failure model 3 1• These results suggest that the
protective effects may not be universal to all forms of heart failure.
Nucleus
PGC-1 a Promoter
Metformin
LKB1
CaMKK ------�
I I
j PGC-1a
I
Ca2+
Inflammation + Protein Synthesis; Mitochondrial Function + Hypertrophy
Figure 2 Metfonnin activates AMPK phosphorylation, regulates cellular glucose signaling pathways, protein synthesis, and energy metabolism. Modified from Facundo HT et al, Circ Res 2009; 104(3):282-4 32•
25
II

Chapter 2
Taken together, convincing evidence has accumulated demonstrating that
metformin ameliorates cardiac remodeling in different models of heart failure in
several species, The underlying mechanisms appear to be related to improved substrate
sensing mechanisms, such as increased AMPK activation and eNOS phosphorylation
(as showed in Figure 2), as well as decreases activation of fibrosis-inducing players,
such as reduced TGF-Pl .
Sulfonylurea derivatives and the cardiovascular system
Sulfonylurea derivatives are the first class widely used oral anti-hyperglycemic
medication and they have been used for the treatment of type 2 diabetes mellitus for
nearly half a century. Sulfonylurea derivatives are insulin secretagogues with a
hypoglycemic potency which is directly related to baseline plasma glucose values 33•
Further, the cellular mechanism of sulfonylurea derivatives is triggering insulin
secretion by closing the ATP-dependent potassium channels in the pancreatic beta cell
membrane (Figure 3). KATP channels have been identified not only in pancreatic P-cells,
but also in neuronal cells, skeletal muscle, vascular and nonvascular smooth muscle
cells 34
•
Figure 3. Targets or action or sulfonylurea derivatives in the pancreatic beta-cell and the cardiomyocyte. Sulfonylurea drugs inhibit KATP channels and prevent K+ efflux through the channel pore, leading to membrane depolarization and opening of voltage-sensitive Ca2+ channels, which allows influx of calcium into the cell. Ca2+ influx induces insulin release in pancreatic beta-cell and increased contractility, ATP use, and action potential duration in the cardiomyocyte. Adapted and modified from 35•
26

Oral antidiabetic drugs in post-M I remodeling
Cardiac and vascular sulfonylurea receptors have been shown to have a different structure from their pancreatic analogue 35. KATP channels are reported to play a protective effect in the ischemic myocardium, regulating the coronary blood flow and protect cardiovascular cells from ischemia/reperfusion injury 36• In the healthy heart, blockade of KATr channels by sulfonylurea derivatives have been reported to reduce resting myocardial blood flow by 20% in a dog model 37
• During ischemia, sulfonylurea derivatives may inhibit the cell hyperpolarization that protects the cell by Ill attenuating calcium accumulation 35 (Figure 3). Thus, from experimental data it seems a that inhibition of cardiovascular KATr channels by sulfonylurea derivatives may lead to increased cardiovascular risk 38.
Sulfonylurea derivatives on myocardial ischemia-reperfusion injury (Table 1) Studies elucidating the effect of sulfonylurea derivatives on myocardial ischemiareperfusion injury have shown contradictory results, and it is challenging to put data into perspective. For example, glibenclamide, the second generation and widely prescribed anti-diabetic drug of this class, was first shown to have beneficial actions on myocardial ischemia-reperfusion injury, including a significantly improved functional recovery at 45 min in the reperfusion period and decreased cardiac lactate accumulation when administered as pre-treatment, although only at very high dose (50 µM) 39. In contrast to the protective effects observed in the first study, glibenclamide prolonged recovery time from ischemia in another study using isolated hearts 40•
However, despite the increased recovery time from ischemia in the latter study, cardioprotective effects including a significantly improved ischemia-induced cardiac functional loss as well as ischemia-induced intracellular acidosis were reported by Legtenberg et al 41
, thus suggesting sulfonylurea-induced cardiac-protection by glibenclamide. This was associated with a decrease in coronary blood flow, which was by another study in isolated perfused rat hearts that were treated with glibenclamide (3x 10-8mol/L) and glimepiride ( I x l0-7 mol/L), both leading to significant reduction in coronary perfusion flow upon reperfusion. Moreover, at 30 minutes of reperfusion in this study, glibenclamide induced a significant increase in left ventricular end-diastolic pressure and significant decreases in left ventricular systolic pressure, left ventricular developed pressure, and the maximum first derivative of left ventricular pressure, while glimepiride induced a significant decreases in left ventricular developed pressure and the maximum first derivative of left ventricular pressure, suggesting that the effects of both drugs on the cardiac function was differential by both sulfonylurea derivatives 42
•
Interestingly, the cardio-protective effect of glibenclamide is, most likely, not attributable to myocardial KATP channel blockade, as glibenclamide preserved pH but not ATP levels during ischemia while it was indicated that the cardioprotective effect of glibenclamide may be explained by inhibition of glycolysis. 41
27
Chapter 2
Unlike glibenclamide, the beta-cell selective sulfonylurca (R)-ACX does not aggravate cardiac ischemia-reperfusion damage as shown in a study using the isolated guinea pig model 43• Collectively, the effects of sulfonylurea derivatives on cardiac ischemia-reperfusion injury are still debated. Altogether the current data available describing the effects of sulfonylurea derivatives on cardiac ischcmia-reperfusion injury are not conclusive more research is needed herein for clarification.
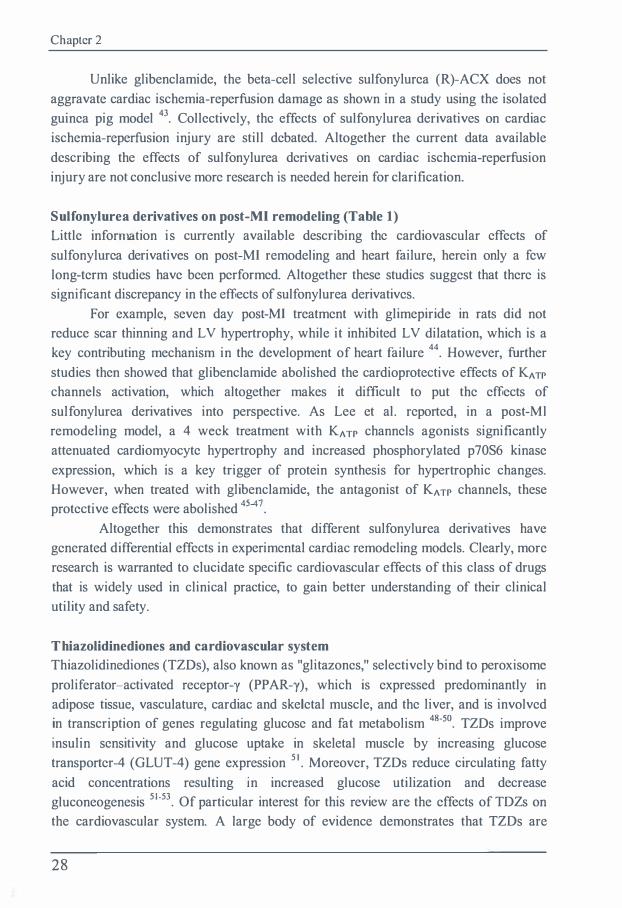
Sulfonylurea derivatives on post-Ml remodeling (Table 1) Little information is currently available describing the cardiovascular effects of sulfonylurca derivatives on post-MI remodeling and heart failure, herein only a few long-term studies have been performed. Altogether these studies suggest that there is significant discrepancy in the effects of sulfonylurea derivatives.
For example, seven day post-MI treatment with glimepiride in rats did not reduce scar thinning and L V hypertrophy, while it inhibited L V dilatation, which is a key contributing mechanism in the development of heart failure 44
. However, further studies then showed that glibenclamide abolished the cardioprotective effects of KATP
channels activation, which altogether makes it difficult to put the effects of sulfonylurea derivatives into perspective. As Lee et al. reported, in a post-Ml remodeling model, a 4 week treatment with KATP channels agonists significantly attenuated cardiomyocyte hypertrophy and increased phosphorylated p70S6 kinase expression, which is a key trigger of protein synthesis for hypertrophic changes. However, when treated with glibenclamide, the antagonist of KATP channels, these protective effects were abolished 4547
.
Altogether this demonstrates that different sulfonylurea derivatives have generated differential effects in experimental cardiac remodeling models. Clearly, more research is warranted to elucidate specific cardiovascular effects of this class of drugs that is widely used in clinical practice, to gain better understanding of their clinical utility and safety.
Thiazolidinediones and cardiovascular system Thiazolidinediones (TZDs), also known as "glitazones," selectively bind to peroxisome prolifcrator-activated receptor-y (PPAR-y), which is expressed predominantly in adipose tissue, vasculature, cardiac and skeletal muscle, and the liver, and is involved in transcription of genes regulating glucose and fat metabolism 48-50• TZDs improve insulin sensitivity and glucose uptake in skeletal muscle by increasing glucose transportcr-4 (GLUT-4) gene expression 5 1
• Moreover, TZDs reduce circulating fatty acid concentrations resulting in increased glucose utilization and decrease gluconeogenesis 51
•53_ Of particular interest for this review are the effects of TDZs on
the cardiovascular system. A large body of evidence demonstrates that TZDs are
28

Oral antidiabetic drugs in post-Ml remodeling
beneficial in improving cardiovascular risk by their favorable effects on lipid metabolism and the vascular endothelium 54
.
Thiazolidinediones and myocardial ischemia-reperfusion injury (Table 1) A number of experimental studies have been performed to investigate the protective effect of TZDs on myocardial ischemia-reperfusion injury. Herein, a large variety of different TZDs have been utilized, all consistently showing protective effects against myocardial ischemia-reperfusion injury.
The protective effect of TZDs on myocardial ischemia-reperfusion injury was first shown in 2001 by Yue et al 55
• The authors demonstrated that the PPAR-y agonist rosiglitazone (3 mg/kg/day) reduced myocardial infarction by 37% and improved contractile dysfunction after a 30 min of coronary ligation followed by 24 hours reperfusion. Moreover, pretreatment with rosiglitazone (3 mg/kg/day) for 7 days further reduced infarct size and also resulted in significant improvement of left ventricular systolic pressure and contractility 55• The reduction of infarct size by another TZD, pioglitazone, was then confirmed in a rat model of regional myocardial ischemia and reperfusion by Wayman and Ito 56• 57
. Further evidence for the infarctsize limiting effect of TZDs stems from a study employing a canine model of acute myocardial infarction utilizing troglitazone 58. ln this study it was shown that the cardioprotective of troglitazone was associated with an attenuated expression of connexin43, which has a crucial role in the synchronized contraction of the heart, in the border zone of the infarct. Moreover, administration of pioglitazone prior to ischemia reduced infarct size by 20% in male Sprague-Dawley (SD) rats 59. The authors suggested that the PBK and P42/44MAPK pathway may be the underlying mechanism herein as these two pathways showed to regulate the survival of the cardiomyocytes. A similar molecular mechanism was described in myocardial ischemia-reperfusion study ( I hour of myocardial ischemia followed by 1 hour of reperfusion) in SD rat hearts after 7 days of pretreatment with rosiglitazone (3 mg/kg/day) 60• The rosiglitazonetreated group displayed a significantly reduced infarct size with concomitant inhibition of p42/44 MAPK 60.
Other mechanisms that have been postulated to mediate the protective effects of TZDs on myocardial ischemia-reperfusion injury include: decreased cardiomyocyte apoptosis 61
, increased phosphorylation of Akt, p42/44 MAPK and eNOS, and inhibition of Bax activation 62-65
. For example, pioglitazone significantly improved heart rate and contractility (dP/dtmax) at 1 and 30 minutes after reperfusion in rats, which was associated with Akt phosphorylation 62
• Interestingly, pioglitazone has been shown to inhibit cardiomyocyte apoptosis and inhibiting MMP-2 6 1
, reduce mitochondrial ultrastructural injury and membrane potential loss in the
29

Chapter 2
ischemic/reperfused SD rat heart , thus indicating that its protective effects may be related to opening mitochondrial(ATP)-sensitive potassium channels 66· 67.
In contrast, a subsequent study utilizing a rabbit ischemia-reperfusion model found that pioglitazone reduced infarct size by activation of PP AR-y, PB-kinase, Akt, and cNOS pathways, but not via opening the mitochondrial KATP channel 68. Similar findings were observed in a mouse model 69' 70• Additionally, continuous infusion of rosiglitazone (0.5 mg/kg/h) significantly reduced infarct size by 20% in Wistar rat hearts after ischemia/reperfusion (30 minutes/4 hours) 7 1 . The authors of this study found that nuclear factor-kappa B (NFKB) phosphorylation was inhibited in the infusion group leading them to conclude that the underlying mechanism responsible for the reduction in infarct size constitutes the inhibition of the NFKB pathway 7 1 .
Notably, activation of Akt appears essential for the cardioprotcctivc effects of TZDs. Administering rosiglitazone (3 mg/kg/day) to the Zucker Diabetic Fatty (ZDF) rat led to protection of the heart from ischemia-reperfusion myocardial injury by activating Akt 72 as similar findings as pioglitazone m non-diabetic · h ·a1 fu · · · 62 64 68-70 1sc cm1 rcper s1on mJury · · .
To summarize, TZDs have consistently shown to decrease experimental myocardial ischemia-reperfusion injury and infarct size. Suggested mechanisms arc activation of Akt, eNOS, and p42/44 MAPK as the mediators of this beneficial effect.
Thiazolidinediones and post-Ml remodeling (Table 1)
The effects of TZDs on heart failure and left ventricular remodeling are more controversial. Mice treated with pioglitazone (3 mg/kg/day) for 4 weeks after large anterior Ml displayed significantly attenuated LV dilatation and dysfunction with pioglitazonc treatment, while L V end-diastolic pressure was decreased and L V dP/dt (max) was partially normalized 73. These improvements were associated with a decrease in myocytc hypertrophy, interstitial fibrosis and a reduced expression of genes implicated in fibrotic and inflammatory pathways, such as TNF-alpha, TGF- (3 1 , and monocytc chemo-attractant protein-I 73. However, in a subsequent study, the same dose of rosiglitazone (3 mg/kg/day) did not modulate LV remodeling and rather increased mortality after 8 weeks post-MI in rats 74. In a further investigation in mice subjected to Ml prior to the onset of treatment, pioglitazone (20 mg/kg) had no effect on LV remodeling, survival, metabolic parameters, inflammation, collagen deposition and endothelial function 75. In contrast, utilizing a rat model with rosiglitazone (3 mg/kg/day) for 8 weeks, Geng et al. demonstrated a beneficial effect of rosiglitazone on post-MI L V remodeling, evidenced by improvement in LV dP/dt max and decreased collagen formation, partly by suppressing myocardial angiotcnsin II and aldosterone, while no effect on mortality was noted 76. However, adding to the flurry of data, Linz et al. reported that rosiglitazone exacerbated cardiac dysfunction in Sprague Dawley rats
30

Oral antidiabetic drugs in post-MI remodeling
with permanent ligation of the left coronary artery 77• In addition to these post-MI
remodeling studies, an increase in myocyte size and atrial natriuretic factor was
observed in pioglitazone treatment (3 mg/kg/day) for 4 weeks in a rat model of aortic
banding 78•
Taken together, there is clear evidence that TZDs are beneficial against
myocardial ischemia-reperfusion injury. However the effects on post-MI remodeling
are unclear. Differences in study design and dose regimen are most likely the
underlying causes for discrepancies in findings between all these studies, and clearly
careful future investigation is warranted to further clarify herein.
New generation anti-diabetic drugs
Glucagon-like peptide analogues and DPP-4 inhibitors Glucagon-like peptide-I (GLP-1) is secreted by entero-endocrine L-cells of the
intestinal mucosa and released into the circulation in response to food intake. GLP-1
analogues have been used for treatment of type 2 diabetes since it improves insulin
secretion, P-cell proliferation and survival 79-8 1• For these reasons, GLP-1 is an
attractive target in the treatment of type 2 diabetes. However, targeting endogenous
GLP is clinically impractical by itself as its half life is only a few minutes due to its
rapid inactivation by the enzyme dipeptidyl peptidase-4 (DPP-4). Therefore, an
analogue of GLP-1 appears more beneficial. Herein, exenatide (also known as
Exendin-4) and liraglutide have already been approved by the FDA as GLP analogues
to treat type 2 diabetes. An alternative approach for enhancing GLP-1 bio-availability
and thus action involves the use of DPP-4 inhibitors (Figure 4). The DPP-4 inhibitors
sitagliptin 82 and saxagliptin 83 have been approved by the FDA as treatment for type 2
diabetic patients in the United States, while vildagliptin has been approved in Europe
as anti-diabetic treatment 84
•
GLP-1 and the cardiovascular system GLP-1 receptors (GLP-IR) are expressed in various tissues outside the pancreas, and
also in rodent and human heart and vascular tissue 85• The function of these receptors in
heart and vasculature are under study. GLP-IR deficient mice have shown to exhibit
increased L V thickness, impaired L V contractility and impaired L V diastolic function,
compared to control mice 86, clearly indicating the importance of this receptor for the
cardiovascular system. Moreover, in a clinical study, 3-day infusion of GLP-1
improved LV function in patients after acute myocardial infarction 87• Thus, in addition
to the effects on glucose metabolism, GLP-1 has been proven to exert cardiovascular
effects 88•
3 1
n

Chapter 2
Food DPP-4
DPP-4 Inhibitor l l Intestine --+ r-A-ct-i-ve_G_L_P ___ 1_ ----+
GLP-1 metabol ite Inactive
- - - . Figure 4 Secretion and metabolism of glucagon-Iike peptide-I (GLP-1 ). Following ingestion of a meal, GLP-1 is released from the intestine in its active form (7-36) in plasma, which is rapidly degraded to the inactive form (9-36) by the enzyme dipeptidyl peptidase-4 (DPP-4). Incretin therapy can increase available GLP-1 activity by inhibiting its enzymatic degradation using DPP-4 inhibitor to prolong the activitv ofGLP-1 .
-
A ? BAD CaspaH Activation
\ I Decreased
Cardiac Myocyte Apoptosls
Figure S. GLP-lR-dependent intracellular signal transduction pathways in the cardiomyocyte. Activation of the GLP-lR leads to a reduction in apoptosis and increase in glucose u�take. ROS, Reactive oxygen species. AC, Adenylate cyclase. Reprinted with permission from the publisher.
32

Oral antidiabetic drugs in post-M l remodeling
GLP-1 limits myocardial ischaemia-reperfusion injury (Table 2) Acute GLP- I infusion studies in rodents showed, for the most part, consistent beneficial cardiac effects entailing a decrease in infarct size and improved L V function. For example, ischemia/reperfusion experiments in rats showed that GLP- I administration prior to ischemia leads to smaller infarct size in the isolated heart 90•92•
Another ischemia-reperfusion study showed that only the GLP- 1 analogue exendin-4, but not GLP- I(9-36) amide exerts infarct-limiting action, while both of them improved LV performance 93• This was partially confirmed by Ossum, et al 94, who studied 30 minutes low-flow ischemia and 30 minutes reperfusion. GLP-I enhanced recovery with significant improvements in L V end-diastolic pressure and L V developed pressure after ischemia, increased LV function, myocardial glucose uptake, and GLUT-I and GLUT-4 translocation during reperfusion, in association with increased p38 MAPK activity and enhanced NO production in isolated rat hearts 95 (Figure 5). Another study then demonstrated that both GLP- I and its metabolite GLP- I (9-36) exerted cardiac and vascular protective effects in isolated mouse hearts after ischemia-reperfusion injury as demonstrated by increased functional recovery, glucose uptake, cAMP and cGMP release, left ventricular developed pressure, and coronary flow 96• However, a study with liraglutide, a long-acting GLP-I analogue, showed no effect on infarct size and hemodynamic parameters in a porcine model 97• Then, applying liraglutide to both healthy and diabetic mice showed higher survival in treated mice with concomitant improved cardiac output. This was associated with the expression and activity of cardioprotective genes in the mouse heart, including Akt, GSK-3P, PPARbeta-delta, Nrf-2, and HO-I 98
. Exenatide was found to play a beneficial effect on ischemiareperfusion in both an adult rat 99 and porcine model, associated with a higher Akt and Bcl-2 phosphorylation and lower active caspase-3 expression 1 00 (Figures 5). Fusion of GLP-1 to human transferrin (GLP- I -Tf) significantly reduced the infarct size and apoptotic index of the cardiomyocytes. Wall motion abnormality and ejection fraction was significantly improved in the post-ischemic group relative to the control group 1 0 1
•
The effect of GLP-1 on post-infarct remodeling and heart failure Only few chronic studies have addressed the effects of GLP- I on cardiac function in post-MI remodeling. A chronic (3 month) infusion study showed that GLP- I improved LV systolic function and prolonged survival in spontaneously hypertensive rats by increasing myocardial glucose uptake and reducing myocyte apoptosis 1 02• Treatment either with GLP-I or the exenatide analogue AC3 I 74 also demonstrated promising cardioprotective effects, including improved L VEF, LV end-diastolic pressure, and cardiac dimensions in a rat MI model 1 03• Further, recombinant GLP-- I increased myocardial insulin sensitivity, glucose uptake and improves left ventricular performance which was associated with significant increases in L V hemodynamic
33

Chapter 2
parameters and systemic vascular resistance in conscious dogs with pacing-induced dilated cardiomyopathy 1 04
• In a type l diabetic rat model, 14 day infusion of GLP-1 analogue cxcndin-4 showed an early protection of cardiac remodeling 105•
Dipeptidyl peptidase-4 inhibitors (Table 2) Two acute studies addressed the role of DPP4 inhibitors in cardioprotection. A study with the DPP-4 inhibitor PFK275-055 (a vildagliptin-analoguc) showed a reduced infarct size with activation of the cardioprotective RISK (reperfusion-induced salvage kinase) pathway in pre-diabetic rats 106
, whereas a study with the DPP-4 inhibitor sitagliptin showed that infarct size or short-term cardiac function were not affected by treatment 1
07• This result was in line with another study which also showed that sitagliptin was associated with a reduction of infarct size 65. However, data on longterm studies of DPP-4 inhibitor on post-MI remodeling arc limited. Administration of vildagliptin for 12 weeks had no beneficial effects on parameters of LV function or cardiac gene expression in nondiabctic rats after coronary artery ligation and development of ischemic cardiac remodeling 1 08• Further studies are needed.
Translation to clinical practice
Over the years, several clinical studies and registries evaluated the safety and efficacy of oral anti-diabetic drugs on cardiovascular risk (Table 3). In general, glucose lowering regimens are associated with less diabetic complications, as shown by the multiccntcr UKPDS study that presented data on long-term oral anti-diabetic agents or insulin treatment and the associated reduction in development of microvascular complications in newly diagnosed type 2 diabetes mellitus 109• It has become apparent that mctformin is the superior oral anti -diabetic drugs in preventing cardiovascular events 15 • Compared to other anti-diabetic drugs, metformin is not only associated with a reduction of morbidity in patients with heart failure 1 10 but also with a lesser cardiovascular hospitalization and all cause mortality 1 1 1 • Both clinical and experimental studies have suggested that metformin may play a beneficial role in the cardiovascular system and could be a novel treatment for patients with myocardial infarction or heart failure, especially for pre-diabetic and obese patients.
Contrasting to metformins ' promising results, clinical studies with sulfonylurea derivatives have produced conflicting results. A large US multicenter trial, the University Group Diabetes Program (UGDP), was the first to report that tolbutamide treatment caused adverse cardiovascular effects in human patients 1 12•
Although several experimental studies have suggested that sulfonylurea derivatives may exert a harmful effect on ischemic-rcperfusion injury, as reviewed above, the
34

Oral antidiabetic drugs in post-Ml remodeling
UKDPS study did not observe a higher risk of myocardial infarction in patients who received sulfonylurea derivatives compared with those treated with insulin alone 109•
Higher mortality was found on a combined sulfonylurea derivative and metformin regimen in patients with coronary artery disease compared with monotherapy with sulfonylurea derivatives 9• Moreover, some clinical studies showed a decreased incidence of cardiovascular complications in patients on sulfonylurea derivatives 52• Collectively, the benefits and harms of sulfonylurea derivatives on the cardiovascular system in clinical practice remain debatable and further investigations need to be performed. Cautious use of sulfonylurea derivatives in patients post-MI or with heart failure seems to be indicated.
Although experimental findings suggest a possible benefit of TZDs in cardiovascular protection, clinical data on cardiovascular outcome are questionable. Three meta-analyses indicated an increase in the incidence of MI and heart failure for TZDs (in particular rosiglitazone, to a lesser pioglitazone) compared to placebo 1 13- 1 15_
TZDs were associated with increased risk of hospital admission for heart failure but were associated with reduced all cause mortality 1 2• The open label trial Rosiglitazone Evaluated for Cardiac Outcomes and Regulation of glycemic in Diabetes (RECORD) did not observe any effects of rosiglitazone on all-cause mortality; however, a higher frequency of heart failure was found in this study 1 16• 1 1 7
• In a recent clinical trial, Pioglitazone Effect on Regression of Intravascular Sonographic Coronary Obstruction Prospective Evaluation (PERISCOPE), pioglitazone treatment led to a significantly decreased rate of progression of coronary atherosclerosis in diabetic patients with coronary artery disease 1 18• To date, the understanding of TZDs on cardiovascular risk and mortality is still limited; partially due to incomplete knowledge of the underlying molecular mechanisms, that are expected to be very complex for agonists of the transcription factor PPAR-y.
Newer anti-diabetic agents, including GLP-1 and its analogues, have been reported to play a protective role on the cardiovascular system in experimental models. Since DPP-4 inhibitors increase the endogenous level of GLP-1 by inhibiting its degradation, DPP-4 inhibitors are also considered to have similar effects as GLP-1 and its analogues. However, these medications have been used only for a few years and no data on large clinical trial are yet available, more long-term studies on cardiovascular effects are ongoing.
In conclusion, based on the literature review mentioned above, metformin should be strongly recommended for diabetic patients with concomitant cardiac disease. Metformin exerts beneficial effects on the cardiovascular system, both in experimental studies as well as in (post-hoc) clinical observations. Data on sulfonylurea derivatives and TZDs have shown controversial results; their use in diabetic patients with cardiovascular disease is under debate and needs further study. In current guidelines,
35

Chapter 2
these classes of drugs are recommended if patients remain hyperglycemic despite metformin use, and no remark with respect to cardiac disease or condition is made. We believe clinicians should use these drugs cautiously. For the more recently developed anti-diabetic agents, the experimental data are promising. However, based on the experiences with sulfonylurea derivatives and TZDs, clinical studies are needed to confirm these promising effects in diabetic patients with high cardiovascular risk.
36

v.) -..)
Table 1 Effects of classical antidiabetic agents in non-diabetic post-MI animal models.
Antidiabetic agents
Biguanides Metformin
Sulfonylureas (Glibenclamide ,gliclazide)
Thiazolidinediones (TZD): (pioglitazone, rosiglitazone)
Acute studies
! Infarct size ,1. 18 . 20-22
t AMPK and eNOS activation 18· 20, 22
t Akt phosphorylation 2 1 No AMPK activation 21
l the time to ischemic contracture 39 t recovery time from ischemia 40 t functional recovery 41
l lactate accumulation 41 l coronary blood flow 41 42
t LVEDP, l LVESP 42
l Infarct size 55-71
t LVESP and dP/dt max and min 550 6 1
l phosphorylation connexin43 proteins 58 f p-Akt 62. 65. 68-70 I eNOS 64, 65, 68, 69 l p42/44 MAPK 60• 65
t PKA 66 l apoptosis 61· 67
l apoptotic cell number 28
Chronic studies
l expression of ANP, BNP, 26- 28
l TGF- f3 128 29 t p-AMPK and eNOS 25·28
l collagen volume 28
l IS, L VEDD and L VESD, l L V wall thinning t L VEF 25•28
No effect on LV hypertrophy and LVEDD, L VESD, L VEF or on p-AMPK 31
t Cardiac hypertrophy 45-47 t phospho-p70S6 kinase levels 45. 47
t L V collagen formation 46, 47
l L V systolic function 47 t progressive L V dilation 47
No effect on infarct size 46
l infarct volume and thickness of the non-infarcted ventricular septum 44
No effect on infarct size 74, 75 t L VEDP and LV dP/dt(max) and dP/dt(min) 74• 77
l myocyte hypertrophy 74 t myocyte hypertrophy 79 l interstitial fibrosis 74, 77
l TNF- a , TGF- f3 I , MCP-1 74 No effect on L V remodeling 750 76
ANP, atrial natriuretic peptide; BNP, brain natriuretic peptide; LVEF, left ventricular ejection fraction; LVESP, left ventricular end-systolic pressure; LVEDP, left ventricular end-diastolic pressure; dP/dtmax and dP/dtmin, the maximal rate of increase and decrease of left ventricular pressure, respectively; L VEDD and L VESD, left ventricular end diastolic and systolic diameter, respectively; AMPK 5' adenosine monophosphate-activated protein kinase; eNOS, endothelial nitric oxide synthase; PKA, Protein kinase A; p42/44 MAPK, mitogen-activated protein kinase p42/44; TGF-�l , transforming growth factor -� 1 ; MCP- 1 , Monocyte chemotactic protein- I .
ml
0 � § :::t. e, "' 0-� c'i'
� 5· "C 0 �
ii 3 8. !!. 5·
(IQ

l.;.) 00
Table 2 Effects of new antidiabetic agents in non-diabetic post-MI animal models.
New antidiabetic agents
Incretin peptides (GLP-1,Exenatide, liraglutide)
DPP-4 inhibitor
(Vildagliptin,
sitagliptin, saxagliptin)
Acute studies
I Infarct size 91-95, 101 , 102
No effect on infarct size 98
f left ventricular developed pressure 95•97, 99
I coronary flow 97
I L V wall thinning and myocardial stiffness 101
t Cardiac output 99 t LVEF 1 02
I myocardial glucose uptake 96, 9' t cAMP and cGMP release 91
t survival 99 t Akt, GSK3 J3 , PPAR- J3 or PPAR- 6 , Nrf-2, and HO- I 99 ' apoptosis 10 1 . 1 02
+ Infarct size 66• 107
t RISK pathway 107
No effect on infarct size 108
I mortality 108
t HO-I , ANP, and pGSK-3 J3 proteins 108
Chronic studies
I myocyte apoptosis 103
j LVEDD !OS
t LV function 103• 1 04
t LVEF 1 04
t myocardial glucose uptake ios
t survival 103
t L V dP/dt stroke volume and cardiac output !OS
No beneficial effects ofDPP-4 inhibition on long-term remodeling 109
LVEF, left ventricular ejection fraction; LVEDD, left ventricular end diastolic diameter; ANP, atrial natriuretic peptide; GSK3P, Glycogen synthase
kinase 3 p; PPAR-P or PPAR-o, peroxisome proliferator-activated receptor beta or delta; Nrf-2, Nuclear factor (erythroid-derived 2)-like 2; HO- I , Heme oxygenase- 1 .
n ::r ""' "'C
N

v.) '-0
Table 3 Clinical data on ischemic events with antidiabetic agents
Classic antidiabetic agents
Biguanides Metformin
Sulfonylureas (Glibenclamide, gliclazide)
Thiazolidinediones (TZD): (pioglitazone, rosiglitazone)
Main findings in clinical studies
Reduction microvascular complications uo Decrease cardiovascular events 15
Reduce morbidity in patients with heart failure 1 1 1
Lesser cardiovascular hospitalization and all cause mortality 1 1 2
UGDP- increase detrimental cardiovascular effects in patients 1 13
UKPDS- no higher risk of myocardial infarction 1 10
Sulfonylureas monotherapy had lower mortality than combination therapy 9
Reduction in incidence of cardiovascular complications in patient 52
Increase in the incidence of myocardial infarction and heart failure 1 14-1 1 6
Increased risk of hospital admission for heart failure but was associated with reduced all cause mortality 12
RECORD-no increased all-cause mortality but increase heart failure 1 18
PERISCOPE- decreased rate of progression of coronary atherosclerosis 1 19
UGDP, University Group Diabetes Program; UKPDS, United Kingdom Prospective Diabetes Study; RECORD, trial of Rosiglitazone Evaluated for Cardiac Outcomes and Regulation of glycemic in Diabetes; PERISCOPE, trial of Pioglitazone Effect on Regression of Intravascular Sonographic Coronary Obstruction Prospective Evaluation.
ml
0: ;· ;:;·
2 q;i s·
!a � @ 3 8. !!. s·
Chapter 2
References
I . Boudina S , Abel ED. Diabetic cardiomyopathy revisited. Circulation 2007;1 15:32 1 3-3223.
2. Ashrafian 1- 1, Frcnncaux MP, Opie LI I. Metabolic mechanisms in heart failure. Circulation 2007; 1 1 6:434-448.
3 . De Groote P, Lamblin N , Mouquet F , Plichon D, McFadden E , Van Belle E, et al. Impact of diabetes mell itus on long-term survival in patients with congestive heart failure. Eur 1/eart J 2004;25:656-662.
4. Dries DL, Sweitzer NK, Drazner M I-I, Stevenson LW, Gersh BJ. Prognostic impact of diabetes mellitus in patients with heart failure according to the etiology of left ventricular systolic dysfunction. J Am Coll Cardiol 200 I ;38:42 1 -428.
5 . de Boer RA, Doehner W, van der I lorst IC, Anker SD, Babalis D, Roughton M, et al. Influence of diabetes mellitus and hyperglycemia on prognosis in patients > or =70 years old with heart failure and effects of nebivolol (data from the Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors with heart failure [SENIORS]). Am J Cardiol 2010;106:78-86.
6. Kannel WB, l ljortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol 1 974;34:29-34.
7. Amato L, Paolisso G, Cacciatore F, Ferrara N, Ferrara P, Canonico S, et al. Congestive heart failure predicts the development of non-insulin-dependent diabetes mellitus in the elderly. The Osservatorio Geriatrico Regione Campania Group. Diabetes Metab 1 997;23:2 1 3-2 1 8.
8 . Lokc YK, Kwok CS, Singh S . Comparative cardiovascular effects of thiazolidinediones: systematic review and meta-analysis of observational studies. BMJ 201 1 ;342:d 1 309.
9. Fisman EZ, Tenenbaum A. A eardiologic approach to non-insulin antidiabetic pharmacotherapy in patients with heart disease. Cardiovasc Diabetol 2009;8:38.
I 0. Ryden L, Stand! E, Bartnik M, Van den Berghe G, Betteridge J, de Boer MJ, et al. Guidelines on diabetes, pre-diabetes, and cardiovascular diseases: executive summary. The Task Force on Diabetes and Cardiovascular Diseases of the European Society of Cardiology (ESC) and of the European Association for the Study of Diabetes (EASD). Eur Heart J 2007;28:88- 1 36.
1 1 . Bailey CJ, Grant PJ. The UK Prospective Diabetes Study. Lancet 1998;352: 1 932; author reply 1 934.
40

Oral antidiabetic drugs in post-MI remodeling
1 2. Eurich OT, McAlister FA, Blackburn OF, Majumdar SR, Tsuyuki RT, Varney J, el al.
13 .
14.
1 5 .
Benefits and harms of antidiabetic agents i n patients with diabetes and heart failure: systematic review. BMJ 2007;335:497.
Kirpichnikov D, McFarlane SI, Sowers JR. Metforrnin: an update. Ann Intern Med 2002;137:25-33.
Ingram DK, Zhu M, Mamczarz J, Zou S, Lane MA, Roth GS, el al. Calorie restriction R mimetics: an emerging research field. Aging Ce/1 2006;5:91- I 08. a
UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metforrnin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. Lancet I 998;352:854-865.
1 6. Schramm TI<, Gislason GH, Vaag A, Rasmussen JN, Folke F, l lansen ML, et al. Mortality and cardiovascular risk associated with different insulin secretagogues compared with metforrnin in type 2 diabetes, with or without a previous myocardial infarction: a nationwide study. Eur Heart J 201 1 ;32: 1 900- I 908.
1 7. Legtenberg RJ, Houston RJ, Oeseburg B, Smits P. Metforrnin improves cardiac functional recovery after i schemia in rats. /-form Met ab Res 2002;34: 1 82- 1 85.
1 8. Solskov L, Lofgren B, Kristiansen SB, Jessen N, Pold R, Nielsen TT, et al. Metforrnin induces cardioprotection against ischaemia/reperfusion injury in the rat heart 24 hours after administration. Basic Clin Pharmacol Toxicol 2008;103:82-87.
1 9. Xing Y, Musi N, Fujii N, Zou L, Luptak I, l-lirshman MF. et al. Glucose metabolism and energy homeostasis in mouse hearts overexpressing dominant negative alpha2 subunit of AMP-activated protein kinase. J Biol Chem 2003;278:28372-28377.
20. Calvert JW, Gundewar S, Jha S, Greer JJ, Bestermann WI-I, Tian R, et al. Acute metforrnin therapy confers cardioprotection against myocardial infarction via AMPK-eNOS-mediated signaling. Diabetes 2008;57:696-705.
2 1 . Bhamra GS, 1 lausenloy DJ, Davidson SM, Carr RD, Paiva M , Wynne AM, et al. Metforrnin protects the ischemic heart by the Akt-mediated inhibition of mitochondrial permeability transition pore opening. Basic Res Cardiol 2008;1 03:274-284.
22. Paiva M, Riksen NP, Davidson SM, 1-Iausenloy DJ, Monteiro P, Goncalves L, et al. Metforrnin prevents myocardial reperfusion injury by activating the adenosine receptor. J Cardiovasc Pharmacol 2009;53:373-378.
23. Paiva MA, Goncalves LM, Providencia LA, Davidson SM, Yellon OM, Mocanu MM. Transitory activation of AMPK at reperfusion protects the ischaemic-reperfused rat myocardium against infarction. Cardiovasc Drugs Ther 20 I 0;24:25-32.
4 1

Chapter 2
24. Kravchuk E, Grineva E, Bairamov A, Galagudza M, Vlasov T. The Effect of Metfonnin on the Myocardial Tolerance to lschemia-Repcrfusion Injury in the Rat Model of Diabetes Mcllitus Type I I. Exp Diabetes Res 201 1 ;201 1 :907496.
25. Gundewar S, Calvert JW, Jha S, Toedt-Pingel I, Ji SY, Nunez D, et al. Activation of AMPactivated protein kinase by metfonnin improves left ventricular function and survival in heart failure. Circ Res 2009;1 04:403-4 1 I .
26. Yin M, van der I lorst IC, van Melle JP, Qian C, van Gilst WI I, Silljc 1 1 1 I, et al. Metfonnin improves cardiac function in a non-diabetic rat model of post-Ml heart failure. Am J Physiol I /earl Circ Physiol 20 1 1 ; 30 I : 1 1459-68.
27. Wang XF, Zhang JY, Li L, Zhao XY, Tao I IL, Zhang L. Mctfonnin improves cardiac function in rats via activation of AMP-activated protein kinase. Clin Exp Pharmacol Physiol 201 1 ;38:94- 1 0 1 .
28. Sasaki 1 1, Asanuma 1 1, Fujita M, Takahama 1 1, Wakeno M, Ito S, et al. Metfonnin prevents pro!:,'fcssion of heart failure in dogs: role of AMP-activated protein kinase. Circulation 2009; 1 19:2568-2577.
29. Xiao 1 1, Ma X, Feng W, Fu Y, Lu Z, Xu M, et al. Mctfonnin attenuates cardiac fibrosis by inhibiting the TGFbeta I -Smad3 signalling pathway. Cardiovasc Res 20 I 0;87:504-5 1 3 .
30. Xie Z, He C, Zou Ml I. AMP-activated protein kinase modulates cardiac autophagy in diabetic cardiomyopathy. Autophagy 201 1 ;7.
3 1 . Benes J, Kazdova L, Drahota Z, 1 loustek J, Medrikova D, Kopecky J, et al. Effect of mctfonnin therapy on cardiac function and survival in a volume-overload model of heart failure in rats. Clin Sci (Lond) 201 1 ;121 :29-4 1 .
32 . Facundo I IT, Jones SP. AMP-dependent protein kinase activators: not just for diabetes? Circ Res 2009;104:282-284.
33. Rosenstock J, Samols E, Muchmore DB, Schneider J. Glimepiride, a new once-daily sulfonylurea. A double-blind placebo-control led study of NIDDM patients. Glimepiride Study Group. Diabetes Care 1 996; 1 9: 1 1 94- 1 1 99.
34. l l iraoka M, Furukawa T. Functional Modulation of Cardiac ATP-Sensitive K( ) Channels. News Physiol Sci 1 998;13: 1 3 1 - 1 37.
35. Brady PA, Terzic A. The sulfonylurea controversy: more questions from the heart. J Am Coll Cardiol 1 998;31 :950-956.
36. Miura T, M iki T. ATP-sensitive K+ channel openers: old drugs with new clinical benefits for the heart. Curr Vase Pharmacol 2003;1 :25 1 -258.
42

Oral antidiabetic drugs in post-Ml remodeling
37. Duncker DJ, Van Zon NS, Altman JD, Pavek TJ, Bache R.1. Role of K+ATP channels in coronary vasodilation during exercise. Circulation 1 993;88: 1 245-1 253.
38. Quast U, Stephan D, Bieger S, Russ U. The impact of ATP-sensitive K+ channel subtype selectivity of insulin secretagogues for the coronary vasculature and the myocardium. Diabetes 2004;53 Suppl 3:S 1 56-64.
39. Docherty JC, Gunter HE, Kuzio 8, Shoemaker L, Yang L, Deslauriers R. Effects of cromakalim and glibenclamide on myocardial high energy phosphates and intracellular pH during ischemia-reperfusion: 3 1 P NMR studies. J Mo/ Cell Cardiol 1 997;29: 1 665-1 673.
40. Kashimoto S, Furuya A, Kume M, Yamaguchi T, Kurnazawa T. Effects of glibenclamide on hydroxyl radical formation in the postischaemic reperfused heart with or without inhalation anaesthetics. Eur J Anaesthesiol 2001 ;18:8 1 1 -8 1 5.
4 1 . Legtenberg R.I, Houston R.I, l leerschap A, Oeseburg 8, Smits P. Glibenclamide attenuates ischemia-induced acidosis and loss of cardiac function in rats. Eur J Pharmacol 2002;434:35-42.
42. Maruyama I, Tomiyama Y, Maruyama K, Ojima K, Kobayashi K, Kobayashi M, et al. Effects of mitiglinide and sulfonylureas in isolated canine coronary arteries and perfused rat hearts. Eur J Pharmacol 2006;531 : 1 94-200.
43. Namekata I, Yamaguchi Y, Moriguchi S, Yamazaki S, Terasawa A, Yamagishi R, et al. (R)-ACX, a pancreatic beta-cell selective sulfonylurea, does not aggravate myocardial ischemia-reperfusion damage. Eur J Pharmacol 2007;577:2 1 1 -2 1 8.
44. EI-Reyani NE, 8aczko I, Lepran 1, Papp JG. Effect of glibenclamide and glimepiride treatment on the development of myocardial infarction in rats. Acta Physiol Hung 2000;87: 1 73- 1 84.
45. Lee TM, Lin MS, Tsai CH, Chang NC. Effects of pravastatin on ventricular remodeling by activation of myocardial KA TP channels in infarcted rats: role of 70-kDa S6 kinase. Basic Res Cardio/ 2007;102 : 1 7 1 - 1 82.
46. Lee TM, Lin MS, Chang NC. Effect of pravastatin on sympathetic reinnervation in postinfarcted rats. Am J Physiol Heart Circ Physio/ 2007;293:1-1361 7-26.
47. Lee TM, Lin MS, Chang NC. Effect of ATP-sensitive potassium channel agonists on ventricular remodeling in healed rat infarcts. J Am Coll Cardiol 2008;51 : 1 309- 1 3 1 8.
48. Schoonjans K, Auwerx J. Thiazolidincdiones: an update. lancet 2000;355: 1 008- 1 0 1 0.
49. Olefsky JM. Treatment of insulin resistance with peroxisome proliferator-activated receptor gamma agonists. J Clin Invest 2000;106:467-472.
43
I

Chapter 2
50. Braissant 0, Foufelle F, Scotto C, Dauca M, Wahli W. Differential expression of peroxisome proliferator-activated receptors (PPARs): tissue distribution of PPAR-alpha, -beta, and -gamma in the adult rat. Endocrinology I 996;137:354-366.
5 1 . Petrazzi L, Grassi D, Polidoro L, D'Aurelio A, Croce G, Properzi G, et al. Cardiovascular risk and cardiometabolic protection: role of glitazones. J Nephrol 2008;21 :826-835.
52. Krentz AJ, Bailey CJ. Oral antidiabetic agents: current role in type 2 diabetes mellitus. Drugs 2005;65:385-41 1 .
53. Yki-Jarvinen I I . Thiazolidinediones. N Eng/ J Med 2004;351 : 1 1 06-I I 1 8.
54. Shah P, Mudaliar S. Pioglitazone: side effect and safety profile. Expert Opin Drug Saf 20 1 0;9:347-354.
55. Yue Tl TL, Chen J, Bao W, Narayanan PK, Bril A, Jiang W, et al. In vivo myocardial protection from ischemia/reperfusion injury by the peroxisome proliferator-activated receptor-gamma agonist rosiglitazone. Circulation 2001 ;1 04:2588-2594.
56. Ito 1 1 , Nakano A, Kinoshita M, Matsumori A. Pioglitazone, a peroxisome proliferatoractivated receptor-gamma agonist, attenuates myocardial ischemia/reperfusion injury in a rat model. lab Invest 2003;83: 1 7 1 5- 1 72 1 .
57. Wayman NS, Hattori Y, McDonald MC, Mota-Filipc I I, Cuzzocrea S, Pisano B, et al. Ligands of the peroxisome proliferator-activated receptors (PP AR-gamma and PP AR-alpha) reduce myocardial infarct size. FASEB J 2002; 16 : I 027- 1 040.
58. Lee TM, Chou TF. Troglitazone administration limits infarct size by reduced phosphorylation of canine myocardial conncxin43 proteins. Am J Physiol I/earl Circ Physiol 2003;285:1 1 1 650-9.
59. Wynne AM, Mocanu MM, Yellon DM. Pioglitazone mimics preconditioning in the isolated perfused rat heart: a role for the prosurvival kinases Pl3K and P42/44MAPK. J Cardiovasc Pharmacol 2005;46:8 1 7-822.
60. Molavi B, Chen J, Mehta JL. Cardioprotective effects of rosiglitazone are associated with selective overexpression of type 2 angiotensin receptors and inhibition of p42/44 MAPK. Am J Physiol / fear/ Circ Physiol 2006;291 :1 1687-93.
6 1 . Cao Z, Ye P, Long C, Chen K, Li X, Wang I I. Effect of pioglitazone, a peroxisomc proliferator-activated receptor gamma agonist, on ischemia-reperfusion injury in rats. Pharmacology 2007 ;79: 1 84- 1 92.
44

Oral antidiabetic drugs in post-MI remodeling
62. Ye Y, Lin Y, Atar S, Huang MH, Perez-Polo JR, Uretsky BF, et al. Myocardial protection by pioglitazone, atorvastatin, and their combination: mechanisms and possible interactions. Am J Physiol Heart Circ Physiol 2006;291 :I 1 1 1 58-69.
63. Ye Y, Lin Y, Manickavasagam S, Perez-Polo JR, Tieu BC, Birnbaum Y. Pioglitazone protects the myocardium against ischemia-reperfusion injury in eNOS and iNOS knockout mice. Am J Physiol Heart Circ Physiol 2008;295:1-12436-46.
64. Ye Y, Keyes KT, Zhang CF, Perez-Polo JR, Lin Y, Birnbaum Y. Additive effect of TAK-49 1 , a new angiotensin receptor blocker, and pioglitazone, in reducing myocardial infarct size. Cardiovasc Drugs Ther 20 I 0;24: I 07- 1 20.
65. Ye Y, Keyes KT, Zhang C, Perez-Polo JR, Lin Y, Birnbaum Y. The myocardial infarct sizelimiting effect of sitagliptin is PKA-dependent, whereas the protective effect of pioglitazone is partially dependent on PKA. Am J Physiol Heart Circ Physiol 201 0;298:H 1 454-65.
66. Li J, Lang MJ, Mao XB, Tian L, Feng YB. Antiapoptosis and mitochondrial effect of pioglitazone preconditioning in the ischemic/reperfused heart of rat. Cardiovasc Drugs Ther 2008;22:283-29 1 .
67. Ye Y, Lin Y, Perez-Polo JR, Birnbaum Y. Oral glyburide, but not glimepiride, blocks the infarct-size limiting effects of pioglitazone. Cardiovasc Drugs Ther 2008;22:429-436.
68. Yasuda S, Kobayashi H, Iwasa M, Kawamura I, Sumi S, Narentuoya B, et al. Antidiabetic drug pioglitazone protects the heart via activation of PPAR-gamma receptors, PB-kinase, Akt, and eNOS pathway in a rabbit model of myocardial infarction. Am J Physiol Heart Circ Physiol 2009;296:1 1 1 558-65.
69. Zhang XJ, Xiong ZB, Tang AL, Ma H, Ma YD, Wu JG, et al. Rosiglitazone-induced myocardial protection against ischaemia-reperfusion injury is mediated via a phosphatidylinositol 3-kinase/Akt-dependent pathway. Clin Exp Pharmacol Physiol 20 1 0;37: 1 56- 1 6 1 .
70. Birnbaum Y, Long B, Qian J, Perez-Polo JR, Ye Y. Pioglitazone limits myocardial infarct size, activates Akt, and upregulates cPLA2 and COX-2 in a PPAR-gamma-independent manner. Basic Res Cardiol 20 1 1 ;106:43 1 -446.
7 1 . Abe M , Takiguchi Y, lchimaru S, Kaj i S, Tsuchiya K, Wada K. Different effect of acute treatment with rosiglitazone on rat myocardial ischemia/reperfusion injury by administration method. Eur J Pharmacol 2008;589:2 1 5-2 19 .
72. Yue TL, Bao W, Gu JL, Cui J, Tao L, Ma XL, et al. Rosiglitazone treatment in Zucker diabetic Fatty rats is associated with ameliorated cardiac insulin resistance and protection from ischemia/reperfusion-induced myocardial injury. Diabetes 2005;54:554-562.
45

Chapter 2
73. Shiomi T, Tsutsui 1 1, 1 layashidani S, Sucmatsu N, lkeuchi M, Wen J, et al. Pioglitazone, a pcroxisome proliferator-activated receptor-gamma agonist, attenuates left ventricular remodeling and failure after experimental myocardial infarction. Circulation 2002; I 06:3 1 26-3 1 32.
74. Lygate CA, Hulbert K, Monfared M, Cole MA, Clarke I<, Neubauer S. The PPARgammaactivator rosiglitazone does not alter remodeling but increases mortality in rats postmyocardial infarction. Cardiovasc Res 2003;58:632-637.
75. Frantz S, l lu I<, Widder J, Bayer B, Witzel CC, Schmidt I, et al. Peroxisomc proliferator activated-receptor agonism and left ventricular remodeling in mice with chronic myocardial infarction. Br J Pharmacol 2004;141 :9- 14.
76. Geng DF, Wu W, Jin DM, Wang JF, Wu YM. Effect of peroxisome proliferator-activatcd receptor gamma ligand. Rosiglitazone on left ventricular remodeling in rats with myocardial infarction. Int J Cardiol 2006;1 13:86-9 1 .
77. Linz W, Wohlfart P, Baader M, Breitschopf K, Falk E, Schafer I -IL, et al. The peroxisome proliferator-activatcd receptor-alpha (PP AR-alpha) agonist, A VE8 1 34, attenuates the progression of heart failure and increases survival in rats. Acta Pharmacol Sin 2009;30:935-946.
78. Weiss CS, Hagenmuller M, Pichler M, Munz S, Ochs M, Buss SJ, et al. Activation of PPARgamma by pioglitazone does not attenuate left ventricular hypertrophy following aortic banding in rats. Naunyn Schmiedebergs Arch Pharmacol 20 1 0;381 :285-295.
79. Todd JF, Wilding JP, Edwards CM, Khan FA, Ghatei MA, Bloom SR. Glucagon-like peptide-I (GLP-1 ): a trial of treatment in non-insulin-dependent diabetes mellitus. Eur J Clin Invest I 997;27:533-536.
80. Zander M, Madsbad S, Madsen JL, I lolst JJ. Effect of 6-week course of glucagon-likc peptide I on glycacmic control, insulin sensitivity, and beta-cell function in type 2 diabetes: a parallel-group study. lancet 2002;359:824-830.
8 1 . Drucker DJ, Nauck MA. The incretin system: glucagon-like peptide- I receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. lancet 2006;368: 1 696- 1 705 .
82. Bergman AJ, Stevens C, Zhou Y, Yi B, Lacthcm M, De Smet M, et al. Pharmacokinetic and pharmacodynamic properties of multiple oral doses of sitagliptin, a dipeptidyl peptidase-IV inhibitor: a double-blind, randomized, placebo-controlled study in healthy male volunteers. Clin Ther 2006;28:55-72.
83. Neumiller JJ, Campbell RK. Saxagliptin: a dipeptidyl pcptidase-4 inhibitor for the treatment of type 2 diabetes mellitus. Am J Health Syst Pharm 20 10;67: 1 5 1 5- 1 525.
46
Oral antidiabetic drugs in post-MI remodeling
84. Verspohl EJ. Novel therapeutics for type 2 diabetes: incretin hormone mimetics (glucagonlike peptide- I receptor agonists) and dipeptidyl peptidase-4 inhibitors. Pharmacol Ther 2009;124: 1 1 3- 1 38.
85. Oeseburg I I, de Boer RA, Buikema H, van der l-larst P, van Gilst WH, Sillje H I-I. Glucagonlike peptide I prevents reactive oxygen species-induced endothelial cell senescence through the activation of protein kinase A. Arterioscler Thromb V asc Biol 20 I 0;30: 1 407- 14 14.
86. Gros R, You X, Baggio LL, Kabir MG, Sadi AM, Mungrue IN, et al. Cardiac function in mice lacking the glucagon-like peptide- I receptor. Endocrinology 2003;144:2242-2252.
87. Nikolaidis LA, Mankad S, Sokos GG, Miske G, Shah A, Elahi D, et al. Effects of glucagonlike peptide- I in patients with acute myocardial infarction and left ventricular dysfunction after successful reperfusion. CirC11lation 2004;1 09:962-965.
88. Sokos GG, Nikolaidis LA, Mankad S, Elahi D, Shannon RP. Glucagon-like peptide-I infusion improves left ventricular ejection fraction and functional status in patients with chronic heart failure. J Card Fail 2006;12:694-699.
89. Ussher JR , Drucker DJ. Cardiovascular Biology of the Incretin System. Endocr Rev 201 2;.
90. Bose AK, Mocanu MM, Carr RD, Brand CL, Yellon DM. Glucagon-like peptide I can directly protect the heart against ischemia/reperfusion injury. Diabetes 2005;54: 146- 1 5 1 .
9 1 . Bose AK, Mocanu M M, Carr RD, Yellon DM. Myocardial ischaemia-reperfusion injury is attenuated by intact glucagon like peptide-I {GLP- 1 ) in the in vitro rat heart and may involve the p70s6K pathway. Cardiovasc Dnigs Ther 2007;21 :253-256.
92. Bose AK, Mocanu MM, Carr RD, Yellon DM. Glucagon like peptide- I is protective against myocardial ischemia/reperfusion injury when given either as a preconditioning mimetic or at reperfusion in an isolated rat heart model. Cardiovasc D111gs Ther 2005;19:9- l l .
93. Sonne DP, Engstrom T, Treiman M. Protective effects of GLP- 1 analogues exendin-4 and GLP- 1 (9-36) amide against ischemia-reperfusion injury in rat heart. Regul Pepi 2008;146:243-249.
94. Ossum A, van Deurs U, Engstrom T, Jensen JS, Treiman M. The cardioprotective and inotropic components of the postconditioning effects of GLP- 1 and GLP- 1 (9-36)a in an isolated rat heart. Pharmacol Res 2009;60:4 1 1 -4 1 7.
95. Zhao T, Parikh P, Bhashyam S, Bolukoglu H, Poomima I, Shen YT, et al. Direct effects of glucagon-like peptide- I on myocardial contracti lity and glucose uptake in normal and postischemic isolated rat hearts. J Pharmacol Exp Ther 2006;317: 1 1 06- 1 1 1 3.
47
Chapter 2
96. Ban K, Noyan-Ashraf Ml I, 1 locfer J, Bolz SS, Drucker DJ, I lusain M. Cardioprotective and vasodilatory actions of glucagon-like peptide I receptor arc mediated through both glucagon-likc peptide I receptor-dependent and -independent pathways. Circulation 2008;1 17:2340-2350.
97. Kristensen J, Mortensen UM, Schmidt M, Nielsen Pl I, Nielsen TI, Maeng M. Lack of cardioprotection from subcutaneously and preischemic administered liraglutide in a closed chest porcine ischemia rcperfusion model. BMC Cardiova5c Disord 2009;9:3 I .
98. Noyan-Ashraf MI i, Momen MA, Ban K, Sadi AM, Zhou YQ, Riazi AM, et al. GLP- 1 R agonist l iraglutide activates cytoprotective pathways and improves outcomes after experimental myocardial infarction in mice. Diabetes 2009;58:975-983.
99. Brown SB, Libonati JR, Selak MA, Shannon RP, Simmons RA. Neonatal cxcndin-4 leads to protection from rcpcrfusion injury and reduced rates of oxidative phosphorylation in the adult rat heart. Cardiovasc Drugs Ther 20 I 0;24: 1 97-205.
1 00. Timmers L, Henriques JP, de Kleijn DP, Devries JI I, Kemperman 1- 1, Steendijk P, et al. Excnatide reduces infarct size and improves cardiac function in a porcine model of ischemia and reperfusion injury. J Am Coll Cardiol 2009;53:50 1 -5 I O.
I 0 1 . Matsubara M, Kanemoto S, Leshnower BG, Albone EF, l l inmon R, Plappert T, et al. Single dose GLP-1 -Tf ameliorates myocardial ischemia/rcperfusion injury. J Surg Res 20 1 1 ;165:38-45.
I 02. Poomima I, Brown SB, Bhashyam S, Parikh P, Bolukoglu 1 1, Shannon RP. Chronic glucagon-like peptide- I infusion sustains left ventricular systolic function and prolongs survival in the spontaneously hypertensive, heart fai lure-prone rat. Circ Heart Fail 2008; 1 : 1 53- 1 60.
1 03 . Liu Q, Anderson C, Broyde A, Polizzi C, Fernandez R, Baron A, et al. Glucagon-like peptide- I and the exenatide analogue AC3 I 74 improve cardiac function, cardiac remodeling, and survival in rats with chronic heart failure. Cardiovasc Diabetol 20 I 0;9:76.
1 04. Nikolaidis LA, Elahi D, l lentosz T, Doverspike A, l luerbin R, Zourelias L, et al. Recombinant glucagon-l ike peptide- I increases myocardial glucose uptake and improves left ventricular performance in conscious dogs with pacing-induced dilated cardiomyopathy. Circulation 2004;1 10:955-96 1 .
1 05. Barakat GM, Nuwayri-Salti N, Kadi LN, Bitar KM, AI-Jaroudi WA, Bikhazi AB. Role of glucagon-like peptide-I and its agonists on early prevention of cardiac remodeling in type I diabetic rat hearts. Gen Physiol Biophys 201 1 ;30:34-44.
I 06. 1- luisamen B, Genis A, Marais E, Lochner A. Pre-treatment with a DPP-4 inhibitor is infarct sparing in hearts from obese, pre-diabetic rats. Cardiovasc Drugs Ther 20 1 1 ;25: 1 3-20.
48

Oral antidiabetic drugs in post-MI remodeling
1 07. Sauve M, Ban K, Momen MA, Zhou YQ, Henkelman RM, Husain M, et al. Genetic deletion or pharmacological inhibition of dipeptidyl peptidase-4 improves cardiovascular outcomes after myocardial infarction in mice. Diabetes 20 I 0;59: I 063- 1 073.
1 08. Yin M, Sillje HH, Meissner M, van Gilst WH, de Boer RA. Early and late effects of the DPP-4 inhibitor vildagliptin in a rat model of post-myocardial infarction heart failure. Cardiovasc Diabetol 20 1 1 ;1 0:85.
1 09. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. lancet 1 998;352:837-853.
I I O. Eurich DT, Majumdar SR, McAlister FA, Tsuyuki RT, Johnson JA. Improved clinical outcomes associated with metforrnin in patients with diabetes and heart failure. Diabetes Care 2005;28:2345-235 1 .
1 1 1 . Johnson JA, Simpson SI-I, Toth EL, Majumdar SR. Reduced cardiovascular morbidity and mortality associated with metforrnin use in subjects with Type 2 diabetes. Diabet Med 2005;22:497-502.
1 1 2. Seltzer I-IS. A summary of criticisms of the findings and conclusions of the University Group Diabetes Program (UGDP). Diabetes 1 972;21 :976-979.
I 1 3 . Nissen SE , Wolski K. Effect of rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. N Engl J Med 2007;356:2457-247 1 .
1 1 4. Singh S, Loke YK, Furberg CD. Long-term risk of cardiovascular events with rosiglitazone: a meta-analysis. JAMA 2007;298: 1 1 89-1 1 95.
1 1 5. Erdmann E, Charbonnel B, Wilcox RG, Skene AM, Massi-Benedetti M, Yates J, et al. Pioglitazone use and heart failure in patients with type 2 diabetes and preexisting cardiovascular disease: data from the PROactive study (PROactive 08). Diabetes Care 2007 ;30:2773-2778.
1 1 6. Home PD, Pocock SJ, Beck-Nielsen 1-1, Gomis R, I lanefeld M, Jones NP, et al. Rosiglitazone evaluated for cardiovascular outcomes-an interim analysis. N Engl J Med 2007;357:28-38.
1 1 7. Home PD, Pocock SJ, Beck-Nielsen H, Curtis PS, Gomis R, 1-Ianefeld M, et al. Rosiglitazone evaluated for cardiovascular outcomes in oral agent combination therapy for type 2 diabetes (RECORD): a multicentre, randomised, open-label trial. lancet 2009;373:2 125-2 1 35.
49
II

Chapter 2
1 1 8. Nissen SE, Nicholls SJ, Wolski K, Nesto R, Kupfer S, Perez A, et al. Comparison of pioglitazone vs glimepiride on progression of coronary atherosclerosis in patients with type 2 diabetes: the PERISCOPE randomized controlled trial. JAMA 2008;299: 1 56 1 - 1 573.
50

Chapter 3
Metf or min improves cardiac function in a
non-diabetic rat model of post-MI heart failure
Meimei Yin, /wan C. C. van der Horst, Joos/ P. van Melle, Cheng Qian, Wiek H. van
Gilst, Herman H. W. Sillje, Rudolf A. de Boer
University Medical Center Groningen, Thorax Center, Department of Cardiology,
University of Groningen, Hanzeplein 1 , 971 3 GZ, The Netherlands
Am J Physiol Heart Circ Physiol. 201 1 Aug;301(2):H459-68. Epub 2011 May 13.
Chapter 3
Abstract
Metformin is the first choice drug for the treatment of patients with diabetes, but its use is debated in patients with advanced cardiorenal disease. Epidemiological data suggest that metformin may reduce cardiac events, both in patients with and without heart failure. Experimental evidence suggests that metformin reduces cardiac ischemia/reperfusion injury. It is unknown whether metformin improves cardiac function (remodeling) in a long-term post-Ml remodeling model. We therefore studied male, non-diabetic, Sprague-Dawley rats that were either subjected to myocardial infarction (Ml) or sham operation. Animals were randomly allocated to treatment with normal water or metformin containing water (250mg/kg/day). At baseline, 6 weeks and 1 2 weeks, metabolic parameters were analyzed and oral glucose tolerance tests (OGIT) were performed. Echocardiography and hemodynamic parameters were assessed twelve weeks after Ml. In the MI model, infarct size was significantly smaller after 1 2 weeks metformin treatment (29.6_t3.2 % vs. 38.0±2.2%, p<0.05). Moreover, metformin resulted in less left ventricular dilatation (LVIDs: 6.0±0.4 vs. 7.6±0.6 mm, p<0.05) and preservation of left ventricular ejection fraction (65.8±3.7 % vs. 48.6±5.6 %, p<0.05) as compared to MI control. The improved cardiac function was associated with decreased ANP (Atrial Natriuretic Peptide) mRNA levels in the metformin-treated group (50% fold reduction compared to Ml, p<0.05). Insulin resistance did not occur during cardiac remodeling (as indicated by normal OGTT) and fasting glucose levels and the pattern of the OGTT were not affected by metformin. Molecular analyses suggested that altered AMPK phosphorylation status and low insulin levels mediate the salutary effects of metformin. Altogether our results indicate that metformin may have potential to attenuate heart failure development after myocardial infarction, in the absence of diabetes and independent of systemic glucose levels.
Key words: Metformin, myocardial infarction, remodeling, heart failure, left ventricular function, diabetes.
52

Metformin in post-MI heart failure
Introduction
The prevalence of patients with diabetes and heart failure (HF) is growing exponentially. Compared to HF patients without diabetes, diabetic HF patients have a poor prognosis and quality of life 1 ' 2• Moreover, diabetes is an established risk factor for incident episodes of HF 3. According to the HF guidelines metformin should be considered as a first-line agent in overweight HF patients with type 2 diabetes without significant renal dysfunction 4
• This recommendation is based on clinical studies showing that metformin seems the only anti-diabetic agent without a harmful cardiac effect in diabetic HF patients 5•
Metforrnin decreases blood glucose by enhancing insulin sensitivity, inducing greater peripheral uptake of glucose, and decreasing hepatic glucose output while lowering plasma insulin concentrations 6
' 7• The cardioprotective effects of metforrnin
can, however, not be attributed to the glucose lowering effects alone 8• Recent
experimental studies suggested ancillary potential mechanisms. More specifically, the protective effects may be conferred via the AMP-activated protein kinase (AMPK) pathway 8-1 3, which is activated by metforrnin. Especially, in ischernia/reperfusion (I/R) models, metformin was shown to decrease the cardiomyocyte apoptosis 1 1 • 14, to improve endothelial function by increasing NO production 8• 1 1 • 1 5
, to maintain myocardial energy production during ischernia 16, and to affect lipid metabolism 1 7- 19
•
Clinical studies show that metforrnin may reduce plasma dipeptidyl peptidase-4 (DPP-4) activity and increase circulating levels of glucagon-like peptide I (GLP-1) which is an incretin hormone that has protective effects on the heart and the vasculature 20-22. Experimental studies employing a pressure-overload model in mice an_d a pacing-model in dogs showed that metformin attenuates cardiac fibrosis by inhibiting collagen synthesis 1 1 ' 13 •
These experimental studies strongly suggest that metforrnin reduces I/R injury. However, little evidence is available to support the use of metformin in chronic cardiac remodeling, e.g. after MI and in HF.
To further investigate the role of metforrnin in HF we conducted a long term study to determine the effects of metforrnin on cardiac function and metabolic parameters in a post-MI rat model.
Methods
Design of the Study Sprague Dawley rats (weight 250-260g, Harlan, The Netherlands) were randomly allocated to left coronary artery ligation (myocardial infarction, MI) or sham surgery.
53
IJ

Chapter 3
The sham procedure was identical to the Ml group except that the ligation was not tied 23. Two days before surgery, rats were fed metformin containing water (250mg/kg/day) or normal water, and this was continued for a period of 1 2 weeks, rendering four experimental groups: sham (N-7), sham+metformin (N=7), Ml (N=8), and MI+metformin (N=9). The animals were further fed ad-libitum with a standard rat diet, and housed in groups of 4-5 rats under a 1 2-hour light: dark cycle. All animals received standard care and the experimental protocol was reviewed and approved by the local Animal Ethical Committee of the University Medical Centre Groningen. At baseline, week 6 and week 12, an oral glucose tolerance test (OGTT) was performed. At week 12, cardiac function was determined by echocardiography. After 1 2 weeks the rats were sacrificed after measuring invasive hemodynamic parameters, and the hearts were rapidly excised, weighed, and prepared for histochemistry and molecular analysis.
Oral glucose tolerance test An OGTT was performed in non-anesthetized rats. After 1 6-hour fasting, glucose (2 g/kg as a 50% solution) was given orally to the animal. Blood was obtained from the tail to measure glucose levels at several time points: 0, 5, 15, 30, 60, and 120 minutes after the glucose administration. Glucose levels were measured with a blood glucose monitor (Accu-Check®, Roche, Germany).
Echocardiographic measurement Echocardiographic measurements were performed by an individual blinded researcher to the treatment groups. Rats were anaesthetized with 2.5 % isoflurane in a gas mixture of N20/02. The M-mode and 20 echocardiography images were obtained with a high-resolution system (Vivid 7, GE, Healthcare, and Chalfont St Giles, UK), using a 1 0 MHz transducer. Diastolic and systolic measurements of LV dimensions (LVIDd, LVIDs), as well as measurements of the thickness of the interventricular septum (IVSs, IVSd) and posterior wall (LVPWs, LVPWd) were recorded. LV fractional shortening (FS %) was calculated as FS= (LVIDd-LVIDs)/LVIDdx l 00¾. LY ejection fraction (EF %) was calculated using the Teichholz method of estimated LV volumes 24.
Haemodynamic measurement Before sacrifice, rats were anesthetized and invasive hemodynamics were measured as described 25
• Briefly, a microtip catheter with pressure transducer (2 Fr, Millar Instr. Inc, Houston, TX, USA) was inserted into the right carotid artery and advanced into the left ventricular cavity. After 5 minutes stabilization, the heart rate (HR), left ventricular end-systolic pressure (LVESP), end-diastolic pressures (LVEDP) and developed left ventricular pressure (dLVP-LVESP-LVEDP) were recorded. The parameters of the
54

Metformin in post-MI heart failure
maximal rates of increase and decrease in developed LV pressures (dP/dtmax and dP/dtmin) were determined.
Procurement of heart tissue for infarct size, cardiomyocyte size and interstitial fibrosis measurement After sacrifice, hearts were rapidly excised and arrested in diastole in 2 M ice-cold KCI. The right ventricle and atria were removed. The basal and apical parts of the LV were snap-frozen in liquid nitrogen. A mid-papillary slice of the LV was fixed in 4% paraformaldehyde overnight and paraffin-embedded. The deparaffinized 3 µm sections were stained with picrosirius red/fast green, as described 26
. The infarct size was calculated as percentage of the scar length to the total LV circumference. The images were obtained with a Leica microscope and analyzed using appropriate software (Image-pro plus, version 4.5.0.29).
Furthermore, sections were stained with a Gomori's silver staining to allow visualization of the cardiomyocytes membranes. We measured cell size from transversally cut cardiomyocytes in the border zone of the infarcted area using image analysis software (Zeiss KS400, Germany). Finally, the collagen volume fraction was examined in sections of the left ventricular free wall, after excluding vessels. Tissue sections were stained with Masson's trichrome stain to evaluate the extent of interstitial fibrosis, modified from previously described methods 25
. The area of stained tissue was calculated as a percentage of the total area within a field by using imagescope software.
Biomolecular assays Arterial blood was collected with EDTA-coated centrifuge tubes. After centrifugation at 3000 rpm for 15 min at 4 °C the plasma was divided into different tubes and snap frozen in liquid nitrogen and stored for future additional analysis. Metformin was measured using high-performance liquid chromatography (HPLC) in the lab of Pharmacy of University Medical Centre Groningen. Insulin levels were measured at 12 weeks after surgery using an ELISA kit (Rat/Mouse insulin 96-well plate assay, Millipore, MA, U.S.A.). The plasma active Glucagon-like peptide ! (GLP-1) and adiponectin levels were measured using the ELISA kits from Linco research and Millipore MA, U.S.A. Myocardial glycogen content was measured using the EnzyChrom™ Glycogen Assay Kit (BioAssay Systems, Hayward, CA, USA), according to manufacturer 's protocol.
Real-time PCR Total RNA from the border zone tissue of infarction was extracted with TRizol reagent (lnvitrogen Corp., Carlsbad, CA, USA) and RNA concentrations were measured with a nano-drop device. First-strand cDNA was prepared using a random primer mix and
55
IJ

Chapter 3
thereafter used as a template for quantitative real-time reverse-transcriptase-PCR
(qRT-PCR) (25 ng/reaction). mRNA levels are expressed in relative units based on a
standard curve obtained by a calibrator cDNA mixture. All measured mRNA
expression levels were corrected for 36B4 reference gene expression. Primer sequences
can be found in Table I .
Table I .Primer sequences used in Real-Time PCR
Gene 5'-3'Forward 5' -3 'Reverse
ANP ATGGGCTCCTTCTCCATCAC TCTACCGGCATCTTCTCCTC
eNOS GACTTTIAAGGAAGTAGCCAATGCA GTGAAGGCGACTATCCTGTATGGCTC
Collagen I ACAGCGTAGCCTACATGG AAGTTCCGGTGTGACTCG
Proco Hagen GAGGGCGAGTGCTGTCCTI GGTCCCTCGACTCCTATGACTTC
36B4 GTTGCCTCAGTGCCTCACTC GCAGCCGCAAATGCAGATGG
ANP: atrial natriuretic peptide; eNOS: Endothelial nitric oxide synthase; Collagen l :col lagen type I ; 36B4: acidic ribosomal phosphoprotein PO.
Western blot analysis Myocardial tissue samples (75 mg), taken from the area-at-risk portion of the LV, were
homogenized in I ml RIPA buffer (50 mM Tris pH 8.0, I % nonidet P40, 0.5%
deoxycholate, 0. 1% SOS, 1 50 mM NaCl) containing phosphatase inhibitor cocktail I
(Sigma), protease inhibitor (ROCHE) and I mM phenylmethylsulfonyl fluoride
(PMSF). Protein concentrations were quantified with the DC protein assay (Bio-Rad
Laboratories, Veenendaal, the Netherlands) with bovine albumin as a standard. Equal
amounts of protein were loaded onto polyacrylamide-SDS gels and after
electrophoreses, proteins were transferred to a PVDF membrane. The membrane was
blocked I h with 5% non-fat milk in PBST and probed with primary antibodies
overnight at 4°C. The following primary antibodies were used: Phospho-AMPKa
Thr l 72 (1 :500, Cell Signaling Technology); AMPKa (1 : 1 000, Cell Signaling
Technology); p-Akt Ser473 ( I : 1 000, Cell Signaling Technology); Akt ( I : 1 000, Cell
Signaling Technology); Phospho-eEF2 Thr56 ( 1 : 1 000, Cell Signaling Technology);
eEF2 ( I : 1 000, Cell Signaling Technology); Phospho-p70S6K Thr389 ( I : 1 000, B&D
systems); p70S6K ( 1 : 1 000, B&D systems); AMPK a l and AMPK a2 1 : 1 000, Cell
Signaling Technology); GLUT4 ( I : 1 000, Cell Signaling Technology); Cleaved
Casepase-3 ( I : 1 000, Cell Signaling Technology); GAP DH (I :20,000, Fitzgerald
56

Metformin in post-MI heart failure
Industries International, Acton, Mass). lmmunoblots were next processed with secondary antibodies for 1 hr at room temperature followed by ECL detection using an ECL+Plus chemiluminescence reagent kit (Amersham).
Statistical Analysis All data are expressed as means ± standard errors of the mean (SEM). Differences among groups were tested by one-way analysis of variance (ANOVA) with a 2-sided Dunnett t-test as post-hoc test, taking the MI group as a comparator. Comparison between groups sham and sham+metformin was tested by independent t tests. P-values <0.05 were considered statistically significant. SPSS (PASW, Chicago, IL, USA) version 1 8.0 was used to perform all statistical analyses.
Results
The effect of metformin on metabolic parameters. To confirm that metformin was consumed by the rats and entered the blood stream, serum metformin levels were measured. In both treatment groups (sham+metformin and MI+metformin), the serum levels of the drug were around 3mg/L, while no metformin could be detected in non-treated groups (Fig. IA, upper panel). As metformin is an oral antihyperglycemic agent, that may lower the blood glucose levels, fasting glucose levels were determined and OGTis were performed. No differences were found in the fasting glucose levels between the groups at baseline, week 6 and 1 2 after surgery (12 weeks results shown in Fig. IA, middle panel). Moreover, no differences could be identified in the OGTis at these intervals (Fig. IB), suggesting that glucose uptake from the plasma was not altered and that long term remodeling after Ml did not generate insulin resistance in these rats. Blood plasma insulin levels were also determined and were significantly decreased in both metformin-treated groups as compared to non-treated groups (Fig. IA, lower panel). Since glucose levels were unaltered, this suggests that metformin sensitized insulin responsiveness in metformin treated animals. Myocardial glycogen content in both metformin-treated groups was significantly decreased compared with non-treated groups (Fig. IC). We also observed a lower body weight gain in metformin treated animals (both sham and Ml) as compared to the untreated animals (Fig. 1D). Food intake was analyzed, but no consistent differences were observed in time and therefore this lower gain in weight did not appear to be linked to food intake ( data not shown). Therefore, we decided to analyze additional plasma parameters controlling metabolism. In particular active GLP- 1 and adiponectin plasma levels were determined by ELISA. No differences were, however, observed in these parameters among the groups (Table 2), suggesting that the
57
IJ

Chapter 3
differences in weight gain are generated at a different level.
A
B
:; 4 C, .s 3
� 2
.g 1 �
:; 4
1 3
! 2 "' 8 I ci 0
.€ 2
.5 :i "' C - 0
7
� 6 0
� 5 u ::,
3
Sham Sham+Met Ml
#
M l+ M e t
•
C
D
_ 30
.Jg 25
t 20 2: c 15 J!! 8 10 Iii 8' 5 � i3 0
oi �1 2 0
. 5 8 0
0
Sham Sham+Met Ml Ml+Met
S h a m S h a m +Met Ml M l+Met
- sham
-<>-• Sham+Met • Ml • Ml+Met
I
o· ... .----.--..----.---r--��-.--�--,--�---.---.---.---.---.----.---r--�---.---.--o 20 40 60 80 100 120 0 20 40 60 80 100 120 0 20 40 60 80 100 120
Baseline & weeks 12 weeks
Figure I . Mctfonnin levels, glucose levels, insulin levels myocardial glycogen content and body weight
gain at 1 2 weeks after M l surgery. Panel I A, upper panel: serum metformin levels; middle panel: fasting glucose levels; lower panel: plasma insulin level. Panel I B: oral glucose tolerance tests were performed at baseline, 6 weeks and 12 weeks after M l surgery. No significant differences were found among all groups.
Panel I C: Myocardial glycogen content. Panel I D: The use of metformin is associated with attenuated body weight gain. •p 0.05 vs. sham group; #P<0.05 vs. M l group.
Table 2
Active GLP-1 (pM)
Adiponectin (µg/mL)
All values arc means±SEM.
58
Sham
6.71±0.43
15.77±0.49
Sham+Met MI MI+Met
5.65±0.33 5.75±0.21 5.58±0.27
16. 1 8±0.74 15.45±0.55 14.93±0.58

Metformin in post-MI heart failure
Cardiac and hemodynamic parameters Infarct size was significantly smaller in the MI+metformin group as compared to the MI control group (MI+metformin 29.6±3.2% versus MI control 38.0±2.2%, P<0.05) (Table 3 & Figure 6B). As expected, MI caused significant reduction of blood pressure, LVESP, dP/dtmax and dP/dtmin, but no improvement was observed after a 12-weeks treatment with metformin. However, it is of note that sham-operated metformin-treated animals also had significantly lower blood pressure and LV pressure, possibly related to decreased oral (water, food) intake. The LVEDP was increased in the MI group as compared to the sham group, and was slightly decreased in the MI+metformin group as compared to the MI group (Table 3).
Table 3 Body weight, LV weight and body weight ratio, infarct size and hemodynamic parameters.
Sham Sham+Met Ml Ml+Met
BW baseline (g) 320±9 314±6 313±4 313±4
BW 12week (g) 433±15 399±9 428±11 394±12
LVW/BW 2.21±0.08 2.38±0.02 2.23±0.04 2.47±0.04#
Infarct size (%) 0 0 38.0±2.2* 29.6±3.2*#
Heart Rate (bpm) 303±8 273±8* 311±10 274±8#
SBP (mmHg) 116±3 105±3* 105±3* 102±2
DBP (mmHg) 79±3 71±3* 76±1* 70±2
LVESP (mmHg) 117 ±3 106±3* 106±3* 104±2
LVEDP (mmHg) 11±2 14±5 18±4 15±2
dP/dtmax (mmHg/s) 7199±299 5444±264* 5836±390* 5166±166
dP/dtmin (mmHg/s) -8399±553 -6496±524* -5516±669* -5488±197
All values are means±SEM. *Indicates statistically significant difference compared to sham-operated rats (P<0.05) # Indicates statistically significant difference compared to MI control rats (P<0.05) BW=body weight; LVW:(eft ventricle weight; LVWNW=the ratio of left ventricular weight and body weight; bpm, beats per minute; SBP, systolic blood pressure; DBP, diastolic blood pressure; LVESP, left ventricular end-systolic pressure; LVEDP, left ventricular end-diastolic pressure; dP/dtmax and dP/dtmin, the maximal rate of increase and decrease of left ventricular pressure, respectively.
59
IJ

Chapter 3
A B 2 4
3
e e E 1 E UI UI
2: 2
1 0 0
Sham Sham+Met Ml Ml+Met Sham Sham+Met Ml Ml+Met
C D * 1 0
1 0 * 8
e 8 e E 6
'5' E 0
0 4
6 ...J
2 4 0 0 Sham Sham+Met Ml Ml+Met Sham Sham+Met Ml Ml+Met
E F 1 00 50
40 - BO
.5! 30 ti � it 60
20
w40 10
0 0 Sham Sham+Met Ml Ml+Met Sham Sham+Met Ml Ml+Met
Figure 2. Effects of mctformin on echocardiographic parameters. Panel A and Panel B: interventricular septum diameters (IVS) in diastole and systole, respectively; Panels C and D: left ventricular internal dimensions (LYID) in both diastole and systole, respectively; panel E: LY ejection fraction, and panel F: fractional shorten ing of the LY. *P<0.05 vs. sham group; #P<0.05 vs. Ml group.
60

Metformin in post-MI heart failure
The presence of MI was accompanied by wall thinning of the anterior wall (Figure 2A and B) as determined by echocardiography. Treatment with metformin significantly attenuated this wall thinning. Furthermore, 12 weeks after MI, severe LV dilatation was observed as shown by the increased LVIDd and LVIDs, and this resulted in lower FS and LVEF. Again, metformin significantly attenuated LV dilatation and partially prevented LV dysfunction (Figure 2C-F).
A
l <( z a: E
z <(
C
<( z a:
i5
5
4
3
2
0
1 ,5
1 ,0
0,5
0,0
*
Sham Sham+Met Ml Ml+Met
*
Sham Sham+Met Ml Ml+Met
B
D
3
l < 2 z a: E
u, z .. 1
0
j 1 ,0
.!!
8, 0,5 .!!! i5
0,0
Sham Sham+Met Ml Ml+Met
Sham Sham+Met Ml Ml+Met
Figure 3. Quantitative real-time reverse-transcriptase polymerase chain reaction (RT-PCR) was conducted and expression was measured of myocardial atrial natriuretic peptide (ANP; A), endothelial nitric oxide
synthase (eNOS; 8), procollagen (C), and collagen I (D), respectively (mRNA corrected for 3684 mRNA level). The relative corrected values are shown for each group. *P<0.05 vs. sham group; #P<0.05 vs. M l group.
3.3. Cardiac gene expression To assess the molecular changes induced by long-term metformin treatment, cardiac gene expression of ANP, endothelial nitric oxide synthase ( eNOS), procollagen and collagen I were measured by RT-PCR (Figure 3). The ANP mRNA level was
61

Chapter 3
significantly increased after Ml compared to sham (P<0.05), but in metformin treated Ml animals this increase in AN P expression was significantly attenuated (Figure 3A). The eNOS mRNA level was markedly decreased in the Ml group as compared to sham, and metformin partially prevented this sharp decrease in eNOS rnRNA levels in Ml animals (Figure 3B). Similar positive metformin effects were found for procollagen and collagen l expression, which were significantly increased in the Ml group as compared to sham, and with a trend to a limited increase in the metformin-treated group (Figure 3C, D).
A
C
6 � 5 Q.
:I: < 4
� .... 2
Q. :I: < Cl.
1
1,4 "' :g 1,2
(i: 1,0
� 0,8
i2 0,6
� 0.4 D:,- 0,2
0,0
--- --
#
Sham Sham+Met Ml Ml+Met
Sham Sham+Met Ml Ml+Met
,\:\IPKa-r••· ,-,
I otal ,\ \ I Pl\.a
Totnl p70S6K
B
D
4
N u. 3 w .. 0 2 � w 'I' 1 0.
0
i5 4 � 3
� 2
- - - d.F2-P 1 '" ,.
-- Totnll' .. 1:F2
#
Sham Sham+Met Ml Ml+Met
- -- -- - GI.I I �
-·-I .. ,. ___ ,., '�G,\PDII
Sham Sham+Met Ml Ml+Met
Figure 4. Effects of mctfonnin on protein expression. Protein levels of phosphorylation of AMPKaThrI 72, phosphorylation of eEF2 Thr56, phosphorylation of p70S6K Thr389 and GLUT4, measured in the border zone of the MI tissue is shown for all groups. Panel A: Metformin sign ificantly increased the phosphorylation of AMPKaThrI 72 after 1 2 weeks both in sham and MI operated groups. Panel B: Mctfonnin sign ificantly increased the phosphorylation of cEF2 Thr56 12 weeks after MI; Panel C: Metfonnin did not affect the phosphorylation of p70S6K Thr389 among all groups; Panel D: GLUT4 expression is decreased in the M I group after I 2 weeks M I ; Mctformin restored this. N:7-9 for all groups. *P<0.05 vs. sham group; #P<0.05 vs. M I group.
Cardiac protein expression To study the molecular effects of metformin treatment, the phosphorylation of AMPK, eEf2, p70S6K were measured in the heart, as well as GLUT-4 protein levels (Figure 4).
62
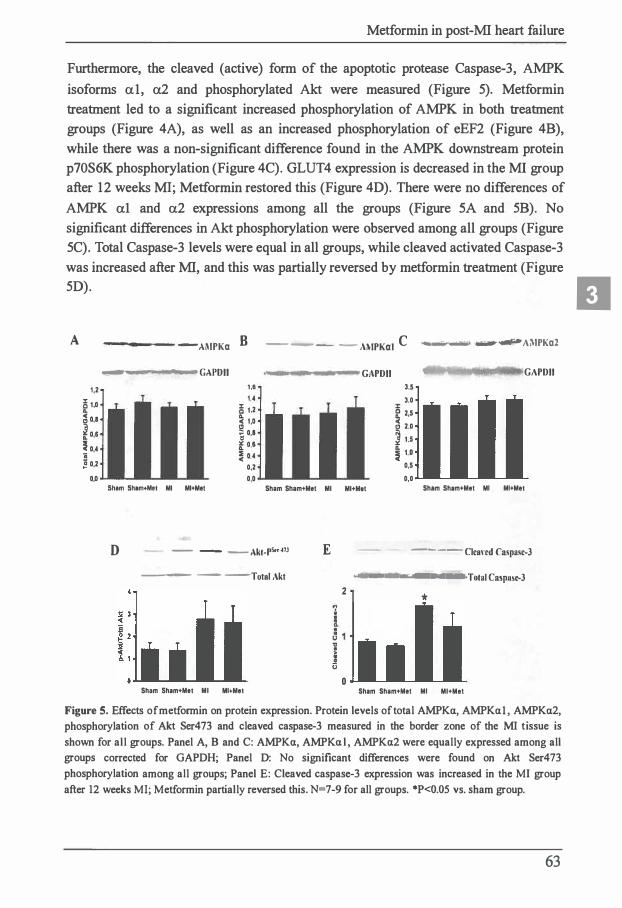
Metformin in post-MI heart failure
Furthermore, the cleaved (active) form of the apoptotic protease Caspase-3, AMPK
isoforms al, a2 and phosphorylated Akt were measured (Figure 5). Metformin
treatment led to a significant increased phosphorylation of AMPK in both treatment
groups (Figure 4A), as well as an increased phosphorylation of eEF2 (Figure 4B),
while there was a non-significant difference found in the AMPK downstream protein
p70S6K phosphorylation (Figure 4C). GLUT4 expression is decreased in the MI group
after 12 weeks Ml; Metformin restored this (Figure 4D). There were no differences of
AMPK al and a2 expressions among all the groups (Figure SA and 5B). No
significant differences in Akt phosphorylation were observed among all groups (Figure
SC). Total Caspase-3 levels were equal in all groups, while cleaved activated Caspase-3
was increased after MI, and this was partially reversed by metformin treatment (Figure
5D).
II A
1,2
5 1,0
� 0,1 � 0,6
� 0,4
;; ! 0,2
0,0
-AMPKa B -- -- - Ai\lPKal C • ,._ ..... -�Ai\lPKa2
� GAPDII 1,8 1,4
S 1,2 .. � 1,0
'ij 0,1 f 0,6 � 0,4
0,2 0,0
Sham Sham+Met Ml Ml+Met Sham Sham+Met
D - -- --Akt-Ps.,m
--- - -Total Akt
Sham Sham+Met Ml Ml+Met
Ml
E
GAPDII GAPDII 3,5
3,0
i 2,5 t, 2,0
l u 1 1.0
0,5
0,0 Ml+Mot Sham Sham+Met Ml Ml+Met
2
0
---- Clcand Caspasc-3
--------•.:Total Caspuse-3
*
Sham Sham+Met Ml Ml+Met
Figure 5. Effects ofmetformin on protein expression. Protein levels of total AMPKa, AMPKal, AMPKa2, phosphorylation of Akt Ser473 and cleaved caspase-3 measured in the border zone of the MI t issue is shown for all groups. Panel A, B and C: AMPKa, AMPKal, AMPKa2 were equally expressed among all groups corrected for GAPDH; Panel D: No significant differences were found on Akt Ser473 phosphorylation among all groups; Panel E: Cleaved caspase-3 expression was increased in the MI group after 12 weeks MI; Metformin partially reversed this. N=7-9 for all groups. *P<0.05 vs. sham group.
63

Chapter 3
1400
1200 * * NE .= 1000
800
600
400
200
0 Sham Sham+Met Ml Ml+Met
B
Sham Sham+Met Ml Ml+Met
C
0,6 *
l 0,5 C
0,4
C 0,3
0 C 0,2
0 0,1 (.)
0,0
Sham Sham+Met Ml Ml+Met
Figure 6. Cardiomyocyte size, infarct size and left ventricular interstitial fibrosis were measured by histology. Panel A: MI was associated with an increase of cardiomyocyte size, and this increase was not modified by metformin treatment. Panel B: Infarct size was measured by sirius red/fast green staining; infarct sizes are presented in Table 2. Panel C: MI induced an increase of interstitial fibrosis of the left ventricular free wall remote from the infracted area, which was partially attenuated by 12 weeks metformin treatment. *P<0.05 vs. sham group.
64

Metformin in post-MI heart failure
Left ventricular hypertrophy and interstitial fibrosis The cross-sectional area of cardiomyocytes was increased in both Ml groups compared to sham groups, and metformin treatment had no effect on the cardiomyocyte hypertrophy in the post-Ml heart failure model (Figure 6A). This contrasts with the LV weights corrected for body weights ratios reported in table 2, which probably is explained by differences in body weights rather than LV weight.Post-Ml heart failure is accompanied by increased fibrosis, which was non-significantly reduced by metformin (Figure 6C).
Discussion
Our study demonstrates that long-term metformin administration is associated with preserved cardiac function in a rat model of post-Ml cardiac remodeling. The key findings are that long-term (12 weeks) metformin treatment after Ml significantly attenuated cardiac remodeling post Ml, evidenced by I) reduced MI size; 2) improved LV geometry (measured by echocardiography); 3) less increase in molecular correlates of LV remodeling (amongst others, less ANP and collagen production); 4) measures of improved glucose and cellular energy metabolism.
Until recently, metformin was contraindicated in HF, mainly because of concerns about lactic acidosis. However, epidemiological data suggest that metformin is safe and may even be the first choice anti-diabetic drug in HF patients with diabetes. In a case-control study in patients with diabetes and HF (N=l.633), metformin was associated with a reduced all cause-mortality (adjusted Odds Ratio (OR) 0.72; P=0.003) 27• In diabetic patients with newly established HF (N=l .305), metformin monotherapy was associated with a reduced I -year mortality when compared with sulfonylurea treatment 28• In HF patients admitted to the hospital (N= I 6.417), metformin use was associated with a lower I-year mortality when compared to treatment with insulin or sulfonylurea (24.7% vs. 36.0%, P<0.0001 ) 29• All-cause re-admission and HF hospitalization were also less common in diabetic patients treated with metformin than in those not treated with an insulin-sensitizing drug. Although results from prospective randomized placebo controlled clinical trials are lacking, these data strongly suggest that metformin use is associated with a better outcome in clinical HF in diabetic patients.
It has been shown that metformin exerts cardioprotective effects in various experimental set-ups, although mostly acute cardiac damage models. First, Solskov et al reported that metformin exerted a protective effect on the rat heart subjected to cardiac ischemia/reperfusion injury in an in vitro Langendorff setup 1 2• This study indicated that, at least in vitro, metformin could exert protective effects when
65
IJ

Chapter 3
administered before a coronary occlusion was inflicted. Another acute study confirmed the cardioprotective effect of metformin in mice subjected to cardiac ischemia/reperfusion model in vivo, also when administered during the reperfusion stage 30
• This indicated that also in vivo, metformin exerts protective effects after Ml, which was confirmed in another study with a longer follow-up, showing improved left ventricular function and survival in mice subjected to ischemia reperfusion injury 8. Moreover, metformin was shown to attenuate cardiac fibrosis induced by pressure overload in mice model and inhibited collagen synthesis 1 3. Interestingly, in dogs in a model of rapid pacing metformin could also prevent progression of HF 1 1 • The precise actions of metformin on the heart are still not fully elucidated, but a central role of activation of AMPK, which is a regulator of cellular energy formation, has been proposed K, 1 1 , t3 , 30
_
Our study is unique in that it used a model of chronic (instead of temporary) ligation of a coronary artery, which leads to large myocardial infarction and cardiac remodeling that resembles the human sequel of events. We herein show that chronic metformin treatment is associated with a decreased extent of myocardial damage, possibly due to both necrosis and apoptosis resulting in reduced Ml size, which is associated with less remodeling over time. Metformin has been shown to inhibit apoptosis, as reported in a dog model of heart failure 1 1
• We found that cleaved caspase-3 levels were increased post-Ml, as reported before 3 1 ; however the use of metformin only non-significantly reduced caspase-3 levels. Increased levels of the anti-apoptotic protein Akt arc associated with suppression of AMPK phosphorylation, which can be restored by metformin 32
• On the other hand, Sasaki et al. 1 1 showed that metformin treatment causes decreased Akt phosphorylation in failing hearts. In our study, the use of mctformin was not associated with meaningful differences in phosporylatcd levels of Akt. Therefore we conclude that the beneficial effects of mctformin cannot, or only marginally, be explained by differences in apoptosis. We furthermore confirm the inhibitory effect of metformin on fibrosis, evidenced in multiple experimental models, indicating that this is a general metformin associated cardiac phenomenon and not only linked to pressure overload model and pacing mode 1 1 • 1 3
• In our study, we observed a decreased expression of collagens and reduced fibrosis.
In support of another study 8, the cardioprotective effects appeared to be
independent of antihyperglycemic effects of metformin. In fact, fasting glucose levels and OGTTs were similar in all groups, despite lower insulin levels in the metformin treated animals. This suggests an insulin sensitizing effect of metformin, resulting in insulin level reductions, lower myocardial glycogen content, enhanced GLUT4 expression, while maintaining normal plasma glucose levels. These observations suggest an improved myocardial glucose uptake, but we did not measure this. Except
66
Metformin in post-Ml heart failure
for insulin, plasma levels of other metabolic hormones did not change, indicating that metformin did not generate major systemic changes. Nevertheless, weight gain in metformin treated animals was reduced and this could not be simply related to changed food uptake. Although, we cannot exclude that nutrient uptake in the intestine has changed, our observation that metformin activates AMPK might point more into the direction of increased cellular metabolism. As described, AMPK is an enzyme that is activated in response to changes in cellular energy metabolism, for instance in muscle contraction, ischemia or by pharmacological agents like metformin 33. In our study, metformin treatment led to an increased phosphorylation of AMPK, resulting in an increased phosphorylation of one of its downstream targets, eukaryotic elongation factor-2 (eEF2). Moreover, activated AMPK has a fundamental role in glycogen synthesis and glucolysis 34, which is supported by our study showing that long-term metformin treatment causes a decreased glycogen content in the myocardium, an observation that is common to most antidiabetic drugs 35. All these effects suggest that metformin may restore the cellular energy flux by inhibition of processes that switch off the ATP-consuming pathways to protect the stressed heart 36•
We observed a strong insulin lowering effect of chronic metformin treatment. It has become apparent that a strong association exists between hyperinsulinemia and incident heart failure. A recent paper provided proof that cardiac insulin signaling itself also exacerbates cardiac remodeling 37. Therefore, part of the beneficial effects that we report herein may be due to low insulin levels and signaling.
AMPK is activated during caloric restriction and stimulates cellular metabolic pathways in order to maintain energy supply. Interestingly, caloric restriction confers cardioprotective effects and metformin-treated animals and long-term dietary restriction animals have similar gene expression patterns 38. Together, this might suggest that the activation of certain AMPK downstream effectors in the heart, rather than changes in cellular metabolism itself, confers cardioprotective effects.
Limitations of the study Sample size and thus power is limited. We started administration of metformin two days before MI, so we cannot separate early and late protective effects in this study. The dose of metformin used in this study was comparable to other studies in rodents and humans (200mg-350mg/kg/day) 15• 39, we established this dose did not cause side-effects like hypoglycemia and renal dysfunction ( data not shown). Since metformin affects various targets, including AMPK and many downstream targets, the study design does not allow proving causality between the molecular targets and functional outcome.
67
IJ

Chapter 3
Conclusions In summary, our study demonstrated that metformin exerts a protective effect on cardiac remodeling in non-diabetic rats with post-Ml heart failure. We postulate that AMPK and low insulin levels are important mediators in the protective effects. These findings underscore the potential beneficial effects of metformin in HF, and provide further evidence that metformin should be prospectively tested for its safety and efficacy in HF, e.g. in a post-Ml trial. We recently launched such a trial (Metformin to Reduce Heart Failure After Myocardial Infarction; NCT0 1217307).
Acknowledgement Supported by the Netherlands Heart Foundation (grant 2007T046) and the lnnovational Research Incentives Scheme program of the Netherlands Organization for Scientific Research (NWO VENI, grant 016.106.117), both to Dr. de Boer.
68

Metformin in post-Ml heart failure
References
I . de Boer RA, Doehner W, van der Horst IC, Anker SD, Babalis D, Roughton M, et al. Influence of diabetes mellitus and hyperglycemia on prognosis in patients > or =70 years old with heart failure and effects of nebivolol ( data from the Study of Effects of Nebivolol Intervention on Outcomes and Rehospitaiization in Seniors with heart failure [SENIORS]). Am J Cardiol 201 0;106:78-86.e l .
2. MacDonald M R, Petrie MC, Varyani F, Ostergren J, Michelson EL, Young JB, et al.
3.
Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur Heart J 2008;29: 1 377- 1 385.
van Melle JP, Bot M, de Jonge P, de Boer RA, van Veldhuisen DJ, Whooley MA. Diabetes, glycemic control, and new-onset heart failure in patients with stable coronary artery disease: data from the heart and soul study. Diabetes Care 201 0;33:2084-2089.
4. Dickstein K, Cohen-Sola! A, Filippatos G, McMurray JJ, Ponikowski P, Poole-Wilson PA, et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the diagnosis and treatment of acute and chronic heart failure 2008 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur J Ileart Fail 2008;10:933-989.
5. Eurich DT, McAlister FA, Blackbum DF, Majumdar SR, Tsuyuki RT, Varney J, et al. Benefits and harms of antidiabetic agents in patients with diabetes and heart failure: systematic review. BMJ 2007;335:497.
6. Kirpichnikov D, McFarlane S I, Sowers JR. Metformin: an update. Ann Intern Med 2002;137:25-33.
7. UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). UK Prospective Diabetes Study (UKPDS) Group. lancet I 998;352:854-865.
8. Gundewar S, Calvert JW, Jha S, Toedt-Pingel I, Ji SY, Nunez D, et al. Activation of AMP-activated protein kinase by metformin improves left ventricular function and survival in heart failure. Circ Res 2009;104:403-4 1 1 .
9. Chan A Y , Dyck JR. Activation of AMP-activated protein kinase (AMPK) inhibits protein synthesis: a potential strategy to prevent the development of cardiac hypertrophy. Can J Physiol Pharmacol 2005;83:24-28.
69
IJ

Chapter 3
10. Musi N, l lirshman MF, Nygren J, Svanfeldt M, Bavcnholm P, Rooyackers 0, el al. Metformin increases AMP-activated protein kinase activity in skeletal muscle of subjects with type 2 diabetes. Diabetes 2002;51 :2074-208 1 .
1 1 . Sasaki 1 1, Asanuma 1 1, Fujita M, Takahama H, Wakeno M, Ito S, et al. Metformin prevents progression of heart failure in dogs: role of AMP-activated protein kinase. Circulation 2009;1 19:2568-2577.
12. Solskov L, Lofgren B, Kristiansen SB, Jessen N, Pold R, Nielsen TT, el al. Metformin induces cardioprotection against ischaemia/reperfusion injury in the rat heart 24 hours after administration. Basic Clin Pharmacol Toxicol 2008;1 03:82-87.
1 3 . Xiao H , Ma X, Feng W, Fu Y, Lu Z, Xu M , el al. Metformin attenuates cardiac fibrosis by inhibiting the TGFbeta I -Smad3 signalling pathway. Cardiovasc Res 20 I 0;87:504-5 13 .
14. Kewalramani G, Puthanvectil P, Wang F, Kim M S, Deppe S, Abrahani A, el al. AMP-activated protein kinase confers protection against TNF- {alpha}-induced cardiac cell death. Cardiovasc Res 2009;84:42-53.
1 5. Zou M l I, Kirkpatrick SS, Davis BJ, Nelson JS, Wiles WG,4th, Schlattner U, el al. Activation of the AMP-activated protein kinase by the anti-diabetic drug metformin in vivo. Role of mitochondrial reactive nitrogen species. J Biol Chem 2004;279:43940-4395 1 .
16. Hardie DG. Minireview: the AMP-activated protein kinase cascade: the key sensor of cellular energy status. Endocrinology 2003 ;144:5 1 79-5 1 83.
1 7. James AP, Watts GF, Mamo JC. The effect of metfonnin and rosiglitazone on postprandial lipid metabolism in obese insulin-resistant subjects. Diabetes Obes Metab 2005;7:38 1 -389.
18 . Stumvoll M, Nurjhan N, Perriello G, Dailey G, Gerich JE . Metabolic effects of mctfonnin in non-insulin-dependent diabetes mcllitus. N Engl J Med I 995;333:550-554.
19. Wu M S, Johnston P, Sheu WI I, Hollenbeck CB, Jeng CY, Goldfine ID, el al. Effect of mctfonnin on carbohydrate and lipoprotein metabolism in NIDDM patients. Diabetes Care 1 990;13 : l -8.
20. Cuthbertson J, Patterson S, O'l larte FP, Bell PM. Investigation of the effect of oral metfonnin on dipeptidylpeptidase-4 (DPP-4) activity in Type 2 diabetes. Diabet Med 2009;26:649-654.
2 1 . Maida A, Lamont BJ, Cao X, Drucker DJ. Metformin regulates the incretin receptor axis via a pathway dependent on peroxisome proliferator-activated receptor-alpha in mice. Diabetologia 201 1 ;54:339-349.
70

Metformin in post-Ml heart failure
22. Oeseburg H, de Boer RA, Buikema H, van der I larst P, van Gilst WH, Sillje H H. Glucagon-like peptide I prevents reactive oxygen species-induced endothelial cell senescence through the activation of protein kinase A. Arteriosc/er Thromb Vase Biol 20 1 0;30 : 1407- 14 14.
23. de Boer RA, Pinto YM, Suurmeijer AJ, Pokharel S, Scholtens E, Humler M, et al. Increased expression of cardiac angiotensin II type I (AT( I )) receptors decreases myocardial microvessel density after experimental myocardial infarction. Cardiovasc Res 2003;57:434-442.
24. Kuipers I, Li J, Vreeswijk-Baudoin I, Koster J, van der Harst P, Sillje HH, et al. Activation of liver X receptors with T0901 3 I 7 attenuates cardiac hypertrophy in vivo. Eur J Heart Fail 201 0;12 : 1 042- 1 050.
25. de Boer RA, Pokharel S, Flesch M, van Kampen DA, Suurmeijer AJ, Boomsma F, et al. Extracellular signal regulated kinase and SMAD signaling both mediate the angiotensin I I driven progression towards overt heart failure i n homozygous TGR(mRen2)27. J Mo/ Med (Berl) 2004;82:678-687.
26. Westenbrink BD, Lipsie E, van der Meer P, van der 1- larst P, Oeseburg 1 1, Du Marchie Sarvaas GJ, et al. Erythropoietin improves cardiac function through endothelial progenitor cell and vascular endothelial growth factor mediated neovascularization. Eur Heart J 2007;28:20 1 8-2027.
27. MacDonald MR, Eurich DT, Majumdar SR, Lewsey JD, Bhagra S, Jhund PS, et al. Treatment of type 2 diabetes and outcomes in patients with heart failure: a nested case-control study from the U.K. General Practice Research Database. Diabetes Care 201 0;33 : 1 2 1 3- 1 2 1 8.
28. Matthews DR, Cull CA, Stratton IM, Holman RR, Turner RC. UKPDS 26: Sulphonylurea failure in non-insulin-dependent diabetic patients over six years. UK Prospective Diabetes Study (UKPDS) Group. Diabet Med I 998;15 :297-303.
29. Masoudi FA, lnzucchi SE, Wang Y, Havranek EP, Foody JM, Krumholz HM. Thiazolidinediones, metformin, and outcomes i n older patients with diabetes and heart failure: an observational study. Circulation 2005;1 1 1 :583-590.
30. Calvert JW, Gundewar S, Jha S, Greer JJ, Bestermann WH, Tian R, et al. Acute metformin therapy confers cardioprotection against myocardial infarction via AMPK-eNOS-mediated signaling. Diabetes 2008;57:696-705.
3 1 . de Boer RA, van Veldhuisen DJ, van der Wijk J, Brouwer RM, de Jonge N, Cole GM, et al. Additional use of immunostaining for active caspase 3 and cleaved actin and PARfragments to detect apoptosis in patients with chronic heart failure. J Card Fail 2000;6:330-337.
7 1
I]

Chapter 3
32. Kovacic S, Soltys CL, Barr AJ, Shiojima I, Walsh K, Dyck JR. Akt activity negatively regulates phosphorylation of AMP-activated protein kinase in the heart. J Biol Chem 2003 ;278:39422-39427.
33. Musi N, Goodyear LJ . AMP-activated protein kinase and muscle glucose uptake. Acta Physiol Scand 2003;178:337-345.
34. Wong AK, l lowie J, Petric JR, Lang CC. AMP-activated protein kinase pathway: a potential therapeutic target in cardiometabolic disease. Clin Sci (Land) 2009;1 16:607-620.
35. Kristiansen SB, Nielsen-Kudsk JE, Botker I IE, Nielsen TT. Effects of KATP channel modulation on myocardial glycogen content, lactate, and amino acids in nonischcmic and ischemic rat hearts. J Cardiovasc Pharmacol 2005;45:456-46 1 .
36. 1 lardic DG. Sensing of energy and nutrients by AMP-activated protein kinase. Am J Clin Nutr 201 I ;93:89 1 S-6.
37. Shimizu I, Minamino T, Toko 1 1, Okada S, Ikeda 1 - 1, Yasuda N, et al. Excessive cardiac insulin signaling exacerbates systolic dysfunction induced by pressure overload in rodents. J Clin Invest 20 1 0;120: 1 506- 1 5 14.
38. Dhahbi JM, Mote PL, Fahy GM, Spindler SR. Identification of potential caloric restriction mimetics by microarray profiling. Physiol Genomics 2005;23:343-350.
39_ Buzzai M, Jones RG, Amaravadi RK, Lum JJ, DeBerardinis RJ, Zhao F, et al. Systemic treatment with the antidiabetic drug metformin selectively impairs p53-deficient tumor cell growth. Cancer Res 2007;67:6745-6752.
72

Chapter 4
Early and late effects of the DPP-4 inhibitor vildagliptin
in a rat model of post-myocardial infarction heart failure
Meimei Yin, Herman H. W Sillje, Maxi Meissner, Wiek H. van Gi/st, Rudolf A. de Boer
University Medical Center Groningen, University of Groningen, Department of
Cardiology, Groningen, The Netherlands
Cardiovasc Diabetol. 201 1 Sep 28;10:85.
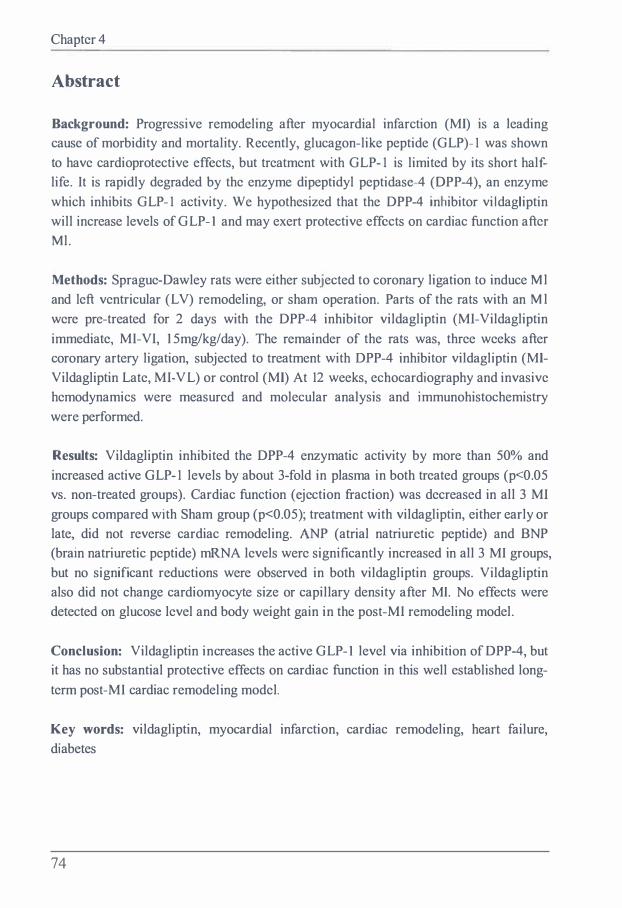
Chapter 4
Abstract
Background: Progressive remodeling after myocardial infarction (MI) is a leading cause of morbidity and mortality. Recently, glucagon-like peptide (GLP)- 1 was shown to have cardioprotective effects, but treatment with GLP- 1 is limited by its short halflife. It is rapidly degraded by the enzyme dipeptidyl peptidase-4 (OPP-4), an enzyme which inhibits GLP- 1 activity. We hypothesized that the DPP-4 inhibitor vi ldagliptin will increase levels of GLP-1 and may exert protective effects on cardiac function after Ml.
Methods: Sprague-Dawley rats were either subjected to coronary ligation to induce Ml and left ventricular (LV) remodeling, or sham operation. Parts of the rats with an M l were pre-treated for 2 days with the DPP-4 inhibitor vildagliptin (MI-Vildagliptin immediate, MI-VI, 15mg/kg/day). The remainder of the rats was, three weeks after coronary artery ligation, subjected to treatment with DPP-4 inhibitor vildagliptin (MlVildagliptin Late, MI-VL) or control (Ml) At 12 weeks, echocardiography and invasive hemodynamics were measured and molecular analysis and immunohistochemistry were performed.
Results: Vildagliptin inhibited the DPP-4 enzymatic activity by more than 50% and increased active GLP- 1 levels by about 3-fold in plasma in both treated groups (p<0.05 vs. non-treated groups). Cardiac function (ejection fraction) was decreased in all 3 MI groups compared with Sham group (p<0.05); treatment with vildagliptin, either early or late, did not reverse cardiac remodeling. ANP (atrial natriuretic peptide) and BNP (brain natriuretic peptide) mRNA levels were significantly increased in all 3 MI groups, but no significant reductions were observed in both vildagliptin groups. Vildagliptin also did not change cardiomyocyte size or capillary density after Ml. No effects were detected on glucose level and body weight gain in the post-MI remodeling model.
Conclusion: Vildagliptin increases the active GLP-1 level via inhibition of DPP-4, but it has no substantial protective effects on cardiac function in this well established longterm post-MI cardiac remodeling model.
Key words: vildagliptin, myocardial infarction, cardiac remodeling, heart failure, diabetes
74

DPP-4 inhibiton in post-Ml heart failure
Introduction
Glucagon-like peptide- l (GLP-1; 7-36 amide), which belongs to the proglucagon family of incretin peptides, is secreted by enterendocrine L cells of the intestinal mucosa and released in response to food intake 1
• GLP-l analogues have been used for the clinical treatment of type 2 diabetes because of its multiple actions on pancreatic function 24. Besides its effects on glucose metabolism, GLP-l has been proven to exert cardiovascular effects in clinical and experimental studies, in the presence or absence of diabetes 5•
GLP- l receptors (GLP- l R) are expressed in rodent and human heart and vasculature 6-8. GLP- lR deficient mice exhibit increased left ventricular (L V) thickness, impaired LV contractility and LV diastolic function compared with control mice 9•
However, whether the beneficial effects of GLP-l on the heart are conferred through direct GLP-lR signaling or indirect, through the GLP-I R-dependent improvement in glucose metabolism is not well established. Administration of GLP-1 improves myocardial function and cardiac output in experimental models of cardiac injury or heart failure. GLP-1 increased cardiac output, and reduced L V end diastolic pressure, in association with improved myocardial insulin sensitivity and myocardial glucose uptake in dogs with rapid pacing-induced congestive heart failure 10. Consistent with the cytoprotective action of GLP-1 in the endocrine pancreas, GLP-1 reduced infarct size in the isolated perfused rat heart and in animal models of myocardial ischernia 1 1 - 1 3
_
A 72 hours infusion of GLP- 1 in patients with acute myocardial infarction (Ml) and an L V ejection fraction (L VEF) less than 40% resulted in significantly improved L VEF and improved regional and global wall motion scores, in association with a trend towards earlier hospital discharge 1 4
• In a pilot study of both diabetic and non-diabetic subjects with heart failure, an improved L V function was observed following a 5 week continuous infusion ofGLP- 1(7-36) 5•
However, active GLP-1 in the circulation is rapidly (within two minutes) degraded by dipeptidyl peptidase-4 (DPP-4) 15
• An alternative approach for enhancing GLP-1 action involves the use of DPP-4 inhibitors. The DPP-4 inhibitor sitagliptin 1 6
and saxagliptin 1 7 have been approved for type 2 diabetic patients. Vildagliptin is approved and used in Europe 1 8•
The studies on cardiovascular effects of GLP-1, discussed above, have consequently assessed only short-term improvements in cardiac performance, like in post-ischemic or cardiomyopathy states. There are no reports on long-term effects of DPP-4 inhibition in a post-Ml cardiac remodeling model. Furthermore, the actions of DPP-4 inhibitors on cardiac remodeling after Ml are incompletely understood. We hypothesized that the DPP-4 inhibitor vildagliptin may exert beneficial effects on
75
I

Chapter 4
infarcted hearts by inhibiting the degradation of active GLP- 1 and other cardiovascular peptides. The purpose of our study was therefore to determine whether vildagliptin has beneficial effects on long-term post-MI remodeling in rats and to explore the mechanisms underpinning these effects.
Methods and Materials
Animals Male Sprague-Dawley rats (Harlan, Zeist, The Netherlands) weighing 250-260g were housed in groups of 4-5 on a 12-hour light-dark cycle with standard rat chow and water available ad libitum. The animals were subjected to sham-surgery or left coronary artery ligation. All experiments were carried out after approval of the Animal Ethical Committee of the University of Groningen for the use of experimental animals and conform to the Guide for Care and Use of Laboratory Animals.
Drugs The DPP-4 inhibitor vildagliptin was kindly supplied by Novartis, The Netherlands. Vildagliptin was dissolved in the drinking water and administered in a final concentration of 15mg/kg/day, which is chosen according to the previous studies 1 9• 20
Experimental protocol Rats were randomly subjected to induction of MI or sham surgery. Briefly, animals were intubated and mechanically ventilated with 2.5% isoflurane in room air emiched with 1 .0L/min oxygen. After left-sided thoracotomy, MI was induced by ligating the proximal portion of the left coronary artery. In sham-operated rats, the same surgery was performed without ligating the suture. Parts of the rats with an MI were pre-treated for 2 days with vildagliptin (MI-Vildagliptin immediate, Ml-VI). The remainder of the rats was, three weeks after coronary artery ligation, subjected to treatment with DPP-4 inhibitor vildagliptin (Ml-Vildagliptin Late, Ml-VL) or control (Ml). At week 12, cardiac function was determined by echocardiography. After 1 2 weeks, rats were anaesthetized and hcmodynamic function was measured invasivcly; thereafter blood was drawn ( either anticoagulated with EDT A, or left to clot for serum) and the hearts were rapidly excised. Myocardial tissue was sectioned transversally and processed for immunohistochemistry or snap-frozen for molecular analysis.
Echocardiographic measurements Cardiac function was assessed by echocardiography by a Vivid 7 (GE Healthcare) equipped with a IO-MHz phase array linear transducer. The echocardiographic
76

DPP-4 inhibiton in post-Ml heart failure
measurements were performed under general anaesthesia with 2.5% isoflurane, by a researcher blinded for the treatment allocation. Both 2-dimensional (2D) images in parasternal long-axis and short-axis view and 2-D guided M-mode tracings were obtained. Short-axis views were recorded at the level of mid-papillary muscles. L V internal dimensions in diastole and systole {LVIDd and LVIDs) were measured using M-mode and calculated from three cardiac cycles. LV fractional shortening (FS %) was calculated as follows: FS = {L VIDd-L VIDs )/L VIDdx 1 00%. L V ejection fraction (EF %) was calculated using the Teichholz method.
Hemodynamic measurements At sacrifice, rats were anesthetized and a micro-tip pressure transducer (Millar Instr. Inc., Houston, TX, USA) was inserted into the right carotid artery. Arterial systolic and diastolic blood pressures (SBP, DBP) were recorded in the aortic arch. The catheter was advanced into the LV cavity. After a 5-min period of stabilization, heart rate (HR), LV systolic pressure {LVSP), LV end-diastolic pressure {LVEDP), and developed L V pressure ( dLVP=L VSP-L VEDP) were measured. For indices of contractility and relaxation, the maximal rates of increase and decrease in L VP dp/dtmax and dpldtmin were determined.
Procurement of heart tissue and infarct size measurement After the rats were euthanized, hearts were rapidly excised and arrested in diastole in 2M ice-cold KC!. The total heart was weighed (heart weight, HW). The right ventricle and atria were removed, and the left ventricle was weighed (left ventricular weight, LVW). The basal and apical parts of the LV were snap-frozen in liquid nitrogen. A mid-papillary slice of the L V was fixed in 4% paraformaldehyde overnight and paraffin-embedded. Paraffin blocks were sectioned, and slides were dehydrated. The 5 µm sections were stained with picrosirius red/fast green 2 1 • The infarct size was calculated as percentage of the scar length to the total L V circumference. The images were obtained with a Leica microscope and analyzed using appropriate software (Image-pro plus, version 4.5.0.29).
Active GLP-1 assay and DPP-4 activity EDTA plasma was used to measure active GLP- 1 and DPP-4 activity, using a commercial Enzyme Linked lmrnunosorbent Assay, according to the guidelines provided by the manufacturer (Quantikine, R&D system, London, UK).
Analytical procedures Glucose levels were measured with a blood glucose monitor (Accu-Check®, Roche, Germany). Plasma triglyceride and cholesterol levels were determined using
77
II

Chapter 4
commercially available kits (Roche Diagnostics, Mannheim, Germany and DiaSys Diagnostic Systerms, Holzheim, Germany).
Capillary density To visualize the capillaries in the myocardium, endothelial cells were stained with Lcction GSI (Sigma-Aldrich Chemie, Zwijndrecht, The Netherlands), as previously described 22• Briefly, 5-µm sections were deparaffinised and rehydrated and endogenous peroxidase was inhibited by methanol/H202 (0.3%) for 15 minutes. Sections were incubated overnight with biotinylated Lectin GSI (1 :100) at room temperature. Then, in a second step, the signal was intensified with an ABC-complex containing peroxidase labeled biotins ( I : 100) (Lab vision, CA, USA). Finally, the sections were incubated with a Ni-Co amplified DAB solution to which a stable peroxide substrate buffer was added (Pierce, CA, USA). Endothelial cells of capillaries and larger vessels were visualized in the myocardium as a brown precipitate. A background staining was not used in order to avoid interference with the Lectin staining. Capillary density in the viable L V wall was calculated as the number of capillaries per tissue area.
Left ventricular hypertrophy First, left ventricular hypertrophy was expressed as the ratio of left ventricular weight to body weight. Microscopically, left ventricles were cut into 5 µm transversal slices from apex to base. Afterwards, sections were stained with a Gomori' s silver staining in order to visualize the membrane of the cardiomyocytes, as described previously 2 1 •
Cardiomyocyte size was measured transversally cut in the border zone of the infarcted area using image analysis (Zeiss KS400, Germany).
Real-time PCR We used myocardial tissue (of border zone of the infarction) to extract total RNA with TRlzol reagent (lnvitrogen Corp., Carlsbad, CA, USA). The nano-drop device was used to quantify the RNA concentration. First strand cDNA was synthesized by reverse transcription reaction by using random primer mix, and used as a template to amplify genes of interest; for this specific primers against ANP (atrial natriuretic peptide), BNP (brain natriurctic peptide), collagen I, MMP-9 (matrix metalloproteinase-9) were designed. All gene expression values were normalized to 36B4 mRNA levels.
Data analysis All data are presented as means ± standard errors of the mean (sem). Data of infarcted rats were only included if the infarction comprised the major part of the LV free wall, since small infarctions ( <20%) are found to be hemodynamic fully compensated (two
78

DPP-4 inhibiton in post-MI heart failure
animals were excluded from the MI group, and three animals were excluded from each vildagliptin-treated groups MI-VI and MI-VL). Statistical analysis among groups was performed by one-way analysis of variance (ANOVA) followed by Tukey post-hoc test. Within-group comparisons between week 3 and week 12 were analyzed by PairedSample T-Test. Differences were considered statistically significant if p<0.05.
Results
Active GLP-1, DPP-4 activity and glucose levels We measured the DPP-4 activity and active GLP-1 levels in plasma after 1 2 weeks of vildagliptin treatment to confirm that continuous administration of vildagliptin (supplied at 20mg/kg in the drinking water) was indeed associated with suppression of plasma DPP-4 activity, and increase in the active GLP-1 levels. Plasma DPP-4 activity was significantly reduced by almost 70% in both treatment groups compared to nontreated groups. This was associated with a significant increase of the active GLP-1 level in both vildagliptin groups (Figure I).
During the 12 weeks of follow up, we measured glucose levels at baseline, week 6 and week 12. No significant changes in glucose levels were observed, suggesting that vildagliptin has no effect on normal glucose levels. The similar findings were observed in plasma cholesterol and triglycerides that no significant differences were found among all groups (Table lB).
A
25
15 20 E
� 1 5 ..J (!)
ffi 1 0
.2: 5 �
0 Sham
B
Ml Ml-VI MI-VL Sham Ml Ml-VI MI-VL
Figure 1 . Effects of Vildagliptin on DPP-4 activity and active GLP-1 levels.A: Vildagliptin reduces DPP-4
activity after 1 2 weeks treatment. B: Vildagliptin increases active GLP-1 levels in plasma after 1 2 weeks treatment. Data are presented as mean±SE. N=S-10 for all groups. *P<0.05 vs. sham group; $P<0.05 vs. M l group.
79
II

Chapter 4
Body Weight, LV weight, and infarct Size Body weight (BW), L V weight (L VW) to body weight ratios (L VW /BW) and infarct sizes are shown in Table I A. Ligation of the left coronary artery resulted in an infarct size of 47±2 % in control-treated MI group (Figure 2B). Although there was no significant reduction in the infarct size, vildagliptin treatment (both immediate and late) was associated with a trend towards smaller infarct size over the 3-month period of treatment compared with the MI control group (Figure 2B) .Thcrc was no difference in body weight between groups both at baseline and at 12 weeks after Ml surgery. The LVW/BW ratios in all Ml groups were significantly increased compared to LVW/BW of the sham-operated group, however, LV hypertrophy was not significantly reduced by vildagliptin treatment (both groups) compared to MI control (Table I A).
Table 1 Characteristics of the experimental groups at sacrifice (12 weeks).
Sham MI MI-VI MI-VL N=S N=lO N=9 N=9
A BW (g) 321±9 313±5 321±2 306±4 (baseline) BW (g) 446±15 449±1 1 436±5 450±7 (12 week) LVW (g) 0.93±0.03 1 .05±0.03* 0.97±0.02 1.08±0.03* (12 week) LVW/BW 2.00±0.05 2.34±0.09** 2.22±0.05 2.39±0.05**
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - · 8 Glucose(mmol/L) 9.00±0.61 7.97±0.47 7.81±0.3 1 9.52±0.42
(3 week) Glucose(mmol/L) 7.15±0.2 1 7.25±0.28 7.06±0. 1 4 7.67±0.17 (6week) Glucose (mmol/L) 8.01±0.34 7.3 1±0.20 7.99±0.3 1 7.64±0.22 (12week) Cholesterol 1 .49±0.09 1.48±0.04 1.45±0.08 1 .39±0.07 (mmol/L)
Triglycerides 0.95±0. 1 9 1.12±0.13 0.84±0. 1 1 0.86±0. 1 2 (mmol/L)
Data arc presented as mean ± SEM; N indicates number of animals; BW, body weight; LVW, left ventricle weight; L VW/BW, left ventricle weight / body weight ratio. **P<0.0 I vs. Sham. *P<0.05 vs. Sham.
80
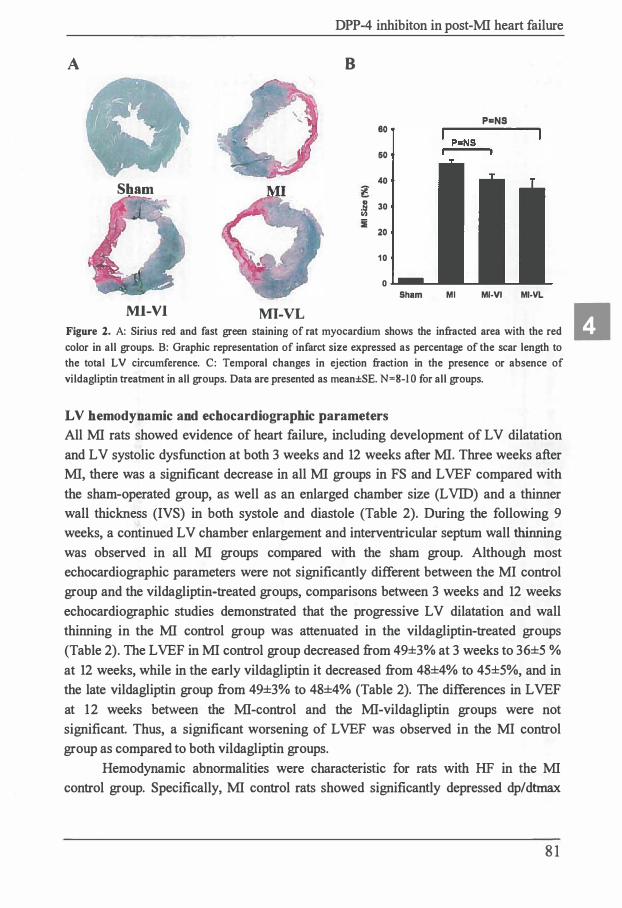
A
Sham
Ml-VI MI-VL
DPP-4 inhibiton in post-MI heart failure
8
80
60
40
I 30
20
10
0 Sham
P=NS
Ml Ml-VI Ml-Vl
Figure 2. A: Sirius red and fast green staining of rat myocardium shows the infracted area with the red color in all groups. B: Graphic representation of infarct size expressed as percentage of the scar length to the total L V circumference. C: Temporal changes in ejection fraction in the presence or absence of vildagliptin treatment in all groups. Data are presented as mean±SE. N=8-I O for all groups.
L V hemodynamic and echocardiographic parameters All MI rats showed evidence of heart failure, including development of L V dilatation
and L V systolic dysfunction at both 3 weeks and 12 weeks after MI. Three weeks after
MI, there was a significant decrease in all MI groups in FS and L VEF compared with
the sham-operated group, as well as an enlarged chamber size (L VID) and a thinner
wall thickness (IVS) in both systole and diastole (Table 2). During the following 9
weeks, a continued L V chamber enlargement and interventricular septum wall thinning
was observed in all MI groups compared with the sham group. Although most
echocardiographic parameters were not significantly different between the MI control
group and the vildagliptin-treated groups, comparisons between 3 weeks and 12 weeks
echocardiographic studies demonstrated that the progressive L V dilatation and wall
thinning in the MI control group was attenuated in the vildagliptin-treated groups
(Table 2). The L VEF in MI control group decreased from 49±3% at 3 weeks to 36±5 %
at 12 weeks, while in the early vildagliptin it decreased from 48±4% to 45±5%, and in
the late vildagliptin group from 49±3% to 48±4% (Table 2). The differences in L VEF
at 12 weeks between the MI-control and the MI-vildagliptin groups were not
significant. Thus, a significant worsening of L VEF was observed in the MI control
group as compared to both vildagliptin groups.
Hemodynamic abnormalities were characteristic for rats with HF in the MI
control group. Specifically, MI control rats showed significantly depressed dp/dtmax
8 1
II

� I Table 2 Echocardiographic parameters of the experimental groups at week 3 and week 12. Week 3 Week 12
Sham MI Ml+VI MI+VL Sham MI Ml+VI Ml+VL
N=8 N=lO N=9 N=9 N=8 N=lO N=9 N=9 HR (bpm) 377±1 1 379±9 383±1 1 407± 1 1 370±12 387±6 377±10 391±6
IVSd(mm) 1 .5±0.1 0.9:t:0.1•• 1 .0±0.01 * 1 .0±0.1 * 1 .6±0.l 0.8±0.1 ** 1 .0±0.1 * 0.8:t:0. 1••
LVIDd(mm) 7.7±0.1 8.3±0.3 8.4±0.2 8.1±0.3 8.0±0.4 l 0. 1±0.3** § 9.7±0.4** § 9.7±0.2 •• §
LVPWd(mm) 1 .8±0.1 1 .8±0.1 1 .9±0. 1 1 .8±0.1 2.1±0.2 2.3±0.2 2.0±0.12 2.0±0.1
IVSs(mm) 2.9±0.1 1 .3±0.2* 2.0±0.6 1 .3±0.2* 2.9±0.2 1 .0±0.2•• 1 .2±0.2•• 1.2±0.2**
LVIDs(mm) 4.2±0. 1 6.5±0.3** 6.0±0.4** 6.3±0.3** 4.6±0.4 8.6±0.5** § 7.7±0.4** 7.6±0.2** §
LVPWs(mm) 2.9±0.1 2.7±0.1 2.6±0.2 2.5±0.1 2.9±0.2 2.7±0.3 2.6±0. 1 2.6±0.2
LVEF (%) 81 .5±1 . 12 49.4±2.7** 47.5±4.4** 49.4±2.9** 78.1±3.2 36. 1±5.1 •• § 45.4±4.5** 48.0±3.7**
%F'S 45.5±1.7 22. 1±1 .5•• 2 1 .4±2.4** 22. 1±1 .5** 43.0 ±3.l 1 5 .9±2. 7* *§ 20.5±2.4** 2 1 .9±2.4**
Data are presented as mean :I: SEM; N indicates number of animals; bpm, beats per minute. **P<0.0 l and *P<0.05 indicate significant differences compared to sham-operated rats in week 3 and week 12 respectively; § P <0.05 indicates significant difference between parameters at week 12 and week 3 using Paired-Sample T-Test. IVSd and IVSs, the thickness of the interventricular septum in diastole and systole; LVIDd and LVIDs, diastolic and systolic left ventricle dimensions; L VPWd and L VPWs, the thickness ofleft ventricle posterior wall in diastole and systole.
< Ill
g: &. <E. �
... . (I) -a <
s· a r:t a. (I) Ill I:""' §' (I) � a t, Q. ""l:i s.: l")
0 i:I a s '"I "O (I) � c:,, (I) E.. Q. .... s· � tlJ �-
.... 1:1"' �- c:,,
=ri g-£ s a .... 0
.g l '"I Ill � fti" (I) Q.
'"I (I)
�� a
� � g: e: (I) er w
.._, (I)
'< Ill
Q.
a (I)
n
.[ � .i:,.
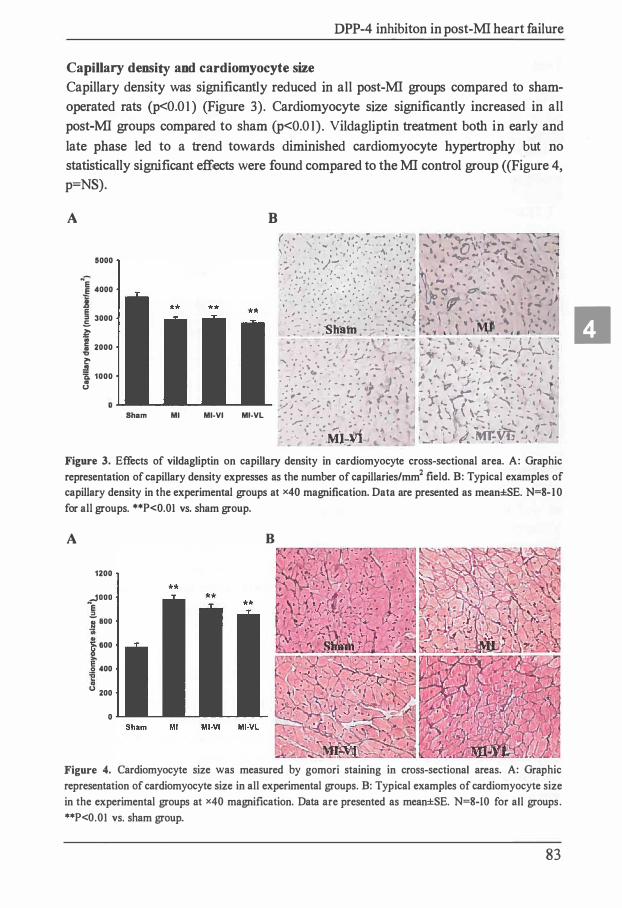
DPP-4 inhibiton in post-MI heart failure
Capillary density and cardiomyocyte size Capillary density was significantly reduced in all post-MI groups compared to shamoperated rats (p<0.01) (Figure 3). Cardiomyocyte size significantly increased in all post-Ml groups compared to sham (p<0.01). Vildagliptin treatment both in early and late phase led to a trend towards diminished cardiomyocyte hypertrophy but no statistically significant effects were found compared to the MI control group ((Figure 4, p=NS).
A
5000
N� 4000
l 3000
� i 2000 � .!l 'a, 1000 .. tJ
B
Sham Ml Ml-VI MI-VL
(., ........ ' ' . .. �, ... -. • ,:;:-. 7 --- , .. ·:.. , , ,..' · q.."1 .l " .. -
,, , ,. -.,· \ , ...... . . , . .,\ •, , f. "' 0\1_, f,'f.e ·--- _ \ I \ , ' . ' > •• • , : ! -, · , - :·, ..... · . ,� .. •. · •· .. ' ' .. ' . .. .. :...=-.. .. '�. �J • . , ... .. -, .- ,.r . , ':'-tj- ·,,· .. · . . . ..... , .. . �- � , ., ... ,, :t ... •
, , . , : . • l • •• ..,.. , ... ' • ., • • •, "• --- ' . ... -""'.-=>, ·· ·. �-· .. , . ·, . . · .. · . ·, ·· . . · • .· 1 · : · 1 , . ... • . ' I' t h . .. · , · · · . . . · . · . · .... �- , ,.. _ ,. .. , \ ., .. ., :,· J ,•, •, · t· . ... ... . ... .. = • · , , : • -
1 ..:Q �.- • • , " \ A.,... ,., , , , , I f " - , ' ,... ' • ., � _.
I_ iJ":" � lfll1,, I, • � "' , • /" ' -- • • : • • • • • • •• ' • • -• <" .. . . I/' ' , • - '- \ t , .. ;J , ., .. . • : . .. .., . . . . . .. . · ... · . , 1· . .. • ,·· , · · " • , . , . •• • • • . • • , .,,
.1- · .. ... . ... f.., ·- ·-,;� \4 ' \ .... .. 'il " , .. .. - : . • -Sh" - • . - . •. - - •" -.
• ... \ ' . .. . ; • • _ • • , ftffl �-� -� •. ".: ·,4. � 1- • I ' 1 '
• --; . . . -. ' • • • � , .: l\. . 'ii ./: • • ! �-i ..... ,� . .. . ... • .. -.� .t J:�'�· , ' :- , -, .. / ' ; .. -
... � t";.-l � � ��
• ' ' :•.\ • .'. • ,_ . J • ,:. "(_ ' I ;'I : :;-:� f"; • . : , < •, ', I • -:- - ; •• , . .. ., • , · ., t. ,b "
.i\. i •-<_ ,,Jr , .... •," to , . " • • • • - - • - -•¼, • } , • • );,,, _) ' . . ..... ,
-: �·- ··. · .. - r_
.'J -::. ... i. - ,
. -� : . ·; '. :
,, , ,'\
....._ : . .. . . :- " . · · ,. I\ , c-r"- h•· • .- -...:..� - . 4 , • / I ,.;' • • I , • t i ' · "' - '\. • "" .1 - � • • ' ' ' • < 9 • "\,, \ \ \.- '1 . - . •
... ,,; :: .:• : ; ;: ': :- ' . " .. • -.. ,
:,' C , · ·, :1..�--. � ;-�
J , ,._ '• " "'"' ,-r• .r...L � I- I
" • \ · � ... ; ;_� .;:-� ,> .f
· _ ·· :·_· .MJ;:.¥1-.. , ,_.,. 1 #..-m•:-YtJ. --:, , · J .
Figure 3. Effects of vildagliptin on capillary density in cardiomyocyte cross-sectional area. A: Graphic representation of capillary density expresses as the number of capillaries/mm2 field. B: Typical examples of capillary density in the experimental groups at x40 magnification. Data are presented as mean±SE. N=S-10 for all groups. **P<0.01 vs. sham group.
A B
1200
..JOOO "e "ij' aoo
f 600
� 400
u 200
0
Figure 4. Cardiomyocyte size was measured by gomori staining in cross-sectional areas. A: Graphic representation of cardiomyocyte size in all experimental groups. B: Typical examples of cardiomyocyte size in the experimental groups at x40 magnification. Data are presented as mean±SE. N=S-10 for all groups. **P<0.01 vs. sham group.
83
II

Chapter 4
Table 3 Hemodynamic parameters of the experimental groups at sacrifice (12 weeks).
Sham MI MI-VI MI-VL
N=8 N=lO N=9 N=9
Heart rate (bpm) 346±16 378±7 350±9 361±12
LVESP (mmHg) 117±4 1 09±3 1 08±3 109±4
LVEDP (mmHg) 6.2±0.8 9.6±1.6* 9.8±1 .3* 7.4±0.5
SBP (mmHg) 1 15±3 1 11±2 1 1 0±3 113±3
DBP (mmHg) 87±2 86±2 85±2 84±2
dPdtmax (mmHg/s) 8744±435 7245±436 6908±396 7952±484
dPdtmin (mmHg/s) -9363±268 -6419±466* -6592±613* -7077±380*
Data are presented as mean ± SEM; N indicates number of animals; LVESP, left ventricular end-systolic pressure; LVEDP, left ventricular end-diastolic pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure; dP/dtmax and dP/dtmin, the maximal rate of increase and decrease of left ventricular pressure, respectively.*P<0.05 vs. Sham.
Cardiac gene expression
ANP and BNP mRNA levels were significantly increased both in the MI control group
as well in as late vildagliptin treatment group compared to sham group (p<0.05).
Vildagliptin treatment both in early and late phase had no significant effects herein
(Figure SA and 5B). Similar results were found for collagen I expression, which was
significantly increased in the MI group compared to sham, while no difference was
observed in collagen I expression between vildagliptin-treated groups and the control
MI group (Figure SC). MMP-9 mRNA levels were similar in all groups (Figure 5D).
Discussion
In the present study, we demonstrate that long-term treatment of the DPP-4 inhibitor
vildagliptin in rats with L V remodeling due to MI increases endogenous active plasma
GLP-1 levels, via inhibition of DPP-4 activity. However, this did not result in a
decreased infarct size nor did it attenuate cardiac remodeling associated with post-MI.
No differences in glucose levels and body weight were found in these non-diabetic rats
when treated with vildagliptin.
84

DPP-4 inhibiton in post-MI heart failure
A B 18 14 * * 1 6
12 * 14
1 12
c( 1 0
_ 1 0
.! 8 z z a: 8 E
a:
6 z 4
4
2 2
0 0
C Sham Ml Ml-VI MI-VL
D Sham Ml Ml-VI MI-VL
1 2 6 *
1 0 5 1 .! 8 c( 1 4 z a: E 6
ni 4
z � 3
� 2
2
0 0 Sham Ml Ml-VI MI-VL Sham Ml Ml-VI MI-VL
Figure 5. Quantitative real-time reverse-transcriptase polymerase chain reaction (RT-PCR) was conducted
and expression was measured of myocardial atrial natriuretic peptide (ANP; A), brain natriuretic peptide
(BNP; B), collagen I (C), and MMP-9 (D), respectively (mRNA corrected for 3684 mRNA level). The
relative corrected values are shown for each group. Data are presented as mean±SE. N=8-I O for all
groups. *P<0.05 vs. sham group.
To our knowledge, this is the first study to assess the effects of immediate and late vildagliptin treatment in a non-diabetic rat model. We furthermore aimed to dissect immediate versus late effects of DPP-4 inhibition. We herein show that neither early nor late vildagliptin treatments exert beneficial effects in MI-induced deterioration in cardiac remodeling. Notably, Ml size was (non-significantly) smaller in the vildagliptin treated rats. However, this effect was observed both in rats immediately treated with vildagliptin as well as in rats in which treatment with vildagliptin started after 3 weeks, so when the infarction scar is fully organized. From this, we postulate that vildagliptin is unlikely to reduce infarct size. The associated differences in L VEF may be ascribed to the differences in infarct size. Other measures of L V remodeling were also unaffected by vildagliptin. For example, both early and late vildagliptin treatment did
85
II

Chapter 4
not reverse the Ml-induced decrease in capillary density, measured at the border zone of the infarcted myocardium. Similarly, both early and late vildagliptin treatment did not counteract Ml-induced cardiomyocyte hypertrophy. Furthermore, both early and late vildagliptin treatment had no effects on the Ml-induced increases in cardiac expression of ANP, BNP. ANP and BNP cardiac gene expression closely associates with the severity of L V dysfunction 23
, so this finding supports the notion that cardiac remodeling is not affected by vildagliptin. Furthermore, the expression of matricellular proteins collagen I and MMP-9 were also not affected by vildagliptin treatment.
A number of acute studies have been previously performed with DPP-4 inhibitors, GLP-1 or GLP-1 analogues, addressing their role in cardioprotection. A study with the DPP-4 inhibitor PFK275-055, a vildagliptin-analogue, showed a reduced infarct size with activation of the cardioprotective RISK (reperfusion-induccd salvage kinase) pathway in pre-diabetic rats 24, whereas a study with the DPP-4 inhibitor sitagliptin showed that infarct size or short-term cardiac function were not affected by the treatment 25• The latter study is in line with our study.
Another mean of increasing GLP- 1 is direct GLP- I infusion. Acute GLP- 1 infusion studies both in patients and rodents did show beneficial effects. In a clinical study, 3-day infusion of GLP-1 improved LV function in patients after acute MI 14•
Moreover, ischernia/reperfusion experiments in rats showed that GLP-1 administration prior to the ischemia leads to smaller infarct size in the isolated heart 1 1 • 1 2• 26• Another ischemia-reperfusion study showed that only the GLP- 1 analogue exendin-4, but not GLP-1(9-36) amide exerts infarct-limiting action, while both of them improved LV performance 27• Apparently, GLP-1 infusion provides a stronger effect than DPP-4 inhibition, probably due to a stronger elevation of GLP-1 levels. The published results from DPP-4 inhibition studies arc variable and this might be explained by different levels of inhibition (different inhibitors used, different dosages), and variable levels of GLP-1.
So, although a number of acute studies have been performed, only few chronic
studies have addressed the effects of GLP- 1 on cardiac function in non-diabetic models. A chronic (3 month) infusion study showed that GLP-1 improved LV systolic function and prolonged sw-vival in spontaneously hypertensive rats by increasing myocardial glucose uptake and reducing myocyte apoptosis 28
• Treatment with either GLP-1 or excnatidc analogue AC3 l 74 also demonstrated promising cardioprotective effects, including improved L VEF, LV end-diastolic pressure, and cardiac dimensions in a rat MI model (comparable to the present model) 29• Our results arc not in concert with the observations that cardioprotection is achieved by GLP-1 treatment. The reasons for the discrepancies between the present study and earlier work may be attributable to the dosing regimen, the different analogue utilized, the levels of GLP-1 achieved, and the timing of the treatment and the species studied 30•
86

DPP-4 inhibiton in post-Ml heart failure
Furthermore, a number of other issues should be considered when discussing the lack of vildagliptin-induced cardioprotection as observed in our study. First, we used a model of non-diabetic rats, with normal glucose levels. Vildagliptin is an antidiabetic agent which exerts its beneficial effects in the cardiovascular system through glycometabolic control. Thus it may be possible that vildagliptin is more beneficial in diabetic models. Second, as a DPP-4 inhibitor, vildagliptin inhibits degradation of GLP- 1 and prolongs its half life in vivo; however, its effects are less strong than continuous GLP- 1 infusion. The elevations in GLP-1 levels achieved by vildagliptin are likely to be lower than achieved by GLP- 1 infusion and thus insufficient to produce cardioprotection. Finally, we do not know if other, hitherto unknown mechanisms, may underpin the effects of vildagliptin in the heart. To date, limited data are available describing the effects of vildagliptin on the cardiovascular system.
In addition, the biological effects of DPP-4 inhibitors appear different from GLP-1 and other GLP- l R agonists 3 1 • Vildagliptin treatment has no effect on body � weight, food intake, energy expenditure and insulin sensitivity 4
• 32• 33. Although it has I.I
been shown that vildagliptin reduced plasma cholesterol and triglycerides in diabetic patients 34
• 35, no effects of vildagliptin on these parameters were found in our post-MI
animal study. However, GLP-1 inhibits glucagon secretion and controls body weight by decreasing food intake, increase insulin sensitivity and improve glucose uptake, which are beneficial cardiovascular factors 36
"38. Moreover, the protective effects of
GLP-1 are also mediated through GLP- lR-independent pathways, partially though beneficial effects of its metabolite GLP-1 (9-36) 39. These differences might explain why we observed only limited improvements in our study with vildagliptin as compared to other studies with GLP-1 and GLP-1 analogues.
Limitations Possibly, the dosage of vildagliptin was not sufficient to observe a cardioprotective effect of vildagliptin. We did not include a group treated with GLP- 1 infusion so we cannot compare DPP-4 inhibition to GLP-1. Furthermore, although plasma glucose was comparable in all groups, we did not assess factors associated with myocardial glucose metabolism, so that we cannot rule out if direct metabolic effects explain the results.
Conclusions Long-term treatment with the DPP-4 inhibitor vildagliptin, started immediate or late after MI, does not preserve cardiac function in a rat post-MI remodeling model of chronic heart failure despite increases in plasma active GLP-1 levels by inhibiting DPP-4 activity.
87
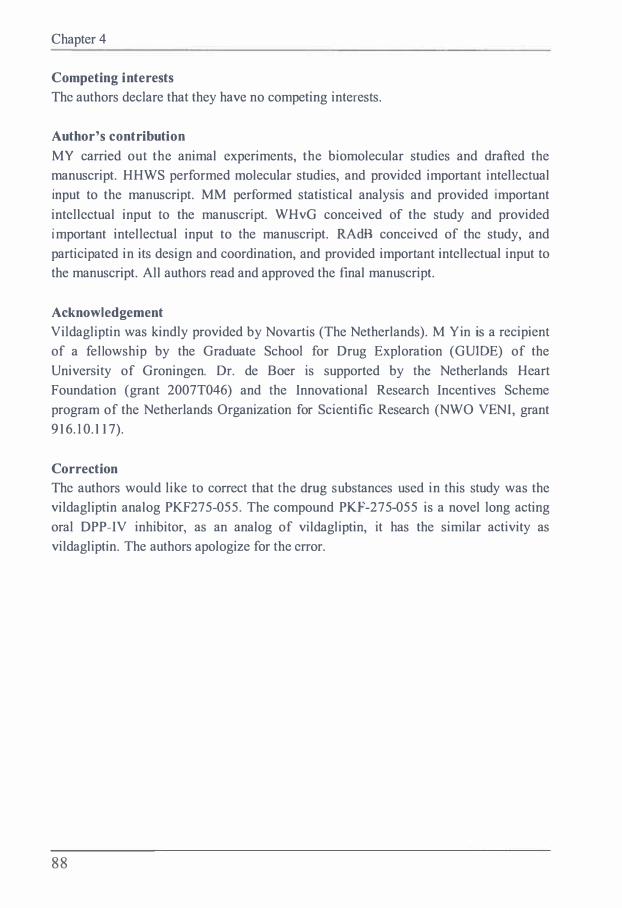
Chapter 4
Competing interests The authors declare that they have no competing interests.
Author's contribution MY carried out the animal experiments, the biomolecular studies and drafted the manuscript. HHWS performed molecular studies, and provided important intellectual input to the manuscript. MM performed statistical analysis and provided important intellectual input to the manuscript. WHvG conceived of the study and provided important intellectual input to the manuscript. RAdB conceived of the study, and participated in its design and coordination, and provided important intellectual input to the manuscript. All authors read and approved the final manuscript.
Acknowledgement Vildagliptin was kindly provided by Novartis (The Netherlands). M Yin is a recipient of a fellowship by the Graduate School for Drug Exploration (GUIDE) of the University of Groningen. Dr. de Boer is supported by the Netherlands Heart Foundation (grant 2007T046) and the Innovational Research Incentives Scheme program of the Netherlands Organization for Scientific Research (NWO VENI, grant 916. 1 0.117).
Correction The authors would like to correct that the drug substances used in this study was the vildagliptin analog PKF275-055. The compound PKF-275-055 is a novel long acting oral OPP-IV inhibitor, as an analog of vildagliptin, it has the similar activity as vildagliptin. The authors apologize for the error.
88

DPP-4 inhibiton in post-MI heart failure
References
I . Nauck MA, Kleine N, Orskov C, Holst JJ, Willms 8 , Creutzfeldt W. Normalization of fasting hyperglycaemia by exogenous glucagon-like peptide I (7-36 amide) in type 2 (non-insulindependent) diabetic patients. Diabetologia 1 993;36:741 -744.
2. Todd JF, Wilding JP, Edwards CM, Khan FA, Ghatei MA, Bloom SR. Glucagon-like peptide) (GLP- 1 ): a trial of treatment in non-insulin-dependent diabetes mellitus. Eur J Clin Invest I 997;27:533-536.
3. Zander M, Madsbad S, Madsen JL, Holst JJ. Effect of 6-week course of glucagon-like peptide I on glycaemic control, insulin sensitivity, and beta-cell function in type 2 diabetes: a parallel-group study. Lancet 2002;359:824-830.
4. Drucker DJ, Nauck MA. The incretin system: glucagon-like peptide- I receptor agonists and dipeptidyl peptidase-4 inhibitors in type 2 diabetes. Lancet 2006;368: 1 696- 1 705.
5. Sokos GG, Nikolaidis LA, Mankad S, Elahi D, Shannon RP. Glucagon-like peptide-I � infusion improves left ventricular ejection fraction and functional status in patients with I.I chronic heart failure. J Card Fail 2006;12:694-699.
6. Bullock BP, Heller RS, Habener JF. Tissue distribution of messenger ribonucleic acid encoding the rat glucagon-like peptide- I receptor. Endocrinology I 996;137:2968-2978.
7. Nystrom T, Gutniak MK, Zhang Q, Zhang F, Holst JJ, Ahren 8, el al. Effects of glucagonlike peptide- I on endothelial function in type 2 diabetes patients with stable coronary artery disease. Am J Physiol Endocrinol Metab 2004;287:E 1 209- 1 5.
8. Oeseburg H, de Boer RA, Buikema H, van der Harst P, van Gilst WI I, Sillje HI I. Glucagonlike peptide I prevents reactive oxygen species-induced endothelial cell senescence through the activation of protein kinase A. Arterioscler Thromb Vase Biol 20 1 0;30: 1 407- 1 4 14.
9. Gros R, You X, Baggio LL, Kabir MG, Sadi AM, Mungrue IN, et al. Cardiac function in mice lacking the glucagon-like peptide-I receptor. Endocrinology 2003;144:2242-2252.
I 0. Nikolaidis LA, Elahi D, I lentosz T, Doverspike A, Huerbin R, Zourelias L. el al. Recombinant glucagon-like peptide- I increases myocardial glucose uptake and improves left ventricular performance in conscious dogs with pacing-induced dilated cardiomyopathy. Circulation 2004;1 1 0:955-96 1 .
1 1 . Bose AK, Mocanu M M, Carr RD, Yellon OM. Glucagon like peptide-I is protective against myocardial ischemia/reperfusion injury when given either as a preconditioning mimetic or at reperfusion in an isolated rat heart model. Cardiovasc Drugs Ther 2005;19:9- I I .
12 . Bose AK, Mocanu MM, Carr RD, Brand CL, Yellon OM. Glucagon-like peptide can directly protect the heart against ischemia/reperfusion injury. Diabetes 2005;54: 146- I 5 1 .
1 3 . Nikolaidis LA, Elahi D , Shen YT, Shannon RP. Active metabolite of GLP-1 mediates myocardial glucose uptake and improves left ventricular performance in conscious dogs with dilated cardiomyopathy. Am J Physiol Hearl Circ Physiol 2005;289:1-12401 -8.
89

Chapter 4
14. Nikolaidis LA, Mankad S, Sokos GG, Miske G, Shah A, Elahi D, et al. Effects of glucagonlikc peptide-I in patients with acute myocardial infarction and left ventricular dysfunction after successful reperfusion. Cin1tlation 2004;1 09:962-965.
1 5. Deacon CF, Pridal L, Klarskov L, Olesen M, Holst JJ. Glucagon-like peptide I undergoes differential tissue-specific metabolism in the anesthetized pig. Am J Physiol 1 996;271 :E458-64.
16. Bergman AJ, Stevens C, Zhou Y, Yi B, Laethem M, De Smet M, et al. Pharmacokinetic and pharmacodynamic properties of multiple oral doses of sitagliptin, a dipcptidyl peptidase-IV inhibitor: a double-blind, randomized, placebo-controlled study in healthy male volunteers. Clin Ther 2006;28:55-72.
1 7. Neumiller JJ, Campbell RK. Saxagliptin: a dipeptidyl peptidase-4 inhibitor for the treatment of type 2 diabetes mellitus. Am J I lea/th Syst Pharm 20 I 0;67: 1 5 1 5-1 525.
1 8. Vcrspohl EJ. Novel therapeutics for type 2 diabetes: incretin hormone mimetics (glucagonlikc peptide- I receptor agonists) and dipeptidyl peptidase-4 inhibitors. Pharmacol Ther 2009;1 24: 1 1 3- 1 38.
1 9. Jin I IY, Liu WJ, Park JI I, Baek I IS, Park TS. Effect of dipeptidyl peptidase-IV (OPP-IV) inhibitor (Vildagliptin) on peripheral nerves in streptozotocin-induced diabetic rats. Arch Med Res 2009;40:536-544.
20. Wang X, Zhang D, Xu W, Liu I I, Wang W. Pharmacokinetics of lipoyl vildagliptin, a novel dipcptidyl peptidase IV inhibitor after oral administration in rats. Xenobiotica 20 1 0;40:707-7 1 2.
2 1 . Yin M , van der I Iorst IC, van Melle JP, Qian C, van Gilst WI I, Sillje I I I I. et al. Metformin improves cardiac function in a non-diabetic rat model of post-MI heart failure. Am J Physiol Heart Circ Physiol 20 1 1 ;.
22. Wcstcnbrink BO, Ruifrok WP, Voors AA, Tilton RG, van Veldhuiscn DJ, Schoemaker RG, et al. Vascular endothelial growth factor is crucial for erythropoietin-induccd improvement of cardiac function in heart failure. Cardiovasc Res 201 0;87:30-39.
23 . de Boer RA, Henning RH, Suurmeijer AJ, Pinto YM, Olthof E, Kirkels JI I, et al. Early expression of natriuretic peptides and SERCA in mild heart failure: association with severity of the disease. Int J Cardiol 200 I ;78:5- 12.
24. I luisamen B, Genis A, Marais E, Lochner A. Pre-treatment with a DPP-4 inhibitor is infarct sparing in hearts from obese, pre-diabetic rats. Cardiovasc Drugs Tuer 201 1 ;25 : 1 3-20.
25. Sauve M, Ban K, Momen MA, Zhou YQ, I Ienkelman RM, I lusain M, et al. Genetic deletion or pharmacological inhibition of dipeptidyl peptidase-4 improves cardiovascular outcomes after myocardial infarction in mice. Diabetes 20 I 0;59: I 063- 1 073.
26. Bose AK, Mocanu MM, Carr RD, Yellon OM. Myocardial ischaemia-reperfusion injury is attenuated by intact glucagon like peptide- I (GLP- 1 ) in the in vitro rat heart and may involve the p70s6K pathway. Cardiovasc Drugs Ther 2007;21 :253-256.
90

27.
28.
29.
30.
3 I .
32.
33.
34.
35.
36.
37.
DPP-4 inhibiton in post-Ml heart failure
Sonne DP, Engstrom T, Treiman M. Protective effects of GLP- 1 analogues exendin-4 and GLP- 1 (9-36) amide against ischemia-reperfusion injury in rat heart. Regul Pept 2008;146:243-249.
Poomima I, Brown SB, Bhashyam S, Parikh P, Bolukoglu 1 1, Shannon RP. Chronic glucagonlike peptide-I infusion sustains left ventricular systolic function and prolongs survival in the spontaneously hypertensive, heart failure-prone rat. Circ Heart Fail 2008;1 : 1 53- 1 60.
Liu Q, Anderson C, Broyde A, Polizzi C, Fernandez R, Baron A, et al. Glucagon-like peptide) and the exenatide analogue AC3 I 74 improve cardiac function, cardiac remodeling, and survival in rats with chronic heart failure. Cardiovasc Diabetol 20 10;9:76.
Anagnostis P, Athyros VG, Adamidou F, Panagiotou A, Kita M, Karagiannis A, et al. Glucagon-like peptide- I -based therapies and cardiovascular disease: looking beyond glycaemic control. Diabetes Obes Metab 20 1 1 ;13:302-3 1 2.
Doupis J, Veves A. DPP4 inhibitors: a new approach in diabetes treatment. Adv Ther II 2008;25:627-643 . •
Flock G, Baggio LL, Longuet C, Drucker DJ. Incretin receptors for glucagon-like peptide I and glucose-dependent insulinotropic polypeptide are essential for the sustained metabolic actions ofvildagliptin in mice. Diabetes 2007;56:3006-30 1 3.
Vella A, Bock G, Giesler PD, Burton DB, Serra DB, Saylan M L, et al. Effects of dipeptidyl peptidase-4 inhibition on gastrointestinal function, meal appearance, and glucose metabolism in type 2 diabetes. Diabetes 2007;56: 1475- 1480.
Matikainen N, Manttari S, Schweizer A, Ulvestad A, Mills D, Dunning BE, et al. Vildagliptin therapy reduces postprandial intestinal triglyceride-rich lipoprotein particles in patients with type 2 diabetes. Diabetologia 2006;49:2049-2057.
Rosenstock J, Baron MA, Dejager S, Mills D, Schweizer A. Comparison of vildagliptin and rosiglitazone monotherapy in patients with type 2 diabetes: a 24-week, double-blind, randomized trial. Diabetes Care 2007;30:2 1 7-223.
Drucker DJ. The biology of incretin hormones. Cell Metab 2006;3: 1 53- 1 65.
Kurukulasuriya LR, Sowers JR. Therapies for type 2 diabetes: lowering HbA l c and associated cardiovascular risk factors. Cardiovasc Diabetol 20 I 0;9:45.
38. Fisman EZ, Tenenbaum A. A cardiologic approach to non-insulin antidiabetic phannacotherapy in patients with heart disease. Cardiovasc Diabetol 2009;8:38.
39. Ban K, Noyan-Ashraf M H, Hoefer J, Bolz SS, Drucker DJ, Husain M. Cardioprotective and vasodilatory actions of glucagon-like peptide I receptor are mediated through both glucagonlike peptide I receptor-dependent and -independent pathways. Circulation 2008;1 1 7:2340-2350.
91


Chapter 5
The effects of the DPP-4 inhibitor vildagliptin
on diabetic cardiomyopathy in Zucker Fatty
Diabetic rats
Meimei Yin 1, Hendrik Buikema 2, Maxi Meissner 1, Wiek H. van Gilst 1, Rudolf A. de
Boer 1
I. Department of Cardiology, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands
2. Department of Clinical Pharmacology, University of Groningen, Groningen, The Netherlands
Vildagliptin in diabetic cardiomyopathy
Abstract
Background - Long-term metabolic syndrome and diabetes mcllitus arc wellestablished risk factors for cardiovascular (CV) disease. A specific CV complication of diabetes is diabetic cardiomyopathy: cardiac remodeling in the absence of coronary heart disease and hypertension. An emerging treatment for this syndrome is the use of glucagon-like peptide- I (GLP- 1 ), a hormone with specific cardioprotcctive effects. However, the use of GLP-1 is limited because it is rapidly degraded by the enzyme dipeptidyl peptidase-4 (DPP-4). Herc we investigated whether DPP-4 inhibition could protect the heart from diabetic cardiomyopathy.
Methods and results - We studied male Zucker Diabetic Fatty (ZDF) rats ( 1 0 weeks of age) and age-matched male Zucker lean (ZL) rats as controls. ZDF rats were randomly allocated to the treatment with drinking water containing DPP-4 inhibitor (vildagliptin, 3 mg/kg/day) or control water, for 15 weeks. ZDF rats had significantly higher plasma glucose levels during compared to ZL, but this was unaffected by DPP-4 inhibitor treatment. Diastolic cardiac function assessed by echocardiography was impaired in ZDF vs. Zucker lean, while systolic function was not affected. This was associated with changes in metabolic profile of the heart: significant reduction in glucose transporter type 4 (GLUT-4), and an increase of pyruvate dchydrogcnase kinase (POK) isozyme 4 and glycogen stores. Furthermore, we observed increased myocardial fibrosis in ZDF rats compared to ZL and DPP-4 treatment reduced fibrosis. This was associated with reversal of collagen I apposition. Furthermore, these changes were associated with an increase of ANP. The functional, morphological and molecular changes were partially amenable to DPP-4 inhibition that attenuated cardiac metabolic and structural remodeling.
Conclusion - ZDF rats with severe diabetes mellitus have impaired diastolic function, associated with collagen formation and impaired myocardial glucose metabolism, suggestive for diabetic cardiomyopathy. DPP-4 inhibition by vildagliptin preserves myocardial diastolic function by reducing cardiac fibrosis and improving myocardial glucose metabolism.
94

Chapter 5
Introduction
Type 2 diabetes mellitus (T2DM) refers to a metabolic disorder that is characterized by high blood glucose due to insulin resistance and relative insulin deficiency 1
•
Cardiovascular (CV) complications are the leading cause of morbidity and mortality in patients with T2DM. The Framingham study showed a higher incidence of heart failure (2.4-fold in men and 5-fold in women) in diabetic patients 2
, and reported that this increased incidence is independent of age, hypertension and coronary artery disease. This suggests that diabetes may also directly cause heart failure - known as diabetic cardiomyopathy 3• Moreover, diabetic patients with established heart failure have worse outcome than non-diabetic patients 4
. However, the pathophysiological link between diabetes and CV disease and heart failure in particular, is still not well understood.
Many studies have shown that human diabetic cardiomyopathy is characterized by diastolic dysfunction with preserved systolic function 5• 6• The early manifestations of left ventricular dysfunction in diabetes present as impaired relaxation and abnormal filling pattern 7
• Diabetic animals have also shown prolongation of relaxation and l!I slowing ofrelaxation velocity 8• 1:1
These observations have been confirmed in animal models of metabolic disease. A longer deceleration time and impaired left ventricular early filling were found in Otsuka Long-Evans Tokushima fatty (OLETF) rats 9
, which are consistent with findings in human type 2 diabetic patients w_ Additionally, an increased late mitral inflow velocity and increased left ventricular end-diastolic pressure was demonstrated in isolated and perfused diabetic rat hearts 1 1
•
The Zucker Diabetic Fatty (ZDF) rats which have a mutation at the leptin receptor gene were used to study more precisely the cardiovascular changes and mechanisms in metabolic syndrome 1 2
• This model shows the clinical features of the metabolic syndrome like hyperglycemia, hyperinsulinemia and hyperlipidemia 1 3• This animal model has been used to study the metabolic syndrome and T2DM.
However, only a limited number of studies have looked into mechanisms responsible for the abnormal diastolic function. In a clinical study, diabetic patients showed cardiomyocyte hypertrophy and myocardial interstitial fibrosis 14, consistent with myocardial alterations in experimental animals 1 5
• These findings suggest that cardiac hypertrophy and fibrosis are important contributors to the diastolic dysfunction. In addition, altered myocardial substrate metabolism reflected in increased Iipolysis, impaired myocardial glucose uptake and utilization, and increased FA oxidation also contribute to high LV stiffness 16
•
95

Vildagliptin in diabetic cardiomyopathy
In our study we targeted the degradation of DPP-4 by administering vildagliptin, a DPP-4 inhibitor, to ZDF rats. We first characterized the cardiac phenotype of the ZDF rat to gain a better understanding of myocardial maladaptations in diabetic cardiomyopathy and second we tested the effect of the DPP4-inhibitor vildagliptin herein.
Materials and Methods
Animals and experimental protocol. All experimental protocols were approved by the Animal Ethical Committee of the University of Groningen for the use of experimental animals and conform to the Guide for Care and Use of Laboratory Animals. Male Zucker Diabetic Fatty (ZDF) rats (10 weeks of age) and age-matched male Zucker lean (ZL) littermates were obtained from Genetic Models (Indianapolis, IN). Animals were kept in the Animal Care Center at the University ofGroningen under controlled conditions (23±1°C; 12:12-h light-dark cycle) and received Formula Diet 5008 (protein 26.8%, carbohydrate 56.4%, (91% starch, 9% simples carbohydrates), PMI Feeds, Richmond, IN)). ZDF rats were randomly allocated to treatment with the DPP-4 inhibitor vildagliptin, dissolved in drinking water, or normal drinking water, for a period of I 5 weeks. Body weight and blood samples were obtained under anesthesia (2.5% isoflurane in room air enriched with I .0 L/min oxygen) at the start of treatment (10 weeks of age) and at the end of treatment (25 weeks of age). During week 25, cardiac function was determined by echocardiography. After I 5 weeks of treatment, rats were anesthetized and hemodynamic function was measured invasively; thereafter blood was drawn ( either anti coagulated with EDT A, or left to clot for serum) and the hearts were rapidly excised. Myocardial tissue was transected transversally and processed for histochemistry or snap frozen for PCR and western blot analysis. Aorta was harvested for vascular assessment, as recently published 1 7•
Drug: The DPP4 inhibitor vildagliptin (Galvus®, Novartis Pharma AG, Basel, Switzerland) was purchased from the pharmacy in the University Medical Center Groningen. Vildagliptin was dissolved in the drinking water and administered in a final concentration of 3mg/kg/day.
Biomolecular assays. Arterial blood was collected in EDTA-coated tubes (plasma) or blank tubes (serum) and centrifuged at 3000 rpm for 15 min at 4 °C. Thereafter, the plasma/serum was divided into different tubes, snap-frozen in liquid nitrogen and stored for future
96
Chapter 5
analysis of plasma glucose, lactate, HbAIC, serum insulin, active GLP-1 and TGFP-1. Insulin levels were measured at 15 weeks after treatment using an ELISA kit (Rat/Mouse insulin 96-well plate assay, Millipore, MA, U.S.A.).
Insulin resistance assessment by homeostasis model assessment (HOMA-IR) HOMA-IR was calculated using the following formula: HOMA index = [fasting insulin (mU/mL) xfasting glucose (mmol/L)]/22.5, a value >2.5 is considered to be insulin resistance. HOMA-IR has a close correlation with the insulin sensitivity index by the standard euglycemic hyperinsulinemic clamp, as shown by Matthews et al 1 8•
Echocardiography. Echocardiographic measurements were performed by one researcher who was blinded to the treatment groups (RADB). Rats were anaesthetized with 2.5 % isoflurane in a gas mixture of N2O/O2• The M-mode and 2D echocardiography images were obtained with a high-resolution system (Vivid 7, GE, Healthcare, Diegem, Belgium), using a IO MHz transducer. LV dimensions (LVIDd, LVIDs), measurements of the thickness of the interventricular septum (IVSs, IVSd) and posterior wall (LVPWs, LVPWd) were recorded. LV fractional shortening (FS %) was calculated as FS = [(LVIDdL VIDs )/L VIDd] x 1 00%. Diastolic function was assessed recording inflow pattern of the left atrium (E, A, E/A ratio, deceleration time), and by measuring tissue velocity imaging (TVI) in the apical 4 chamber recording; septa! and lateral E were recorded and the average TVI value are presented in cm/s.
Hemodynamic measurements. Before sacrifice, rats were anesthetized and invasive hemodynamics was measured as described 1 9• Briefly, a microtip catheter with pressure transducer (2 Fr, Millar Instr. Inc, Houston, TX, USA) was inserted into the right carotid artery and advanced into the left ventricular cavity. After five minutes stabilization, the heart rate (HR), left ventricular end-systolic pressure (LVESP), end-diastolic pressures (LVEDP) and developed left ventricular pressure ( dL VP=LVESP-L VEDP) were recorded. The parameters of the maximal rates of increase and decrease in developed L V pressures ( dP/dtmax and dP/dtmin) were determined. Corrected dP/dtmax and dP/dtmin, the maximal rate of increase and decrease of left ventricular pressure divided by systolic blood pressure, respectively.
Tissue procurement; Masson and Sirius red staining for fibrosis. After sacrifice, hearts were rapidly excised and arrested in diastole in 2M ice-cold KC!. The right ventricle and atria were removed. The basal and apical parts of the L V were snap-frozen in liquid nitrogen. A mid-papillary slice of the LV was fixed in 4%
97
E

Vildagliptin in diabetic cardiomyopathy
paraformaldehyde overnight and paraffin-embedded. The deparaffinized 3 µm sections were stained with picrosirius red/fast green, as described previously 20• The collagen volume fraction was examined in sections of the left ventricular free wall excluding vessels. Tissue sections were stained with Masson's trichrome stain to evaluate the extent of perivascular fibrosis, modified from previously described methods 2 1 • The area of stained tissue was calculated as a percentage of the total area within a field by using image scope software.
Realtime PCR.
Total RNA from heart tissue was extracted with TRizol reagent (Invitrogen Corp., Carlsbad, CA, USA) and RNA concentrations were measured with a nano-drop device. First-strand cDNA was prepared using a random primer mix and thereafter used as a template for quantitative real-time reverse-transcriptase PCR (qRT PCR) (25 ng/reaction). mRNA levels are expressed in relative units based on a standard curve obtained by a calibrator cDNA mixture. All measured mRNA expression levels were corrected for 36B4 reference gene expression.
Western blot.
Myocardial tissue samples (75 mg), taken from the LV, were homogenized in 1 ml RIPA buffer (50 mM Tris pH 8.0, 1% nonidet P40, 0.5% deoxycholate, 0.1% SOS, 150 mM NaCl) containing phosphatase inhibitor cocktail 1 (Sigma), protease inhibitor (ROCHE) and I mM phenylmethylsulfonyl fluoride (PMSF). Protein concentrations were quantified with the DC protein assay (Bio-Rad Laboratories, Veenendaal, the Netherlands) with bovine albumin as a standard. Equal amounts of protein were loaded onto polyacrylamide-SDS gels and after electrophoresis, proteins were transferred to a PVDF membrane. The membrane was blocked I h with 5% non-fat milk in PBST and probed with primary antibodies overnight at 4°C. The following primary antibodies were used: AMPKa (1:1000, Cell Signaling Technology); Phospho-AMPKa Thr172 ( I :500, Cell Signaling Technology); p-Akt (I : I 000, Cell Signaling Technology); Phospho-GSK-3 (I: 1000, Cell Signaling Technology); Phospho-PKA (I : 1000, Cell Signaling Technology); Phospho-p38 ( I : 1000, Cell Signaling Technology); p38 (1:1000, Cell Signaling Technology); MMP-9 (1 :1000, Abeam), collagen I ( 1 :1000, Abeam), TGFP-1 ( 1 : 1000, Abeam), Phospho-smad2/3 ( 1: 1000, Cell Signaling Technology); eNOS (1:1000, Cell Signaling Technology); GLUT4 (1:1000, Cell Signaling Technology); and GAPDH (I :20,000, Fitzgerald Industries International, Acton, Mass). Immunoblots were next processed with secondary antibodies for 1 hr at room temperature followed by ECL detection.
98

Chapter 5
Data analysis. All data are presented as means ± s.e.m. Differences between groups were analyzed using one-way analysis of variance (ANOV A) follow by 2-sided Dunnett t-test as a post-hoc test, taking the ZDF group as a comparator. Differences were considered statistically significant if p<0.05.
Results
Biometric parameters, parameters of glucose metabolism No significant differences in body weight, heart weight, LV weight, LV weight and body weight ratio were found at the end of treatment period among all groups (Table 1).
Plasma glucose levels and �nsulin levels were measured at baseline and 15 weeks after vildagliptin treatment. At both time points, plasma glucose levels were significantly increased in ZDF rats compared to ZL rats, and no effects of DPP-4 inhibition with vildagliptin were observed. We also observed hyperinsulinernia in treated and untreated ZDF rats compared to ZL rats at baseline; treatment with vildagliptin normalized plasma insulin levels in ZDF rats to levels comparable to those of ZL rats after 15 weeks of treatment. (Table I ).
Plasma NEFA levels were reduced 40% in vildagliptin treated ZDF rats compared to untreated ZDF rats, although still 2-fold higher compared to ZL rats. Additionally, ZDF rats displayed significantly reduced plasma lactate levels compared to ZL rats while the plasma lactate levels appeared normal in the vildagliptin treated rats. In addition, glycogen content was significantly increased in ZDF rats, while a significant decrease of the myocardial glycogen content was found in the vildagliptin group (Table I).
DPP-4 inhibition improved parameters of myocardial glucose metabolism in ZDF rats Next we assessed several parameters of myocardial glucose metabolism. First, we found that myocardial glycogen content was substantially increased, by 4-fold, in the untreated ZDF rats compared to ZL rats (Figure IA). The increase in myocardial glycogen content in untreated ZDF rats was associated with a significant reduction of phosphorylated (p-) GSK-3 and GLUT4 protein expression (Figures 1B and C) and also GLUT 4 mRNA levels (Figure ID). Vildagliptin-treated ZDF rats had a significantly reduced myocardial glycogen content compared to untreated ZDF rats (Figure IA), and restored expression levels of myocardial p-GSK-3 and GLUT4 (Figures IB and C), however no effect was found on myocardial GLUT 4 mRNA levels (Figure ID). Lastly, we observed that untreated ZDF rats displayed significantly
99

Vildagliptin in diabetic cardiomyopathy
higher myocardial mRNA levels of pyruvate dehydrogenase kinase isozyme 4 (PDK4) compared to ZL rats (Figure l E), which was partially reversed upon vildagliptin treatment. No differences were found in protein levels of p-AMPK, p-Akt and eNOS between all groups (Figure IF). Altogether, these data indicate that diabetes in ZDF rats is associated with distinct alterations in myocardial glucose metabolism and homeostasis in ZDF rats, and that DPP4-inhibition by vildagliptin largely reverses these changes.
Table 1 General parameters
Zucker+Lean ZDF ZDF+VIL N=7 N=7 N=7
BW (15 week) (g) 387± 1 1 410± 19 409±8
HW (g) 1.31±0.12 1.14±0.02 1. 1 8±0.04
LVW (g) 0.92±0.09 0.82±0.01 0.86±0.03
LVW/BW 2.36±0.18 2.00±0.07 2.12±0.08
Glucose (15 weeks) 9.6±0.4 23.9± 1 .7 ** 21.5±2.4 ** (mmol/L) Insulin (15 weeks) 0.28±0.04 0.28±0.05 0.34±0.04 (mmol/L) HbAcl (15 weeks) 3.57±0.04 9.54±0. 1 6 ** 9.00±0.20 **
HOMA index 0.69±0.07 8.72±1.80** 10.10±1.93** (Baseline) HOMA index 0.85±0.14 2.18±0.50* 2.28±0.41 * (15 weeks) NEFA (mmol/L) 143.3±29.4 494.4±72 * 308.6±55.9
Lactate (mmol/L) 2.17±0.25 l .43±0.09 2.3 1±0.35 #
Ketone bodies 0.77±0.14 1.07±0.15 0.82±0.10 (mmol/L)
Data are presented as means ± SEM; N indicates number of animals; BW, body weight; I IW: heart weight; LVW, left ventricle weight; LVW/BW, left ventricle weight / body weight ratio; HOMA index: Homeostasis Model Assessment. **P<0.0 1 vs. Zucker lean.*P<0.05 vs. ZDF lean. # P<0.05 ZDF vildagliptin vs ZDF.
1 00

Chapter 5
A
12 * '[ 10
8
6
4
a 2
0 ZL ZOF ZDF+VIL
D
1,6
� 1,2
i 0,6 *
3 0,4
0,0 ZL ZDF ZDF+VIL
GSK-313 -
ZDF ZDF+VIL
GAPDH ---------
#
*
ZL ZDF ZDF+VIL
E
1,6 *
! 1,2
� 0,8
� 0,4
0,0 ZL ZDF ZDF+VIL
C ZL ZOF ZDF+VIL
GLUT4 GAPDH----------
#
*
ZL ZDF ZDF+VIL
F
ZL ZDF ZDF+VIL
p-AMPK- - -
p-Akt
eNOS ·-- - . -GAPDH
Figure 1 Effects of vildagliptin on myocardial glucose metaboli m following 1 5 weeks treatment. A, Myocardial glucogen content. B and C, lmmunoblot analysis of Glycogen synthase kinase (GSK)-3�
phosphorylation and glucose transporter type 4 (GLUT4) protein expressions. Levels of protein were quantified by densitometry and normalized against GAPDH as a loading control. D and E, GLUT4 and pyruvate dehydrogenase kinase isozyme 4 (PDK4) mRNA expression. Data are presented as fold change. E, Representative immunoblots of 5' adenosine monophosphate-activated protein kinase (AMPK)
phosphorylation, Protein Kinase B (Akt) phosphorylation and endothelial nitric oxide synthase (eNOS) protein expressions. Values are means ± s.e.m. N 7, *P<0.05 vs. sham group; #P<0.05 vs. M l group.
Diabetes, DPP-4 inhibition by vildagliptin, and diastolic function.
To more precisely investigate the myocardial alterations of diabetic cardiomyopathy and the effect of vildagliptin treatment herein, we then extensively assessed parameters of cardiac function. First, we observed abnormal filling velocities in untreated ZDF rats, as their early filling velocity (E) was significantly reduced compared to ZL rats (Figure 2A). No differences between all groups were observed in the atrial filling phase (A) (Figure 2B). As a result, the early to late diastolic inflow velocity ratio (E/A ratio) was decreased (Figure 2C) in untreated ZDF rats compared to ZL rats. Vildagliptin treatment led to a trend to preservation of diastolic function (E, E/A ratio). We additionally show that the tissue velocity was significantly reduced in untreated ZDF compared to ZL rats. This reduction was non-significantly reversed by vildagliptin treatment (Figure 2D). Altogether, these parameters suggest an early manifestation of abnormal L V diastolic function. Contrary, systolic function was preserved in ZDF rats, as left ventricular fractional shortening was similar in all groups (Figure 2E).
101
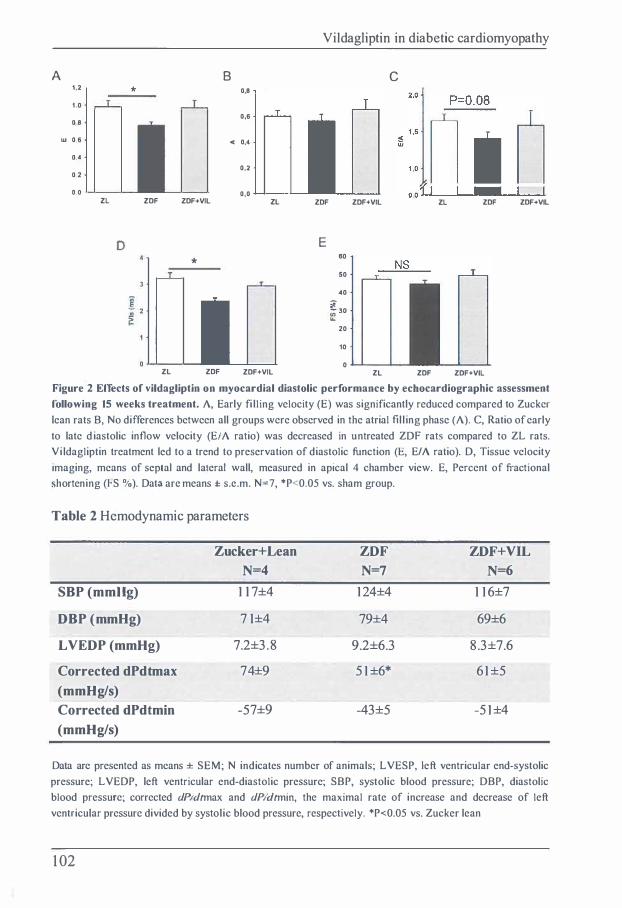
Vildagliptin in diabetic cardiomyopathy
A 8 C 1,2 * 0,8
1,0
0 8 0,6
w 0,6 C 0,4
0.4
0,2 0,2
o.o 0,0 ZL ZDF ZDF+VIL ZL ZDF ZDF+VIL ZL ZDF ZDF+VIL
D E
* 60
50
40
l 30
20
10
0 ZL ZDF ZDF+VIL ZL ZDF ZDF+VIL
Figure 2 Effects of vildagliptin on myocardial diastolic performance by echocardiographic assessment following 15 weeks treatment. A, Early fi lling velocity (E) was significantly reduced compared to Zucker lean rats B, No differences between all groups were observed in the atrial filling phase (A). C, Ratio of early to late d iastolic inflow velocity (E/A ratio) was decreased in untreated ZDF rats compared to ZL rats. Vi ldagliptin treatment led to a trend to preservation of diastolic function (E, E/A ratio). D, Tissue velocity imaging, means of septa! and lalcral wall, measured in apical 4 chamber view. E, Percent of fractional shortening (FS %). Data arc means ± s.c.m. N=7, *P<0.05 vs. sham group.
Table 2 Hcmodynamic parameters
Zucker+Lean ZDF ZDF+VIL N=4 N=7 N=6
SBP (mmHg) 117±4 124±4 116±7
DBP (mmHg) 71±4 79±4 69±6
LVEDP (mmHg) 7.2±3.8 9.2±6.3 8.3±7.6
Corrected dPdtmax 74±9 51±6* 61±5 (mmHg/s) Corrected dPdtmin -57±9 -43±5 -51±4 (mmHg/s)
Data arc presented as means ± SEM; N indicates number of animals; LVESP, left ventricular end-systolic pressure; LVEDP, left ventricular end-diastolic pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure; corrected dP/dtmax and dP/dtmin, the maximal rate of increase and decrease of left ventricular pressure divided by systolic blood pressure, respectively. *P<0.05 vs. Zucker lean
1 02

Chapter 5
Next we evaluated hemodynamic outcomes in ZDF rats treated or not treated
with vildagliptin. Untreated ZDF rats had worse hemodynamic outcome compared with
Zucker lean rats as demonstrated by a slightly elevated left ventricular end diastolic
pressure and worse maximal rates of increase and decrease of left ventricular pressure
( dP/dtmax and clP/dtmin) were both worse in ZDF rats compared to Zucker lean rats
(Table 2). Vildagliptin treatment appeared to have no benefit in any of the
hemodynamic parameters (Table 2).
A
Masson staining:
perivascular fibrosis
Sirius Red/Fast Green:
interstitial fibrosis
Polarized Light: interstitial fibrosis
B 0,6
0,4
� 0,2
0,0
ZL
*
ZL ZDF
ZDF ZDF+VIL
C 7
l 6 *
.. 5 #
4 i! # jij 3 � �
2
ZDF+VIL ZL ZDF ZDF+VIL
Figure 3 Effects ofvildagliptin on myocardial fibrosis following 15 weeks treatment. A. Representative
photographs ofperivascular fibrosis indicated by Masson's trichrome staining (upper panel) and interstitial
fibrosis indicated by Sirius red/fast green staining (middle panel). The lower panel shows polarized light
photographs of interstitial fibrosis. B and C, Bar graphs to indicate the ratio of perivascular fibrosis to the
whole vessel area and the volume of interstitial fibrosis. Data are means ± s.e.m. N=7, *P<0.05 vs. sham
group; #P<0.05 vs. MI group.
103

Vilclagliptin in diabetic cardiomyopathy
DPP-4 inhibition decreases myocardial fibrosis in ZDF rats
Next, we evaluated alterations in cardiac morphology and the effect of vilclagliptin
treatment. Myocardial fibrosis and collagen deposition constitute the initial structure
changes in diabetic hearts 22• Masson's trichrome staining and picrosirius red fast green
staining both showed increased myocardial fibrosis in untreated ZDF rats (Figure 3A).
DDP-4 treatment reduced both interstitial and perivascular fibrosis, by 50% and 30%
respectively, compared to untreated ZDF rats (Figures 3B and 3C), reaching levels
similar to ZL rats.
A
MMP-9
GAPDH
C
TGF(3-1 GAPDH
4
3
0
0,3
i 0,2 e a. -g! 0,1
0,0
ZL ZDF ZDF+VIL
* *
ZL ZDF ZDF+VIL
ZL ZDF ZDF+VIL -...,..._,,_�
ZL ZDF ZDF+VIL
B
Collagen I
GAPDH
6
5
0
p-smad2/3 GAPDH
2,0
1 ,6
ij 1 ,2 .. E
'&_ 0,8
0,4
0,0
ZL ZDF ZDF+VIL
*
#
ZL ZDF ZDF+VIL
ZL ZDF ZDF+VIL
,__,_-.._..._....,_._
ZL ZDF ZDF+VIL
Figure 4 Effects of vildagliptin on myocardial fibrosis protein expressions following IS weeks treatment. Representative immunoblots and bar graphs to indicate the changes of protein matrix metallopeptidase 9 (MMP-9, A), collagen-I (B), Transforming growth factor beta 1 (TGF�-1, C) and phosphorylation of smad2/3 (D). Data are means ± s.e.m. N=7, *P<0.05 vs. sham group; #P<0.05 vs. MI group.
To further understand the antifibrotic effects of vilclagliptin treatment we then
analyzed the mRNA and protein expression offibrotic factors. The pro-fibrotic proteins
MMP-9 and collagen-I were both significantly increased in untreated ZDF rats
104

Chapter S
compared to ZL (Figure 4 A and B). Vildagliptin treatment led to significant reduction in collagen- I protein expression (Figure 4B); however no differences were found in MMP-9 protein levels (Figure 4A). The expression of other pro-fibrotic proteins, such as TGF-�l and p-smad2/3 appeared not to be increased in untreated ZDF rats, but were unaffected by vildagliptin treatment (Figures 4C and D).
We then studied important stress pathways in cardiac remodeling. Phosphorylated PK.A was significantly decreased in ZDF compared to ZL rats, while vildagliptin treatment restored p-PKA levels (Figure SA). Furthermore, a significant increase level of p-P38 was observed in the hearts from ZDF rats, which was decreased by vildagliptin treatment (Figure SB). No differences of p-Erk were found among all groups (Figure SC).
A ZL ZDF ZDF+VIL
p-PKA ----- - - --t-PKA - - - -
2,0
1 ,6
� 1,2
0,8
ZL ZDF
C ZL ZDF
--
ZDF+VIL
ZDF+VIL
p-Erk p44/p42 =--==�;::.;;;; __
t-Erk p44/p42 --==-------1,2
w 0 9 �
0 ... :;;, 0,6 ui
0,3
Discussion
ZL ZDF ZDF+VIL
B
p-P38 t-P38
2,5
2,0
1\- 1,5 _g
] 1 ,0
0,5
ZL ZDF ZDF+VIL ---------�----------------*
o,o �-�-ZL ZDF ZDF+VIL
Figure 5 Effects of vildagliptin on phosphorylation of PKA, P-38, and Erk protein expressions following 15 weeks treatment. Representative immunoblots and bar graphs of phosphorylation of protein kinase A (PKA, A), P38 mitogen-activated protein kinases (p-38, B) and extracellular-signal
regulated kinase (Erk, C). Protein levels are normalized against total PKA, P-38 and Erk respectively. Data are means ± s.e.m. N=7, *P<0.05 vs. sham group; #P<0.05 vs. Ml JJT"Olln
In this study we first characterized the cardiac phenotype in the ZDF rat, a rat model of diabetes mellitus, and second we tested the effects of the DPP4-inhibitor vildagliptin
105

Vildagliptin in diabetic cardiomyopathy
on myocardial structure and function. We demonstrate here that the alterations in cardiac function of the ZDF rat are characterized by an impaired diastolic dysfunction, evidenced by lower E (and thus E/A ratio) and lower tissue velocity, indicative for early phase of diabetic cardiomyopathy. These unfavorable cardiac changes were associated with an increase of myocardial interstitial and perivascular fibrosis, production of pro-fibrotic factors, and changes in myocardial glycometabolic factors. We further demonstrate that factors, and changes in myocardial glycometabolic factors. We further demonstrate that treatment with the DPP-4 inhibitor vildagliptin exerted protective effects on cardiac function, since a trend of improvement of diastolic function was observed. Vildagliptin treatment partially reversed fibrosis, and, additionally, vildagliptin treatment appeared to beneficially affect fatty acid metabolism as demonstrated by the decrease in plasma NEFA levels in the treated ZDF rats. Quite surprisingly, vildagliptin had no clear effect on plasma glucose levels, and thus the beneficial effects of vildagliptin on cardiac function and structure in ZDF rats appear to be glucose-independent.
We demonstrate diastolic dysfunction upon hyperglycemia in the ZDF model as evidenced by changes in L V filling (E, E/ A ratio) and TYi indicating early stage of diastolic function as seen in diabetic cardiomyopathy. Our observations of an impaired diastolic function and maintained systolic function in untreated ZDF rats arc altogether consistent with earlier research on cardiac abnormalities in diabetic cardiomyopathy 23•
Increased LV diastolic stiffness and relaxation disturbances have been reported in both clinical and experimental studies before and have been found to be present in 27-70% of the diabetic patients 23• Given the explosion in type 2 diabetes mellitus, the associated cardiac abnormalities represent a major health care problem.
Previous research had already demonstrated increased fibrosis in myocardium and impaired cardiac function due to long-term hyperglycemia in ZDF rats 24-26. Here we confirm these earlier studies by showing that the interstitial fibrosis in the myocardium was significantly increased in ZDF rats. This increase in interstitial fibrosis was further associated with an increase in collagen I mRNA and protein expression. Moreover, our findings parallel earlier studies on cardiac abnormalities under hyperglycemic conditions. It has previously been found that cardiac fibrosis induced by sustained hyperglycemia increases myocardial stiffness, prolongs atrial filling phase, and finally results in impaired LV relaxation 27. Myocardial fibrosis and collagen deposition arc the culprit mediators that initiate cardiac diastolic dysfunction, myocardial fibrosis and diabetic hearts has frequently been observed. For example, both interstitial and perivascular fibrosis were observed in diabetic patients by biopsies 28 and experimental studies demonstrated increased fibrosis in the diabetic myocardium 16• 24• 25• 29• 30. Moreover we extend earlier work and show that the increase in fibrosis and collagen deposition was accompanied by over expression of protein levels of the
1 06

Chapter 5
pro-fibrotic proteins collagen I and extracellular matrix breakdown protein MMP-9. An earlier experimental study showing increased cardiac fibrosis in prediabetic OLETF rats suggested TGFP-I as the fibrotic mediator in this condition 9• However, we were not able to detect any differences in TGFP- I protein levels and its downstream target protein smad2/3 in this study. Phosphorylated PKA and p-38 were significantly changed in the ZDF myocardium. Vahtole et al. also reported that an increase in the phosphorylation of the p38 MAPK in the diabetic post-MI infarct myocardium, in Goto-Kakizaki rats 31 and streptozotocin (STZ)-induced type I diabetes mellitus 32.
DPP-4 inhibitors are relatively new antidiabetic agents. The effect of DPP-4 inhibitors (including vildagliptin) is to inhibit the degradation of GLP-I , which has been shown to exert multiple protective effects on both pancreases and heart, including reduction of fibrosis 33 34• Thus we investigated whether vildagliptin treatment can protect from diabetic cardiomyopathy. In our study, we found that vildagliptin reversed interstitial and perivascular fibrosis, and these findings were associated with a significant decreased collagen I protein expression. In a recent study, Chaykovska showed that another DPP-4 inhibitor linagliptin has an antifibrotic effect demonstrated by elevation cardiac expression ofTGF-P l , TIMP-1 , COLLl A l as well as COLL3AI mRNA levels 35
• Phosphorylated PKA and p-38 were partially restored by the vildagliptin treatment, although without an effect of decreasing the MMP-9 protein expression. It has been suggested that p38 MAPK play a role to regulate myocyte apoptosis, cellular hypertrophy, cardiac fibrosis, and cardiac cytokine-mediated inflammation 32• 36•
In addition to the structural changes in diabetic hearts, alterations in myocardial glucose metabolism have also been confirmed by many studies. The insulin-resistant ZDF rats represent numerous early path physiological changes in cardiac carbohydrate metabolism 37• It has been shown that high glycogen content, decreased glycogen synthase and low rate of glucose transport were present in the diabetic rat heart 16• 38.
Specifically, hearts from ZDF rats have impaired lactate oxidation, without clear functional consequence 39. In our study, the ZDF animals manifest elevated glucose levels and insulin levels, suggesting the early phase of diabetes, since hyperinsulinernia is provoked by high glucose levels. At the end of the experiment, a reduction of insulin levels was found in our study, indicating that pancreatic beta bells cannot longer respond to high glucose levels, which showed a later phase of diabetes. However, vildagliptin treatment had no effects on systemic glucose and insulin levels. However, we found a significant increase of myocardial glycogen content in ZDF animals, consistent with a previous study 38, and vildagliptin treatment reduced the myocardial glycogen content in the ZDF rats. Furthermore, we also found that the significant increase of myocardial glycogen content was associated with a decline of phosphorylated GSK-3 and GLUT4 protein expression. Vildagliptin normalized glycogen content, glycogen synthesis and glucose transport which could all contribute
107
Vildagliptin in diabetic cardiomyopathy
to an improved cardiac function. Furthermore, a significant elevation of NEFA plasma levels as well as a significant reduction of the lactate plasma levels was observed in ZDF rats. Vildagliptin trended to improve NEFA plasma level, demonstrating that vildagliptin may exert a beneficial effects on diabetic hearts mediated by fatty acid metabolism.
Conclusion: We describe that myocardial metabolic, structural, and functional dysfunction exists in diabetic ZDF rats, characterized by increased glycogen content and changes in glucose-specific genes, and interstitial and perivascular fibrosis. Treatment with the DPP-4 inhibitor vildagliptin led to an improvement in cardiac fibrosis and myocardial metabolism resulting in improved cardiac diastolic function, independent from systemic glucose levels. DPP-4 inhibition may be useful in patients with diabetic cardiomyopathy, and future clinical studies should be designed to evaluate the effects of DPP-4 inhibitors on cardiac function.
Competing interests
The authors declare that they have no competing interests.
Acknowledgements
Ms. Yin is a recipient of a fellowship by the Graduate School for Drug Exploration GUIDE (University of Groningen, Groningen, the Netherlands). The study was supported by Angteq BV, Groningen, the Netherlands. The research from Dr. de Boer is supported by the Netherlands Heart Foundation (grant 2007T046) and the lnnovational Research Incentives Scheme program of the Netherlands Organization for Scientific Research (NWO VENI, grant 916.10.117).
108

Chapter 5
References
I . Lin Y, Sun Z. Current views on type 2 diabetes. J Endocrinol 20 1 0;204: 1 - 1 1 .
2. Boudina S, Abel ED. Diabetic cardiomyopathy revisited. Circulation 2007;1 1 5:32 1 3-3223.
3. Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol I 974;34:29-34.
4. De Groote P, Lamblin N, Mouquet F, Plichon D, McFadden E, Van Belle E, et al. Impact of diabetes mellitus on long-term survival in patients with congestive heart failure. Eur Heart J 2004;25:656-662.
5. Bell OS. Diabetic cardiomyopathy. Diabetes Care 2003;26:2949-295 1 .
6. Liu JE, Palmieri V, Roman MJ, Bella JN, Fabsitz R, Howard BY, et al. The impact of diabetes on left ventricular filling pattern in normotensive and hypertensive adults: the Strong I leart Study. J Am Coll Cardiol 2001 ;37: 1 943- 1 949.
7. Falcao-Pires I, Goncalves N, Moura C, Lamego I, Eloy C, Lopes JM, et al. Effects of diabetes mellitus, pressure-overload and their association on myocardial structure and function. Am J Hyper/ens 2009;22: 1 1 90- 1 I 98.
8. Brown RA, Fil ipovich P, Walsh MF, Sowers JR. Influence of sex, diabetes and ethanol on intrinsic contractile performance of isolated rat myocardium. Basic Res Cardiol 1 996;91 :353-360.
9. Mizushige K, Yao L, Noma T, Kiyomoto 1 1, Yu Y, l losomi N, et al. Alteration in left ventricular diastolic filling and accumulation of myocardial collagen at insulin-resistant prediabetic stage of a type II diabetic rat model. Circulation 2000;101 :899-907.
1 0. Astorri E, Fiorina P, Contini GA, Albertini D, Magnati G, Astorri A, et al. Isolated and preclinical impairment of left ventricular filling in insulin-dependent and non-insulindependent diabetic patients. Clin Cardiol I 997;20:536-540.
1 1 . Joffe II, Travers KE, Perreault-Micale CL, Hampton T, Katz SE, Morgan JP, et al. Abnormal cardiac function in the streptozotocin-induced non-insulin-dependent diabetic rat: noninvasive assessment with doppler echocardiography and contribution of the nitric oxide pathway. J Am Coll Cardiol I 999;34:2 1 1 1 -2 1 1 9.
1 2. Phillips MS, Liu Q, Hammond HA, Dugan V, Hey PJ, Caskey CJ, et al. Leptin receptor missense mutation in the fatty Zucker rat. Nat Genet 1 996;13: 1 8- 1 9.
1 09
m
Vildagliptin in diabetic cardiomyopathy
1 3. Fredersdorf S. Thumann C, Ulucan C, Griese DP, Luchner A, Riegger GA, et al. Myocardial hypertrophy and enhanced left ventricular contractility in Zucker diabetic fatty rats. Cardiovase Pathol 2004;13 : 1 1 - 1 9.
1 4. Nunoda S, Genda A, Sekiguchi M, Takeda R. Left ventricular endomyocardial biopsy findings in patients with essential hypertension and hypertrophic cardiomyopathy with special reference to the incidence of bizarre myocardial hypertrophy with disorganization and biopsy score. 1/eart Vessels 1 985;1 : 1 70- 1 75.
1 5 . Ganguly PK, Pierce GN, Dhalla KS, Dhalla NS . Defective sarcoplasmic reticular calcium transport in diabetic cardiomyopathy. Am J Physiol 1 983;244:E528-35.
1 6. van den Brom CE, I luisman MC, Vlasblom R, Boontje NM, Duijst S, Lubbcrink M. et al. Altered myocardial substrate metabolism is associated with myocardial dysfunction in early diabetic cardiomyopathy in rats: studies using positron emission tomography. Cardiovase Diabetol 2009;8:39.
1 7. Ocscburg I I, de Boer RA, Buikema H, van der 1 -Iarst P, van Gilst WI I, Si llje I II I. Glucagonlikc peptide I prevents reactive oxygen species-induced endothelial cell senescence through the activation of protein kinase A. Arteriosc/er Thromb Vase Biol 20 1 0;30 : 1407- 14 14.
1 8. Matthews DR, I Iosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. I Iomcostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia I 985;28:4 1 2-4 1 9.
1 9. Wcstcnbrink BD, Ruifrok WP, Voors AA, Tilton RG, van Vcldhuisen DJ, Schoemaker RG, et al. Vascular endothelial growth factor is crucial for erythropoietin-induced improvement of cardiac function in heart failure. Cardiovase Res 20 1 0;87:30-39.
20. Yin M, Sillje I II I, Meissner M, van Gilst WI I, de Boer RA. Early and late effects of the DPP-4 inhibitor vildagliptin in a rat model of post-myocardial infarction heart failure. Cardiovase Diabetol 20 1 1 ;10:85.
2 1 . Yin M, van der I Iorst IC, van Melle JP, Qian C, van Gilst W I I, Sillje I 1 1-1, et al. Metformin improves cardiac function in a non-diabetic rat model of post-M I heart failure. Am J Physiol I /earl Cire Physiol 20 1 1 ;.
22. Falcao-Pires I, Leite-Moreira AF. Diabetic cardiomyopathy: understanding the molecular and cellular basis to progress in diagnosis and treatment. I /earl Fail Rev 20 1 1 ;.
23. Voulgari C, Papadogiannis D, Tentolouris N. Diabetic cardiomyopathy: from the pathophysiology of the cardiac myocytcs to current diagnosis and management strategies. Vase I lea/th Risk Manag 20 I 0;6:883-903.
1 1 0

Chapter 5
24. Forcheron F, Basset A, Abdallah P, Del Carmine P, Gadot N, Beylot M. Diabetic cardiomyopathy: effects of fenofibrate and metformin in an experimental model--the Zucker diabetic rat. Cardiovasc Diabetol 2009;8: 1 6.
25. Huang TH, Yang Q, Harada M, Li GQ, Yamahara J, Roufogalis BD, et al. Pomegranate flower extract diminishes cardiac fibrosis in Zucker diabetic fatty rats: modulation of cardiac endothelin- 1 and nuclear factor-kappaB pathways. J Cardiovasc Pharmacol 2005;46:856-862.
26. Marsh SA, Powell PC, Agarwal A, Dell'Italia LJ, Chatham JC. Cardiovascular dysfunction in Zucker obese and Zucker diabetic fatty rats: role of hydronephrosis. Am J Physiol Heart Circ Physiol 2007;293:H292-8.
27. Jain A, Avendano G, Dharamsey S, Dasmahapatra A, Agarwal R, Reddi A, et al. Left ventricular diastolic function in hypertension and role of plasma glucose and insulin. Comparison with diabetic heart. Circulation 1 996;93: 1 396- 1402.
28. van Heerebeek L, Hamdani N, Handoko ML, Falcao-Pires I, Musters RJ, Kupreishvili K, et al. Diastolic stiffiless of the failing diabetic heart: importance of fibrosis, advanced glycation end products, and myocyte resting tension. Circulation 2008;1 1 7:43-5 1 .
29. Ares-Carrasco S, Picatoste 8, Benito-Martin A, Zubiri I, Sanz AB, Sanchez-Nino MD, et al. Myocardial fibrosis and apoptosis, but not inflammation, are present in long-term experimental diabetes. Am J Physiol Heart Circ Physiol 2009;291:1-12 1 09- 1 9.
30. Westermann D, Rutschow S, Jager S, Linderer A, Anker S, Riad A, et al. Contributions of inflammation and cardiac matrix metalloproteinase activity to cardiac failure in diabetic cardiomyopathy: the role of angiotensin type I receptor antagonism. Diabetes 2007;56:64 1 -646.
3 1 . Vahtola E, Louhelainen M, Forsten H , Merasto S, Raivio J , Kaheinen P, et al. Sirtuin l -p53, forkhead box O3a, p38 and post-infarct cardiac remodeling in the spontaneously diabetic Goto-Kakizaki rat. Cardiovasc Diabetol 201 0;9:5.
32. Westermann D, Rutschow S, Van Linthout S, Linderer A, Bucker-Gartner C, Sobirey M, et al. Inhibition ofp38 mitogen-activated protein kinase attenuates left ventricular dysfunction by mediating pro-inflammatory cardiac cytokine levels in a mouse model of diabetes mellitus. Diabeto/ogia 2006;49:2507-25 1 3.
33. Drucker DJ. The biology of incretin hormones. Cell Metab 2006;3 : 1 53- 1 65.
34. Robinson E, Cassidy RS, McDermott BJ, Green BD, Grieve DJ. 49 Glucagon-like peptide) protects against cardiac remodelling after myocardial infarction via specific actions on the extracellular matrix. Heart 201 1 ;97:e7.
1 1 1

Vildagliptin in diabetic cardiomyopathy
35. Chaykovska L, von Websky K, Rahnenfuhrer J, Alter M, Heiden S, Fuchs I I, el al. Effects
of DPP-4 Inhibitors on the I leart in a Rat Model of Uremic Cardiomyopathy. PloS One 20 I I ;6:e2786 I .
36. Li M, Georgakopoulos D, Lu G, I lester L, Kass DA, I lasday J, el al. p38 MAP kinase
mediates inflammatory cytokine induction in cardiomyocytes and extracellular matrix
remodeling in heart. Circulation 2005;1 1 1 :2494-2502.
37. Chatham JC, Seymour AM. Cardiac carbohydrate metabolism in Zucker diabetic fatty rats.
Cardiovasc Res 2002;55: 1 04- 1 1 2.
38 . Lajoie C, Calderone A, Trudeau F, Lavoie N, Massicotte G, Gab'llOn S , et al. Exercise
training attenuated the PKB and GSK-3 dephosphorylation in the myocardium ofZDF rats.
J Appl Physiol 2004;96: 1 606- 1 6 1 2.
39. Wang P, Lloyd SG, Zeng 1 1, Bonen A, Chatham JC. Impact of altered substrate utilization
on cardiac function in isolated hearts from Zucker diabetic fatty rats. Am J Physiol Heart Circ Physiol 2005;288:1 12 1 02- 1 0.
1 12

Chapter 6
Diabetes is associated with an increased incidence of non-ischemic heart failure in patients with coronary
artery disease
B. Daan Westenbrink, MD PhD, Meimei Yin, Rudolf A. de Boer, MD PhD, J. Herre Kingma, MD PhD, Wayne J. Warnica, MD, Richard Bai/lot, MD, Jean L. Rouleau, MD PhD and Wiek H.
van Gilst, PhD.for the IMAGINE investigators
From the Department of Cardiology, University Medical Center Groningen, Groningen, the Netherlands (BDW, MY, RAB, WHO), Medisch Spectrum Twente, Enschede, the Netherlands
(JHK), Foothills Hospital, University of Calgary, Canada (WJW), Hospital Laval, Laval University, Canada (RB)and Institut de Cardiologie de Montreal, University of Montreal,
Montreal, Canada (JLR).

Chapter 6
Abstract
Aim: To determine whether diabetes is associated with an increased incidence of heart failure after coronary artery bypass grafting (CABG), and whether this can be explained by the recurrence of coronary ischemia.
Methods and results: We retrospectively analysed prospectively collected data from the IMAGINE trial, which tested whether early post-operative initiation of quinapril after CABG would reduce cardiovascular events in stable low risk patients with normal cardiac function. Of the 2553 patients included in the IMAGINE trial, 253 (10%) had diabetes (HBAlc 6.8 ± 1.2 %), of which 1 51 (60%) were treated with mctformin and 6 1 (24%) with insulin. During the maximal follow up of 43 months, the incidence of Major Adverse Coronary Events (MACE), coronary revascularisations or a composite of all cause cardiac and cerebrovascular events was comparable between diabetic and non-diabetic patients. Diabetes was, however, associated with a 3-fold higher incidence of hospitalizations for heart failure (adjusted hazard ratio (adj. HR) 3. 1 3, 95% confidence interval (Cl) 1.36-7. 19, p=0.007). A MACE never preceded heart failure hospitalisations in patients with diabetes and the incidence of recurrent ischemia was lower than in non-diabetic patients (HR 0.48, 95%CI (0.25-0.95), p=0.034). The use of mctformin was associated with a trend towards reduced heart failure hospitalisations within the subgroup of diabetic patients (adj. HR 0.27, 95% CI (0.1-1. 1 ), p=0.067).
Conclusions: Diabetes is associated with an increased incidence of non-ischemic heart failure in patients with coronary artery disease.
Key words: Coronary artery bypass grafting, diabetes, heart failure, mctformin
1 14

Diabetes increased incidence ofnon-ischemic heart failure after CABG
Introduction
Diabetes is associated with a two-fold higher lifetime risk of heart failure l-4_ Although diabetes predisposes to multiple other risk factors for heart failure, these cannot fully explain the high incidence of heart failure in patients with diabetes 5
• It has thus been hypothesized that diabetes causes a distinct, "diabetic" cardiomyopathy 6•
Diabetes is also a classical coronary risk factor associated with more extensive coronary artery disease (CAD), frequent revascularisation procedures and a higher incidence of Major Adverse Coronary Events (MACE) after revascularisation 7
• 8•
These coronary sequelae of diabetes are plausible explanations for the development of heart failure and diabetic cardiomyopathy is therefore defined as heart failure developing in the absence of CAD 6
• However, if heart failure can result from a diabetes-specific pathology in patients without CAD, there is no compelling reason why this could not also affect diabetic patients with CAD. We therefore hypothesise that diabetic cardiomyopathy may also develop in diabetic patients with established CAD.
We evaluated whether diabetes was associated with an increased incidence of heart failure after Coronary Artery Bypass Grafting (CABG) and whether the development of heart failure is associated with the recurrence of ischemia or MACE. For this purpose we examined the contemporary IMAGINE (Ischemia Management with Acupril post bypass Graft via Inhibition of the coNverting Enzyme) trial database of2553 low risk patients undergoing CABG 9• J O_
Methods The design of the IMAGINE trial, has been described in detail previously 9, as well as the results of the main study J O_ In brief, the IMAGINE study was a double-blind, placebo-controlled, parallel-group, randomized, multicenter international trial conducted in patients who underwent CABG surgery between November 1 999 and September 2004. The main goal of the study was to test whether early initiation of an ACE inhibitor after CABG (initiated within the hospital phase) would reduce the rate of cardiovascular events in patients at relative low risk. The ethics committees of all participating institutions approved the research protocol and all patients provided written informed consent.
Patients Patients were screened for eligibility within 4 weeks of surgery or following surgery and randomized within 7 days after CABG except for patients included in France (N=235, 9.1%), where randomization occurred within 10 days after CABG. Treatment consisted of the ACE inhibitor, quinapril, with forced up titration to 40 mg daily within
1 1 5

Chapter 6
4 months if tolerated, or matching placebo. Due to increasing evidence for the benefit of ACE inhibitors in patients with diabetes, all patients on insulin and diabetic patients with rnicroalbuminuria were no longer eligible for the study starting November 2001. The final sample size of the IMAGINE study was 2553 patients.
Endpoints We used the same primary and secondary endpoint of the IMAGINE trial, an additional composite endpoint of Major Adverse Cardiac Events (MACE) and, furthermore, considered all individual endpoints separately. The primary endpoint was a composite of cardiovascular death or resuscitated cardiac arrest, nonfatal myocardial infarction, coronary rcvascularization, unstable angina that required hospitalization, documented angina that did not require hospitalization, stroke and congestive heart failure that required hospitalization. The pre-specified secondary endpoint was a composite of the primary end point with the addition of transient ischemic attack and any other cardiovascular event that required hospitalization. MACE was defined as cardiovascular death, resuscitated cardiac arrest, unstable angina or myocardial infarction.
Statistical analysis Data arc given as means ± standard deviation (SD) when normally distributed, as median and interquartile range (IQR) in case of skewed distribution and as frequencies and percentages for categorical variables. Differences in variables between groups were compared with student T-tcst, Mann Whitney-U test, x2 test or Fishers exact test, where appropriate. Differences between the diabetic and the non-diabetic groups were estimated as a hazard ratio (HR) with associated adjusted two-sided 95% confidence interval (Cl) from a Cox proportional hazards regression model, that included the effects of age, gender, treatment assignment, diabetic and cardiovascular medications, left ventricular ejection fraction (L VEF), smoking status, systolic and diastolic blood pressure, creatinine values, history of hypertension / percutaneous coronary interventions / myocardial infarction / previous CABG surgery and stroke, vessel disease, completeness of revascularization ( defined as complete when all vessels > I mm with a stenosis >70% were bypassed) and beating heart (off pump) surgery. Because we recently showed that mctformin attenuates heart failure development after myocardial infarction in an experimental model 1 1 , we also evaluated the effect of mctformin on the incidence of heart failure within the subpopulation of patients with diabetes, controlling for the use of insulin, pre-operative left ventricular ejection fraction, history of myocardial infarction and hypertension. Cumulative event rate were calculated by the Kaplan Meier method and displayed graphically. All statistical analysis was performed using SPSS, Chicago version 18.0.
1 16

Diabetes increased incidence ofnon-ischemic heart failure after CABG
Results
Demographics of the study population
Of the 2553 patients included in the IMAGINE trial, 1 0% had a history of diabetes, of
which 151 (60%) were treated with metformin and 61 (24%) with insulin.
Demographics of the population according to the presence of diabetes are given in
Table 1 . Patients with diabetes were significantly younger, more often female and had
higher baseline systolic blood pressures and a history of hypertension more often than
non-diabetic patients. All other demographics were comparable between diabetic and
non-diabetic patients.
Effect of diabetes on the incidence of cardiovascular events after CABG
The median follow up time was 2.95 years. During this period, diabetes was not
associated with an increased incidence of the primary or secondary IMAGINE
endpoints or MACE (table 2). When the individual endpoints were considered
separately, patients with diabetes displayed a significant higher incidence of heart
failure requiring hospitalisation (table 2, figure 1) and a reduced incidence of
documented angina not requiring hospitalisation (table 2). All other component
endpoints were comparable between patients with or without diabetes.
Exploration of heart failure and cardiovascular events in diabetic subpopulation
In patients with diabetes, a MACE never preceded hospitalization for heart failure and
only one diabetic patient developed a MACE after heart failure had developed.
Randomisation to quinapril did not affect the incidence of heart failure hospitalisations
or other component or individual endpoints. In diabetic patients treated with metformin,
there was a trend towards reduced heart failure hospitalisations, even after controlling
for the concomitant use of insulin, pre-operative left ventricular ejection fraction,
history of myocardial infarction and hypertension (adj. HR 0.27 95% CI (0.1-1.1),
p=0.067).
Discussion
In the current analysis of low risk patients with normal cardiac function after scheduled
CABG, diabetes was associated with a 3-fold higher incidence of hospitalisations for
heart failure. Surprisingly, heart failure in patients with diabetes developed without the
recurrence of ischemia or a preceding MACE. In fact, patients with diabetes had fewer
ischemic events than non-diabetic patients. These findings suggest that diabetic
patients may develop heart failure of non-ischemic origin that is not directly linked to
117

Chapter 6
vascular events, even when they have already developed severe CAD.
Hospitalizations for heart failure
1 .00
Diabetics
- Non-diabetics cii >
.f 0.95
:, u,
HR 3.1 3, 95% Cl (1 .36-7.19) p=0.007
0.90 ...... --------------
0 500 1 000
Time (days)
1 500
Figure 1 . Kaplan-Meier analysis of the cumulative incidence of heart failure hospitalisations according to the presence or absence diabetes. HR, Hazard Ratio; 95% Cl, 95 percent confidence interval
1 .00
�
� -� 0.95 :J u,
Hospitalizations for heart failure
- Metformin
- other
HR 0.27, 95% Cl (0.1 -1 .1 ), p=0.067
0.90 ....... --------------
0 500 1000
Time (days)
1500
Figure 2. Kaplan-Meier analysis of the cumulative incidence of heart failure hospitalisations in patients with diabetes, according to the use of metformin. HR. Hazard Ratio; 95% CI, 95 percent confidence interval
1 1 8

Diabetes increased incidence of non-ischemic heart failure after CABG
Table 1: Demographics of the study population according to the presence of diabetes
Variable
Age Female, n (% of patients) White, n (% of patients) Quinapril group, n (% of patients)
Medical History, n (% of patients) Previous M l Previous Stroke Previous CABG Previous PC! Hypercholesterolaemia I Ii story of hypertension Current smoker
Laboratory values, Mean ± SD HBAI C Haemoglobin (mg/dL) LDL cholesterol (mmol/L) I IDL cholesterol (mmol/L) Creatinine (µmol/L)
I lemodynamic measurements, Mean ± SD LVEF (%) Systolic blood pressure (mmHg) Diastolic blood pressure (mmHg)
Operative characteristics Beating heart surgery, n (% of patients) Number of distal anastomosis, Mean ± SD Triple vessel disease, n (% of patients) Complete revascularization, n (% of patients)
Baseline medications , n (% of patients) Metformin Insulin Beta blocker Calcium channel inhibitor Angiotensin receptor blocker ACE-I Platelet inhibitor Statin Diuretic
Non-Diabetic (n=2300) 6 1 ± 1 0 283 ( 1 2) 22 14(96) 1 1 59 (50)
897 (39) 47 (2) 56 (2) 407 ( 1 8) I I O (9) 1 055 (45) 469 (20)
5.6 ± 1 .2 75 ± 42 2.8 ± I I . I ± 0.4 87 ± 1 8
60 ± 9.7 1 2 1 ± 14 70 ± 9
427 ( 1 9) 3.2 ± I . I 1 470 (64) 2044 (99)
1 803 (78) 828 (36) 58 (2.5) 454 (20) 1 693 (74) 1 490(65) 202 (8.8)
Diabetic (n=253) 62 ± 1 0 4 1 ( 1 6) 239 (95) 1 2 1 (48)
1 04 (4 1 ) 7 (3) 8(3.2) 48 ( 1 9) 1 02 ( 1 1 ) 146 (57) 39 ( 1 5)
6.8 ± 1 .2 74 ± 43 2.9 ± I I . I ± 0.3 88 ± 21
59 ± 9.5 1 24± 14 70 ± 9
49 ( 1 9) 3.2 ± I . I I 70 (67) 2 1 1 (88)
1 5 1 (60) 61 (24) 203 (80) 1 04 (4 1 ) 1 4 (3.5) 59 (23) 1 98(78) 1 60(63) 32 ( 1 3)
p
0.037 0.035 0.69 1 0.097
0.487 0.632 0.382 0.535 0.742 >0.0001 0.084
0.802 0.094 0. 1 9 1 0.496
0.2 1 1 0.002 0.865
0.723 0.7 19 0. 1 36 0.03 1
0.057 0.833 1 .000 0.933 0. 1 04 0.394 0.092
SD, standard deviation; Ml, myocardial infarction; CABG, coronary artery bypass graft surgery; PCl, percutaneous coronary intervention; LDL, low density lipoprotein; HDL, High density lipoprotein;
1 19

N 0 Table 2. Incidence of the primary and secondary endpoints and their components in diabetic compared to non-diabetic patients
Unadjusted Adjusted
Variable Non- Diabetic HR (95%CD p HR (95%CI) p diabetic (n=253) (n=2300)
Primary composite endpoint 295 ( 1 3) 35 ( 1 3) 1 .41 (0.54- 1 2.5) 0.234 Secondary composite endpoint 453 (20) 57 (23) 1 .07 (0.08- 1 .42) 0.6 1 6 Major Adverse Cardiac Events 1 3 1 (5.7) I 8 (7. 1 ) 1 .22 (0.75-2.00) 0.425 All cause mortality or resuscitated arrest 34 ( 1 .5) 3 ( l .2) 0.78 (0.24 1 -2.55) 0.687 Acute coronary syndromes 1 00 (4.3) 1 5 (5.9) 1 .33 (0. 78-2.30) 0.506 Coronary revascularization 84 (3. 7) 9 (3.6) 0.95 (0.48- 1 . 90) 0.893 HF requiring hospitalization 20 (0.9) 1 1 (4.3) 4.09 ( 1 .86-8.99) <0.000 1 3 . 1 3 ( l .36-7. 1 9) 0.007 Documented angina 1 63 (7. 1 ) 9 (3 .6) 0.49 (0.25-0.96) 0.039 0.48 (0.25-0.95) 0.035 Stroke or TIA 44 ( 1 .9) 4 ( 1 .6) 0.8 1 (0.29-2.25) 0.683 Other CV hospitalizations 1 74 (8) 29 ( 12) 1 .54 ( 1 .04-2.28) 0.033
CHF, congestive heart failure; TIA, transient ischemic cerebrovascular attack, CV; cardiovascular, HR, hazard ratio, 95%CI, 95% confidence interval, Adjusted for, age, gender, treatment assignment, days after CABG-surgery, baseline medications, left ventricular ejection fraction, systolic and diastolic blood pressure, creatinine, h istory of hypertension / percutaneous coronary interventions I myocardial infarction I previous CABG surgery / peripheral vascular disease I stroke, number of distal anastomosis, completeness ofrevascularization, and beating heart (off pump) surgery.
n ::r �
"O ('i) '"I 0\

Diabetes increased incidence of non-ischemic heart failure after CABG
Diabetes is a potentially modifiable coronary risk factor that is rapidly emerging.
Approximately 80% of patients with diabetes will develop a myocardial infarction and
a high percentage of them will undergo a coronary revascularisation procedure during
their lifetime 7• 8• 1 2• Furthermore, the recurrence of cardiovascular events and restenosis
rates are also markedly higher in diabetic than in non-diabetic patients 8• From the
burden of CAD in diabetic patients, it does not appear surprising that diabetes is
associated with an increased incidence of heart failure. Indeed, a recent study showed
that while the association between diabetes and heart failure was independent of over
65 potential confounders, heart failure in patients with diabetes still predominantly
developed after a myocardial infarction 5•
In the current analysis, heart failure after CABG developed in diabetic patients
in the absence of new coronary events or recurrent ischemia. Furthermore, the
increased incidence of heart failure was also independent of other risk factors for heart
failure, including history of myocardial infarction and hypertension, LVEF and renal
function, suggesting that heart failure was caused by a distinct diabetes related process.
It therefore appears that diabetic cardiomyopathy can also develop in patients with
severe CAD. Thus, while our analysis does not dispute that CAD can cause heart
failure in diabetes; it does show that the mere presence of CAD in a diabetic patient
does not necessarily explain the aetiology of heart failure. If our findings are be
substantiated by other reports in the future, this would also implicate that the definition
of diabetic cardiomyopathy should be revised.
The current analysis was not adequately powered to conclusively identify factors
that modulate the incidence of heart failure in patients with diabetes. In an exploratory
analysis, however, we observed an interesting trend towards reduced heart failure in
patients treated with metformin. Several epidemiological studies have associated
metformin with a reduced event rate in patients with diabetes 13
• Moreover, a recent
study from our group showed that metformin attenuated heart failure after myocardial
infarction in rats without diabetes 1 1
• Metformin may thus have the potential to prevent
heart failure in diabetic patients. Given the limitations stated above, these results
should be interpreted with caution. Nevertheless, it does merit further investigation.
Limitations The IMAGINE study involved a relatively healthy low risk population and patients
with severe or complicated diabetes were specifically excluded from our study. While
this could be regarded a strength of the study, it does also limits the ability to extend
our findings to the general CABG population. Moreover, the fact that diabetes was not
associated with an increased incidence of the other individual or composite endpoints,
at least partially reflects the low event rate in the IMAGINE trial. Patients with clinical
heart failure and systolic left ventricular dysfunction were excluded from IMAGINE,
12 1
Chapter 6
but we cannot exclude that some patients might have had pre-operative diastolic dysfunction that influenced the propensity to be hospitalised for heart failure. Finally, despite the use of extensive multivariable adjustments, we cannot be certain that the relation between diabetes and non-ischemic heart failure is causal since we employed a retrospective analysis of prospectively collected data. Future studies are needed to further define the prevalence of diabetic cardiomyopathy in patients with CAD undergoing CABG.
Conclusions Diabetes is associated with an increased incidence of non-ischemic heart failure in patients with coronary artery disease. The cause for heart failure hospitalizations in the diabetic subset of the IMAGINE population seemed mostly non-ischemic, which points towards the possibility that direct diabetic factors provoke heart failure development.
122

Diabetes increased incidence of non-ischemic heart failure after CABG
References
I . Kannel WB, 1-ljortland M , Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol 1 974;34:29-34.
2. Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321 :405-4 12 .
3 . Gottdiener JS, Arnold AM, Aurigemma GP, Polak JF, Tracy RP, Kitzman DW, et al. Predictors of congestive heart failure in the elderly: the Cardiovascular I Iealth Study. J Am Coll Cardiol 2000;35: 1 628-1 637.
4. Nieminen MS, Brutsaert D, Dickstein K, Drexler 1-1, Follath F, 1-larjola VP, et al. Eurol-leart Failure Survey II (El IFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J 2006;27:2725-2736.
5 . Roy 8, Pawar PP, Desai RV, Fonarow GC, Mujib M, Zhang Y, et al. A propensity-matched study of the association of diabetes mellitus with incident heart failure and mortality among community-dwelling older adults. Am J Cardiol 20 1 1 ;1 08: 1 747- 1 753.
6. Murarka S, Movahed M R. Diabetic cardiomyopathy. J Card Fail 20 l 0;16:97 1 -979.
7. 1-llatky MA, Boothroyd DB, Bravata DM, Boersma E, Booth J, Brooks MM, et al. Coronary artery bypass surgery compared with percutaneous coronary interventions for multivessel disease: a collaborative analysis of individual patient data from ten randomised trials. Lancet 2009;373 : 1 1 90- 1 1 97.
8. Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS), European Association for Percutaneous Cardiovascular Interventions (EAPCI), Wijns W, Kolh P, Danchin N, Di Mario C, et al. Guidelines on myocardial revascularization. Eur Heart J 201 0;31 :2501 -2555.
9. Wamica JW, Gilst WV, Baillot R, Johnstone D, Block P, Myers MG, et al. Ischemia Management with Accupril post bypass Graft via Inhibition of angiotensin coNverting enzyme (IMAGINE): a multicentre randomized trial - design and rationale. Can J Cardiol 2002;18: 1 1 9 1 - 1 200.
1 0. Rouleau JL, Wamica WJ, Baillot R, Block PJ, Chocron S, Johnstone D, et al. Effects of angiotensin-converting enzyme inhibition in low-risk patients early after coronary artery bypass surgery. Circulation 2008;1 17:24-3 1 .
123
Chapter 6
1 1 . Yin M, van der Horst IC, van Melle JP, Qian C, van Gilst WI I, Sillje 1-11 1, et al. Metforrnin improves cardiac function in a non-diabetic rat model of post-M I heart failure. Am J Physiol I !earl Circ Physiol 201 1 ;.
1 2. Narayan KM, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF. Lifetime risk for diabetes mellitus in the United States. JAMA 2003;290: 1 884- 1 890.
13 . Mcssaoudi SE, Rongen GA, de Boer RA, Riksen NP. The cardioprotcctive effects of mctforrnin. Curr Opin Lipido/ 20 1 1 ;22:445-453.
1 24

Chapter 7
Summary and future perspectives

Chapter 7
Summary and future perspectives
Summary
Heart failure is characterized by cardiac dysfunction, severe symptoms and is associated with major morbidity and mortality 1
, and health care costs. The triggers that stimulate the development of heart failure are diverse, such as coronary artery disease, hypertension, dilated cardiomyopathy, valvular disease or diabetes 2• Diabetes has increased dramatically as a risk factor for coronary artery disease which can lead to myocardial infarction and subsequently to heart failure. Despite the diverse causes of heart failure, the clinical progression and underlying mechanisms share a common pathway. After cardiac injury, the heart starts to hypertrophy and reshapes as a response to injury, this process is called cardiac remodeling 3• Although pharmacological treatment has already achieved significant improvement, the outcome for heart failure patients is still poor. New therapeutically strategies on heart failure are therefore needed.
In chapter 1, we discuss the relationship between heart failure and diabetes. The most important conclusion is that diabetes and heart failure are both major and growing public health issues. In addition, they are strongly interrelated and can affect, aggravate and provoke each other.
In chapter 2, we provide an overview of the available data from experimental studies evaluating the effect of oral diabetic medication on cardiac remodeling and heart failure. It is concluded that some anti-diabetic drugs, especially metformin and agents interfering with the GLP-1/DPP-4 system, exert cardioprotection, independent of their effect on glucose metabolism, in various experimental models. For metformin, this is supported by post hoc analyses from clinical trials. No prospective trials have been conducted specifically evaluating heart failure outcomes with antidiabetic treatment. We propose that these studies should be performed in diabetic, but even more interestingly, in pre-diabetic subjects.
In chapter 3, we evaluated whether the first line anti-diabetic drug, metformin, would exert protective effects on cardiac remodeling in a post-Ml rat model. In this well-established experimental heart failure model, approximately 40% of the LV wall is infarcted, which is associated with a significant increase of ANP. Echocardiographic and hemodynamic parameters showed that, in control rats, cardiac function was remarkably reduced long term (10-12 weeks) after myocardial infarction, and left ventricular wall thinning, dilatation, and reduced systolic function was observed. Concomitantly, cardiac hypertrophy developed after myocardial infarction, evidenced by enlarged cardiomyocytes, and a significant decrease of capillary density.
1 26

Summary and future perspectives
Metformin treatment resulted in a moderate decrease in infarct size, and attenuation of cardiac remodeling, as evidenced by decreased ANP mRNA expression, improvement of systolic function and less left ventricular dilatation as compared to untreated myocardial infarction. In addition, molecular analyses suggested that altered AMPK phosphorylation status and low insulin levels could be the mechanisms underpinning the observed cardioprotection in this non-diabetic post-Ml animal model. We, furthermore, evaluated whether long-term heart failure would provoke insulin resistance. However, fasting glucose levels and the pattern of the oral glucose tolerance test suggested that no insulin resistance did occur during cardiac remodeling, and metformin did not affect this. Altogether, our results indicate that metformin has the potential to attenuate heart failure development after myocardial infarction in the absence of diabetes, independent of systemic glucose levels, and independent from insulin intolerance.
In chapter 4, we investigated the effect of the DPP-4 inhibitor, vildagliptin, on post-Ml cardiac remodeling. Vildagliptin is a member of a new class of anti-diabetic drugs, the incretins, which are reported to have a beneficial role on the cardiovascular system. DPP-4 breaks down rapidly GLP-1, and a DPP-4 inhibitor prevents this to occur and thus raises GLP- 1 levels. We, therefore, hypothesized that the DPP-4 inhibitor, vildagliptin, would also have a protective effect on cardiac function in postMI heart failure model.
We used the same well-established rat post-Ml heart failure model as in chapter 3. The DPP-4 inhibitor, vildagliptin, increased endogenous active GLP-1 levels approximately 3 -fold, associated with an (expected) inhibition of 70% in DPP-4 activity. However, the infarct size and cardiac function did not differ between DPP-4 inhibitor treated animals and controls. All other measures of cardiac remodeling were also not affected. The reasons for the failure of DPP-4 inhibition to halt adverse cardiac remodeling may be various: the dosing regimen, the different analogue utilized, the levels of G LP- I achieved, and the timing of the treatment and the species studied. These findings indicate, that despite an increase in plasma GLP- 1 levels by inhibiting DPP-4 activity, long-term treatment with the DPP-4 inhibitor, vildagliptin, does not afford cardiac protection in a rat post-Ml model of heart failure.
In chapter 5, we explored the effect of the DPP-4 inhibitor, vildagliptin, on the early stage of diabetic cardiomyopathy. Since the incidence of diabetes is on the rise, we expect to see more often myocardial dysfunction in diabetic subjects, also in the absence of CAD or hypertension. Currently, only few data are available showing what effects are conferred by specific anti-diabetic treatment with respect to myocardial function and metabolism. We used Zucker Diabetic Fatty (ZDF) rats, which have a mutation in the leptin receptor gene, associated with obesity and diabetes, to study the myocardial changes and mechanisms pertinent to the metabolic syndrome. The animals
1 27
Chapter 7
develop insulin resistance in the beginning of the study (age of 10 weeks), evidenced by increased glucose and insulin levels. In the following 15 weeks of the experiment, insulin levels in the ZDF animals decreased significantly, indicating pancreatic function failure.
In this experiment, the heart of ZDF animals showed impaired diastolic function, altered myocardial metabolism, and myocardial fibrosis. The echocardiographic function parameters E, E/A ratio, and TVI were significantly decreased in the ZDF group compared to the Zucker lean animals, which served as control. These changes were associated with more collagen deposition, both interstitial as perivascular, which is consistent with an increased collagen I protein expression. P-38 MAPK and p-PKA were identified as potential contributors to the myocardial dysfunction and fibrosis. Alterations in myocardial substrate metabolism were also found in the present study, including abnormal lipid metabolism and glucose homeostasis. Increased NEFA were present in the ZDF animals, and myocardial glycogen content was significantly increased as well. The elevated glycogen content resulted in attenuation of phosphorylation of GSK-3 and GLUT4. Vildagliptin treatment attenuated myocardial fibrosis and left ventricular stiffness in diabetic animals, which led to a trend towards improvement of diastolic function. These changes were associated with a decrease of collagen I and of p-38 protein expression. Improved glucose metabolism was suggested by the observation of restored myocardial glycogen content and increased phosphorylation of GSK-3 and GLUT4 protein, which suggests that vildagliptin improves glucose uptake in the diabetic animal model.
In chapter 6, we evaluated whether diabetes was associated with an increased incidence of heart failure after coronary artery bypass grafting (CABG) in the IMAGINE (lschemia Management with Acupril post bypass Graft via Inhibition of the coNverting Enzyme) trial. IMAGINE was a double-blind, placebo-controlled, randomized, multicenter international trial evaluating whether an ACE inhibitor, quinapril, administered early after CABG could reduce cardiovascular mortality and morbidity. From the 2553 patients, 10% had diabetes, of which 60% were treated with metformin and 24% were treated with insulin. During a median follow up of approximately three years, the incidence of the primary ( composite of cardiovascular death or resuscitated cardiac arrest, nonfatal myocardial infarction, coronary revascularization, unstable angina that required hospitalization, documented angina that did not require hospitalization, stroke and congestive heart failure that required hospitalization) and secondary ( of the primary end point with the addition of transient ischemic attack and any other cardiovascular event that required hospitalization) IMAGINE endpoints or major coronary events were comparable between the diabetic and non-diabetic patients. However, a 3-fold higher incidence of hospitalisation due to heart failure was observed in diabetic patients. Furthermore, there was a trend towards
128

Summary and future perspectives
reduced heart failure hospitalisations in diabetic patients treated with metformin, suggesting a protective potential on heart failure in diabetes.
Future perspectives
Diabetes and heart failure are very prevalent and it has been demonstrated that they affect each other mutually. As we know, many diseases are not isolated, stand alone problems. This is true for obesity, hypertension, metabolic syndrome, and thus also for diabetes and heart failure. This condition can be described as a cardiometabolic syndrome, as these two diseases can aggravate and provoke each other; i.e. patients with diabetes have a high risk to develop cardiovascular disease and subsequent heart failure, and in reverse order, heart failure patients with diabetes have worse outcome. For this reason, the cardiometabolic syndrome has become an important new target for research and treatment in cardiology during the last decade. However, there are very few studies that looked into the two diseases together. Therefore, it is mandatory to perform further clinical studies to focus on this cardiometabolic syndrome, enrolling patients with both diabetes and heart failure.
In addition, both clinical studies and experimental studies have shown that diabetes specific treatment may be useful not only to correct glucose levels, but also to beneficially affect the heart directly. Our experimental study showed that metformin attenuates cardiac remodeling in the post-Ml, non-diabetic heart failure model 4. Based on this experimental study, we hypothesized that metformin has a potential beneficial effect in non-diabetic patients with left ventricular dysfunction. Therefore, we designed a!t and started a phase IV clinical trial that is called "Metformin to Reduce Heart Failure Ill After Myocardial Infarction" (GIPS-lll, NCT01217307). This study is still ongoing and will evaluate the effect of metformin in non-diabetic patients after myocardial infarction. Non-diabetic patients following ST-elevation myocardial infarction are selected and given metformin 500 mg twice daily during 4 months. The primary outcome is the effect of metformin treatment on left ventricular ejection fraction. The incidence of cardiovascular events during follow-up is the secondary outcome.
Finally, over the years many experimental studies have reported protective effects of anti-diabetic drugs on the cardiovascular system. The majority of these studies were performed in non-diabetic animals, as reviewed in this thesis. In contrast however, the relatively small number of clinical trials performed so far, have been mostly negative or controversial in their findings s-s when compared to the reported experimental data. The explanation for this controversy is largely unknown but it stresses the importance of confirmative large clinical trials. Certainly for the newer anti-diabetic drugs like GLP-1 analogues and DPP-4 inhibitors, there are promising
1 29

Chapter 7
and consistent results available from experimental studies outlining their cardioprotective potential but again large clinical trials are needed. The investment in this research will help our understanding of the mechanism of action of these drugs and certainly will generate new insight in the interplay between diabetes and heart failure.
130

Summary and future perspectives
References
I . Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, Ho KK, et al. Long-term trends in the incidence of and survival with heart failure. N Engl J Med 2002;347: 1 397-1 402.
2. Cohn JN, Bristow MR, Chien KR, Colucci WS, Frazier 01 I, Leinwand LA, et al. Report of the National Heart, Lung, and Blood Institute Special Emphasis Panel on Heart Failure Research. Circulation I 997;95:766-770.
3. Fedak PW, Verma S, Weisel RD, Li RK. Cardiac remodeling and failure: from molecules to man (Part !). Cardiovasc Pathol 2005;14: 1 - 1 1 .
4. Yin M, van der Horst IC, van Melle JP, Qian C, van Gilst WI I, Sillje I IH, et al. Metformin improves cardiac function in a non-diabetic rat model of post-Ml heart failure. Am J Physiol
Heart Circ Physiol 20 1 1 ;.
5 . Eurich DT, McAlister FA, Blackburn DF, Majumdar SR, Tsuyuki RT, Varney J, et al.
Benefits and harms of antidiabetic agents in patients with diabetes and heart failure: systematic review. BMJ 2007;335:497.
6. Eurich DT, Tsuyuki RT, Majumdar SR, McAlister FA, Lewanczuk R, Shibata MC, et al.
7.
Metformin treatment in diabetes and heart failure: when academic equipoise meets clinical reality. Trials 2009;10: 1 2.
Fisman EZ, Tenenbaum A. A cardiologic aP.proach to non-insulin anti-diabetic pharmacotherapy in patients with heart disease. Cardiovasc Diabetol 2009;8:38.
•
8. Gavin JR 3rd, Bohannon NJ. A review of the response to oral anti-diabetic agents in patients with type 2 diabetes. Postgrad Med 201 0;122:43-5 1 .
13 1


Nederlandse Samenvatting

Samenvatting en toekomstperspectieven
Samenvatting
Hartfalcn wordt gckarakteriscerd door cardiale dysfunctie en ernstige symptomen en is gcassocicerd met hoge morbiditeit, mortaliteit 1
, en hoge ziektekosten. Hartfalen kan door diverse triggers worden veroorzaakt; hartfalen kan onder andere opgewekt wordcn door aandoeningen van de kransslagaders (myocardinfarct), hypcrtensie, gcdilatccrdc cardiomyopathie, klcplijden en diabetes 2• Ondanks de vcrschillende oorzakcn van hartfalen, is het klinisch beloop ongeveer hctzelfdc en zijn ook de ondcrliggcndc mechanismcn van zickteprogressie veelal gelijk. Na hct ontstaan van schadc aan hct hart wordt het hart groter (hypertrofie) en verandert het hart als rcactic op de ontstane schade. Dit proces wordt remodeling genoemd3 • Hoewel farmacologische behandeling heeft geleid tot een aanzienlijke verbetering is de prognosc voor patientcn met hartfalen nog steeds slecht. Nieuwe therapeutische strategiccn zijn daarom noodzakclijk.
Diabetes is een thans veelvoorkomende risicofactor voor coronaire hartziekte, welke kan leiden tot een hartinfarct en vervolgcns tot hartfalcn. Diabetes hccft ccn reciprokc relatie met hartfalen: diabetes vergroot de kans op het ontwikkclcn van hartfalen, maar patienten met hartfalen krijgen ook vaker diabetes. Als ccn van bcidc condities ontstaat als de andcr reeds aanwczig is, is het prognostischc effect hicrvan grater dan je zou verwachtcn - diabetes en hartfalen versterken elkaar. Alhoewel er vele studies zijn gedaan naar antidiabetica met speciaal oog voor de effecten op het hart, zijn er relatief wcinig data over de cffccten van orale anidiabctica op het proces van remodeling en hartfalcn. Dit proefschrift bcschrijft ccn aantal cxpcrimentclc studies waarin is bcstudccrd hoe bepaalde oralc antidiabetica het ontstaan van hartfalcn bei"nvloeden.
In hoofdstuk 1 bespreken we de relatie tussen hartfalen en diabetes. Diabetes en hartfalcn zijn bcide grote problemen voor de volksgezondheid; het ziekteverloop van hartfalen en diabetes kan elkaar bei"nvloeden en elkaar versterken. Daamaast lijkt hct crop dat de aanwezigheid per se van de ene ziekte de anderc ziekte kan uitlokken.
In hoofdstuk 2 gcvcn we ccn ovcrzicht van de beschikbarc gegcvcns uit cxpcrimentele studies, we beschrijvcn de effecten van orale diabetes medicatie op cardialc remodeling en hartfalen. We concluderen dat van een aantal behandelingen, met name metformine en stoffcn die interfcrercn met hct GLP-1/DPP-4-systcem, is aangetoond dat ze het hart bcschermen in verschillende experimentele modellen. Dit wordt wat betreft mctforminc ondcrstcund door post-hoc analyses van grate klinische studies. Er zijn
1 34

Nederlandse samenvatting
geen prospectieve studies uitgevoerd waarbij het effect van behandeling van diabetes op hartfalen is onderzocht. Wij stellen voor dat deze studies worden gedaan, bij diabetici en wat mogelijk nog interessanter is, in pre-diabetici.
In hoofdstuk 3 hebben we onderzocht of metformine, het eerstelijns diabetesmiddel, beschermende effecten heeft op de cardiale remodeling in een post-MI rat model. Dit model wordt gekenmerkt door post-MI hartfalen, waarbij ongeveer 40% van de LV wand geinfarceerd is, en geassocieerd is met een significante toename van genexpressie kenmerkend voor cardiale remodeling, zoals ANP. Echocardiografische en hemodynamische parameters laten zien dat in controle ratten hartfunctie op de lange termijn ( 1 0-12 weken) sterk verminderd was na een myocardinfarct. We zagen een dunnere linkerkamer wand, dilatatie en een verminderde systolische functie. Daamaast zagen we hypertrofie van het hart, blijkend uit vergrote cardiomyocyten, en een significante afname van de capillaire dichtheid.
Behandeling met metformine resulteerde in een kleine afname van de infarct grootte en daarbij passende vermindering van cardiale remodeling, zoals blijkt uit verminderde ANP expressie (50% reductie), verbetering van de systolische functie en minder dilatatie van het linker ventrikel in vergelijking met het onbehandelde myocardinfarct. Moleculaire analyses wijzen op een rol voor de veranderende AMPK fosforylatie en lage insuline levels als beschermingsmechanismen voor het hart in dit non-diabetische post-MI model. Daamaast hebben we onderzocht of een lange duur van hartfalen insulineresistentie zou kunnen veroorzaken. Echter, basale bloedsuikerwaarden en de orale glucose tolerantie test suggereerde dat er geen insulineresistentie voorkwam tijdens de cardiale remodeling en dat metformine hier ook geen effect op had. Samengevat, onze resultaten wijzen er op dat metformine potentie heeft om de ontwikkeling van hartfalen na MI te remmen, in de afwezigheid van diabetes en onafhankelijk van systemische glucoselevels en onafhankelijk van insuline intolerantie.
In hoofdstuk 4 hebben we het effect van de DPP-4-remmer vildagliptine op post-MI cardiale remodeling onderzocht. Vildagliptine maakt deel uit van een nieuwe klasse van anti-diabetica, de incretines, waarover gepubliceerd is dat ze ook een beschermend effect hebben op het cardiovasculaire systeem. DPP-4 breekt GLP-l snel af, een DPP-4-remmer verhindert dit en verhoogt daarmee de GLP-1 levels. Onze hypothese was dat de DPP-4-remmer vildagliptine een beschermend effect heeft op de hartfunctie in een post-MI hartfalen model.
In deze studie hebben we hetzelfde model gebruikt als in hoofdstuk 3, het post-MI hartfalen model. De DPP-4 remmer vildagliptine verhoogde het actieve endogene
1 35

GLP-l -niveau ongeveer 3 maal, <lit is geassocicerd met een (verwachte) remming van 70% van de DPP-4-activiteit. Echter, de grootte van het infarct en cardiale functie warcn gclijk in de met DPP-4-rcmmer bchandelde dieren en controle dieren. Ook alle andcrc metingen van cardiale remodeling waren onveranderd. Mogelijke redenen voor <lat DPP-4 rcmming geen effect heeft op de cardiale remodeling in <lit model zijn: de doscring, de gebruikte analoog, de bereikte GLP- l levels, de timing van de bchandeling en de bestudeerde diersoort. Deze resultaten wijzen crop <lat ondanks de stijging van actieve plasma GLP- l levels door remming van de DPP-4-activiteit, een langdurige behandeling met de DPP-4-remmer vildagliptine hct hart nict substanticcl bcschcrmt in een post-Ml model in ratten.
In hoofdstuk 5 wilden we de effecten van de DPP-4 remmer vildagliptine onderzockcn in een vroeg stadium van diabetische cardiomyopathie. Omdat de incidcntic van diabetes toeneemt verwachten we vaker diabetische cardiomyopathie te zien, gckcnmerkt door myocardialc dysfunctie bij diabetes patienten, in de afwczighcid van coronairlijden of hypertensie. Op <lit moment zijn er slechts weinig gegevens beschikbaar over de effecten van specifieke anti-diabetische behandeling op de myocardiale functie en metabolisme. We hebben Zucker Diabetic Fatty (ZDF) rattcn gebruikt, <lit zijn ratten met een mutatie in het gen voor de lcptine receptor. Dczc mutatic is geassocieerd met obesitas en diabetes. Dit model hcbbcn we gcbruikt om de myocardiale veranderingen en mechanismen te bestudcren die relevant zijn voor het mctabool syndroom. De dieren ontwikkelen insuline-resistentie in het begin van de studic (lecftijd van IO weken), blijkend uit verhoogde glucose- en insulinespiegels. In de daarop volgende 15 weken van het experiment daalden de insuline niveaus in de ZDF diercn aanzienlijk, wat aangecft <lat de alvleesklier niet mccr functioneerde.
Het hart van de ZDF ratten toonde ecn gestoorde diastolischc functic, ccn veranderend metabolisme en fibrose. Functieparameters E, E/A-ratio, en TVls, gemeten via cchocardiografie, waren significant afgenomen in de ZDF-groep in vergelijking met de controle Zucker lean ratten. Deze veranderingen waren geassocieerd met mecr collageen dcpositie, zowel intcrstiticcl en pcrivasculair, en cen verhoogdc collagecn I eiwit expressie. P-38 MAPK en P-PKA wcrden gei"dcntificccrd als potcnticlc mechanismcn van de myocardiale dysfunctie en fibrose. Daamaast zijn er veranderingen in het myocardiale mctabolismc gevonden in de huidige studie, inclusief een afwijkcnde vetstofwisseling en glucose homeostase. Verhoogde NEFA waren aanwczig in de ZDF dicren, en de hocvcclhcid myocardiaal glycogeen was significant verhoogd. De verhoogdc glycogeen levels rcsultcerden in ecn verminderde fosforylatie van GSK-3 en GLUT4. Behandeling met vildagliptine verminderde myocardiale fibrose en linker ventrikel stijfbeid in de diabetische dieren, <lit leidde tot een trend van
1 36
Nederlandse samenvatting
een verbeterde diastolische functie. Deze veranderingen waren geassocieerd met een afuame van collageen I levels en fosforylering van p-38 eiwit expressie. Normalisering van de glycogeen hoeveelheid en toename van de fosforylatie levels van GSK-3 en GLUT4 eiwit wijzen op een verbeterd glucose metabolisme. Dit suggereert <lat vildagliptine de opname van glucose verbetert in <lit diabetische diermodel.
In hoofdstuk 6 hebben we onderzocht of diabetes geassocieerd is met een toegenomen incidentie van hartfalen na een coronaire bypassoperatie (CABG) in de IMAGINE (lschemia Management with Acupril post bypass Graft via Inhibition of the coNverting Enzyme) trial. De IMAGINE was een dubbel-blind, placebo-gecontroleerde, gerandomiseerde, internationale multicenter studie om te onderzoeken of een ACEremmer, quinapril, vroeg toegediend na CABG de cardiovasculaire mortaliteit en morbiditeit zou kunnen verminderen. Van de 2553 patienten had 10% diabetes, waarvan 60% werden behandeld met metformine en 24% werden behandeld met insuline. Tijdens een follow-up van ongeveer drie jaar (mediaan) was de incidentie van de primaire (samengestelde eindpunt van cardiovasculaire dood of reanimatie na een hartstilstand, niet-fataal myocardinfarct, coronaire revascularisatie, instabiele angina pectoris waarvoor ziekenhuisopname noodzakelijk was, gedocumenteerd angina pectoris waarvoor ziekenhuisopname niet noodzakelijk was, beroerte en hartfalen waarvoor ziekenhuisopname noodzakelijk was) en secundaire (van de primaire eindpunt met de toevoeging van transient ischaemic attack en alle andere cardiovasculaire gebeurtenis waarvoor hospitalisatie vereist was) IMAGINE eindpunten of "major" coronaire events vergelijkbaar tussen de patienten met en zonder diabetes. Echter er was een 3-voudige hogere incidentie van ziekenhuisopname ten gevolge van hartfalen bij diabetespatienten. Verder was er een trend naar minder ziekenhuisopnames ten gevolge van hartfalen bij patienten met diabetes behandeld met metformine, wat duidt op een potentieel beschermend effect voor hartfalen bij diabetes. Ook uit deze studie blijkt weer <lat diabetes de kans op hartfalen sterk vergroot, een bevinding die consistent is met andere klinische observaties en experimentele studies. Metformine lijkt het beste eerste keus middel te zijn.
Toekomstperspectieven
Diabetes en hartfalen zijn veelvoorkomende ziekten die invloed op elkaar hebben. Vee! ziekten staan niet op zichzelf. Dit geldt voor obesitas, hypertensie, het metabool syndroom, en zeker voor diabetes en hartfalen. Deze conditie kan warden omschreven als het cardiometabool-syndroom, omdat deze twee ziekten elkaar kunnen versterken en elkaar kunnen veroorzaken, <lat wil zeggen <lat patienten met diabetes een hoog
1 37

risico hebben op hart- en vaatziekten en daaropvolgend hartfalen, en in omgekeerde volgorde, hartfalen patienten met diabetes hebben een slechtere uitkomst. Om deze reden is het cardiometabool-syndroom het laatste decennium uitgegroeid tot een belangrijk nieuw onderwerp in het onderzoek en in de behandeling in de cardiologie. Er zijn weinig studies die deze ziektes tegelijkertijd bestuderen, daarom is het aan te raden om het spectrum van deze ziekten en niet de twee ziekten afzonderlijk te bestuderen. We zullen verdere studies uitvoeren om ans verder te verdiepen in het cardiometabool-syndroom, met zowel diabetes en hartfalen.
Uit zowel klinische studies als experimentele studies blijkt dat antidiabetica niet allcen van nut kunnen zijn om glucoselevels te corrigeren, maar dat ze oak rechtstreeks invloed kunnen hebben op het hart. Onze experimentele studie toonde aan dat metformine cardiale remodeling vermindert in het post-MI niet-diabetische hartfalen model 4
• Op basis van deze experimentele studie hebben we de hypothese dat metformine een potentieel gunstig effect heeft bij niet-diabetische patienten met linker ventrikel dysfunctie. Daarom hebben wij een fase IV klinische studie opgezet en gestart, met de naam Metformin to Reduce Heart Failure After Myocardial Infarction (GIPS-lll, NCT01217307). Deze studie loopt en zal de effecten van metformine bij niet-diabetische patienten na een myocardinfarct evalueren. Niet-diabetische patienten na een ST-elevatie myocardinfarct warden geselecteerd en krijgen 500mg metformine tweemaal daags gedurende 4 maanden. De primaire uitkomst is het effect van metformine behandeling op de linker ventrikel ejectiefractie. De incidentie van cardiovasculaire gebeurtenissen tijdens de follow-up is de secundaire uitkomst.
Door de jaren heen zijn er een groat aantal experimentele studies geweest die beschermende effecten hebben gerapporteerd van anti-diabetische geneesmiddelen op het cardiovasculaire systeem. Het merendeel van deze studies zijn gedaan in nietdiabetische dieren, zoals beschreven in dit proefschrift. Daarentegen zijn de resultaten van het relatief kleine aantal klinische studies tot nu toe meestal negatief of tegenstrijdig geweest in hun bevindingen s-s in vergelijking met de gerapporteerde experimentel<? data. De verklaring voor deze tegenstrijdige uitkomsten is grotendeels onduidelijk, rnaar het benadrukt het belang van grate klinische studies. Zeker voor de nieuwere anti-diabetische drugs zoals GLP-1 analogen en DPP-4-remmers zijn er veelbelovende en consistente resultaten verkregen uit experimentele studies waarin hun potentie om het cardioprotectief te werken duidelijk wordt, rnaar wederom zijn er grate klinische trials nodig. De investering in dit onderzoek zal het begrip van het werkingsmechanisme van deze geneesmiddelen vergroten en zal zeker nieuwe inzichten geven in de relatie tussen diabetes en hartfalen en mogelijke kansen bieden om hierop te intervenieren.
1 38

Nederlandse samenvatting
References
I . Levy D, Kenchaiah S, Larson MG, Benjamin EJ, Kupka MJ, I lo KK, et al. Long-term trends in the incidence of and survival with heart failure. N Engl J Med 2002;347: 1 397-1402.
2. Cohn JN, Bristow MR, Chien KR, Colucci WS, Frazier OH, Leinwand LA, et al. Report of the National Heart, Lung, and Blood Institute Special Emphasis Panel on Heart Failure Research. Circulation I 997;95:766-770.
3. Fedak PW, Verma S, Weisel RD, Li RK. Cardiac remodeling and failure: from molecules to man (Part I). Cardiovasc Pathol 2005;14: I - I I .
4. Yin M, van der Horst IC, van Melle JP, Qian C, van Gilst WH, Sillje HH, et al. Metformin improves cardiac function in a non-diabetic rat model of post-Ml heart failure. Am J Physiol Heart Circ Physiol 20 I I ;.
5 . Eurich DT, McAlister FA, Blackbum DF, Majumdar SR, Tsuyuki RT, Varney J , et al. Benefits and harms of antidiabetic agents in patients with diabetes and heart failure: systematic review. BMJ 2007;335:497.
6. Eurich DT, Tsuyuki RT, Majumdar SR, McAlister FA, Lewanczuk R, Shibata MC, et al. Metformin treatment in diabetes and heart failure: when academic equipoise meets clinical reality. Trials 2009;10: 1 2.
7. Fisman EZ, Tenenbaum A. A cardiologic approach to non-insulin antidiabetic pharmacotherapy in patients with heart disease. Cardiovasc Diabetol 2009;8:38.
8. Gavin JR 3rd, Bohannon NJ. A review of the response to oral antidiabetes agents in patients with type 2 diabetes. Post grad Med 20 1 0;122:43-5 1 .
1 39

l

Acknowledgements

What an experience!
Four years can be a long period during which many changes can occur. However, when I look back at this period, these four years felt like they flew by: I still clearly remember the first day I came here in the middle of the night. People around me were interested in the reasons why I came over, and to be honest, in the beginning I did not have a clear vision myself. I would often answer: "I would like to know more of the world and experience a different culture. Now I feel I know the answer and I can say there is no better way to spend the passed four years, which were memorable, pleasant and meaningful. People here in the Netherlands are hospitable and helpful, and the department provided a good environment for both studying and practicing research. Although there were difficult moments at time, due to the understanding and support from all of you, I always managed to pull through and was able, with great pleasure, to finish this thesis. I would like to express my sincere gratitude to everybody who was involved in this project.
First and foremost, I would like to thank my promoter Prof. dr. Wiek van Gilst. Dear Wick, thank you very much for your support through the years. Thank you for giving me opportunity to exercise and improve my work. You really helped me in finding out what I like and what kind of person I want to be. Your expertise, guidance, and continuous encouragement have always inspired me through the difficult time of my study. I would also like to thank you for your concerns about my future career and without your help, I would never have been writing these words !
1 would like to thank my co-promoters Dr. Rudolf de Boer and Dr Herman Sillje. Dear Rudolf, 1 enjoyed all the discussions we had about work and life. As you know, I am not a confident person: your advice, encouragement and understanding helped me to strengthen up my confidence and made me "survive". 1 am also impressed by your optimistic character. You can always find the positive side of pretty much every situation. You are an enthusiastic person and encouraged me to keep my head high, even during the more difficult times. Thank you for your trust and long-lasting support. Dear Herman, your rigorous attitude in both research and writing is unforgettable. Without your help in the study and correction of the manuscripts, I would never have finished this thesis.
My utmost thanks for the critical reviews from the reading committee members, Prof. Dr. M.P. van den Berg, Prof. Dr. A.A. Voors and Prof. Dr. J.H. Kingma. Thank you for your consideration and efficient assessment of my thesis.
1 42
Acknowledgements
My special thanks go to everybody from the GUIDE office. Thank you for the financial support and problem solving capabilities during my study.
From the Department of Cardiology I would like to thank Dr. Iwan van der Horst and Dr. Joost van Melle for their contribution to my first published article.
I also would like to express my warmest gratitude to my nice colleagues in the Department of Experimental Cardiology. Carla and Danielle, thanks your help with everything both in and out of work. Carla, many thanks for being there with me to go to the dentist ! Pim, Beatrijs, Alexander and Peter, you are hard-working supervisors and generous, thank you for your helpful suggestions on my work during the PhD meetings and lunch meeting. Irene, Hasan, Maxi, it is nice to hear your stories about life as a postdoc. Thank you all for sharing experience with me. Maxi, thank you so much for all your hard work on my thesis. You always know how to make a sentence more beautiful.
I deeply appreciated all the help from our technicians. Dear Maaike Goris, I had a great time working with you during my first animal experiment. It was a difficult period for me. When I felt confused and lost, you came to help me and finished my first experiment which was so important for me. Although it was a rough start, we eventually ended up great by finishing the entire job together. Thank you very much for your help and time. Dear Inge and Bianca, we had a great time working together in CDL. I learned a lot of animal experimental techniques from both of you. Thank you for all of the help from you. Dear Janny, I am grateful for all your help in the molecular analysis. Dear Martin, Silke, Linda and Bibiche: thank you for your help, guidance and patience during my lab duties.
Many thanks to all my lovely PhD colleagues. Dear Irma, you were so friendly to give me so much useful information about the PhD defense. This helped me a lot. Thank you for all your encouragements. I loved our talks together. Dear Hisko, you are a very hard-working guy. Every time I would see you, you would be in the lab. Thank you for all your support and guidance. Dear Willem-Peter, thank you for setting a good example in finishing your thesis. My old roommates, Anne-Margreet, Mariusz, Michael, Reinout, Atze and Frank, thank you all for many interesting talks and funny jokes during our time together. All of you made me feel at home and relaxed during working hours. I also obtained lots of knowledge on Dutch culture from all of you. Mariusz, you are kind person who likes to help pretty much everyone in our group. Dear Anne-Margreet, as one of my Paranymphs, I would especially like to thank you for all your hard work and effort to help me with the defense preparations, including
1 43
writing my Dutch summary for me. Michael and Frank, you are such funny guys who arc very interested in Chinese culture and you like to learn Chinese ! ! Some day I hope both of you are able to speak Chinese and visit China again. Reinout, thank you for inviting me to your home, and get the chance to meet your wife and your daughter. I remember I made your daughter cry when I gave that panda toy to her: she is so funny. I wish you and your family all the best in the future. Atze, you arc so impressive with your "art work". You had so much patience while helping me with the colorful figures and I wish you good luck in the future.
For other PhDs, Megan, Wardit, Leonie, Renee, Niek, Vincent, I wish you all good luck during your projects.
To our badminton coach, Adriaan, thank you very much for teaching us your badminton techniques! We had many wonderful times together.
Special thanks to my Chinese friends in the Netherlands. Life is a journey! It was wonderful to meet up so far from home. The sad thing is we now have to go our own separate ways at this time. Qian Cheng and !iii, thank you for helping me the first two years. Lu Bo, Han Jina, Zhao Yan, Tan Hongtao, Wei Yunwci, Hun an, Sundi, I wish you all a wonderful life in China. Hongjuan and Deli, I wish you a great time in the Netherlands and I hope you get together with your family soon. For many other Chinese friends I got to know in Groningen: Liu Bo, Yu Zilin, Xiao Yu, Miao Yan, Liu Heng, thank you for the great times we shared together: especially all the cooking, playing badminton and card games. I wish you all a great future whatever you do and wherever you are.
I also wish to express my sincere appreciation to my promoter in China. Dear Prof. yanjie Lu, I appreciate your help and concern very much, without your encouragement, I would never have gone to Groningen and finish my PhD. You are always patient and nice to me. You are more than a teacher. I am grateful that I was able to be your student.
To my family:
ffi� (8}t�Mt� , !�i�Hh,fW8#F=f z.,'GJ, , !2J, ntrIJthlu!?:¥9:{:f ,f:Jt�n�i3:tl::&:it , 1El.Jt tE P-J 'Li' rg_ fh,fl' J -_a)tJJt!ii!�if&l't'-JA . Jtfh,ff JiJ:JJtfj��Jt JJ)Z � , fJMJ;it-1=5 , Jtfh,ff Jtft T JJt -·IJJ . tEi3: Bl (f.J llI!if , w-JC:JJt:fifixl�Ji!l,�fh,ffJ , I*! � .'�:l-��A·!*e,:;: , J/¥/� ·�+�;!0.is:B!Jtx,J(j{J:if)t'rd' i't''.l . JJtXfh,ff J�� , 1lrlit Htf1j;fJt'.tlt1� i=I c.Jt I� ;fb(8 , J;J
144

Acknowledgements
T § i=.zjliJT �,11'] , fE!)tdh,ffJ!PMJK�f!J!f�ft. Tfij)t-:fm l�!H1ft-Jx�ft. fh,fi'JiJG
ftidn-ff J ft-JMHtL :is:Jtft-]I�t,;: ft-J 1* l*1 o !�iM1h,ff J� T ft-1-W i¥'-ft-J1**:Et
:Ii, :is: ffi-W 'fl-iJ:ft El c.�JK�iPx El c., -W:ffl3Jt:1h,ff J ft-JJ}J :W o t5U,¥r1h,ff J 1J<:iif;_:!;J
1* fil!J� , *lflr ,�1 � !
ffi�ft-J��. �ft-JA��-T ��. ��A�m���ffift-J� �. ftJtffi:!;f�ffi ft-JA, �Jtft�tlft-JM*�M��ft-JA, ��ft*��:is:#��. ili��Wfi-
1-,w A ft-JJifi ;s= , fl=!JtliRHh,-��ffi ft-J ��;; �, iJ: ft T felt 1*JKfiffif�tmlilR ft-J Amt tE ft :!;J :itI o 1h, 1iR� ft-m}.!;. .LI:: 1!i :k ft-J A , Jt PJ � -1-A� M" ft-J A , :is: 1:iJ ii\ft � 1M tE ,1)
� . -�ft���*ft-J"� ' ����ffift-J -W , ft:ffl3�ffl�*ft-J�*:ffl3Mm�
,,�j!i:ft-J ' iMiMfh,�ft:+iJ \[ T -1-mtf O iMi�HdlID-1L��!Sttf=l=-ft, xt-�=}Jt , t5Hh,
li'lHdlx�M"f.ll'li 'tR* !
Thanks to everybody who has ever supported me: life has become deeper. Your love
and support keeps me out of plight. In the end I can see a new world. You bring the
best out of me and make my life even more splendid. Last but not least, thanks for life,
which gives me so much!
Meimei Yin
1 45

1/1,tJO JJjf;
Related Documents











