
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Edinburgh Medical Journal February 1951
UNCOMMON DRUG RASHES
By G. A. GRANT PETERKIN, M.B.E., M.B., F.R.C.P.Ed.
LTHOUGH, like the character in Bernard Shaw's play, I am " a
^evout believer in the department of witchcraft called medical science," cannot at times help agreeing with Voltaire's definition that
" a
"
ysician is one who pours drugs of which he knows little into a body 0 which he knows less." Hence the title of this lecture.
But one must remember that, considering the vast quantities of assorted drugs absorbed by the patient on his own initiative or on ^dical advice, the incidence of drug eruptions, i.e. dermatitis medica-
mentosa, is extraordinarily low. For instance, Kinnear (1950) states at in 1946 the people of Sweden consumed half a ton of phenolpthalein,
^e1: this communal catharsis does not seem to have been accompanied y any appreciable rise in the number of rashes due to this drug, ccording to Sutton (1949), the incidence of dermatitis medicamentosa
ln *937 at the University of Kansas Hospital was one in every 2000 Patients, and this tallies closely with the proportion seen in the Skin ePartment of the Edinburgh Royal Infirmary during the past four
years.
Strictly speaking, a drug eruption is not the reaction of the skin to the local application of a drug, but indicates absorption of the Medicament through some channel or another. Thus a drug rash May be produced in many ways?the actual deep inunction of a drug sUch as mercury ; the inhalation of one like ephedrine ; the injection ?f one like gold or arsenic ; the insertion of one into a cavity such as
mouth, rectum, vagina, bladder, lungs or wounds ; and finally Vla the placenta or mother's milk. Of course, once the skin has been Sensitised to a drug which has produced a contact dermatitis, the eternal administration of this in future may give rise to a drug rash either generalised or closely simulating the original dermatosis. This action is well exemplified by reactions to sulphonamides and penicillin.
Many drug reactions, however, do not appear to be true allergic phenomena, and some are really due to toxins liberated from a septic ?cus by the action of the medicine, e.g. the occurrence of erythema Nodosum or erythema multiforme after the treatment of a streptococcal
A Honyman Gillespie Lecture delivered on 8th June 1950. VOL. LVIII. NO. 2 41 D

42 G. A. GRANT PETERKIN
infection of the throat with sulphonamides. Others, again, appear o e due, in part at least, to hypovitaminosis, as in the case of tropical ic enoid dermatitis due to mepacrine and in sulphonamide light ermatitis. Curiously enough, those unhappy individuals, sometimes
re erred to as "
atopic," subject to asthma, hay-fever and eczema, are particularly apt to develop drug rashes, and it is the exception to
o tain a history of such diseases in patients with dermatitis medica- mentosa.
A drug may be taken for weeks, months or years before it produces a reaction, or the skin may show its intolerance after a single dose.
goo example of the former is the pustular eruption which occurs a
!t!j a Pat^ent ^as been taking a cough mixture containing potassium
10 1 e or months or years ; and of the latter, the urticaria produced ^ t
vj rSt *nject*on ?f penicillin in 1943 in a man who could not possibly have been previously sensitised to it. The time required for this sensitisation seems to be 7 to 14 days, but after this has been
fh^ ,1S 6 react*on may occur within forty-eight hours. Once
is as appened, the same cutaneous response may be expected ?i ?C<~,Ur use ?f that particular drug and also sometimes to re a e substances or even on occasion to apparently unrelated su stances. The response, too, occurs to doses considerably lower
ose used pharmacologically, but is quite different from the ognise toxic effect of the medicine. No known antibodies have
emonstrated in these cases, though no other explanation would a equate to explain the majority. Though intradermal and
p c tests sometimes give positive findings, it is generally agreed that they are quite unreliable in these patients. aturally, the physician wants to know what drugs are liable to
produce rashes. The answer is that practically all drugs have been ?
aS Pro<^uc^nS eruptions, with a very few exceptions, which c u e common purges such as castor oil, cascara sagrada, and salts
magnesium sulphate. The dermatoses due to drugs may take many orms and can mimic almost every kind of skin disease. There- ore, one must constantly bear in mind the possibility that a drug has een responsi le for the patient's condition, even though it closely
resembles some common skin trouble. It should also be remembered hat in not a few cases drugs may not only produce a rash but also ? ? may be attributed to infection. A good example of
is is t e drug-fever caused by sulphonamides which has often led o e patient being given more and more assorted sulpha drugs.
esions closely resembling the following diverse conditions can be ue so e y to drugs . lupus erythematosus ; acne vulgaris ; malignant Un??"rS ' scarlet fever ; measles ; lichen planus ; psoriasis ; erythema mu ti orme
, erythema nodosum ; pemphigus ; purpura ; erysipelas ; sma -p?x and exfoliative dermatitis. This afternoon I do not intend to give a ist of all the drugs and the rashes they may produce as this 1st can e found in any text-book on dermatology, but instead to

UNCOMMON DRUG RASHES 43
deal with a few of the frequently prescribed medicines and indicate some of the curious reactions they can cause. The drugs which I ave selected are :?
1. Phenolpthalein
2. Barbiturates
3. Quinine 4. Mepacrine
5. Heavy Metals, e.g. gold, bismuth and arsenic 6. SULPHONAMIDES
7. Antibiotics
But before doing so, I would like to draw attention to one of the
^ost curious kinds of dermatitis medicamentosa?the Fixed Drug ruption. This was first recognised in the eighties and clearly escribed by Louis Brocq in 1894, and was due to antipyrin. ramowitz and Noun (1937) aptly quote Brocq's original descrption
^vhich still is perfectly accurate :?" The cutaneous manifestations aPPeared as round or oval apparently oedematous plaques from the SlZe ?f a coin to that of a palm, recurring on various parts of the body and
accompanied by an itching or burning sensation. The patches ^ere dusky red at their onset and showed definite borders. At times
ese lesions progressed to form bullae. Desquamation or crusting v
_
ter the bullous lesions) appeared as the eruption faded, leaving a P^mentation of variable shade and duration in the areas affected.
special characteristic of the eruption was the tendency to relapse and recurrence of the lesions in situ."
The pigmentation, which may vary in shade from a faint cafe-au-lait to a deep blue-black, may take a long time to disappear. It is melanin
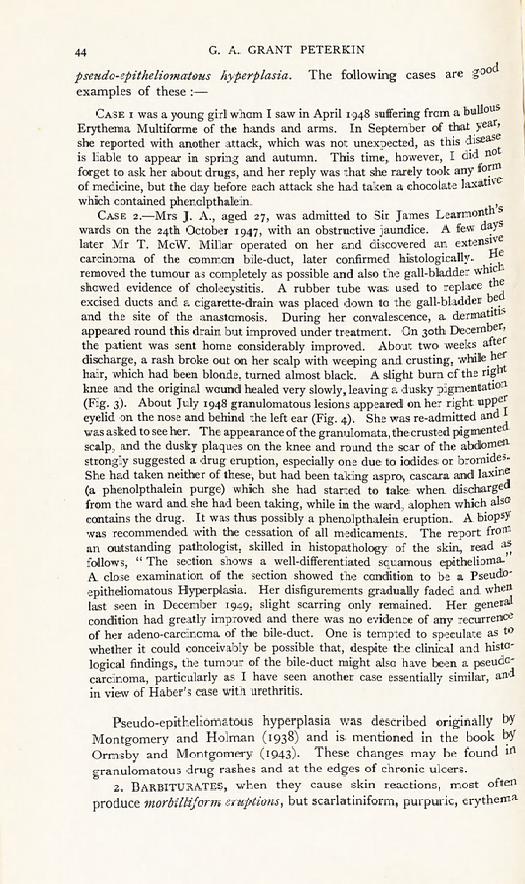
Pigment and therefore dopapositive. In the case of heavy metals, e PJgmentation is partly due to the drugs themselves. This curious reaction (Fig. 1) can be provoked by many drugs,
^eluding phenolpthalein, sulphonamides, antipyrin, phenacetin, bar- . rates, arsenicals, quinine, salicylates, bromides, iodides, mercury, lsrnuth, penicillin and mepacrine.
r- PHENOLPTHALEIN characteristically produces a Fixed Drug ruption, in the form of multiple dusky-red plaques which fade
gradually when the drug is stopped, leaving a brown pigmentation. ls contained in about 100 official and proprietary remedies (Belote
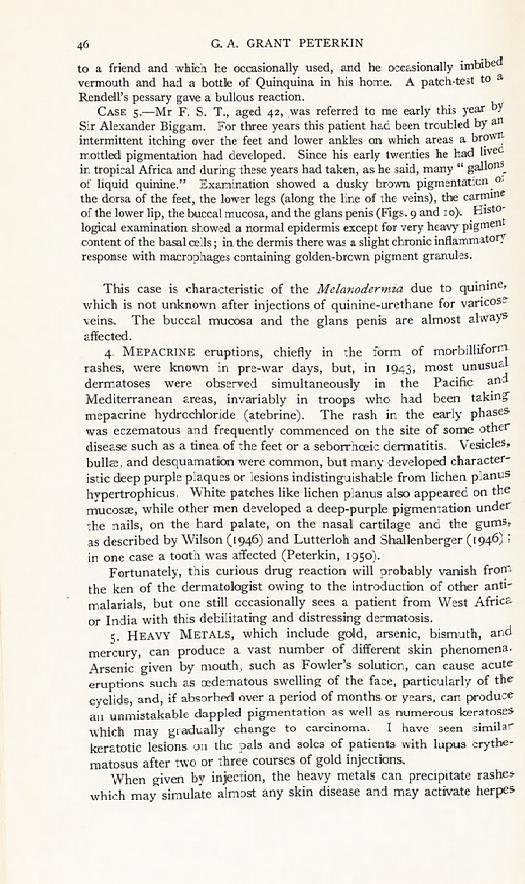
and Whitney, 1937), while one must remember that it is contained in
ri?colate and chewing gum laxatives and in some pink icing-sugars. n occasions it occurs as a single perianal plaque (Fig. 2), and is an
Unc?mmon cause of pruritus ani, while Haber (1950) described a
case with urethritis. This drug may also cause localised pruritus with no skin changes,
as described by Aubrey (1932) and Hunt (1932), and on occasions erythema multiforme and granulomatous lesions which histologically closely resemble squamous-cell carcinoma?the condition called
44 G. A. GRANT PETERKIN
pseudo-epitheliomatous hyperplasia. The following cases are good examples of these :?
Case i was a young girl whom I saw in April 1948 suffering from a bull?uS
Erythema Multiforme of the hands and arms. In September of that year' she reported with another attack, which was not unexpected, as this disease is liable to appear in spring and autumn. This time, however, I did
no
forget to ask her about drugs, and her reply was that she rarely took any f?yItl of medicine, but the day before each attack she had taken a chocolate laxat^e which contained phenolpthalein.
Case 2.?Mrs J. A., aged 27, was admitted to Sir James Learmont 5
wards on the 24th October 1947, with an obstructive jaundice. A few day5
later Mr T. McW. Millar operated on her and discovered an extensive carcinoma of the common bile-duct, later confirmed histologically- f1 removed the tumour as completely as possible and also the gall-bladder whic showed evidence of cholecystitis. A rubber tube was used to replace the
excised ducts and a cigarette-drain was placed down to the gall-bladder be and the site of the anastomosis. During her convalescence, a dermatitis
appeared round this drain but improved under treatment. On 30th December* the patient was sent home considerably improved. About two weeks after
discharge, a rash broke out on her scalp with weeping and crusting, while her
hair, which had been blonde, turned almost black. A slight burn of the right knee and the original wound healed very slowly, leaving a dusky pigmentation (Fig. 3). About July 1948 granulomatous lesions appeared on her right uppe^ eyelid on the nose and behind the left ear (Fig. 4). She was re-admitted and
*
was asked to see her. The appearance of the granulomata, the crusted pigmente scalp, and the dusky plaques on the knee and round the scar of the abdomen strongly suggested a drug eruption, especially one due to iodides or bromides- She had taken neither of these, but had been taking aspro, cascara and laxme
(a phenolpthalein purge) which she had started to take when discharged from the ward and she had been taking, while in the ward, alophen which also contains the drug. It was thus possibly a phenolpthalein eruption. A biopsy was recommended with the cessation of all medicaments. The report from
an outstanding pathologist, skilled in histopathology of the skin, read aS
follows, " The section shows a well-differentiated squamous epithelioma.
A close examination of the section showed the condition to be a Pseudo-
epitheliomatous Hyperplasia. Her disfigurements gradually faded and when last seen in December 1949, slight scarring only remained. Her general condition had greatly improved and there was no evidence of any recurrence of her adeno-carcinoma of the bile-duct. One is tempted to speculate as to
whether it could conceivably be possible that, despite the clinical and histo-
logical findings, the tumour of the bile-duct might also have been a pseudo- carcinoma, particularly as I have seen another case essentially similar, and in view of Haber's case with urethritis.
Pseudo-epitheliomatous hyperplasia was described originally by
Montgomery and Holman (1938) and is mentioned in the book by
Ormsby and Montgomery (1943). These changes may be found in
granulomatous drug rashes and at the edges of chronic ulcers. 2. BARBITURATES, when they cause skin reactions, most often
produce morbilliform eruptions, but scarlatiniform, purpuric, erythema

UNCOMMON DRUG RASHES 45
Tnultiforme-like and fixed eruptions may be seen. In pre-war days when phenobarbitone was often prescribed as the original luminal, a generalised pruritus was occasionally noted, but these are now rare.
ery occasionally, as described by Moss and Long (1942), Stevens- Johnson Disease, which may be a particularly severe type of erythema Multiforme, is seen with involvement of the mouth, eyes, genitalia, as WeH as other areas (Fig. 5).
During the past twelve months I have seen four cases of a peculiar lnd, as they in some ways look clinically like lupus erythematosus and
ln s?nie like tinea corporis (Figs. 6 and 7). Histological sections show a
non-specific inflammatory reaction such as is commonly seen in drug erUptions. This dermatosis appears as erythematous circinate patches Wlth a raised papulo-vesicular edge, and usually affects the face and neck, areas exposed to the sun, though parts such as the arms may be involved. The " bat's -wing" distribution simulates lupus erythe- matosus most effectively.
Case 3.?In spring 1949, Miss J. W., aged 67, noticed an erythematous Tash affecting the cheeks, forehead and neck. This gradually became more extensive during the hot summer and she was referred for advice on the 23rd August. Despite the close resemblance to lupus erythematosus, the colour nes were not exactly true, there was no follicular plugging, and there was a ennite raised papulo-vesicular margin. For the past two years she had been
. Klng phenobarbitone, gr. i, twice daily. A section showed a non-specific lrtflamrnatory reaction with no sign of lupus erythematosus. Treatment c?nsisted in stopping the drug, and by early November the rash had dis- appeared.
3- QUININE can produce many varied kinds of reactions, the most characteristic being a scarlatiniform erythema, an eczematous
dermatosis and a melanodermia. Physicians should be aware, and should warn quinine-sensitive patients, that the drug is not only used 0r malaria and as a febrifuge, but is also an ingredient in such things
as tonic-water, and alcoholic drinks like Italian vermouth, and aperitifs, c-g- Quinquina. Quinine-urethane injections for varicose veins should 11 ?t be forgotten. The following two cases are good illustrations of Quinine sensitivity.
Case 4.?Mr A. C., aged 42, had no skin trouble until he was on his orteymoon in 1937. Within a week of marriage he developed an acute ermatitis of his penis and scrotum with gross oedema (Fig. 8). He suspected at this might have been caused by cocoa-butter pessaries, and on avoiding ese had no recurrence of the dermatitis until 1941 when he was in the Army, unng his Service career he had several eczematous attacks, which affected
Principally his scalp, though again the genitals were involved, though mildly. ese were diagnosed as seborrheic dermatitis, and disappeared after two
?r three weeks in hospital. Since demobilisation he has had several recurrences at
Regular intervals, with involvements of the scalp, ears, and redness of the eyelids and genitalia. Quinine sensitivity was suspected, as the so-called Seb?rrhoeic dermatitis might well have been due to a hair-tonic which belonged
vol. lviii. no. 2 d 2
46 G. A. GRANT PETERKIN
to a friend and which he occasionally used, and he occasionally imbibed vermouth and had a bottle of Quinquina in his home. A patch-test to
&
Rendell's pessary gave a bullous reaction. Case 5.?Mr F. S. T., aged 42, was referred to me early this year by
Sir Alexander Biggam. For three years this patient had been troubled by an
intermittent itching over the feet and lower ankles on which areas a brown mottled pigmentation had developed. Since his early twenties he had lived in tropical Africa and during these years had taken, as he said, many
"
gall?n^ of liquid quinine." Examination showed a dusky brown pigmentation 0
the dorsa of the feet, the lower legs (along the line of the veins), the carmine of the lower lip, the buccal mucosa, and the glans penis (Figs. 9 and 10). Histo-
logical examination showed a normal epidermis except for very heavy pigment content of the basal cells; in the dermis there was a slight chronic inflammatory response with macrophages containing golden-brown pigment granules.
This case is characteristic of the Mclanodermia due to quinine, which is not unknown after injections of quinine-urethane for varicose veins. The buccal mucosa and the glans penis are almost always affected.
4. MEPACRINE eruptions, chiefly in the form of morbilliform
rashes, were known in pre-war days, but, in 1943, most unusual dermatoses were observed simultaneously in the Pacific and Mediterranean areas, invariably in troops who had been taking
mepacrine hydrochloride (atebrine). The rash in the early phases was eczematous and frequently commenced on the site of some other disease such as a tinea of the feet or a seborrhoeic dermatitis. Vesicles,
bullae, and desquamation were common, but many developed character- istic deep purple plaques or lesions indistinguishable from lichen planus hypertrophicus. White patches like lichen planus also appeared on the mucosae, while other men developed a deep-purple pigmentation under the nails, on the hard palate, on the nasal cartilage and the gumsr as described by Wilson (1946) and Lutterloh and Shallenberger (1946) ;
in one case a tooth was affected (Peterkin, 1950). Fortunately, this curious drug reaction will probably vanish from
the ken of the dermatologist owing to the introduction of other anti-
malarials, but one still occasionally sees a patient from West Africa or India with this debilitating and distressing dermatosis.
5. Heavy Metals, which include gold, arsenic, bismuth, and
mercury, can produce a vast number of different skin phenomena- Arsenic given by mouth, such as Fowler's solution, can cause acute
eruptions such as oedematous swelling of the face, particularly of the
eyelids, and, if absorbed over a period of months or years, can produce an unmistakable dappled pigmentation as well as numerous keratoses which may gradually change to carcinoma. I have seen similar
keratotic lesions on the pals and soles of patients with lupus erythe- matosus after two or three courses of gold injections.
When given by injection, the heavy metals can precipitate rashes
which may simulate almost any skin disease and may activate herpes

UNCOMMON DRUG RASHES 47
zoster. Thus these injections can be responsible for eczematous, Vesicular, bullous, morbilliform, scarlatiniform, purpuric rashes or for eruptions similar to seborrhoeic dermatitis, erythema multiforme, or hchen planus.
This lichenoid eruption is very like a mild mepacrine drug rash and usually commences like an intractable seborrhoeic dermatitis (Figs. 11
and 12). It is in these cases that B.A.L. therapy is most effective, though B.A.L. itself can produce cutaneous reactions. A somewhat uncommon reaction is acrocyanosis with erythema
and swelling of the palms and soles following injections of arsenic ?r gold, and similar to that occasionally observed just before the
efflorescence of a mepacrine rash. To these drugs can now be added !Tlercury as a cause of this type, for Warkany and Hubbard (1948), ln an interesting paper, showed that of 20 cases of acrodynia (" pink disease") 18 showed mercury in the urine, in 15 over 5? microgram Per litre, while 80 per cent, of controls showed none at all. The mercury ad been absorbed as calomel,
"
teething powders " and ammoniated
^ercury ointment. This finding has been confirmed by Bivings and ewis (1948) and by other physicians. It has also been noted that
atypical cases of " pink disease "
may occur in children of an age ?r?up older than is generally associated with the disease.
Case 6.?E. H., aged 2 years 5 months, was seen by me at the Royal 0spital for Sick Children at the request of Dr J. L. Henderson, who has mdly supplied the following history. At the age of 9 months the boy developed
af1 erythematous rash of the extremities, and from that age the parents noticed at a general muscular weakness was present. The rash and the weakness
Persisted, as well as a itchy follicular eruption of the trunk. The child was Pacid, never of an irritable disposition, and was of normal intelligence. lamination showed a quiet child with swollen dusky-red feet and hands
arici an erythemato-papular rash on the body. There was marked generalised ypotonia of all muscles and all reflexes were absent except for flexor plantar
responses. He was able to pull himself to his feet and move round his cot yt was ungainly and apparently could not walk unaided. A provisional lagnosis of atypical Pink Disease was made. It was found that the child ad been given mercury in the form of a grey powder in large doses since the
of 6 months. All investigation, including blood counts and biopsy, gave tle help in the elucidation of his case, but three weeks after admission the
excretion of mercury was 1-05 mgm. per litre and about ten days later 90 Micrograms per litre. As he was showing slow but steady progress, it was
ecided that B.A.L. should not be given in the meantime, despite the good results obtained by Bivings and Lewis (1948).
The classic work by Carleton and Peters and their colleagues (1946) showed that lewisite interfered with carbohydrate metabolism by attacking the sulphur groupings of the protein to which Vitamin Bx ls linked, and that this toxic action could be counteracted by B.A.L. ^ hich absorbed the arsenic. More recently it has been demonstrated that a similar action occurs with other heavy metals and this too can

48 G. A. GRANT PETERKIN
be controlled by B.A.L. Hughes (1950) tentatively suggests that the-
injuries to the body from heavy metals can result in lesions indistinguish- able from those which characterise vitamin deficiency. He instances- three cases?a purpuric rash due to gold ; an extensive seborrhoe1C dermatitis due to the same cause ; and an exfoliative dermatitis caused by arsenic. Many others have drawn attention to this resemblance
to
vitamin deficiencies, not only in people with gold and arsenic intoxica-
tion, but also in mepacrine eruption and in sulphonamide light dermatitis. The mepacrine rash produces lesions suggestive
0
vitamin A and vitamin B complex deficiency, and the sulphonamide one suggests deficiency of riboflavin and nicotinic acid. These effects
have been attributed to liver damage or to intereference with the
synthesis of vitamin B in the gastro-intestinal tract and by micro-
organisms. The mercurial diuretics such as mersalyl can be responsible f?r
various eruptions, but characteristically produce an (EdematousV
erythematous swelling around the site of the injection. 6. SuLPHONAMIDES. Fortunately the dangers of sulphonamide
therapy are now widely recognised, but even yet one sees many
reactions to sulphonamides, especially of the type associated with
photosensitivity. This is the most common kind and resembles to-
some extent a severe seborrhoeic dermatitis, though it can be readily distinguished from this by several features?the carmine of the lower
lip shows a marked cheilitis ; conjunctivitis is usually present ; and the nose is always involved. Sulphonamides can also cause rashes like lupus erythematosus, erythema multiforme, erythema nodosum and pemphigus, as well as morbilliform, scarletiniform, acneform, and
purpuric rashes. The chemical relationship of the sulphonamides (e.g. sulphanilamide
or para-aminobenzene-sulphonamide) with para-aminobenzoic acid
again draws one's attention to the association of drug eruptions and
possible vitamin deficiency. It is not surprising that the drug Para- amino-salicyclic acid can also produce skin reactions. Kierland and Carr (1949) have reported four cases of intolerance to the drug?one a Fixed Drug Eruption and the others scarlatiniform rashes.
I happen to have seen one case of an entirely different type.
Case 7.?Miss C. E., aged 16, was admitted to hospital in December 1948 with an infiltrative tuberculous lesion at the right apex, associated with
fatigue, malaise, anorexia and loss of weight. After 6 months, she developed an effusion at the right base and three months later cavitation in the right apical region. On the 15th October 1949, she began P.A.S. in a dosage of
15 grm. daily and by the 27th November had had a total of 540 grm. On
the 15th November the cervical glands on the left side became enlarged and
tender, but there was no acute infection of the throat and a swab showed no
significant organisms. On the 27th November she developed diarrhoea and
vomiting and her temperature rose to iox? F. ; the P.A.S. was discontinued. On the day her temperature rose, she developed an extensive rash on the face,
ftt.'C -
Fig i.?Fixed drug eruption, due to sulphonamides. Fig i.?Fixed drug eruption, due to sulphonamides.
Fig. 2.?Fixed drug eruption of perianal region, due to phenolpthalein. Fig. 2. Fixed drug eruption of perianal region, due to phenolpthaleir

II
gEjfl
Fig. 3.?Case 2 Fixed drug reaction
Phenolpthalein?deeply pigmented plaque on knee.
Fig. 3.-?Case 2 Fixed drug reaction
Phenolpthalein?deeply pigmented plaque on knee.
Fig. 4.?Case 2 Fixed drug eTU^ ai0v
Phenolpthalein pseudoepitheH011 hyperplasia of nose and eyelid.
Fig. 4.?Case 2 Fixed drug erU^ll?totf Phenolpthalein pseudoepitheli?nia hyperplasia of nose and eyelid.
w
ml
Fig. 5.?Stevens-Johnson disease. Fig. 5.?Stevens-Johnson disease. Fig. 6.?Phenobarbitone rash?lupuS erythematosus type below ear.
Fig. 6.?Phenobarbitone rash?-lupuS erythematosus type below ear.

^henobarbitone rash?ringworm-like type on forearm.
^ ??.?III
IG' ^henobarbitone rash?ringworm-like type on forearm.
Fig. 8.?Case 4?Quinine reaction. Fig. 8.?Case 4?Quinine reaction.
^?- II.?Gold dermatitis showing
seborrhoeic dermatitis " appearance. ,JG' ?Gold dermatitis showing seborrhcjeic dermatitis " appearance.
s:
II
m
:
jf.
> r"
Fig. 12.?Gold dermatitis showing lichenoid lesions
on abdomen.
Fig. 12.?Gold dermatitis showing lichenoid lesions
on abdomen.

Fig. 9.?Case 5?Melanodcrmia of mouth, due to quinine. Fig. 9.?Case 5?Melanodermia of mouth, due to quinine.
Fig. xo.?Case 5?Melanodermia of leg, due to quinine. Fig. io.?Case 5?-Melanodermia of leg, due to quinine.
UNCOMMON DRUG RASHES 49
chest and back which spread to the limbs. Treatment with penicillin and Benadryl having had no effect, she was transferred on the 6th December to Bangour Hospital, under the care of Dr Alastair W. Wright, who has been good enough to give these details of her case and who called me into con- futation on the nth December. Examination showed a severe eruption ^distinguishable from the exudative type of Sulphonamide Light Dermatitis. The exposed areas were worst involved ; the face and neck were crusted and cozing, the hands vesico-bullous. A marked glossitis and stomatitis as well as a blepharoconjunctivitis were present, but the picture was not that of Stevens-Johnson Disease. On the forearms was a heliotrope maculo-papular rash and on the trunk were maculo-papular and scarlatiniform areas. W.B.C. s Were 36,000 per cu.mm. with 50 per cent, eosinophils.
From the 15th December the rash steadily improved and the temperature settled to normal. By the 21st January 1950 she had completely recovered from her dermatitis. On that date she was given a test dose of 4 grm. P.A.S. at 4 p.m. That evening she vomited, the following day a widespread papular rash appeared and the temperature rose to ioi? F. Within a week this rash had disappeared except for a slight residual area on the chest. She was
transferred to the tuberculosis wards and a month later had a defluvium capitis with eventual full regrowth of hair.
7- Antibiotics. The introduction of the antibiotics has resulted *n so much amelioration in the total of human suffering that it is with regret that one must mention that they too have their imperfections. Within a few months of the introduction of penicillin, it was shown that a considerable proportion of the patients treated developed reactions of various kinds, apart from the extremely common contact dermatitis. Of 209 patients given penicillin by injection, 12 were
observed by Lyons (1943) to develop a giant urticaria sometimes
accompanied by joint pains. This reaction is now so well recognised that the dermatologist considers it the commonest cause of acute
Urticaria. Intolerance to penicillin may reveal itself in other ways ?by the occurrence of an eczematous outbreak ; erythemato-papular and vesicular eruptions ; erythema nodosum ; severe rashes not unlike
Sulphonamide Light Dermatitis ; the reactivation of a dormant
fungus infection, as described by Feinberg (1944) ; or, most uncommon, an erythematous cedematous swelling around the site of the injections.
Streptomycin is even more liable than penicillin to provoke skin troubles. Roseolar, maculo-papular, morbilliform, scarlatiniform, Urticarial, follicular, as well as erythema multiforme-like rashes have been described by Steiner and Fishburn (1947), while Pallister (1949) described two deaths from dermatitis and stomatitis during strepto- mycin therapy.
Like penicillin and streptomycin, Chloromycetin can cause a
distressing stomatitis, but I have no experience of it being responsible for a rash.
Aureomycin also not infrequently incites a stomatitis and, though Spink and Yow (1950) say that they
"
have not encountered blood
dyscrasias, skin eruptions or fever due to the drug," yet Peck and

5o G. A. GRANT PETERKIN
Feldman (1950) record three?one urticarial ; one like erythema multiforme with urticaria ; and one eczematoid of the groins and
scrotum. Nelson (1950, personal communication) observed the re-
currence of a contact dermatitis due to penicillin, after aureomycin
therapy. I have comparatively little experience of the drug, but I
have had two patients with reactions?in one a generalised desquama- tion occurred after ten days' treatment, and in the other a solitary
plaque of erythema nodosum over the shin appeared after a few days- No doubt more general use of the newer drugs will give rise to other
types of toxic reaction. In this paper no mention has been made of treatment, chiefly
because the essential treatment of drug rashes consists in masterly
inactivity, despite the strong temptation to do something positive for the patient. I categorically disagree with those who recommend the antihistamines in drug eruptions, particularly as they themselves are by no means guiltless in causing reactions. Those I have seen
have been not dissimilar to sulphonamide eruptions, such as light dermatitis.
Summary
No attempt has been made in this article to enumerate all the
drugs which can produce rashes, nor to mention all the eruptions that have been listed as being due to them. The intention has been to
record a series of somewhat unusual reactions provoked by drugs that are in everyday use?phenolpthalein, barbiturates, quinine, mepacrine, the heavy metals, the sulphonamides, and the antibiotics.
The curious phenomenon of the Fixed Drug Eruption is described and examples are given, particular mention being made of a pseudo- epitheliomatous hyperplasia due to phenolpthalein.
Phenobarbitone, among other things, is shown, in four patients, to have caused an eruption with a close clinical resemblance to both
lupus erythematosus and tinea corporis. An acute exudative dermatosis due to various quinine products is
depicted and also a melanodermia due to this drug. A brief reference to mepacrine dermatitis is followed by notes on
rashes due to heavy metals, with especial reference to a form of acro-
cyanosis and its relation to " pink disease." P. amino-salicylic acid occasionally gives skin reactions, one case
being indistiguishable from a severe sulphonamide light dermatitis. The fact that penicillin and streptomycin can inflict dermatoses
on patients is well known, but new remedies such as aureomycin, often regarded as relatively non-toxic, may also give rise to distressing reactions, two of which are recounted.
Acknowledgements are due to Mr T. McW. Millar, F.R.C.S., for Figs. 3 and 4 ;
to Dr Donald Forsyth for Fig. 5 ; to Dr W. B. MacKenna for Figs. 11 and 12 ; and
to Mr T. C. Dodds, F.R.P.S., for the remainder.
UNCOMMON DRUG RASHES 5r
REFERENCES
Abramowit., E. W., and Noun, M. H. (1937), Arch. Derm. Syph. Chicago, 35, 875. Aubrey, G. (1932), Lancet, 1, 1015 Belote, G. H., and Whitney, H. A. K. (1937), Arch. Dertn. Syph. Chicago, 36, 279. Bivings, L., and Lewis, G. (1948), Journ. Pediat., 32, 63. Carleton, A. B., Peters, R. A., Stocken, L. A., Thompson, R. H. S., and
Williams, D. I. (1946), Journ. clin. Invest., 25, 497. Feinberg, S. M. (1944), Journ. Allergy, 15, 271. Haber, H. (1950), Brit. Jourti. Derm. Syph., 62, 22. Hughes, W. (1950), Brit. Med. Journ., 1, 634. Hunt, E. (1932), Lancet, 1, 905. Kierland, R. R., and CARR, D. T. (1949). Proc. Mayo. Clin., 24, 539. KlNNEAR, J. (1950), Practitioner, 164, 213. Lutterloh, C. H., and Shallenberger. P. L. (1946), Arch. Derm. Syph. Chicago,
53, 349- J-Yons, C. (1943), Journ. Amer. Med. Ass., 123, 1007. Montgomery, H., and Holman, J. C., Jr. (1938), Proc. Mayo Clin., 13, 465- Moss, R. E., and LONG, W. E. (1942), Arch. Derm. Syph. Chicago, 46, 386. ORMSBY, O. S., and MONTGOMERY, H. (1943), Diseases of the Skin, 6th ed., Kimpton,
p. 780. Pallister, R. A. (1949), Brit. Med. Journ., 2, 1271. Beck, s. M., and Feldman, F. F. (1950), Journ. Amer. Med. Assoc., 142, 1137- Beterkin, G. A. G. (1949), Brit. Journ. Derm. Syph., 61, 287. Spink, W. W., and YOW, E. M. (1950), Journ. Amer. Med. Assoc., 141, 965. Steiner, K., and Fishburn, G. W. (1947), Arch. Derm. Syph. Chicago, 56, 511. Sutton, R. L., and Sutton, R. L. Jr. (1949), Handbook of Diseases of the Skin,
C. V. Mosby Co., St Louis, p. 100. ARK ANY, J., and HUBBARD, D. M. (1948), Laricet, 1, 829.
Wilson, D. J. (1946), Arch. Derm. Syph. Chicago, 54, 377.
Related Documents











